
Abstract
Snowboarding injuries examined at Sumi Memorial Hospital have increased in number from 1999 to 2000 because of the increased popularity of this sport after its broadcast at the 1998 Winter Games in Nagano, Japan. 6,11-13 Since 2000, more than 1500 patients who sustained snowboarding injuries have attended Sumi Memorial Hospital. Several characteristics of snowboarding-related injuries have been shown. First, the common causes of injury include falling and jumping failure. Second, upper extremities are commonly injured. Third, beginner snowboarders are at a high risk of these injuries. 1-5,10,12,13 Idzikowski et al 7 reported that upper extremity injuries accounted for 49.0% of total snowboarding injuries, 7430 between 1988 and 1998, and that falling is the predominant mechanism of these injuries. Matsumoto et al 8 showed that the most common location of snowboarding-related injury was the upper extremity (40% of all snowboarding injuries; n, 7051) and that falls accounted for 60% of the 2706 injuries that occurred between 1995 and 2000.
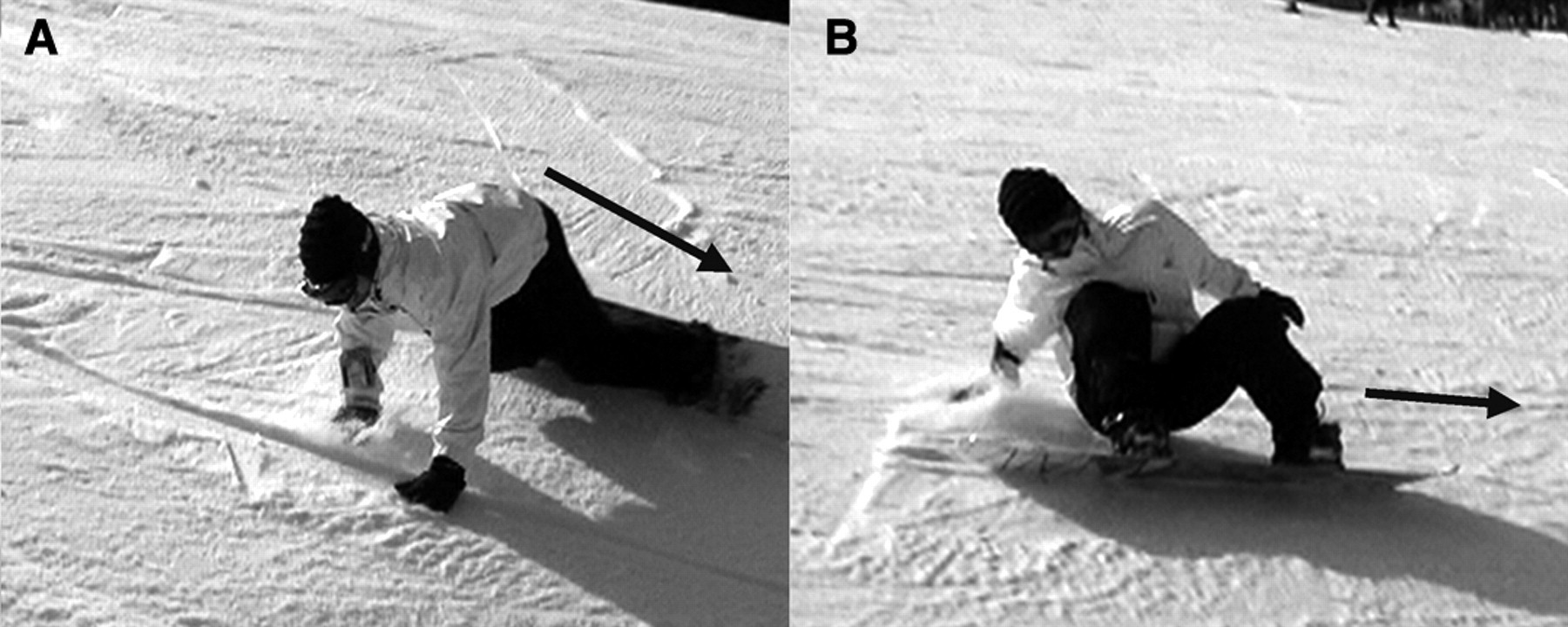
Regarding snowboarding-related upper extremity injuries, several reports on wrist fractures are available. A majority of the wrist fractures were sustained during a backward fall and occurred on the opposite side of the sliding direction. 5,9 There are 2 snowboarding stances: regular and goofy 8,11 (Figure 1). A snowboarder in the regular stance directs his or her left leg in the sliding direction, whereas the one in the goofy stance directs his or her right leg in the sliding direction; that is, the left side of the body in the regular stance and the right side in the goofy stance are oriented in the sliding direction. Commonly, right-handed snowboarders choose the regular stance. There are 2 falling directions in snowboarding: a forward fall and a backward fall (Figure 2). Briefly, 2 edges of a snowboard play an important role in sliding, the front and back edges. Specifically, there are 2 turn waves during snowboard sliding: the front turn and the back turn. In the former, snowboarders must use the front edge of the snowboard and in the latter, they must use the back edge. The contact of the edge with the snow makes it possible for the board to slide and turn smoothly. However, an edge can occasionally be the cause of a fall if it is caught in the snow (Figure 2).

