
Abstract
The treatment of hyaline articular cartilage lesions has been considered a great health problem and has been challenging to physicians for more than 2 millennia. 13 During the past decades, several promising treatments of full-thickness cartilage and osteochondral articular lesions have emerged.
Bone marrow–stimulating procedures were introduced by the Pridie drilling. In this technique, the trabecular bone is drilled, allowing bone marrow mesenchymal stem cells and fibroblasts to invade the lesion along with the blood to form a clot. 33 The repair tissue produced is fibrous in character. Another technique is spongialization; the subchondral bone plate is removed to allow fibrous tissue to grow from the bone marrow and cover the trabecular bone. 8 More recently, abrasion arthoplasty was introduced; a superficial abrasion of the subchondral bone plate surface allows bleeding from capillaries into the abraded area, which creates a fibrous cover of the lesion. 15
The most popular and frequently used is the microfracture technique including abrading the tidemark and creating small holes perpendicular to the subchondral bone plate to allow bleeding into the defect. 36 Microfractures usually result in a fibrous-fibrohyaline unstructured repair tissue. This tissue lacks the biomechanical and viscoelastic features of hyaline cartilage. The potential short-term improvement in symptoms is usually followed by repair tissue failure and potentially by gradual deterioration to osteoarthritis and return of symptoms. 21
Subsequent techniques aim to replace the cartilage in the defect area, using osteochondral autografts, allografts, or synthetic materials. Autologous periosteal or perichondreal grafts were tried in the past but without long-term success. 2,18 More recently, allografts or synthetic polymers (PGA or PLLA scaffolds, TruFit CB, Smith & Nephew, London, United Kingdom) or ceramics (carbon fibers) have also been used. 9 Mosaicplasty is a popular reconstructive technique during which autologous osteochondral cylinders (harvested from less weightbearing areas of the femoral condyles) are transferred into the defect area and implanted in a mosaic pattern. 12
Autologous chondrocyte implantation (ACI) or transplantation (ACT), introduced in 1987 in Sweden by our group, was the first cell-based biological approach to the treatment of full-thickness cartilage lesions. Autologous chondrocytes from cartilage biopsy samples are isolated and cultured in the laboratory and then implanted into a debrided lesion under a periosteal cover. Periosteum has been used to provide a waterproof covering of the chondrocyte suspension. Moreover, it has also been suggested that the periosteal cambium layer cells may play a chondrogenic role, providing growth factors and potential mesenchymal stem cells developing into chondrocytes. 7,14,22,26,31
The first clinical report was published in 1994 and showed satisfactory results for isolated femoral condyle lesions. 5,6,11 Several cohort studies followed, showing good to excellent results for the vast majority of the patients. 5,29-31 In the study with the longest follow-up period, clinical outcomes were improved 5 to 11 years postoperatively compared with the baseline. 29 Although this study gave valuable information about medium- to long-term follow-up, it is of great interest to investigate what happens 10 to 20 years after the implantation to evaluate the effect of the prolonged age and the onset of osteoarthritis that will probably affect some patients after so many years. 32
The purpose of this study was to investigate the long-term clinical results of ACI with periosteum, assessing outcomes in patients covering a period that starts with the first operated cases, in 1987, and follow-up of 10 to 20 years postoperatively. Our hypothesis, based on previous cohort studies, was that ACI provides a durable solution to the treatment of full-thickness cartilage lesions of the knee, maintaining the good clinical results even after a long period of time.
Materials and Methods
Patients
From October 27, 1987, when the first ACI was performed, until the end of 1998, 590 patients had been operated with ACI with periosteum. The indication for an ACI procedure was any symptomatic full-thickness cartilage lesion up to 16 cm2. Patients with previous surgeries were also included. Patients with meniscal or anterior cruciate ligament (ACL) lesions were operated with ACI along with the treatment of their concomitant lesion and restoration of the knee stability. Age over 65 years or prolonged osteoarthritis were considered a contraindication for ACI.
Three hundred forty-one surveys were posted to the treated patients. Two hundred twenty-four patients replied to our mail, corresponding to a response rate of 65%. They filled out 5 subjective questionnaires: Lysholm score, 19 Tegner-Walgren, 37 modified Cincinnati (Noyes), 25 Brittberg-Peterson score, 4,31 and Knee Injury and Osteoarthritis Outcome Score (KOOS). 34 The KOOS and Noyes questionnaires were not described until the end of the 1990s; thus, there are no preoperative values for any of the patients. However, they are widely used today, and we used them in our long-term follow-up for comparison with future studies. The Brittberg-Peterson functional assessment score was based on a 10-cm visual analog scale and with 13 studied parameters. Value 0 corresponds to normal functional status and the maximum of 130 to severe disability. 31 The Lysholm and KOOS scores are both validated questionnaires to be used in cartilage repair. 16,34 The patients were also asked to grade their current status during the past 10 years as better, worse, or unchanged. Finally, they were asked whether they would do the operation again (yes or no).
Information about baseline measurements and features of cartilage lesions or concomitant injuries were collected retrospectively from the patients’ medical files. Some questionnaire measurements at baseline and interim assessments were also available from previous studies.
