
Abstract
Meniscal tears can be treated with total or partial meniscectomy. However, several authors have proved that these 2 treatments often lead to accelerated deteriorative effects on the articular cartilage. 3,6,21 Therefore, meniscal repair has become a well-accepted method to prevent articular degeneration in recent years.5,20 Tears can be mainly repaired with sutures and all-inside suture devices. 7,8
Evaluation of the meniscal healing status after repair is important for the surgeon to inform the patients whether they can increase their activities or return to sports.11 The long-established evaluation method for repaired meniscus generally depends on clinical assessment, including symptoms and physical signs.4 Because of the surgeon’s subjectivity, this method hardly gives an objective or accurate evaluation and tends to lead to a false-positive or false-negative diagnosis. Other more objective methods such as arthrography or second-look arthroscopy are invasive; therefore MRI has been proposed as a better alternative to evaluate the repaired meniscus. 1,16 However, MRI is less reliable in postoperative evaluation of meniscal repair, as the scar at the repaired site always expresses a grade 3 signal that was seen as evidence of an unhealed meniscus. 23,24,28
Although several authors have pointed out the limitation of MRI, few studies have applied second-look arthroscopy as a gold standard for each consecutive case to evaluate the MRI diagnostic value. Meanwhile, none of the previous studies compared the diagnostic accuracy of second-look arthroscopy, clinical assessment, and MRI. This study not only applied the above 3 different methods for every involved case, but we also used 5 different MRI sequences to improve the MRI diagnostic value. The purpose of this study was to make a conclusive comparison and to propose some suggestions for evaluating meniscal healing status. On the basis of our observation, we hypothesized that second-look arthroscopy was the only method that could evaluate the repaired meniscus comprehensively and accurately, and MRI value could be improved when combined sequences were applied.
Materials and Methods
Patients and Inclusion Criteria
Ninety-one patients underwent arthroscopic meniscal repairs consecutively between July 2005 and June 2007 at our institute. Patients involved in our study met the following inclusion criteria: (1) aged less than 50 years, (2) vertical tears >10 mm in length, (3) tears were located in the red zone or red-white zone, (4) patients agreed to undergo second-look arthroscopy while removing the staples used to fix the reconstructed anterior cruciate ligament (ACL) at the tibial site, and (5) no additional injury on the operated knee joint.
The final study group consisted of 81 patients (89 menisci), including 68 male and 13 female patients, 40 left knees and 41 right knees. The mean age at the time of meniscal repair was 25.4 ± 7.7 years (range, 15-50 years). Among the 89 menisci, 65 were medial and 24 were lateral. The duration from the initial injury to meniscal repair ranged from 1 day to 18 years, with a mean time of 14.0 ± 30.1 months. All 81 patients underwent second-look arthroscopy, clinical assessment, and MRI protocol between September 2007 and May 2009. The mean follow-up time (interval between meniscal repair and the postoperative evaluation) was 25.4 ± 6.0 months (range, 17.4-48.3 months).
Meniscal Repair
All tears were vertical and longitudinal, 10 to 40 mm long, and located in the peripheral two-thirds of the meniscus (red zone and red-white zone). The meniscus is anatomically divided into 3 parts: anterior horn, body, and posterior horn. In our study, all involved tears were located at the meniscal body, posterior horn, or in more than 1 part (from anterior horn to posterior horn or from body to posterior horn). Injury details of the repaired menisci are presented in Table 1. Eighty-nine meniscal repairs were performed by 1 experienced surgeon (J.-K.Y.). The operative techniques of meniscal repair in our study were divided into 3 types: (1)bioabsorbable arrow (Linvatec Biomaterials Ltd., Tampere, Finland) technique in 43 cases, described by Albrecht-Olsen et al 2 and Gill and Diduch 15 ; (2) FasT-Fix (Smith & Nephew Endoscopy, Andover, Massachusetts) technique in 35 cases, described by Caborn 9 ; and (3) polydioxanone suture (PDS) technique in 11 cases, reported by Post et al. 25 We changed the repair technique mainly according to new international trends, and also according to the meniscal injury status.