Two snowboarding stances: A, in regular stance, a snowboarder directs his or her left leg toward the sliding direction; B, in goofy stance, the snowboarder directs his or her right leg toward the sliding direction. Black arrows indicate sliding directions.
Two falling directions in regular stance: A, a snowboarder falls forward when the front edge is caught by the snow, as a consequence of moving the body weight from heel to toe during sliding or turning; B, a snowboarder falls backward when the back edge is caught by the snow, as a consequence of moving the body weight from toe to heel during sliding or turning.
Although snowboarding activity has been classified according to 2 stances and 2 falling directions, the precise associations among upper extremity injuries, stances, and falling directions remain unknown. This fact motivated us to perform the present study. Given the preceding information, we hypothesized that some significant patterns should be shown in the prevalence of snowboarding-related upper extremity injuries in relation to the stances or directions at the time of fall. Therefore, the purpose of the present study was to elucidate how the locations and sides of upper extremity injuries vary depending on the snowboarding stance and the direction of the fall.
Materials and Methods
Patients
For this study, 1918 patients were chosen who sustained upper extremity injuries owing to falls during snowboarding/ sliding and who were treated at Sumi Memorial Hospital (Okumino, Gifu, Japan) from 2000 to 2008. Injuries from jumps, the half-pipe, and collisions with another person or a stationary object were excluded from data analysis. In the present study, inclusion criteria were as follows: injury to the upper extremity comprising fractures or dislocations of the wrist (including those of scaphoid and lunate), forearm, elbow, upper arm, shoulder, clavicle, and acromioclavicular joint. Exclusion criteria were (1) contusions, sprains, lacerations, and abrasion without fractures or dislocations as judged by radiographs of the upper extremity (fingers, including the carpometacarpal joint of the thumb; wrist, including scaphoid and lunate; forearm; elbow; upper arm; shoulder; acromion; clavicle; and the acromioclavicular joint) and (2) fractures or dislocations of the fingers, including the carpometacarpal joint of the thumb and metacarpals, wrist (except scaphoid and lunate), the scapula, and the sternoclavicular joint. Sumi Memorial Hospital serves as a primary emergency center for more than 10 skiing facilities in the Okumino area of Gifu, Japan. Because there are no other emergency hospitals in this area, almost all the snowboarders who are injured come to this hospital, thus giving us an advantage in terms of data validity.
Evaluations
We first established and analyzed these cases and then classified them according to various factors obtained from the medical records. On each visit of the injured snowboarders, detailed information on snowboarding, the complaints, and the symptoms was acquired with a questionnaire created by Hiroshi Sumi in 1988. The questionnaire evaluated 8 variables (see below). Responding to the questionnaire with the help of friends and relatives was mandatory before seeing the attending physician; hence, data collection was 100%, which is why the present study is prospective. The number of snowboarders who visited the snowboarding area was calculated as follows to analyze the overall incidence of upper extremity injuries caused by falling during snowboarding: The number of snowboarders was estimated from admission registrations by counting the number of individually issued snowboarding passes at each facility.