Seventy-four percent of the patients had isolated cartilage lesions (159/215 patients), while 26% had multiple lesions (56/215). Forty patients had 2 lesions (one only in the patella). Twelve patients had 3 lesions, and 4 patients had more than 3 lesions. The mean size of lesions per patient was 7 cm2 (range, 0.6-27), while the mean size per lesion was 5.3 cm2 (range, 0.6-15.8). The age of the patients at the time of ACI was 33.3 years (SD, 9.5; range, 14-61.5).
Concomitant procedures with ACI were performed mainly because of ligamentous insufficiency. Forty-six patients had an ACL reconstruction (42 had it at the same time with ACI and 4 before ACI). Twenty one of the patients (21/224) had a high tibial osteotomy before or during ACI, 5 had a reconstruction of a collateral ligament, and 2 had a posterior cruciate ligament (PCL) reconstruction.
Thirty-four percent (76/224) had a history of meniscal lesion and partial or total meniscectomy before or during ACI. Sixty-six percent (148/224) did not have meniscal involvement at least until the implantation. Thirty-seven percent of the patients (30/82) had a previous operation that included drilling or shaving of the chondral lesion.
The current follow-up evaluation pertains to 12.8 years on average since the time of implantation (range, 9.3-20.7). The average age of the patients was 33.3 years (range, 14-61) at the time of the ACI. The current average age is 46 years at the follow-up evaluation (range, 26-74) (Table 1). Statistical significance was defined by a P value of less than .05. We carried out univariate association tests for continuous variables using the t test or paired t test. We analyzed binary outcomes using the χ2 test or Fisher exact test. S-Plus software was used for the analysis.
Evaluated Patients 10 to 20 Years Postoperatively and Their Current Age a
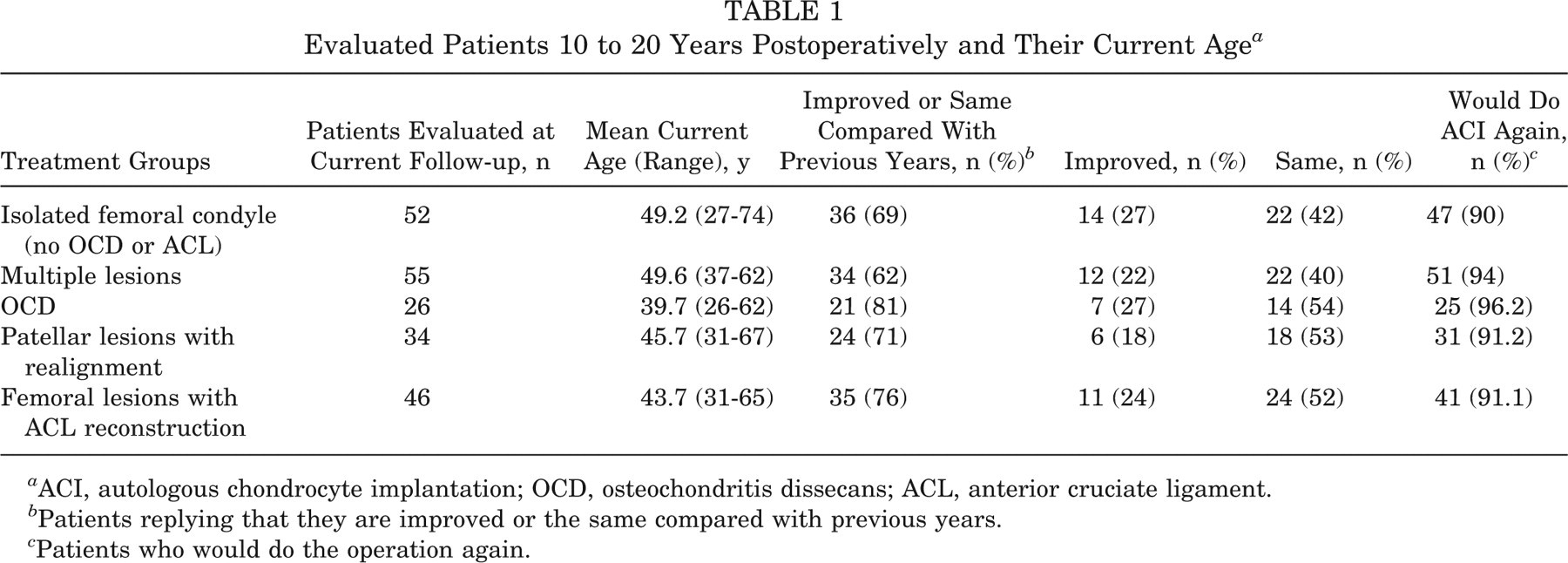
ACI, autologous chondrocyte implantation; OCD, osteochondritis dissecans; ACL, anterior cruciate ligament.
Patients replying that they are improved or the same compared with previous years.
Patients who would do the operation again.