Details of Injury and Repair for the Involved Meniscus a
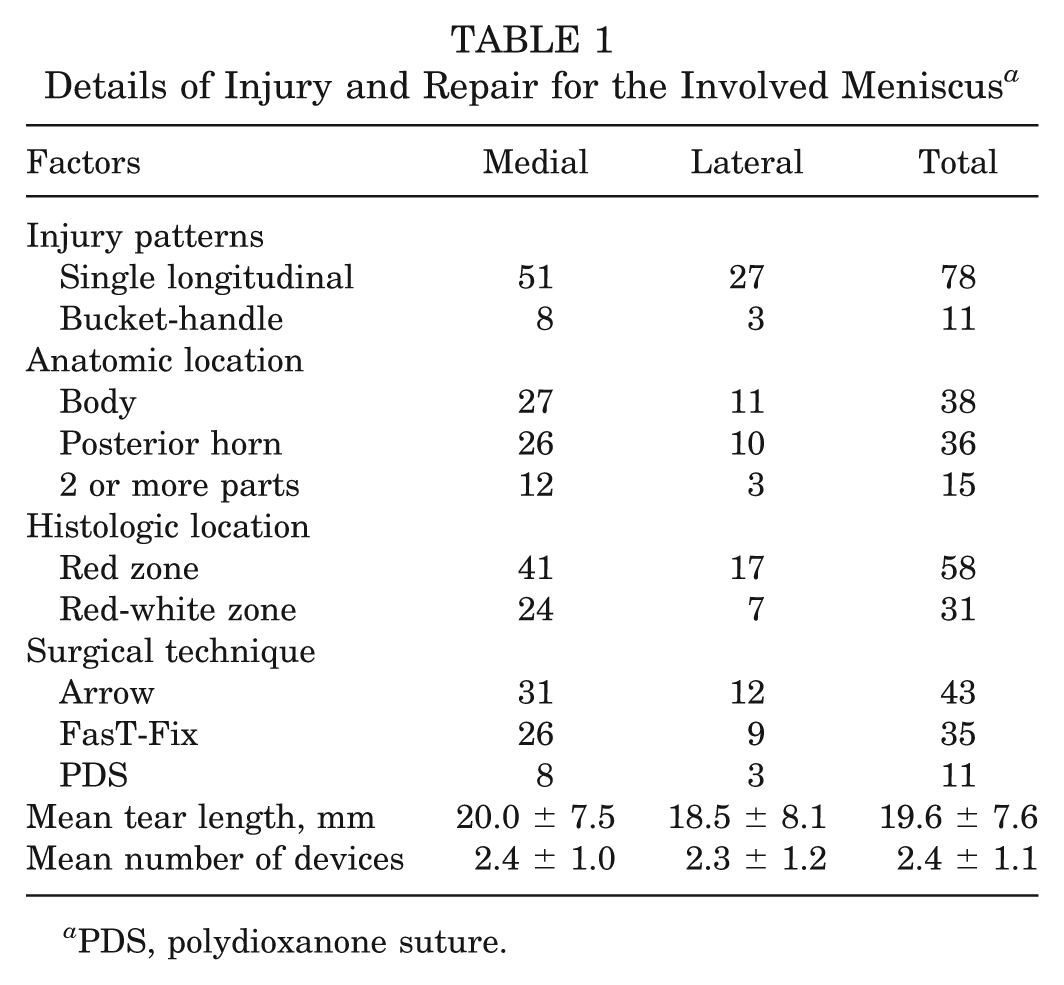
PDS, polydioxanone suture.
Repair details are also presented in Table 1. All 81 patients had concomitant ACL reconstruction because of ACL rupture. Endobuttons (Smith & Nephew) were used for fixation at the femoral side, while staples were used at the tibial side. The staples always brought some discomfort symptoms, such as pain or extrusion. Thus, we had the opportunity to carry out the second-look arthroscopy while taking out the staples for ACL reconstructed cases.
Rehabilitation Programs
The rehabilitation programs were designed according to the combined procedure of meniscal repair and ACL reconstruction that was used in our institute. 22 A double-upright hinged brace was used postoperatively on the patients. During the first 6 weeks, early full extension was emphasized, but flexion was limited to less than approximately 120° as the location of the repaired site was at the posterior horn. Flexion was allowed to exceed 120° from the seventh week after operation, and normal flexion was reached shortly afterward. Full weightbearing was allowed starting on the sixth to seventh week after operation. The brace was withdrawn in week 8 to 10, depending on the muscle strength of the involved leg. Full sports activity was allowed from 6 to 12 months postoperatively, when the muscle strength of the involved knee had achieved 85% that of the healthy knee.
Second-Look Arthroscopy
All 81 patients (89 menisci) underwent second-look arthroscopy by an experienced surgeon (X.G.) while taking out the staples at the tibial sites. The interval between the meniscal repair and second-look arthroscopy ranged from 17.4 to 48.3 months, with a mean of 25.4 ± 6.0 months. The repaired meniscus was confirmed as completely healed if all of the following 3 criteria were met 22 : (1) smooth surface of previously repaired sites on both the tibial and femoral sides by overall observation, (2) no cleft was detected at the repaired sites by probing with a probe, and (3) good stability for the repaired sites by pulling with a probe. Otherwise, we diagnosed the repaired meniscus as unhealed.
Clinical Assessment
All 81 patients underwent clinical assessment the day before second-look arthroscopy. According to the criteria of Barrett et al, 4 an unhealed meniscus was defined by symptoms or physical signs such as swelling, joint-line tenderness, locking or blocking, and a positive McMurray test. Absence of the 4 signs suggested a completely healed meniscus. In this study, expression of the 4 symptoms or signs was recorded respectively. Meanwhile, we evaluated the preoperative (before meniscal repair) and postoperative (before second-look arthroscopy) functional scores, including Tegner score, Lysholm score, and Subjective International Knee Documentation Committee (IKDC) 2000 evaluation.
