
Abstract
Hamstring injuries are very common in sports. The majority are minor injuries, but a significant percentage may be major injuries as classified by Levine et al. 5 Proximal and distal avulsion injuries are described in the literature. These include complete avulsion of the proximal hamstring origin from the ischial tuberosity, as well as distal avulsion injuries. Distal avulsion injuries of the biceps femoris are the most common distal injury, and typically are associated with varus hyperextension mechanism multiligament knee injuries. 2-4,6,9 Isolated reports of distal semimembranosus avulsion have been reported. 1 This report is a retrospective case series reviewing our experience with 17 isolated distal semitendinosus tendon complete ruptures in elite-level professional athletes. There have been 2 case reports in the English-language literature. 7,8 This is the first reported case series related to distal semitendinosus ruptures in athletes and the first to report the results of treatment.
Materials and Methods
Study Group
Twenty-five cases of complete distal semitendinosus tendon ruptures were identified in elite-level athletes over the study period (1991-2005). There were 20 professional athletes, 4 collegiate athletes, 1 amateur male athlete, and no female athletes in the series. The study group consisted of 17 professional athletes followed for an average of 13 months (range, 4-55). Follow-up was obtained by office or training room examination by one of the authors (or a colleague if the player was in another organization) and discussion with the player, trainers, and strength/conditioning coaches. This retrospective case series is the collective experience from 2 sports medicine practices in 2 different major metropolitan cities. Eight National Football League players, 8 Major League Baseball players, and 1 National Hockey League player were included in the study group (Table 1). We have only seen this diagnosis in elite-level athletes. This retrospective study was conducted in a manner consistent with the principles of the Declaration of Helsinki.
Demographic Information and Recovery Times After Treatment for All 17 Players a
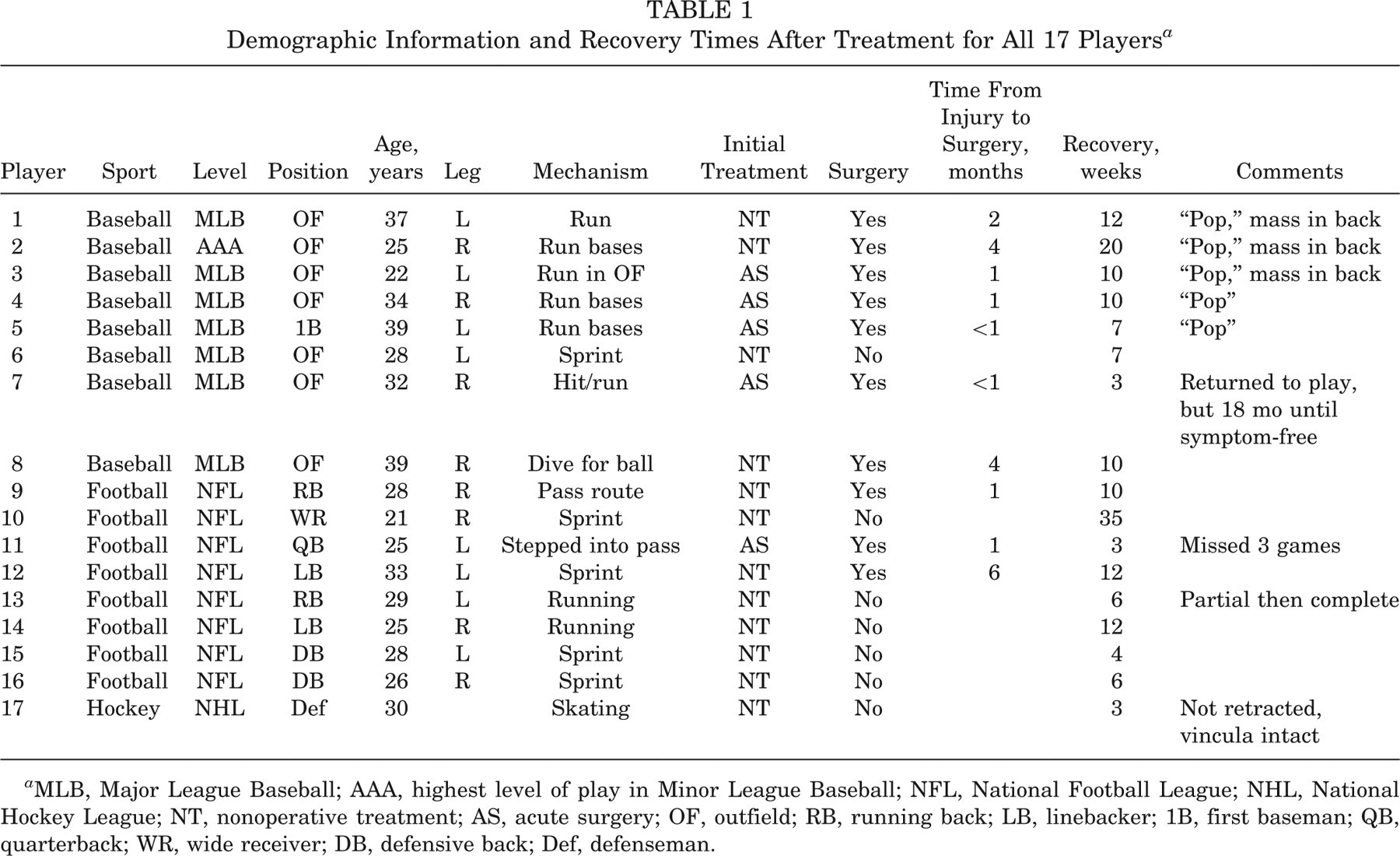
MLB, Major League Baseball; AAA, highest level of play in Minor League Baseball; NFL, National Football League; NHL, National Hockey League; NT, nonoperative treatment; AS, acute surgery; OF, outfield; RB, running back; LB, linebacker; 1B, first baseman; QB, quarterback; WR, wide receiver; DB, defensive back; Def, defenseman.
Clinical Findings
The history given by the majority of players was that they felt a “pop” or sharp, searing, acute pain, usually occurring during sprinting or an extended stride. Only 15% had any prior pain or minor injury predating the rupture. Almost all began limping immediately after the injury. Ninety percent had pain and difficulty with full knee extension, and some were unable to walk effectively without crutches.