Cartilage Retrieval
Arthroscopic evaluation of the knee joint was performed as the first stage of ACI under general or spinal anesthesia and tourniquet controlled bloodless field. During the arthroscopy, the entire knee joint was assessed for any concomitant meniscal lesion, cruciate ligament rupture, or other injury. In cases of meniscal injury, the treatment was performed after the cartilage biopsy, while ACL or PCL reconstructions were scheduled for the second surgery. The whole cartilage was examined by inspection and probing. The location, size, and depth of the cartilage lesion were recorded. 5,28,29 Small pieces of cartilage (300-500 mg in total) were retrieved from a less weightbearing area, usually the medial rim of the trochlea and occasionally from the lateral rim of the trochlea or femoral notch, for culture and subsequent implantation.
Chondrocyte Implantation
After the cell culturing, a second surgery was performed to implant the cells into the cartilage defect area. A parapatellar arthrotomy, which should be adapted to the specific location of the cartilage defect, was undertaken.
Clinical and radiological assessments were performed to examine any potential indications for a realignment procedure. A realignment procedure was scheduled for patients with patellar lesions and patellofemoral malalignment. Tibial osteotomies were performed in cases of excessive varus or valgus deformity to protect the implanted area. If a corrective operation had been planned (osteotomy, reconstruction of extensor mechanism, ACL reconstruction), this took place before the implantation of the cells. In case of tibial osteotomy, medial transfer of the tibial tuberosity, or ACL graft fixation, the fixation was performed at the end of the procedure before the implantation of the cells.
The cartilage lesion area was assessed, incised, and debrided with a curette down to the subchondral bone and until reaching healthy cartilage in the periphery of the defect. Care was taken to avoid bleeding of the subchondral bone. Through a second incision, a periosteal patch slightly bigger than the lesion template was harvested from the proximal medial tibia. Fat fibers and vessels covering the periosteum were carefully removed before retrieval, making the flap as thin as possible. Then, the harvested periosteum was sutured over the defect area with the cambium layer facing the subchondral bone. 28 Injection of the cells’ suspension between the periosteum and the subchondral bone was performed, and the injection site was then closed with a suture and fibrin glue.
Results
Seventy-four percent of the patients (165/224) reported they were better or the same during the past years, while 26% reported they were worse. Ninety-two percent were satisfied with the operation and would do the ACI again (202/219). The Lysholm score was improved from 60.3 preoperatively to 69.5 in the latest follow-up (P = .009 from 2-sample t test, P = .0016 from paired t test pertaining to 58 patients). The Tegner score was 7.22 preoperatively and 8.2 at follow-up (P = .002 from 2-sample t test, P = .0008 from paired t test pertaining to 109 patients), and the Brittberg-Peterson improved from 59.4 preoperatively to 40.9 postoperatively (P < .001 from 2-sample t test, P = .004 from paired t test pertaining to 53 patients). The KOOS scores were 74.76 for pain, 63 for symptoms, 81 for activities of daily living (ADL), 41.5 for sports, and 49.3 for quality of life (QOL). The Noyes score was 5.4.
Subgroup analysis showed an inferior final outcome for the patients with bipolar lesions (18 patients in the patellofemoral joint, 2 in the medial and 2 in the lateral compartment) compared with patients with multiple unipolar lesions (Lysholm, P = .02; Tegner-Wallgren, P = .01; Brittberg-Peterson, P = .003; Noyes, P = .03; KOOS pain, P = .003; KOOS symptoms, P = .12; KOOS ADL, P = .001; KOOS sports, P = .14; KOOS QOL, P = .007). The presence of meniscal injuries before ACI or history of bone marrow procedures before the implantation did not seem to affect the final outcomes. Furthermore, the age or the size of the lesion did not seem to correlate with the final outcome.
Isolated Femoral Condyle Defects
Fifty-two patients with isolated femoral lesions were evaluated. Forty-one of the lesions were located on the medial condyle and 11 on the lateral, while the size per lesion was between 0.6 and 14 cm2 (mean, 4.9). The mean patient age at the time of surgery was 35.5 years (range, 16.7-61.6).
Forty-seven patients (90%) responded that they had benefitted from the treatment and would do the operation again. Thirty-six of the patients (69%) reported that their condition was the same or improved compared with previous years (Table 1).
The average Lysholm score was 60.1 (range, 46-81) before surgery and 72.6 (range, 25-96) at the end of the study (Table 2). The average Tegner-Wallgren score was 8 (range, 2-14) at the final measurement (Table 3). Thirty-seven patients (84%) had a score of 6 or more. The overall Brittberg-Peterson score was 65.9 preoperatively (range, 31-107) and 38.4 (range, 3-102.8) postoperatively, suggesting an overall improvement in the QOL and knee function (Table 3). The Noyes score was 5.4 (range, 1-9); the average KOOS was 77.3 for pain, 65 for symptoms, 83.1 for ADL, 45.1 for sports, and 51 for QOL (Table 4).