Magnetic Resonance Imaging Examination Programs
All 81 patients were examined by MRI 1 or 2 days before or after second-look arthroscopy. The MRI scans were performed with a 1.5-T MRI system (Magnatom Sonata, Siemens Medical Systems, Erlangen, Germany) by using a knee coil (Siemens Electric). The following sequences were obtained: (1) sagittal T1-weighted spin echo: repetition time (TR) 600 ms, echo time (TE) 12 mm; (2) sagittal proton density (PD) spin echo: TR 3000 ms, TE 14 mm; (3) sagittal T2-weighted spin echo: TR 3000 ms, TE 85 mm; (4) coronal PD fat-saturated spin echo: TR 3500 ms, TE 14 mm; and (5) coronal T2-weighted fat-saturated spin echo: TR 3500 ms, TE 85 mm. The direction of sagittal scans was made vertical with the connected line of the posteromedial and lateral femoral condyles, while the coronal scans were parallel. The other parameters for all 5 sequences included matrix, 256 × 256; field of view, 16 cm; thickness, 4 mm; and space, 0.4 mm.
One experienced musculoskeletal radiologist (Z.-Z.Z.) and 1 surgeon of sports medicine (Y.M.) reviewed the MRI scans to reach a consensus. In the MRI scans, the signal grade at the repaired site was assessed, using the criteria of Crues et al 12 : (a) grade 0: low signal intensity was shown, which was always defined as a normal meniscus; (b) grade 1: irregularly marginated intrameniscal signal was shown, which was always globular in shape; (c) grade 2: linear signal was shown, without abutting or communicating with an articular surface; and (d) grade 3: similarly linear signal intensity was shown, but extending to the articular surface, whether to the tibial or to the femoral site. Signal intensity was analyzed for the 5 sequences. A grade 3 signal found at the repaired site was considered to be an unhealed meniscus. On the contrary, grade 0 through 2 signal indicated a healed meniscus.
The findings of the MRI examination and clinical assessment were compared with findings from second-look arthroscopy, which was used as the gold standard. The sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) were calculated for MRI and clinical diagnosis, respectively.
Statistics
Statistical analysis was performed with SPSS 15.0 (SPSS, Chicago, Illinois). The mean value for quantitative variables was expressed as mean ± standard deviation. Differences of healing status between categorical variables within each category were assessed with the χ2 test, including the Fisher exact test for binary variables and Pearson test for trinary variables. Differences in the mean value of each quantitative variable between healed and unhealed groups were assessed with an independent-samples t test. The paired-samples t test was used for comparison of the preoperative and postoperative Tegner score, Lysholm score, and Subjective IKDC 2000 evaluation. A P value less than .05 was considered to be statistically significant.
Results
Second-Look Arthroscopy
Among the 89 repaired menisci, 77 were completely healed (Figure 1A), including 59 medial menisci and 18 lateral menisci, with a total healing rate of 86.5%. The healing rates for the medial and the lateral meniscus were 90.8% and 75.0%, respectively; for the red and the red-white zone, they were 86.2% and 87.1%, respectively. The healing rate of single longitudinal tears was significantly higher than for bucket-handle tears (P < .05). The differences between the healed and the unhealed groups are presented in Table 2. The details of the unhealed meniscus under second-look arthroscopy are presented in Appendix 1 (see online Appendix for this article at http://ajs.sagepub.com/supplemental/). All the unhealed menisci were partially resected according to the principle of preserving as much meniscal tissue as possible during second-look arthroscopy (Figure 2A).
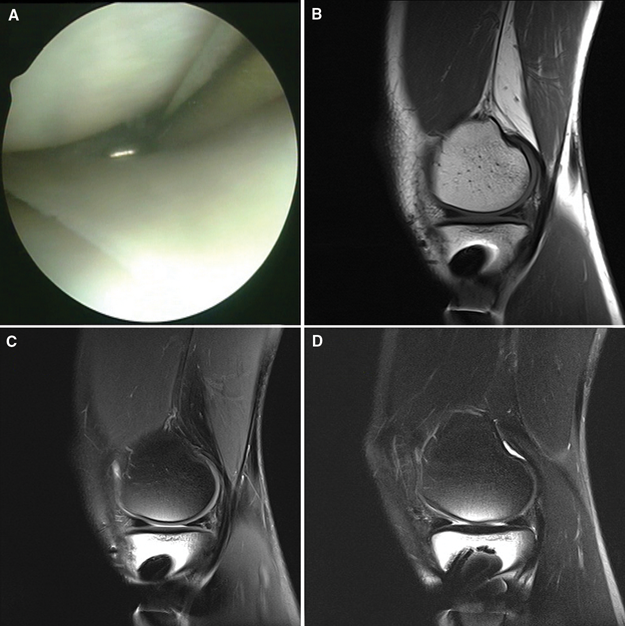
A 31-year-old man with an injured medial meniscus located in the body (red-white zone) and repaired with 2 FasT-Fix devices. At the final follow-up time of 20.8 months, occasional swelling was reported, while the repaired meniscus was confirmed as completely healed by second-look arthroscopy. A, the repaired meniscus showed good stability, smooth surface, and no cleft. B and C, sagittal T1-weighted and proton density images showed grade 3 signals, indicating poor specificity. D, sagittal T2-weighted image showed grade 0 to 1 signal, indicating good specificity and accuracy.