Sex and age of patients
Sex and age were examined from the medical records.
Skill level
Skill level was assigned by self-declaration into1 of the 3 categories: beginner, intermediate, and expert.
Snowboarding instructions
Patients were asked from whom they had received snowboarding instructions. The answer was assigned by self-declaration into 1 of the following 3 levels: instruction received from a licensed instructor, instruction received from a friend (an unlicensed person), and no instruction received. Moreover, we investigated for a significant difference in the prevalence of receiving snowboarding instruction among the 3 skill levels.
Sliding stances
Two sliding stances were studied (regular and goofy) in the injured snowboarders at the time of their falling.
Location of upper extremity injuries with each stance
Anteroposterior and lateral radiographs were obtained in all cases. Physicians who initially examined these injured patients filled out the survey concerning the diagnoses. We subsequently confirmed the diagnoses. We then classified the location of each injury—clavicle fracture, acromioclavicular joint dislocation, shoulder dislocation, upper arm fracture, elbow fracture or dislocation, forearm fracture, or wrist fracture—according to whether it resulted during a fall in the regular or goofy stance.
Right- or left-side injuries with each stance
The side of the upper extremity injuries, right or left, was classified according to whether it resulted during a fall while in the regular or the goofy stance.
Falling direction
The direction of the fall was classified into 2 groups, forward and backward. In each type of injury (eg, wrist fracture, upper arm fracture, shoulder dislocation, and elbow dislocation), the direction of the fall was assessed.
Right- or left-side injuries in relation to the direction of the fall
The side of the upper extremity injuries, right or left, was classified according to the direction of the fall and relative to the type of injury that occurred (eg, wrist fracture, upper arm fracture, shoulder dislocation, and elbow dislocation).
Statistical Method