Mean Values of Lysholm Score Preoperatively (Available Number of Values in Parentheses) and in Current Follow-up, With P Values a
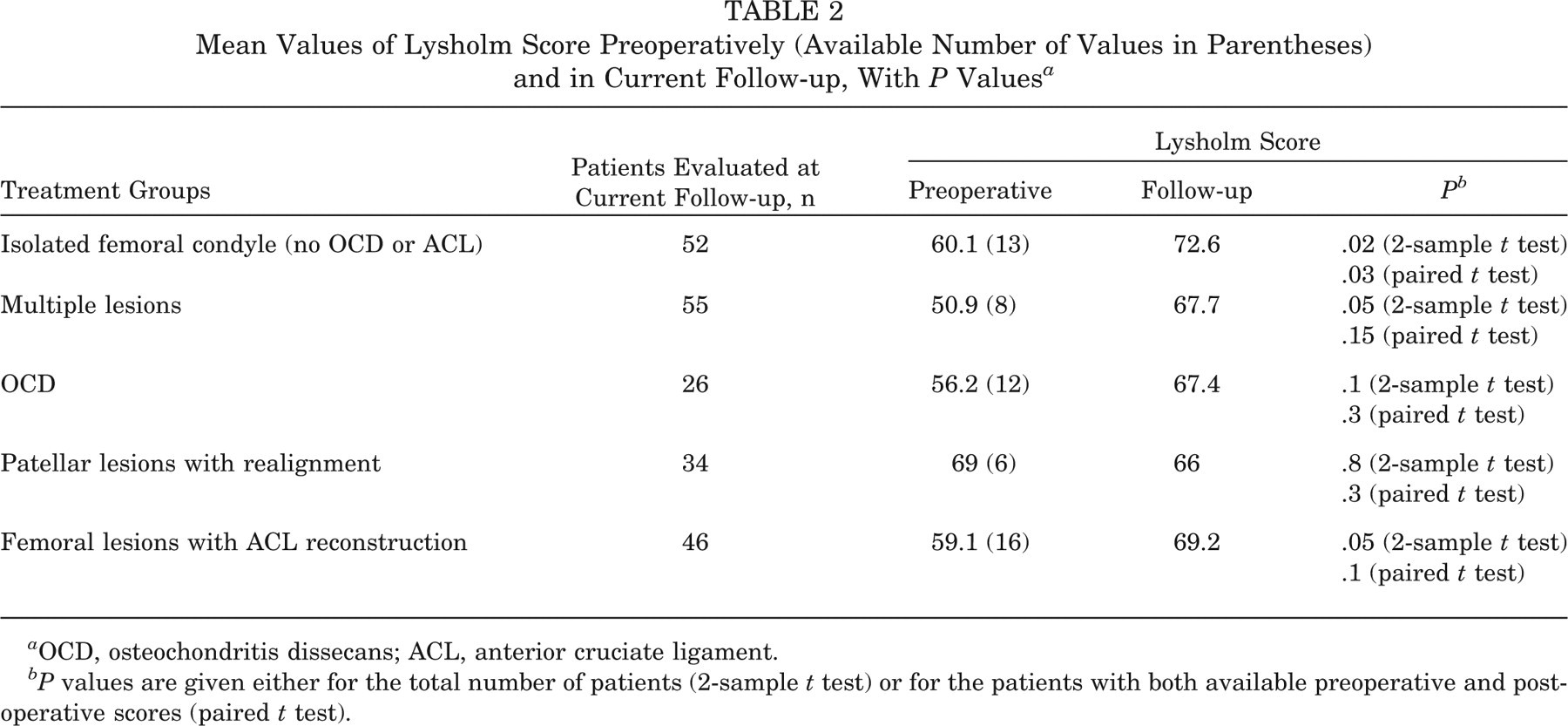
OCD, osteochondritis dissecans; ACL, anterior cruciate ligament.
P values are given either for the total number of patients (2-sample t test) or for the patients with both available preoperative and postoperative scores (paired t test).