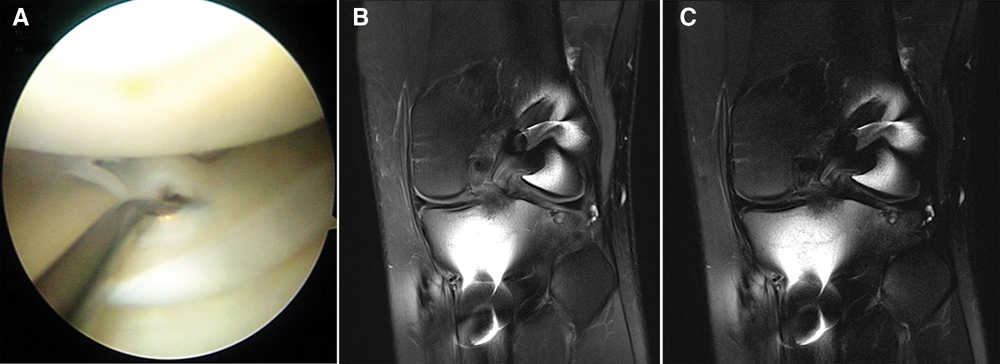
A 19-year-old male patient with an injured medial meniscus located in the posterior horn (red zone) and repaired with 2 FasT-Fix devices. At the final follow-up time of 19.8 months, no symptoms were reported, while the repaired meniscus was confirmed as unhealed by second-look arthroscopy. A, posterior horn was unhealed during second-look arthroscopy. B, coronal proton density image showed grade 3 signal. C, coronal T2-weighted image showed grade 3 signal.
Differences Between Healed and Unhealed Groups Confirmed by Second-Look Arthroscopy a
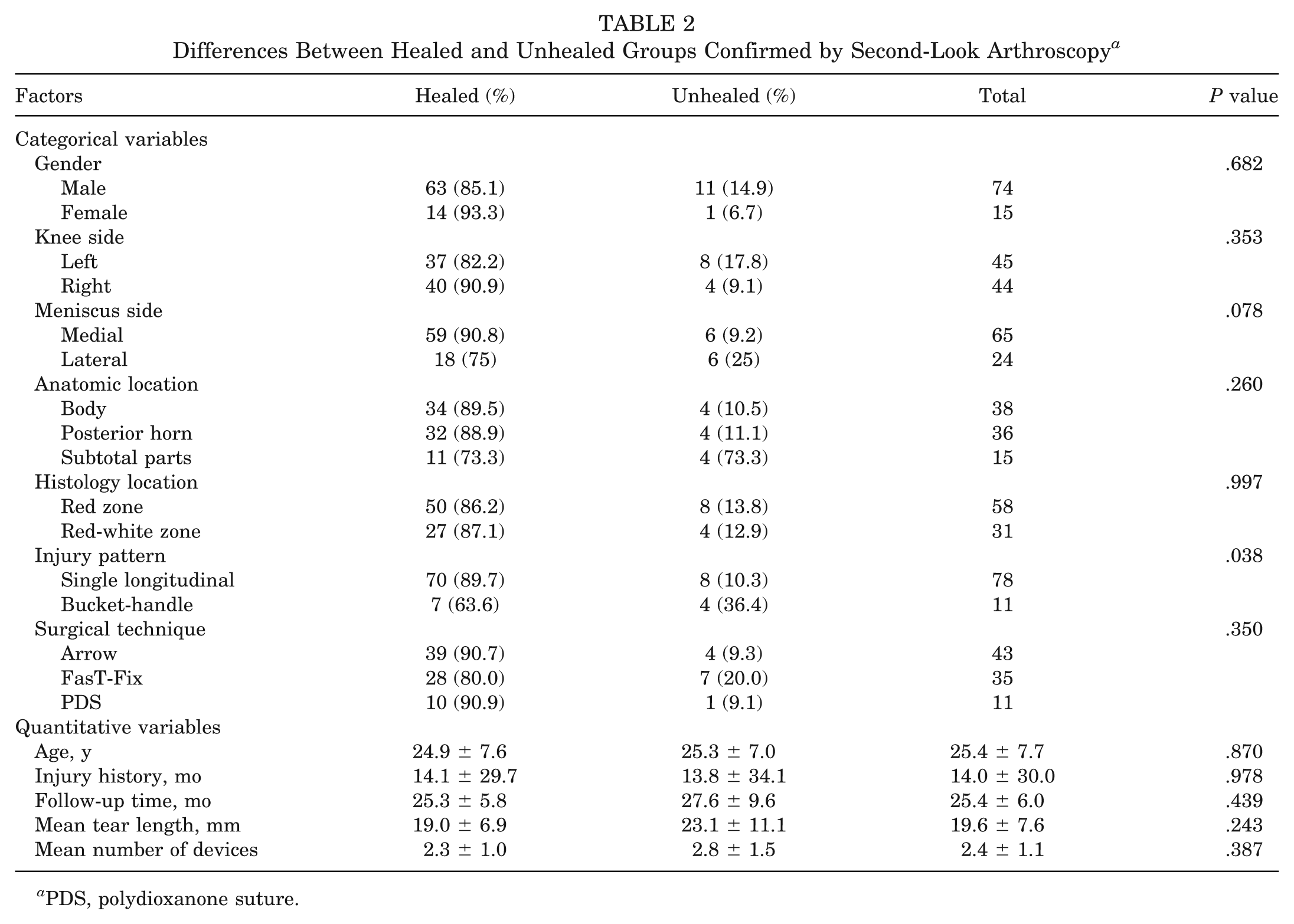
PDS, polydioxanone suture.