Examination demonstrated tenderness only or a tender mass in the medial aspect of the popliteal region, swelling, and commonly ecchymosis. Knee flexion was consistently weak, and there was even occasional puckering of the popliteal skin with hamstring muscle contraction in chronic cases.
Magnetic Resonance Imaging Findings
In acute cases, MRI demonstrated edema, semitendinosus tendon retraction, and decreased muscle volume on axial images (Figure 1). Chronic cases demonstrated similar findings, as well as occasional presentation of severe fibrosis on axial images, creating a ringing effect around the tendon similar to growth rings in the trunk of a tree (Figure 2).
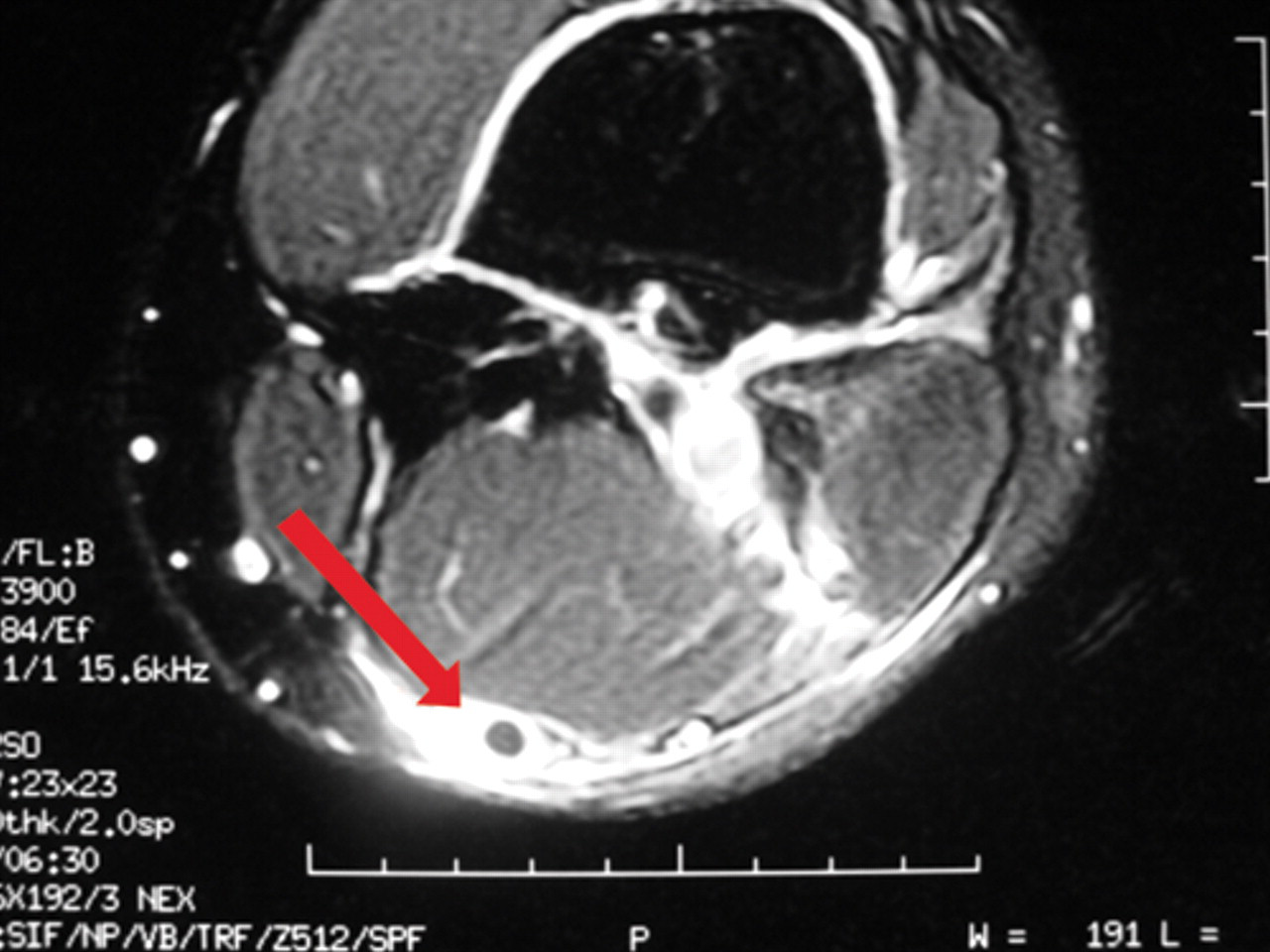
Magnetic resonance axial image of acute semitendinosus distal tendon (arrow) avulsion. Note surrounding edema and lack of tendon diameter hypertrophy. The void left by the retracted volume of muscle belly is fluid filled.
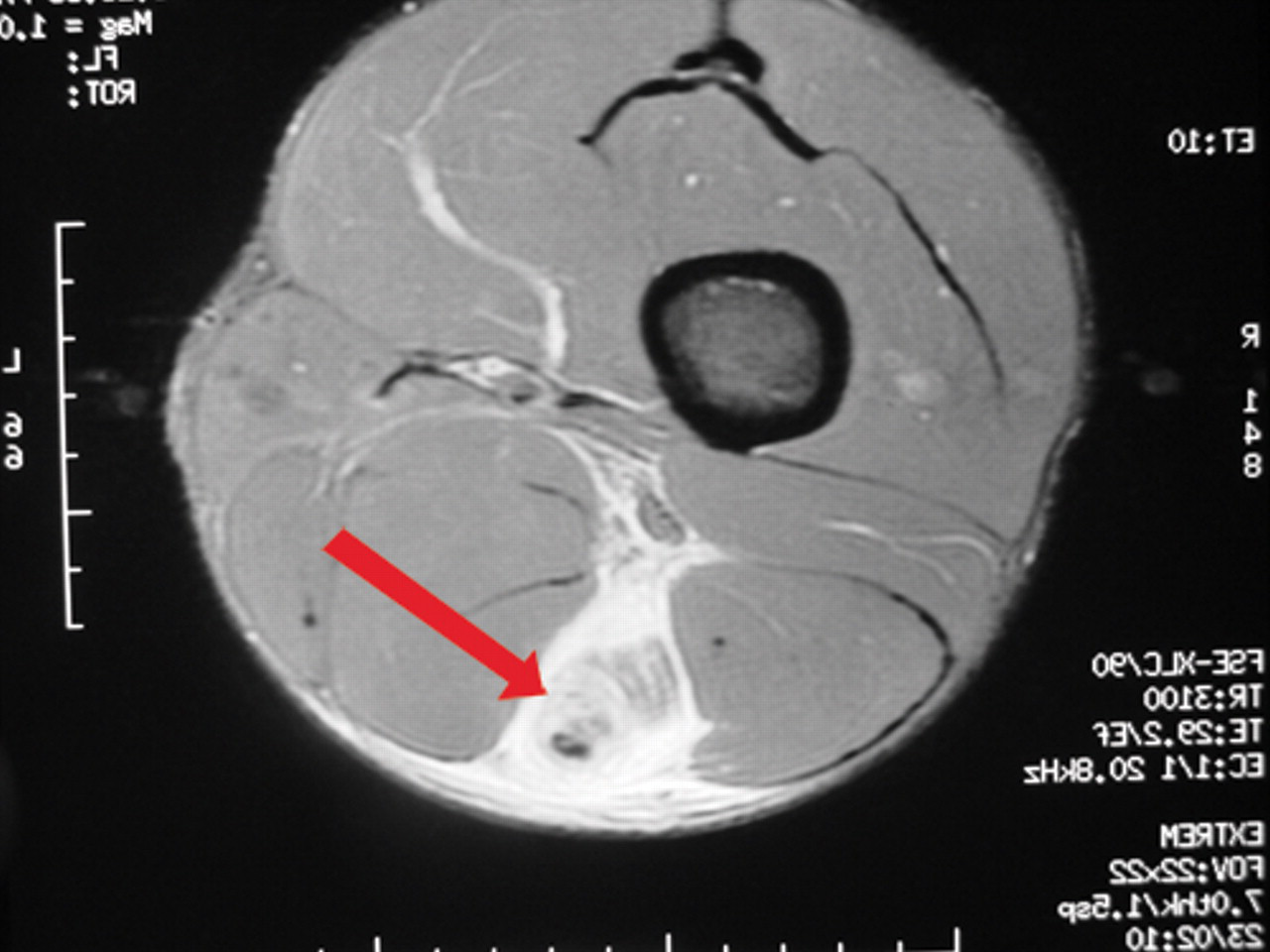
Magnetic resonance axial image of chronic distal semitendinosus tendon (arrow) avulsion. Note the edema and fibrosis surrounding the tendon, like growth rings of a tree.
Treatment
For the purposes of retrospective review, we evaluated the experience with both nonoperative treatment and surgical treatment, with particular concern regarding the time frame for return to play after this injury in professional sports. Early in the study period, all players were treated nonoperatively with the expectation that a full recovery would follow. Twelve players had initial nonoperative treatment (NT) and later in the study period, 5 players had surgery early during the acute injury phase (acute surgery [AS]). Acute surgery was defined as surgery within the first 4 weeks after injury.
Nonoperative treatment included rest and use of crutches as needed until independent. This included treatment modalities, rehabilitation, and progression to running, sprinting, and sport/position-specific drills. Strength training was always with isotonic resistance, and in some cases progressing to isokinetic resistance. We used an isotonic resistance assessment as the measure of strength, compared with the normal uninjured leg. Isokinetic strengthening was variably used for rehabilitation purposes, but not for maximal strength assessment at the time of return to play or follow-up. No athlete was allowed to return to participation until recovery of 80% strength as compared with the uninjured thigh (3 sets or 12 isotonic repetitions), in addition to completion of a graduated functional position-specific rehabilitation program.