Mean Values of Tegner-Wallgren and Brittberg-Peterson Scores Preoperatively (Available Number of Values in Parenthesis) and in Current Follow-up, With P Values a
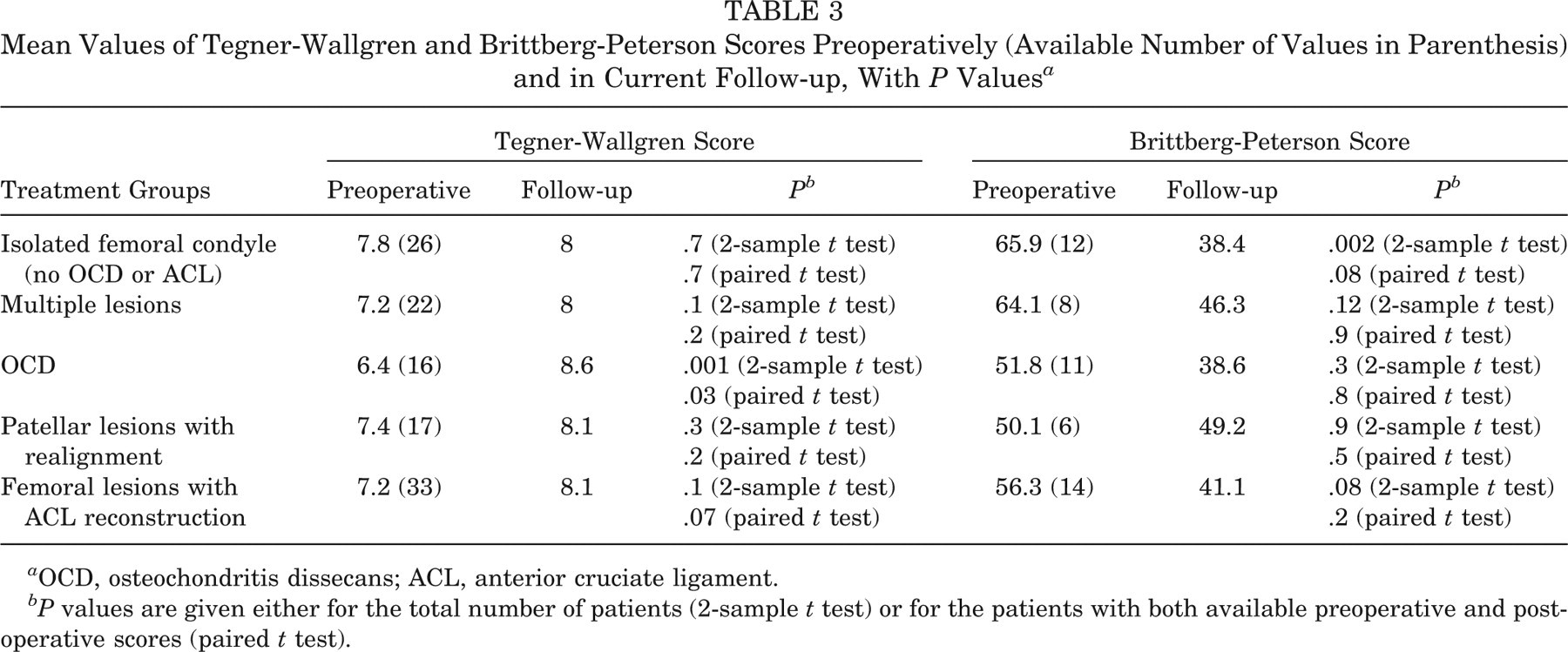
OCD, osteochondritis dissecans; ACL, anterior cruciate ligament.
P values are given either for the total number of patients (2-sample t test) or for the patients with both available preoperative and postoperative scores (paired t test).
Mean Values of KOOS Score and Noyes Score at 10 to 20 Years’ Follow-up a
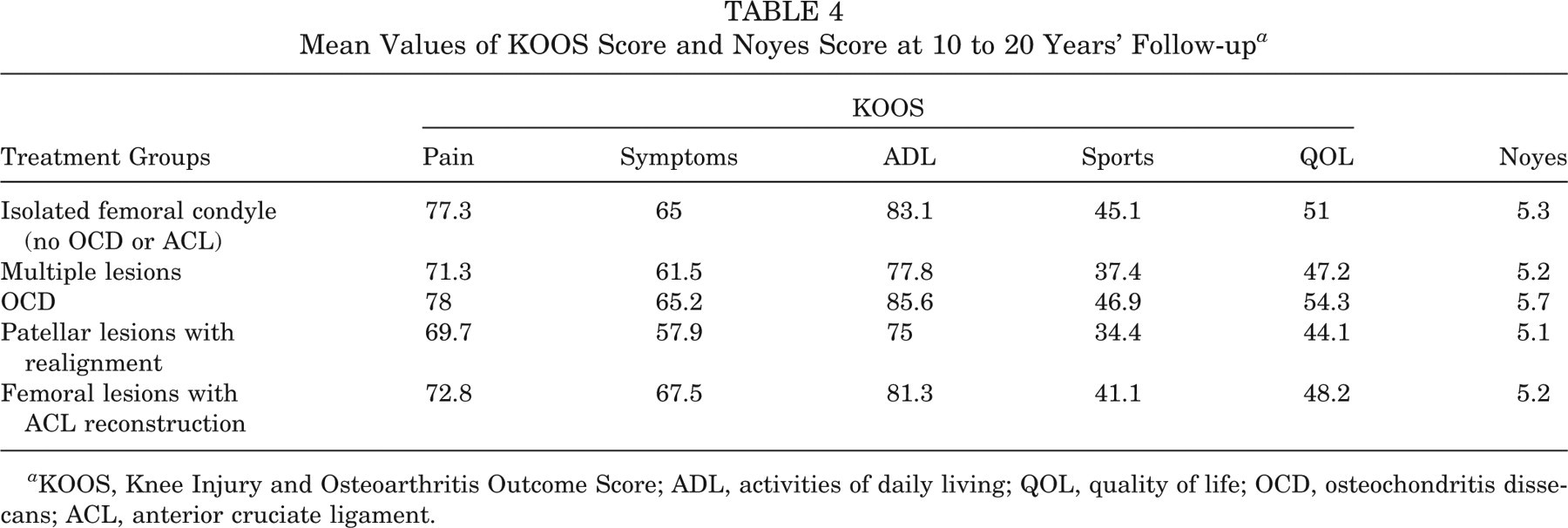
KOOS, Knee Injury and Osteoarthritis Outcome Score; ADL, activities of daily living; QOL, quality of life; OCD, osteochondritis dissecans; ACL, anterior cruciate ligament.