Clinical Assessment
Using the criteria of Barrett et al, 4 26 cases that showed at least 1 symptom or physical sign were diagnosed as unhealed meniscus. The healing rate of clinical assessment was 70.8%, significantly lower than the healing rate found by second-look arthroscopy. The distributions of symptoms or physical signs were swelling in 11 cases, joint-line tenderness in 20 cases, locking or blocking in 2 cases, and positive McMurray test in 6 cases. In the 26 symptomatic patients, 16 cases had 1 sign or symptom, 8 cases had 2, 1 case had 3, and 1 had 4. The sensitivity, specificity, accuracy, PPV, and NPV were calculated for groups with different numbers of symptoms or physical signs, as presented in Table 3. The diagnostic value of clinical assessment could be improved when a repaired meniscus with 2 or more signs was defined as unhealed. The diagnostic value of each sign (symptom or physical sign) is presented in Table 4. Among the 12 unhealed cases confirmed by second-look arthroscopy, 7 patients showed different signs, while the other 5 expressed good clinical results. The 3 functional scores at the final follow-up for the healed group confirmed by second-look arthroscopy were significantly higher than the unhealed group (P < .05), while the scores before second-look arthroscopy between the 2 groups had no difference (P > .05). The details are shown in Table 5.
Diagnostic Results of the Different Number of Symptoms or Physical Signs a
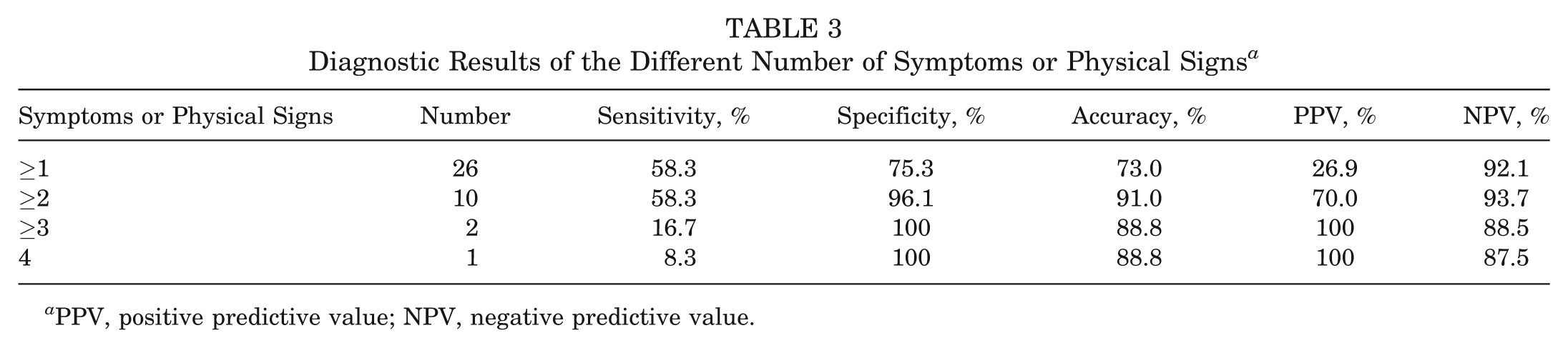
PPV, positive predictive value; NPV, negative predictive value.
Diagnostic Results of the Different Clinical Signs a
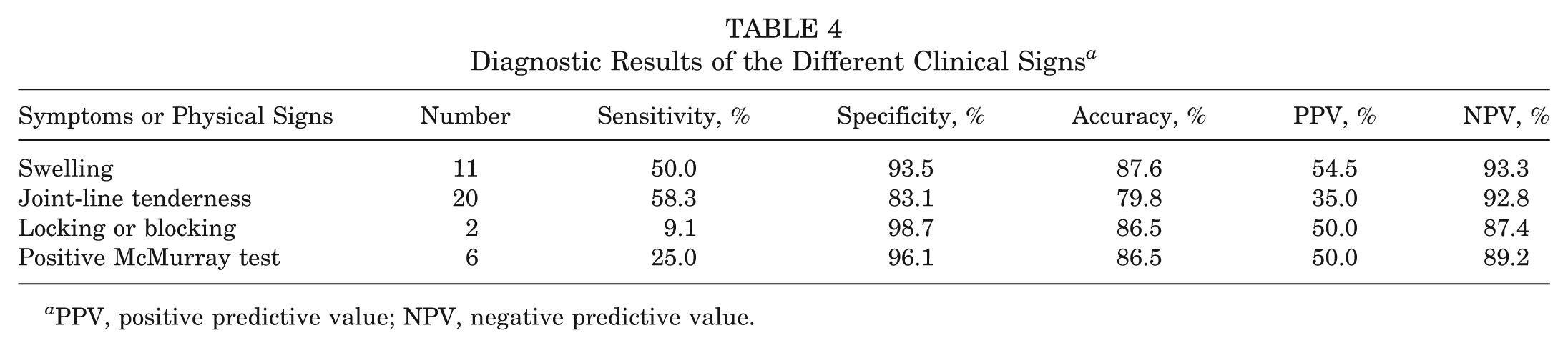
PPV, positive predictive value; NPV, negative predictive value.