We used a contingency analysis (Aspin-Welch t test) to compare the 2 stances or the 2 falling directions relative to the type of injuries that occurred. A P value of < .05 was considered statistically significant.
Results
During this period, about 10.8 million snowboarders visited the Okumino area, and 16 564 patients who sustained snowboarding injuries received primary treatment in Sumi Memorial Hospital. Among these cases, 1918 patients (1.12%) had upper extremity injuries per the inclusion criteria, as caused by falls without jumps or collisions (see Table 1). The overall incidence of upper extremity injuries per the inclusion criteria was 0.19 per 10 000 snowboarder visits.
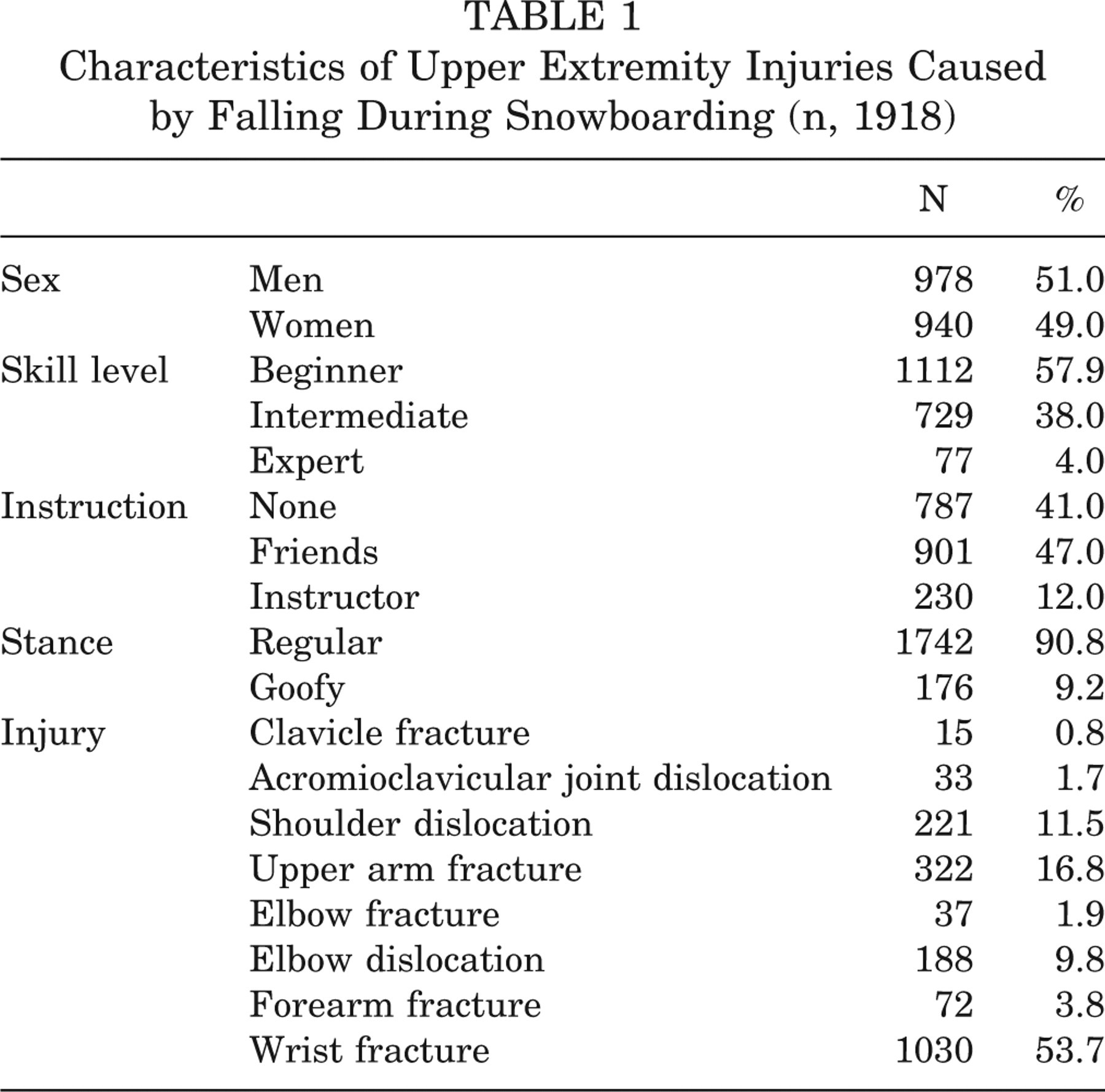
Characteristics of Upper Extremity Injuries Caused by Falling During Snowboarding (n, 1918)
Sex and Age of Patients
The study group comprised 978 men (51.0%) and 940 women (49.0%). The age of the patients was 23.8 ± 4.9 years (range, 5 to 49 years).
Skill Level
The skill level was identified as beginner in 1112 patients (57.9%), intermediate in 729 patients (38.0%), and expert in 77 (4.0%).
Snowboarding Instruction
In sum, 901 patients (47.0%) had been given snowboarding lessons by a friend who was not licensed as an instructor; 787 (41.0%) had received no instruction; and 230 (12.0%) had received instructions from a licensed instructor. Moreover, there was no significant difference in the prevalence of receiving snowboarding instructions among the 3 skill levels. Only 11.0% of beginners, 12.1% of intermediates, and 17.3% of experts had received instructions from a licensed instructor.
Sliding Stances
We found that 1742 injuries (90.8%) occurred when the snowboarder assumed a regular stance and 176 (9.2%) occurred in the goofy stance.
Location of Upper Extremity Injuries With Each Stance
In the regular stance, 52.7% of the injuries were wrist fractures, 17.4% were upper arm fractures, 11.4% were shoulder dislocations, and 10.2% were elbow dislocations. In the goofy stance, 63.6% of the injuries were wrist fractures, 10.8% were upper arm fractures, 11.9% were shoulder dislocations, and 5.7% were elbow dislocations. No significant difference was observed in the prevalence of upper extremity injuries between the regular and goofy stances (see Table 2).