Multiple Femoral Condyle Lesions or Trochlea
Fifty-five patients had multiple lesions including a femoral condyle or trochlear lesion (mean, 2.4 lesions). Forty had 2 lesions, 10 had 3 lesions, and 5 patients had 4 lesions. Thirty-seven of those had a defect in the medial femoral condyle, 18 in the lateral femoral condyle, and 29 in the trochlea.
The average age at the time of the implantation was 37.8 years (range, 23.8-50.4), and the average size per lesion was 4.8 cm2 (range, 1.2-14). Thirty-four (61.8%) of those patients replied that they were better or the same compared with previous years, and 51 (94%) would do the operation again (Table 1).
The Tegner-Wallgren average score was 8 (range, 3-11), and the Lysholm was 67.7 (range, 17-100) at the time of latest follow-up (Tables 2 and 3). Overall, the Brittberg-Peterson was 46.3 (range, 1.7-115.8), and the Noyes was 5.2 (range, 1-10) (Tables 3 and 4). The KOOS score was on average 71.3 for pain, 61.5 for symptoms, 77.8 for ADL, 37.4 for sports, and 47.2 for QOL (Table 4).
Osteochondritis Dissecans Lesions
Twenty-six patients with osteochondritis dissecans (OCD) were evaluated. All lesions were isolated. Fifteen lesions were located on the medial femoral condyle, 9 on the lateral femoral condyle, and 2 on the patella. Average lesion size was 6.2 cm2 (SD, 2.9; range, 1-12). The average age was 26.8 years at the time of the implantation (range, 15.7-52.4). Twenty-one patients (81%) replied that they were better or the same compared with previous years. Twenty-five (96.2%) would do the operation again (Table 1).
The mean Lysholm score was 67.4 (SD, 16.4; range, 31-95) (Table 2). The Tegner-Wallgren score was 8.6 at the latest follow-up (SD, 1.6; range, 5-13) (Table 3). Twenty-four patients had a Tegner-Wallgren score ≥6. Preoperatively, the Tegner-Wallgren score was on average 6.4 (SD, 2.2; range, 1-9), and the mean Lysholm score was 56.2 (SD, 22; range, 13-85) (Tables 2 and 3). The total Brittberg-Peterson score was a mean of 38.6 (SD, 29; range, 2.7-99) at the end of the study and 51.8 (SD, 32; range, 9.4-104) preoperatively (Table 3). The mean Noyes score was 5.7 (range, 3-9); the KOOS was 78 for pain, 65.2 for symptoms, 85.6 for ADL, 46.9 for sports, and 54.3 for QOL (Table 4).
Patellar Lesions (With and Without Realignment)
There were 73 patients with patellar lesions (mean size, 5.1cm2; SD, 2.61; range, 1-12). Thirty-nine patients (of 73) had an isolated patellar lesion with an average size of 6.1 cm2 (range, 1-12). Eighteen patients had kissing lesions in the patellofemoral joint (patellar lesion: mean size, 3.7 cm2; range, 1-7.5; and trochlear lesion: mean size, 6.77 cm2; range, 1.3-20).
Thirty-four of those 73 patients also had some sort of realignment surgery. Twenty-one had an extensor mechanism reconstruction and trochleaplasty. Eight had an extensor mechanism reconstruction only, including tibial tuberosity transfer, medial soft tissue plication (vastus medialis obliquus and medial patellofemoral ligament), and lateral release (1 of those had it 6 years after the ACI, and another one also had an ACL reconstruction before the ACI). One patient had medial plication and trochleaplasty and one, lateral release and trochleaplasty. Three had a tibial osteotomy (1 of those had it 4 years after the ACI). The average age was 34 years (range, 14.1-57.2) at the time of ACI. Twenty-four of 34 patients (70.6%) replied that they were better or the same compared with the previous years, and 31 (91.2%) would do the operation again (Table 1).
The mean Lysholm score was 66 (range, 17-100) (Table 2). The mean Tegner-Wallgren score was 8.1 at the latest follow-up (range, 3-14), and 32 patients had a score ≥6 (Table 3). Preoperatively, the mean Tegner-Wallgren score was 7.4 (range, 3-14), and the mean Lysholm score was 69 (range, 47-85) (Tables 2 and 3). The final mean Brittberg-Peterson score was 49.2 (range, 31-65) compared with 50.1 (range, 31-65) preoperatively (Table 3). The average Noyes score was 5.1 (range, 1-10); the mean KOOS was 69.7 for pain, 57.9 for symptoms, 75 for ADL, 34.4 for sports, and 44.1 for QOL (Table 4).
Thirty-nine patients without need of a realignment procedure had preoperative ACI mean Lysholm and Brittberg-Peterson scores of 60.8 and 68, respectively. The current scores were 68.5 and 43.8, respectively. The Tegner-Wallgren increased from 6.9 to 7.8. Statistical analysis did not show any significant differences for any of the final outcomes between patients with and without a realignment procedure for patellar lesions.