Functional Scores Between Unhealed and Healed Groups Before Second-Look Arthroscopy and Final Follow-up a
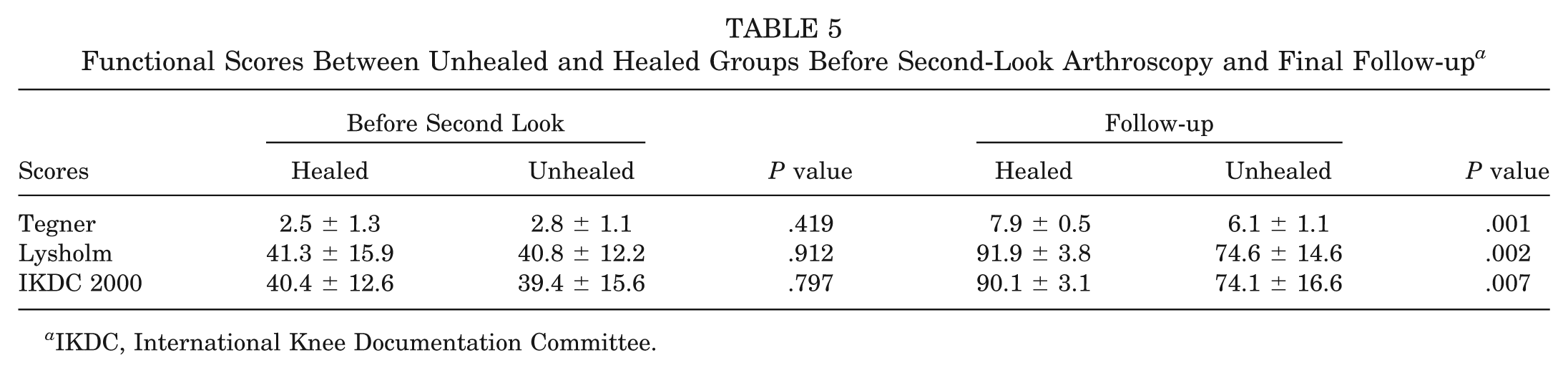
IKDC, International Knee Documentation Committee.
Magnetic Resonance Imaging Examination
The grade 3 signal had higher proportions in sagittal T1 and PD images (48.3% and 62.9%, respectively), while they were lower in sagittal and coronal T2 images (16.9% and 6.7%, respectively). The healing rate according to sagittal T2 imaging was 83.1%, close to the results of second-look arthroscopy. The number of different signal grades and the healing rates diagnosed by MRI for each sequence are presented in Table 6. In the PD images (both sagittal and coronal), the FasT-Fix–repaired group had a significantly lower healing rate than the other 2 repair groups (P < .05). In the coronal images (both PD and T2), the subtotal injured menisci (subtotal injuries involve more injury to meniscal tissue, eg, injuries from anterior horn to posterior horn or from body to posterior horn) and bucket-handle tears had a significantly lower healing rate than the other group (P < .05). Compared with other sequences, the T2 sequences indicated better diagnostic value, which showed higher specificity and accuracy (Figure 1, B-D). However, the sagittal T1 and PD images showed higher sensitivity than other sequences. The details of diagnostic results are presented in Table 7. Among the 12 unhealed menisci that were confirmed by second-look arthroscopy, 11 cases showed grade 3 signal in at least 1 sequence; only 1 showed grade 0 signal in all 5 sequences. Additionally, 5 cases of 12 unhealed meniscus showed grade 3 signal in all 5 sequences, while none of the healed menisci had this expression (Figure 2, B and C).