Surgical treatment was used for those in the NT group who failed nonoperative treatment and for the 5 acute cases. Failure of nonoperative treatment was defined by 1 of the following: no substantial improvement in hamstring muscle weakness or pain over a 6-week period, intractable pain on sprinting, or persistence of scarring in the distal medial thigh that did not improve with soft tissue rehabilitation techniques. Mixed results of nonoperative treatment in our early experience led us to consider whether surgery in the acute stage of injury might speed recovery. Because there was no literature to rely on, we needed to consider surgical repair versus resection of the retracted torn tendon. We chose to investigate resection of the torn tendon because of the generally known favorable outcomes after harvesting medial hamstring tendons for ligament reconstruction. The procedure was performed through an oblique incision on the posteromedial knee parallel to the course of the distal semitendinosus tendon. In some cases, 2 small incisions were made—1 over the distal hamstring tendons inferior to the medial joint line of the knee, and 1 proximally at the level of the distal musculotendinous junction of the semitendinosus, which is approximately 15 cm proximal to the popliteal crease. In all surgical cases, the distal tendon of the semitendinosus was completely resected using scissors or sharp dissection (Figure 3). All inflamed or fibrotic peritenon was resected, and all adhesions were released. Even in acute cases, we found the tendon to be too hypertrophied to resect with the usual size tendon harvesters used in knee ligament surgery. We never attempted surgical repair of the tendon, based on the knowledge that it can be harvested without adverse effect and the fear that repair might greatly prolong recovery, thus leading to pain, scarring, or both.
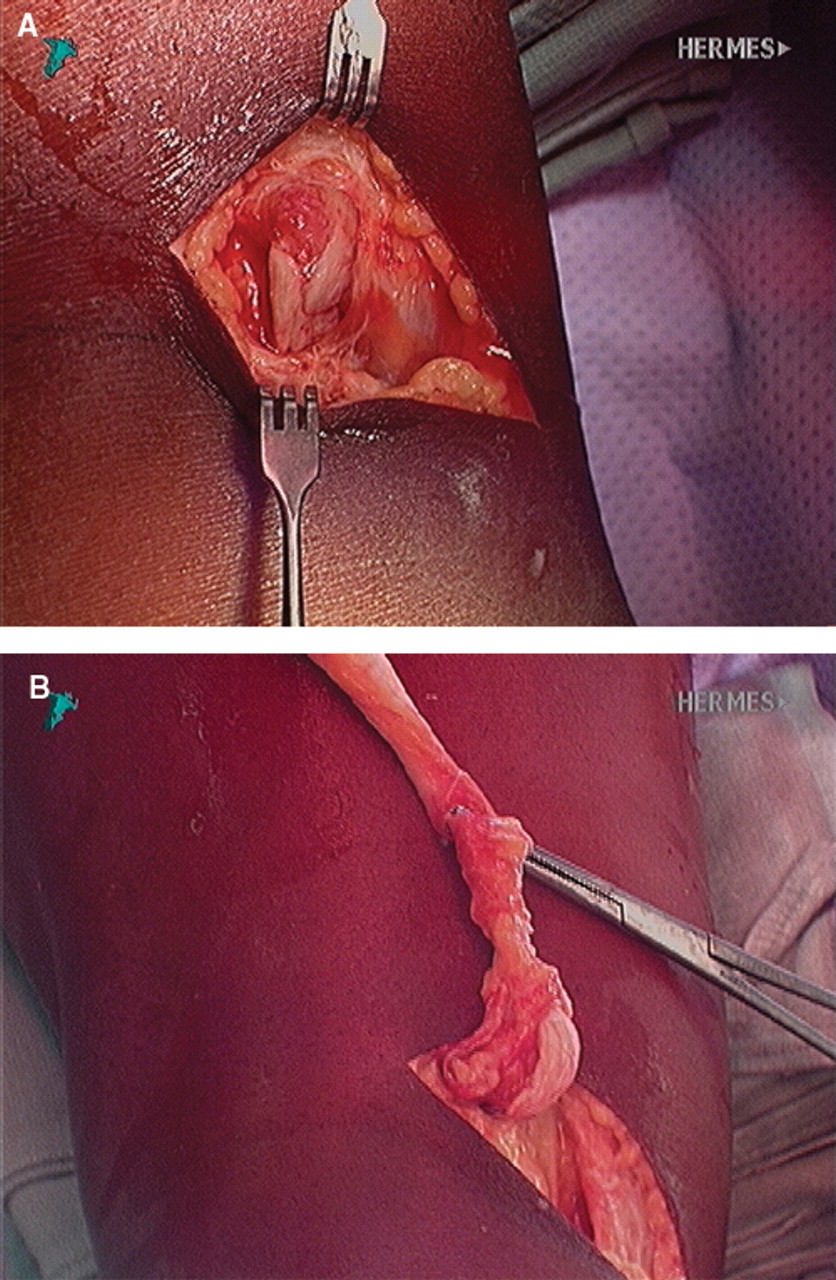
Surgical exploration of torn distal semitendinosus tendon in a professional athlete. The orientation is the posterior view of the left popliteal incision (proximal is top). A, balled-up retracted tendon (arrow) creating a mass directly posterior to the semimembranosus tendon. B, same view demonstrating the proximal reflection of the tendon (arrow) after delivering it through the incision.