Distribution and the Side of Various Upper Extremity Injuries in Regular and Goofy Stances a
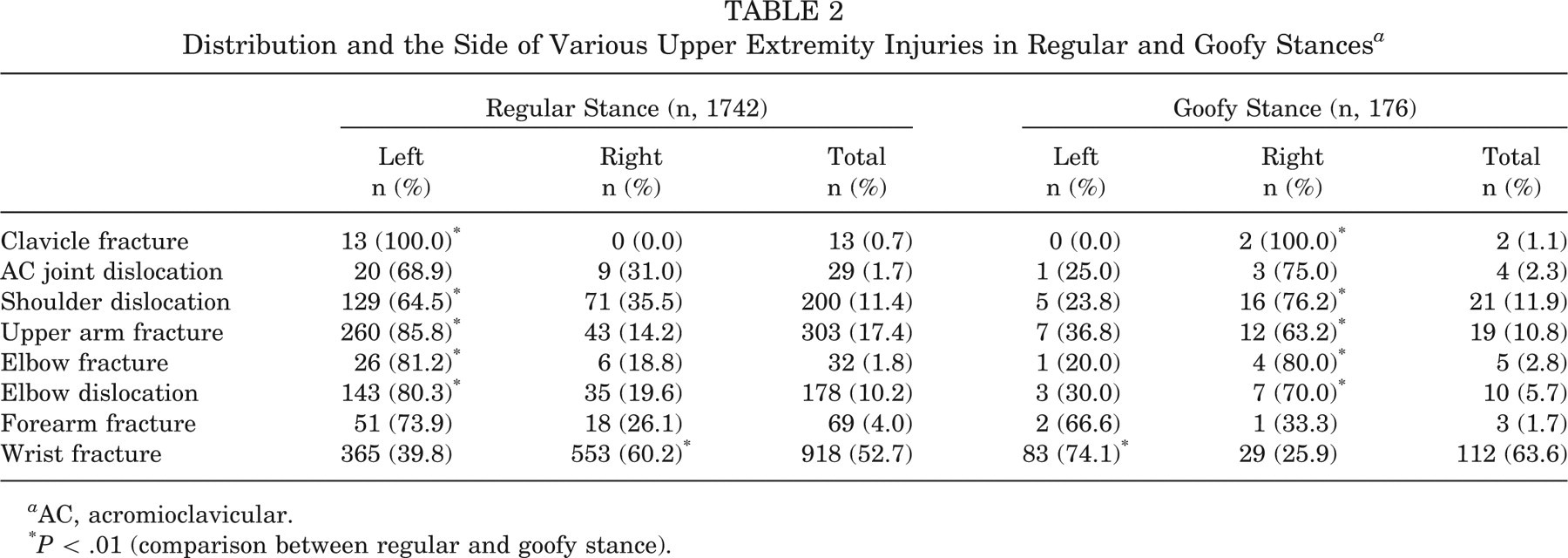
AC, acromioclavicular.
P < .01 (comparison between regular and goofy stance).
Right- or Left-Side Injuries With Each Stance
In the regular stance, 60.2% of wrist fractures occurred on the right side (P < .01), and 64.5% of shoulder dislocations, 100.0% of clavicle fractures, 85.8% of upper arm fractures, 81.2% of elbow fractures, and 80.3% of elbow dislocations occurred on the left side (P < .01). In contrast, in the goofy stance, 74.1% of wrist fractures occurred on the left side (P < .01), and 76.2% of shoulder dislocations, 63.2% of upper arm fractures, 80.0% of elbow fractures and 70.0% of elbow dislocations occurred on the right side (P < .01). It was shown that irrespective of the 2 stances, 61.7% of wrist fractures occurred on the side opposite to the sliding direction, whereas 65.6% of shoulder dislocations, 82.9% of upper arm fractures, 80.1% of elbow fractures, and 79.8% of elbow dislocations occurred on the same side as the sliding direction.