Signal Grades for the 5 MRI Sequences a
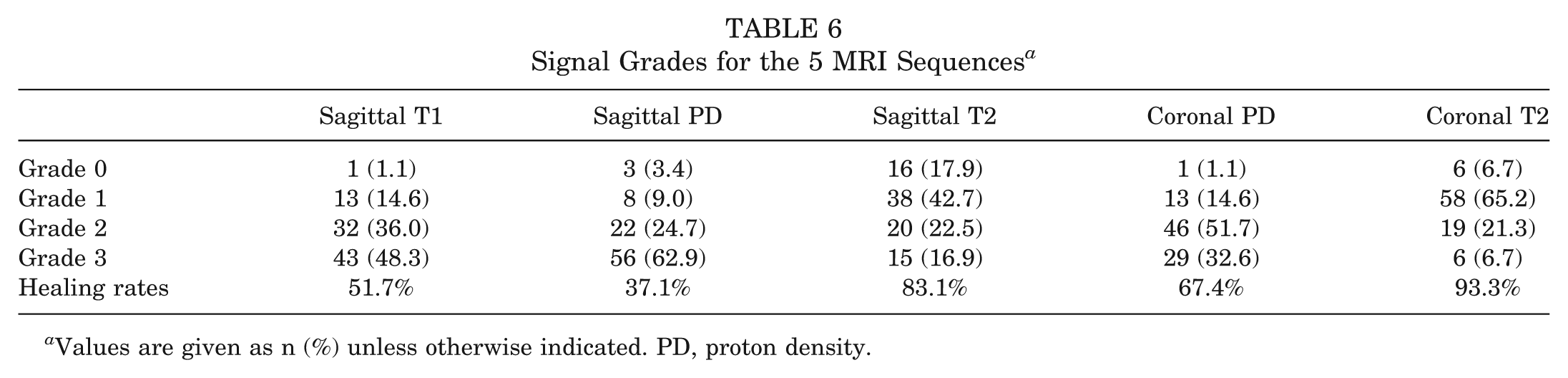
Values are given as n(%) unless otherwise indicated. PD, proton density.
Diagnostic Results (in Percentages) of Each MRI Sequence a
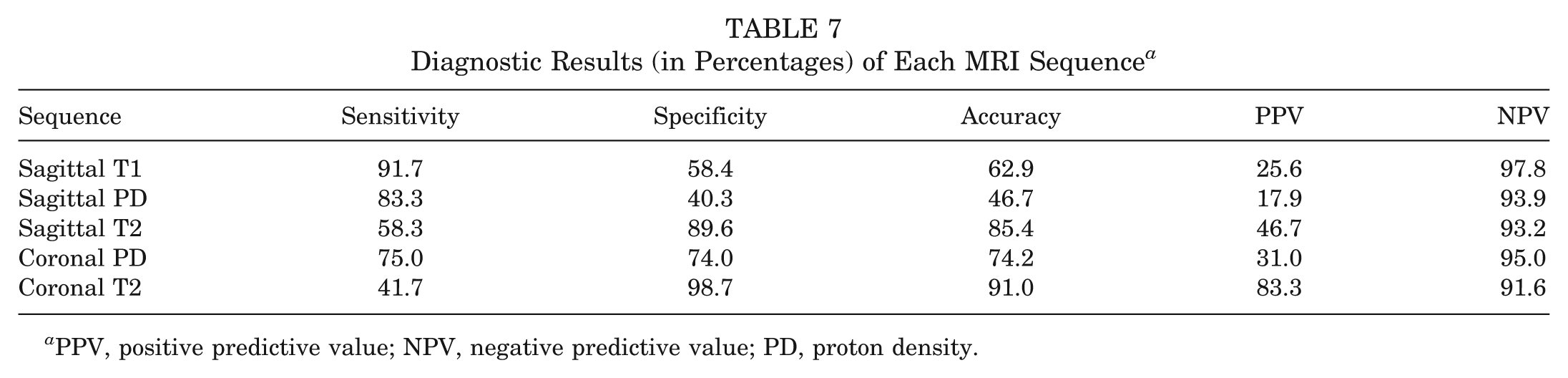
PPV, positive predictive value; NPV, negative predictive value; PD, proton density.
Discussion
The meniscus is important for preserving a multitude of normal knee joint functions, such as shock absorption, force transmission, stability maintenance, and joint lubrication. 14,18,19 Because of these critical functions of an intact meniscus, it is important to preserve as much meniscal tissue as possible for patients with meniscal injury. Thus, meniscal repair has become the optimal treatment for vertical tears located at the vascular zone. 8,27
The evaluation of the healing status for a repaired meniscus is difficult but useful for the surgeon in guiding the patient’s rehabilitation procedures. The main diagnostic methods for a repaired meniscus include second-look arthroscopy, MRI, and clinical assessment. Second-look arthroscopy, which is always recommended as the gold standard, has obvious advantages in evaluating the healing status, but it is hardly used for every case because of the high cost and invasiveness of this technique. 1 Although clinical assessment is the simplest method for the evaluation, it is highly dependent on the experience of the surgeon. 17 Accordingly, MRI is proposed to be an ideal diagnostic method in evaluating meniscal healing status. 10 The first study using MRI after meniscal repair was reported by Farley et al 13 and indicated persistent pathologic signals after meniscal repair. Steenbrugge et al 28 stated that such signals represented edematous or fibrous scar tissue, not true lack of healing. Consequently, the diagnostic value of MRI in evaluating repaired meniscus is questioned. However, no studies used second-look arthroscopy as the gold standard for each consecutive case and also no studies made a conclusive comparison among the 3 diagnostic methods. Our study addressed this study gap and additionally applied 5 sequences for MRI diagnosis.