Follow-up
All 17 players were followed for an average of 13 months (range, 4-55). Return to play at the preinjury level without a significant reinjury was a key element in determining the time of recovery. For those athletes whose sport was not in season, we used clearance to play in the same manner. Follow-up examination was performed at the time of clearance to play or return to play. Range of motion deficit and tenderness were assessed. “Recovery” from the injury was measured from the date of injury and was defined as requiring all of the following: (1) return of >80% isotonic knee flexion strength as compared with the normal opposite leg, (2) no pain when sprinting, (3) having progressed through a sport-specific functional rehabilitation program, and (4) being cleared to play at the preinjury level of professional or amateur competition. Further time lost due to the same injury was also reported.
Statistics
A confidence level of 95% was used to determine statistical significance of difference between the 2 groups. One-way analysis of variance was used to compare the NT group time to recovery to the AS time to recovery.
Results
The study group was divided into those players receiving initial NT and those receiving initial surgical treatment within the first 4 weeks of injury (AS) (Table 1). For those players who had initial NT, the injury, pain, and swelling often demonstrated initial improvement in response to treatment modalities and rest. There was often improvement of clinical symptoms over the first 2 to 3 weeks, and some continued to improve to full recovery. However, some players had difficulty progressing with advanced functional and sport-specific rehabilitation, and developed chronic pain and hamstring weakness during functional activities and weight training. These players failed to continue to improve and some even regressed.
Nonoperative Treatment Group
Twelve players were treated with initial NT. Seven of those 12 recovered at an average of 10.4 weeks (range, 3-35). Five players (42%) failed NT, averaging 16.8 weeks (range, 4-40) and subsequently had surgery. Those 5 cases recovered at an average of 12.8 weeks (range, 10-20) postoperatively. Therefore, total time to recovery in this subset (42%) of the NT group was 29.6 weeks (range, 14-52) (Table 1). As a whole, the 12 players in the NT group recovered in an average of 18.4 weeks (±15.7).
Acute Surgery Group
Five players underwent surgery within the first 4 weeks after injury. These 5 players recovered at an average of 6.8 weeks (±3.2) postoperatively.
In the AS group, we found that peritendinous edema and seroma formation was quite impressive. Additionally, there was a stricture between the semimembranosus tendon and the popliteal fascia where this avulsed retracted tendon tended to be tethered and create a tender mass in the medial aspect of the popliteal fossa. We found that these injuries were complete tears, either at the distal insertional aspect of the pes anserine tendon or somewhere along the medial aspect of the knee near the insertion.
Final examination at follow-up showed full and symmetrical knee range of motion, and little or no tenderness in all 17 players. At midrange follow-up averaging 13 months (range, 4-55 months), there was no difference between groups once recovery was achieved, and loss of hamstring flexibility was not evident after full recovery. The data do not support conclusions regarding long-term outcome comparisons for these 2 treatment approaches. In comparing the 2 treatment groups as a whole, average recovery for all players in the AS group was 6.8 weeks (±3.2) and for the NT group it was 18.4 weeks (±15.7). There was no statistically significant difference in recovery time between the 2 groups (P = .128). However, the trend was for quicker recovery in the AS group.