Falling Directions
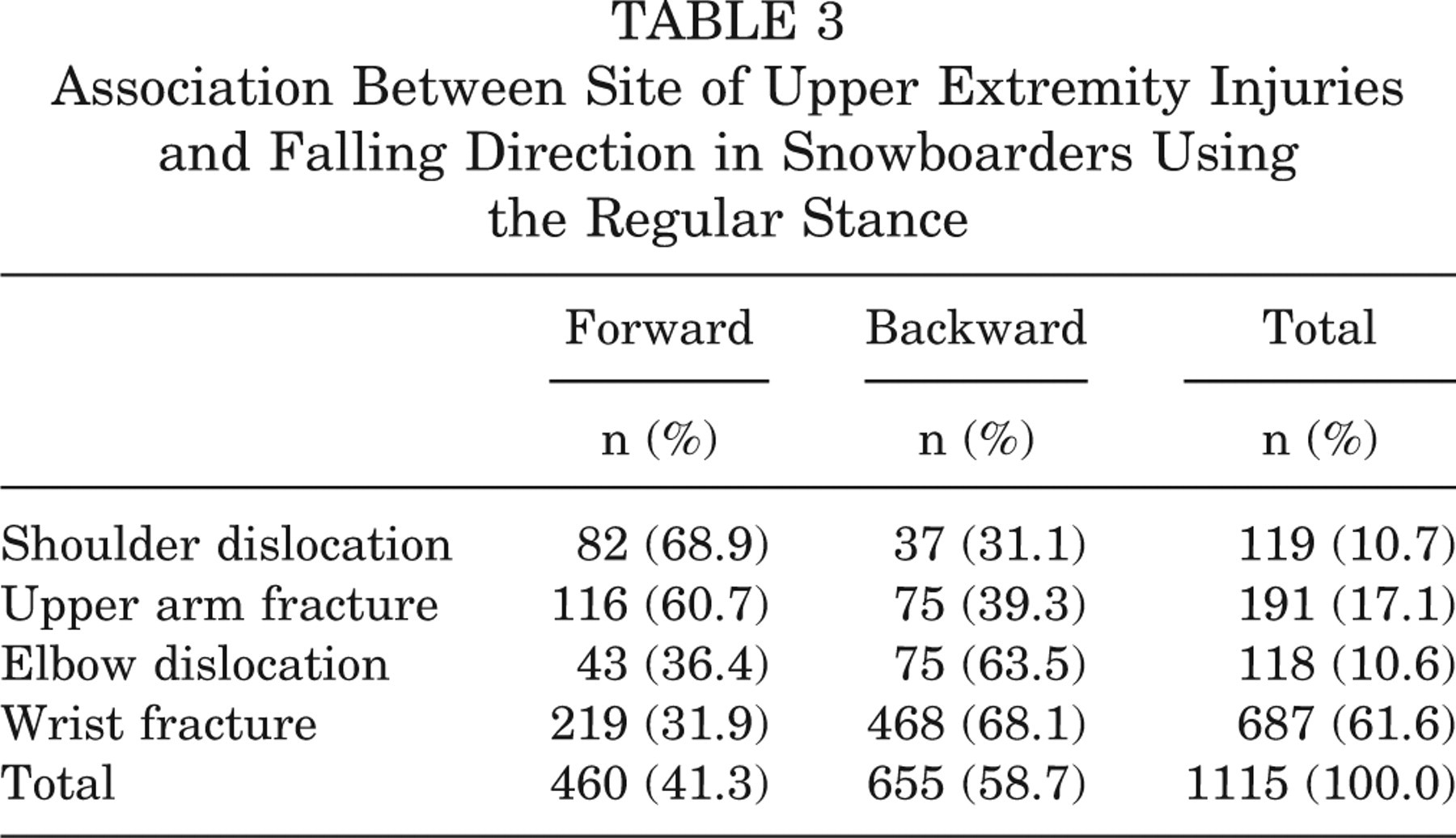
In snowboarders who used the regular stance (n, 1742), 68.9% of shoulder dislocations and 60.7% of upper arm fractures occurred when the snowboarders fell forward, whereas 63.5% of elbow dislocations and 68.1% of wrist fractures occurred when they fell backward (Table 3).
Association Between Site of Upper Extremity Injuries and Falling Direction in Snowboarders Using the Regular Stance
Right- or Left-Side Injuries in Relation to the Direction of the Fall
In snowboarders who used the regular stance (n, 1742), the frequency of shoulder dislocations was significantly higher on the left side (the sliding direction) than on the right side when caused by falling forward, whereas no specific tendency in the side of injury was observed because of a backward fall (P < .01). Most upper arm fractures and elbow dislocations occurred on the left side in both forward and backward falls. However, more than half the wrist fractures occurred on the right in both forward and backward falls (Table 4).