Femoral Condyle Lesions With ACL Reconstruction
Forty-six patients had a femoral condyle lesion and also an ACL reconstruction. In 42 cases, the ACL reconstruction was performed at the time of implantation, and in 4 cases, the reconstruction took place before ACI. Thirty-seven patients had a lesion on the medial femoral condyle and 13 on the lateral femoral condyle. Thirty-seven had an isolated femoral condyle lesion, and the remaining 9 had from 2 to 4 lesions (6 patients with 2 lesions, 2 patients with 3 lesions, and 1 patient with 4 lesions).
The average size of medial femoral condyle lesions was 4.5 cm2 (range, 1.2-10), and the mean size of the lateral was 4.6 cm2 (range, 2.4-10.5). The average age at the time of the implantation was 31.1 years (range, 17.5-50.5). Thirty-four patients evaluated their current status to be better or the same compared with previous years, and 41 of them (91.1%) would do the operation again (Table 1).
The mean Tegner-Wallgren score was 8.1 (range, 3-15), and the mean Lysholm score was 69.2 (range, 34-100) (Tables 2 and 3). The average Brittberg-Peterson score was 41.1 (range, 2-103.4), and the Noyes score was 5.2 (range, 1-9) (Tables 3 and 4). The average KOOS score was 72.8 for pain, 67.5 for symptoms, 81.3 for ADL, 41.1 for sports, and 48.2 for QOL (Table 4). The preoperative values for the Tegner-Wallgren and Lysholm scores were 7.2 and 59.1, respectively; the Brittberg-Peterson total mean score was 56.3 (Tables 2 and 3).
Discussion
Autologous chondrocyte implantation is considered an effective treatment option for full depth chondral or osteochondral defects of the knee. 23,30 There are many studies demonstrating the durability of the clinical improvement even 11 years after the implantation. 29 However, given the young age of patients being operated for such lesions, a longer duration of symptom relief would be of great importance. It remains questionable how the repaired tissue reacts during aging and how it follows the natural gradual development of osteoarthritis at the age of 50s or 60s.
In the present study, we tried to assess the long-term effectiveness of ACI as far as 20 years after the first implantation performed in our center. The average age of participating patients at follow-up was 46.1 years, ranging from 25.8 to 74.2. Aging is anticipated to impose limitations on extreme or sports activities. A soccer player operated with ACI at the age of 30 years, having a Tegner-Wallgren score of 15 preinjury, is not expected to retain that score 15 years later at the age of 45 years, even if the cartilage lesion is filled with normal hyaline cartilage. This applies to the majority of patients after a long period of time; the level of activity also reflects the age or changes in social life.
Our study did not include a control group, for example, patients with untreated cartilage lesions or people with no lesions, to reflect the anticipated deterioration of activity level due to aging. That would be crucial to investigate how the expected changes of activity level with age compare with our findings. A study by Shelbourne et al 35 presented the physical history of untreated cartilage lesions over time. The evaluation took place 8.7 years after the surgery, and the patients all had ACL reconstructions, sustaining cartilage defect lesions of only 1.7 cm2 in size. A similar study was presented by Widuchowski et al 38 with a long follow-up time (10-15 years). However, Widuchowski et al studied only ACL-treated patients with small chondral lesions (mean defect size was 2.1 cm2), and therefore, their findings are not comparable with our results.
The limited availability of preoperative measurements in our sample decreases the statistical power of our comparisons. As all assessed scores were not used during the first years of our study, we lack some preoperative data for some patients. Therefore, the clinical generalizability of the findings pertaining to comparisons between the preoperative scores and long-term measurements is limited. Nevertheless, the final scores along with the high patient satisfaction reveal an increased level of activity and quality of life. Our patients sustained concomitant lesions, such as meniscal injuries or ACL ruptures. Although these lesions have been addressed before or during the ACI, the effect on the final outcome remains uncertain. In related literature, studies presenting long-term results in patients with nonreconstructed ACL ruptures reported a decrease in Lysholm score from 96 one year after the injury to 86 at 15 years’ follow-up. 17 The KOOS score is presented 15 years after an untreated ACL injury as follows: pain 90, symptoms 88, ADL 94, sports 76, QOL 74. 24 Age-specific KOOS scores in the general population are given by the epidemiological study of Paradowski et al 27 ; the mean KOOS score for the age group of 35 to 54 years was 87.4 men/88.8 women (pain), 86.5 men/89.5 women (symptoms), 89.1 men/88.6 women (ADL), 76 men/79.3 women (sports), and 77.7 men/83.4 women (QOL).
The KOOS results in our study are comparable with the results from the “STAR” clinical trial. 39 At 48 months, the average KOOS score was 72.2 for pain, 70.8 for symptoms, 55.8 for sports, 81 for ADL, and 52.2 for QOL, while the modified Cincinnati score was 6.31. The longest follow-up presented in this study was 48 months after the implantation, and the mean age of patients was significantly lower than in our study. That might be the reason for the slightly better scores regarding the sports domain of the KOOS score compared with our findings. However, the KOOS scores are similar to those presented in our study.