Discussion
During the study period, there was no article in the English-language literature related to this diagnosis or its treatment. Therefore, we used clinical judgment alone in treating these injuries. It became evident that this was a problematic injury in professional sports, and players were advised of this. As the series mounted, it became evident that surgical treatment was an option that did, in certain cases, offer a relatively quick recovery and return to full participation at their prior level. Surgery was successful in early cases of failed NT, and was later successful in acute cases. Therefore, this review was undertaken to study the results of the 2 treatment approaches and report our collective experience.
Subsequent to the study period, Schilders et al 7 presented a case report of “partial rupture of the distal semitendinosus tendon treated by tenotomy.” They described, “…a new clinical entity: partial rupture of the distal semitendinosus tendon; which has failed to settle with conservative treatment; and has been successfully treated by tenotomy.” Sekhon and Anderson 8 recently reported NT of this injury in 2 professional athletes as a case report lacking long-term follow-up.
Our report is the first reported case series of complete distal rupture of the semitendinosus tendon. We analyzed both nonoperative and surgical treatment, and have tried to determine appropriate treatment guidelines for sports medicine physicians. We did find a frustratingly high incidence of failed NT (42%). Our study methods do not allow conclusions regarding the long-term outcome of treatment methods.
We believe that distal rupture of the semitendinosus probably is an uncommon injury. However, we do not believe it is rare, and have identified 25 such cases. It is likely that this injury has been clinically misdiagnosed as a distal-third muscle-belly hamstring injury without adequate MRI. To adequately make this diagnosis, it is imperative to obtain MRI of the thigh and knee, so that the full course of the semitendinosus tendon is visualized.
This injury occurred in adult elite-level athletes (20-35 years of age) in our series, and we have not identified this injury in high school or recreational athletes. We did identify 4 elite-level collegiate athletes and 1 other elite amateur with this diagnosis, but they were not participants in our study.
It has been our experience that distal semitendinosus tendon avulsion injuries cause much more time loss from sports than hamstring muscle-belly injury on average. Additionally, 42% of these injuries fail initial NT and ultimately undergo surgery, in our experience. The recovery may be prolonged, but generally this is not a career-ending injury.
We had difficulty identifying factors that would predict who would do well with NT, and who would fail NT. Therefore, it is difficult to know which players will do well without surgery, and which players will struggle. The group having AS recovered more quickly than the group having delayed surgery after initial NT. On the basis of our clinical experience with this entity, we lean toward recommending AS in the elite-level athlete for whom time to recovery is very important. That opinion is primarily related to what seems to be a more favorable time frame to return to participation. We certainly would modify that if the player seems to be doing quite well, walking normally, and progressing well with a nonoperative rehabilitation program. Clinical judgment should prevail in this setting. If there is a painful mass, inability to walk well with normal gait pattern, or inability to extend the knee fully, then the recommendation for early surgery is an easier determination. Regardless of the treatment, this injury can be frustrating for the athlete and clinician because of its unpredictable nature and prolonged recovery.
A strength of this study is that it identifies this injury as a cause of significant time loss from participation in professional sports, and more than would be expected of hamstring muscle-belly injuries. We report experience with surgical and NT with results regarding timing of return to play for both treatments. This information is new to the literature. Weaknesses of this initial Level 4 case series include a lack of 2-year follow-up, lack of maximal isokinetic testing at final follow-up, and lack of statistical significance and adequate power to make firm recommendations based on the data. Selection bias can be present in such a case series, and perhaps that is true in our series. It was not our objective to attempt to prove a hypothesis, but rather to make observations and increase awareness. A new awareness of the injury and its response to treatment, and our experience returning these athletes to the field of competition, may aid other team physicians in the management of such injuries. There is a need for a heightened awareness of this clinical diagnosis in elite-level athletes. Further study of treatment options will improve the management of these injuries in all athletes.
Footnotes
Presented at the 33rd annual meeting of the AOSSM, Calgary, Alberta, Canada, July 2007.
The authors declared that they had no conflicts of interests in their authorship and publication of this contribution.