Association Among 2 Falling Directions and 2 Injured Sides in Regular Stance (n, 1115)
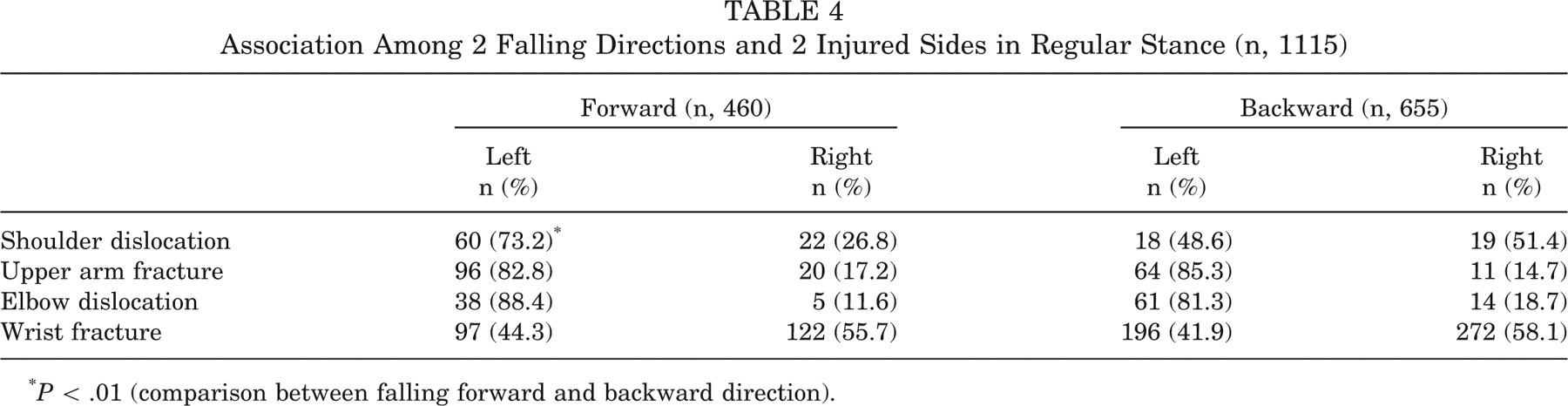
P < .01 (comparison between falling forward and backward direction).
Discussion
This is the first time that several significant associations have been reported between the site and side of snowboarding-related upper extremity injury and the stance and direction at the time of fall. First, irrespective of the 2 stances and the side of the body, most wrist fractures occurred on the side opposite the sliding direction. Yet most shoulder dislocations, upper arm fractures, elbow fractures, and elbow dislocations occurred on the same side as the sliding direction. Second, shoulder dislocation and upper arm fracture were caused by falling forward, whereas elbow dislocation and wrist fracture were caused by falling backward. Third, shoulder dislocation occurred significantly more often on the sliding side when falling forward than falling backward. However, in upper arm fracture, elbow dislocation, and wrist fracture, no significant difference was noted in relation to the direction of the fall; that is, upper arm fracture and elbow dislocation occurred on the sliding side, and wrist fractures occurred on the opposite side of the sliding direction in both forward and backward falls. As such, we recognize that it is important to understand snowboarding-related upper extremity injuries according to whether they occur on the left or right and whether they occur on the same side or the opposite side of the sliding direction. Future studies should therefore compare injuries between the anterior aspect of the upper extremity to the posterior aspect of the upper extremity in relation to fall direction irrespective of the stances (regular and goofy).
Several similarities exist between the present results and those of previous studies regarding wrist fractures. First, Davidson and Laliotis 5 have already suggested falling backward as the main onset of injury. Second, Matsumoto et al 9 have noted the dominant injured side being the opposite side of the sliding direction. However, the present results—specifically, the injury pattern in shoulder dislocation, upper arm fracture, and elbow dislocations in relation to sliding direction and falling direction—have not been described.