In our study, we found that second-look arthroscopy, which evaluated repaired meniscus from 3 aspects as mentioned in the Materials and Methods section, was the most conclusive and accurate evaluating method. The total healing rate was 86.5%, consistent with the complete healing rates between 42% and 88% as previously reported, despite the fact that most of them were not the results of second-look arthroscopy. 26 Logan et al 19 have reported that medial meniscal repairs were significantly more likely to fail than lateral ones, when diagnosed by clinical assessment. However, no significant difference of healing rate was detected between the medial and lateral menisci in our study (P = .078), even if the medial meniscus demonstrated the trend of higher healing rate. One of the interesting findings of our study was that bucket-handle tears had a lower healing rate than single longitudinal tears, with a healing rate of 63.6% and 89.7%, respectively. This difference may be caused by the longer tears and less repair stability. Meanwhile, when compared with the healed group, the mean follow-up time for the unhealed group was 27.6 months, there was no significant difference. This indicated that the unhealed status was not induced by short follow-up time. During second-look arthroscopy, 3 cases in 12 unhealed menisci were diagnosed as healed ones at first sight, because of the smooth surface and good stability. But when we probed the primary repair sites, we detected small clefts, with lengths of 5 to 7 mm. So we suggest that probing at the repair sites should be done carefully.
During clinical assessment, we found that the most common symptom was joint-line tenderness, which also appeared in healed cases. In the study by Barrett et al, 4 the authors defined clinical failure as showing 1 or more symptoms. Following the above criteria, we obtained a lower success rate compared with our results of second-look arthroscopy. Also, the low sensitivity, specificity, and accuracy demonstrated that the diagnostic value of clinical assessment was very small. However, we accidentally found that using 2 or more signs as an unhealed diagnostic criterion could improve the specificity and accuracy, while the sensitivity was still low. Despite the improvements made, we found difficulties in detecting all unhealed cases by clinical assessment. In addition, the 2 cases with 3 or 4 symptoms were all confirmed unhealed during second-look arthroscopy. Thus, it was our hypothesis that 3 or more combined symptoms could be used as the diagnostic expression of unhealed menisci, which could be confirmed by future study with more cases.
In 5 MRI sequences, the healing rate on sagittal T2-weighted images was similar to that of second-look arthroscopy. The healing rate on sagittal PD images was the lowest, because of its sensitivity to healing scar and other soft tissue. Compared with sagittal sequences for PD and T2, each coronal sequence had a higher healing rate. Although we failed to find a conclusive explanation for this phenomenon, we suggest that (1) the higher amount soft tissue in the posterior horn in coronal images increased the difficulties in identifying grade 3 signal and (2) the fat-saturated characteristic of coronal sequences reduced the grade 3 signals, which were induced by soft tissue with fat. Steenbrugge et al 28 noted persistent grade 3 signal 13 years after repair. However, in our study, 1 patient with the longest follow-up time of more than 4 years, whose meniscus was healed, showed grade 3 signals in sagittal sequences and grade 0 signals in coronal sequences. During the comparison, we found that the subtotal injured menisci and bucket-handle tears had higher rates of grade 3 signal in coronal sequences. This is because both the subtotal injuries and the bucket-handle tears had long injury length, which could induce more fibrocartilaginous scars and result in more grade 3 signals during the healing procedure. Moreover, in the 2 PD sequences, the repairs with FasT-Fix showed more grade 3 signals than the other 2 repair patterns. This is because FasT-Fix is nonabsorbable and thus induces more reaction. In the results of diagnostic tests, the T2 sequences showed higher specificity and accuracy, while the PD and T1 sequences showed higher sensitivity. Therefore, we could not acquire an ideal sequence that showed high sensitivity as well as high specificity. In the MRI evaluation, 7 cases, which were all unhealed during second-look arthroscopy, showed grade 3 signals in all sequences. This seems to indicate that the repaired meniscus was unhealed when grade 3 signals appeared simultaneously in all 5 sequences. The results of clinical and MRI evaluation for each unhealed case are presented in Appendix 3 (see online Appendix for this article at http://ajs.sagepub.com/supplemental/).
Finally, we realized that the study had some considerable limitations. First, we only observed the cases that had concomitant ACL reconstruction. Thus, we could not obtain the MRI imaging of isolated meniscal repair and thus cannot comment on the efficacy of MRI for imaging isolated meniscal repairs. Second, we used 3 techniques (PDS, bioabsorbable arrow, and FasT-Fix ) in our study, which might affect the MRI expressions and induce the bias of the diagnostic results. Third, the number in the unhealed group was small, which affected the evaluation of diagnostic value. In further study, cases of isolated repair would be included, and the total case number would be increased.
Conclusion
Second-look arthroscopy was the most dependable way to determine meniscal healing by using 3 criteria. The bucket-handle tears had a lower healing rate than single longitudinal tears. Clinical assessment had obvious limitations in detecting healed menisci, but had high specificity when cases with 2 or more symptoms were considered as unhealed. In MRI examination, T2 sequences had obviously higher specificity and accuracy, while PD and T1 sequences had higher sensitivity. Subtotal injuries, bucket-handle tears, and repairs with FasT-Fix had higher rates of grade 3 signals in different sequences. Also, the coronal sequences had lower rates of grade 3 signals than relative sagittal sequences.
Footnotes
One or more authors has declared a potential conflict of interest: This study was supported by the foundation “Second Period of 985 Projects” of Peking University Health Science Center.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.