Multiple cartilage lesions (2 or more) of the femoral condyle or trochlea seem to provide similar subjective scorings preoperatively and at the final follow-up compared with other patient groups. However, patients with multiple lesions seem to undergo a progressive decline compared with previous years, with the bipolar lesions having an inferior outcome compared with the rest of the multiple lesions. Only 61.8% of patients with multiple lesions claimed to be better or the same compared with the previous assessment, although 94.4% would do the operation again. That probably reflects a possible deterioration during the past years, but this assumption remains to be proven. The increasing age of that patient group (reaching on average 33 years at the time of the implantation and about 46 years in the current follow-up [range, 26-74]) and the possible onset of osteoarthritis might explain this observation. However, Lysholm, Tegner-Wallgren, and Brittberg-Peterson scores appear significantly improved. The latest follow-up values do not differ from the other operated groups, even though average preoperative Lysholm and Brittberg-Peterson scores were much worse than in the other groups.
Lesions of the patellofemoral joint have always been more demanding and more difficult to treat than femoral condyle lesions. The first studies showed a significantly smaller benefit for patients with patellar lesions, comparable with those with multiple ones. 5,29 That can be explained by the more complex pathogenesis of such defects. They are usually the result of a more complicated anatomical malfunction, causing patellofemoral malalignment with maltracking or instability of the patella. Factors that may contribute to patellar instability are developmental malformations like dysplasia of the trochlear groove (eg, shallow or convex trochlea) or the patella, patella alta, or imbalance of the muscular function (malfunction of the vastus medialis obliquus). Subluxations are often present together with or without episodes of patellar dislocation, contributing to chondral lesions. Those anatomical or functional background factors must be recognized before ACI and must be addressed before or during the implantation of the chondrocytes.
Our series of 34 cases with patellar lesion and a concomitant realignment procedure shows results comparable with those from other patient groups. Level of activities according to the Tegner-Wallgren score is increased even 10 to 20 years postoperatively, and 91.2% seem to benefit from the surgery and would have it again. However, the Lysholm score, although giving final results similar to the other groups, was found almost equal to the preoperative levels, especially because of the relatively high preoperative scoring. This may be attributed to a remaining occasional patellar subluxation noticed as instability or giving way by the patients (25% of the Lysholm score is devoted for “instability”). The total Brittberg-Peterson score was also found to be lower than in the other groups and equal to the preoperative levels.
The patellar lesions without the need of realignment procedures show a different image, with both Lysholm and total Brittberg-Peterson scores being improved (from 60.8 to 68.5 and from 68 to 43.8, respectively). That indicates that more complicated cases needing realignment procedures may not keep improving over a long period of time, but they do not seem to deteriorate either.
Osteochondritis dissecans is probably the patient group with the best subjective results. A possible explanation could be the younger age of those patients, being on average 39.7 years old at the current follow-up compared with other groups ranging from 43.7 to 49.6. It is anticipated that the healing potential is increased in younger ages and the musculoskeletal recovery is more effective. Besides that, younger patients are not yet restricted in level of activities as the onset of osteoarthritis is not yet apparent.
Some caveats of our study must be acknowledged, most of them associated with the longitudinal nature of the study and the retrospective way of collecting preoperative data. We had a response rate of 65%; although this number is lower than the recommended limit of 70% and implies a reduced reliability of our results, it might appear as an acceptable rate given the long term of follow-up as many treated patients could not be reached or tracked. Moreover, many of the included patients were not followed during the last years; that makes it impossible to report the complication rate and any procedures performed during those years in a reliable way. Not all of the questionnaires had been answered preoperatively, as previously mentioned, reducing the power of the statistical comparisons. Finally, as there is no control group, no comparison can be made with the nonoperative treatment of cartilage lesions or with other possible surgical treatments. Furthermore, despite the improvement shown in all questionnaires, it remains questionable whether the amount of improvement is clinically significant.
The patients included in our study were treated with the first generation of ACI using periosteum for the coverage of the treated area. Second- and third-generation ACI techniques have been developed since 1987, using either manufactured coverings or scaffolds for the 3-dimensional culturing of the chondrocytes. 1,20 There is evidence from short- and medium-term follow-up studies that shows that these techniques have comparable or better results than those obtained from first-generation ACI. 10 Third-generation ACI performed fully arthroscopically can further improve outcomes in the future. 3 More studies of high quality are necessary to confirm the long-term effectiveness of these techniques.
According to the results from our study, first-generation ACI seems to be an effective and durable solution to the treatment of large full-thickness chondral and osteochondral lesions of the knee joint. Despite the initial controversy and skepticism regarding patellofemoral lesions, it seems that ACI provides satisfactory results in all cases, even in difficult cases with concomitant patellar instability. Our study shows that an improved clinical picture along with a high level of activities characterizes patients even 10 to 20 years after the implantation.
Footnotes
The authors declared that they had no conflicts of interest in their authorship and publication of this contribution.