To understand the present results on snowboarding-related upper limb injuries, we first need to understand the behavior of the snowboarders from the moment they lose postural control until they hit the snowy ground. They consistently and instinctively thrust their upper extremity toward the ground in response to the sensation of falling (Figure 2). From the viewpoint of snowboarding safety, this behavior is dangerous. As such, the palm contacts the ground first, with the elbow extended. Taking into account the difference in mechanism between the front turn and the back turn, we speculate that 2 movements during front and back turns, at the time of fall, result in axial loading variations and, thus, different injuries. That is, when one falls in a forward direction with the shoulder abducted and externally rotated (Figure 2A), it applies axial loading to the proximal part of the humerus, consequently leading to proximal humeral fracture and shoulder dislocation. When one falls backward (Figure 2B), it applies axial loading to the wrist and hyperextension moment to the elbow joint, consequently leading to wrist fractures and posterior elbow dislocation. Taking into account the positions at which their hands come in contact with the snow/ground at the time of fall, we speculate that the snowboarders’ body control against multidirectional falls may be essential to prevent upper extremity injuries.
Then, what type of body control is required by snowboarders? We suggest 2 falling techniques: baseball head sliding and judo ukemi (see video supplement, available at http://ajs.sagepub.com/supplemental/). In general, licensed snowboarding instructors teach falling techniques that simulate head sliding in baseball and ukemi in judo, as recommended by the Japanese Snowboarding Association since 1982. First, to prevent upper extremity injuries, snowboarders need to absorb and radiate the traumatic energy of hitting the ground as much as possible through areas of the trunk, buttocks, and lower extremities—and not through the upper limbs. This maneuver decreases not only upper extremity injuries but also head and face injuries. In fact, body control such as that used in baseball when sliding head first is recommended when one falls forward. In contrast, when one falls in a backward direction, body control like that used in judo ukemi is preferable. Ukemi is a special technique in judo. It is carried out when players fall on the ground so that they can protect themselves from injury. In ukemi, when players lose their body balance and fall, they hit the ground with the whole dorsal side of both upper limbs and the torso with a backward jump. Consequently, the players fall on the ground gracefully.
Although licensed snowboarding instructors widely teach falling techniques that simulate baseball head sliding and judo ukemi, experienced baseball and judo players might acquire those techniques through continual discipline. However, the present study shows that most injured snowboarders did not receive instructions from a licensed instructor. Therefore, inexperienced snowboarders should not only receive instruction but also be well trained in these body control maneuvers.
The design of the present study has several limitations. First, only injured patients were analyzed at primary care prospectively. Therefore, more clinically relevant data would derive from information about uninjured snowboarders and from comparative study of those who were injured during snowboarding and those who were not. Second, patients were excluded when they had fracture and dislocation on fingers as well as upper extremity contusion. Information about the number of patients classified by exclusion criteria may provide more relevant data. Third, we did not collect data regarding the duration of stay of snowboarders, which would have provided us with a rough estimate of the risk. Fourth, a bypass effect of the injured population should be taken into account. Injured snowboarders may have traveled away from the ski area. Therefore, all injuries may not have been registered within the ski area or in the local hospitals, which can consequently lead to bias. Fifth, the number of snowboarders who visited the snowboarding area was calculated, but this number was not completely accurate. Sixth, this study was based on information obtained from questionnaires that depended on self-declaration. Moreover, some of the snowboarders sustained upper extremity injuries with complicated head contusions that could have stopped them from answering the questionnaire because of the accompanied memory loss, which could have caused bias. Seventh, this survey studied the stance at the time of fall. However, we need to know whether the stance usually adopted during sliding is identical to the stance at the time of fall. Therefore, we should add this question to our questionnaire and survey it in the future. Eighth, there were fewer patients with a goofy stance than a regular stance, so we concluded that statistical analysis could not be applied for those with a goofy stance—particularly in fall directions and right- or left-side injuries in relation to fall direction. We should therefore analyze and evaluate these classifications in the future. Ninth, the 2 behaviors of snowboarders during falls in Figure 2 do not result in fractures and dislocations; as such, we cannot speculate on whether these motions necessarily lead to upper extremity injuries.
Conclusion
We have described the characteristic features of snowboarding-sustained upper extremity injuries caused by falling. The injured side in the regular and goofy stance is reversed. Shoulder dislocation and upper arm fracture are related to the mechanism of falling forward, whereas elbow dislocation and wrist fracture are related to the mechanism of falling backward. Finally, we suggest how injuries could be prevented from a clinician’s point of view.
Footnotes
The authors declared that they had no conflicts of interests in their authorship and publication of this contribution.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.