
Abstract
Meniscal allograft transplantation is a useful technique by which to alleviate pain and perhaps retard degenerative changes in the symptomatic meniscus-deficient knee. 4,11,16 When a meniscal allograft is implanted with bone plugs or a bone bridge, accurate size matching of the graft to the host is crucial. 12 Although limited studies have investigated the knee’s tolerance for measurement mismatch, estimates indicate that graft size should be within 10% of the native meniscus. 2,16
Currently, there are 2 predominant methods for sizing the allograft: radiographic analysis, as proposed by Pollard et al, 9 and magnetic resonance imaging (MRI) interpretation, as proposed by Haut et al. 3,5 In the Pollard method, there is a correction made for magnification; the width is then calculated on the anteroposterior radiograph of the knee, by measuring from the tibial metaphyseal margin to the peak of the tibial eminence. The length is measured on the lateral radiograph, and a 70% adjustment is made for the lateral meniscus and an 80% adjustment for the medial meniscus. Haut et al 5 used MRI parameters of the meniscus to predict the required allograft size, and most recently Prodromos et al 10 confirmed the accuracy of MRI in this application. However, the described studies have substantial standard deviations of measurement and relatively large average error rates. 1,5,14,15 There is no standardized protocol for meniscal sizing at this point. 1,5,14,15
The need for accurate meniscal allograft size estimation led us to investigate techniques for accurately determining the size of the required meniscal allograft. The majority of contemporary studies have used radiographic measurements for sizing. The major limitation with plain radiographic measurements is that error lies with the indistinct bony landmarks, which may vary according to the rotation and the inclination when the radiographs are taken. The purpose of this study was to determine the reliable bony landmarks of the lateral tibial plateau on radiographs using our protocol, to (1) reproduce these locations and (2) compare them with measurements based on the traditional method described by Pollard et al. 9 Our hypothesis was that our protocol for radiologic measurements would provide reproducible bony landmarks and that the measurements of lateral tibial plateau would correlate with the actual anatomic values.
Materials and Methods
Patient Data
Of 89 fresh lateral menisci obtained during total knee arthroplasty, 25 samples were adequate for evaluation. The samples were obtained carefully, including the attached proximal tibia and without injuring the meniscus itself and the bony attachment sites. The patient inclusion criteria comprised mild to moderate osteoarthritis (Kellgren-Lawrence grade I or II) with mechanical axis deviation of less than 15°. We excluded knees with lateral compartment osteoarthritic change and injured or degenerated lateral meniscus. Any failure in obtaining the preoperative radiograph according to the authors’ strict protocol resulted in the samples being excluded. The mean age of the patients was 74.1 years (range, 63-82 years). Each patient received a detailed explanation of the protocol and discussed the protocol with us before signing the consent form for participation.
Radiographic Measurements
The nomenclature for describing meniscal size can be confusing. By convention, meniscal width is the medial-lateral coronal plane dimension, as determined from the anterior-posterior (AP) radiograph. Meniscal length is the anteroposterior sagittal plane dimension, as determined from the lateral radiograph. All images were taken on 14- × 17-in. (36- × 43-cm) film using a focus-to-film distance of 72 in. (183 cm). All radiographs were taken and measurements done on a picture-archiving and communication system (PACS, GE Healthcare, Chicago, Illinois). Preoperative images were taken using a size marker (10-cm bar) to normalize them for magnification. It was important to place the magnification bar at the level of lateral tibial plateau—that is, just lateral to the patellar tendon where the Gerdy tubercle is situated—to minimize the bias of magnification factor.
For AP and lateral radiographs, the radiographic beam was angled 10° caudally at neutral rotation. This lateral view differentiated the lateral plateau cortical margins from the medial plateau (Figure 1). The transition points, which are the turning points from the slope to the lateral plateau, could then be identified. Figure 2 illustrates the schematic radiologic measurements: The width measurements were done as described by Pollard et al 9 (Figure 2A); for length measurements, our protocol was used (Figure 2B). The conventional Pollard measurement (Figure 2C) was done for comparison. On AP radiographs, 2 parallel lines (A and B) were drawn tangential to the lateral and medial borders of the tibia plateau. A line perpendicular to these ran tangentially to the lateral intercondylar spine (C). The distance from the lateral border of the tibial plateau to the midpoint of the lateral intercondylar spine was measured (width, W). On lateral radiographs, based on our protocol, the anterior and posterior transition points (d, e) are identified. The distance between these points was recorded (length, L). For the conventional Pollard method, 9 the sagittal tibial plateau distance was measured at the joint line between a line parallel to the anterior tibia above the tuberosity and one tangent to the posterior plateau margin perpendicular to the joint line (Figure 2C).
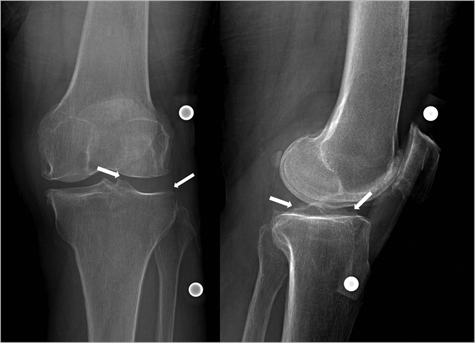
Radiographs taken according to our protocol. Regarding the position of the magnification markers (10-cm bar), as placed at midlevel of lateral plateau (ie, at the level of Gerdy tubercle lateral to patellar tendon), rotation was applied (eg, overlapping of femoral condyles for neutral rotation). Notice the medial tibia plateau and the lateral tibia plateau, which are distinguished. The cortical margins of each plateau and the transition zone to anterior and posterior slopes can be identified (arrows). This view was accomplished by slight tilting (5° to 10°) of the projection beam caudally.
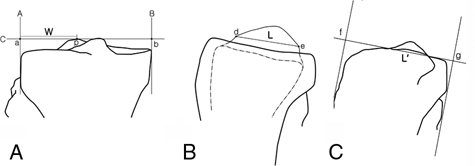
Lateral meniscus: schematic anterior-posterior (A) and lateral (B and C) representation of radiologic measurements: A, on anterior-posterior view, A and B are tangents to the lateral and medial tibia plateau, and a tangent line (C) is drawn between them. The intersection points are marked as a and b; p is the peak point of the lateral intercondylar spine. The width (W) is defined from a to p. B, on lateral view, the anterior and posterior transition points of lateral tibia plateau can be identified as d and e. The distance between these 2 points defines the length (L). C, by Pollard’s method, the length (L’) is the distance at the joint line between a parallel line to the anterior tibia above the tuberosity (f) and one tangent to the posterior plateau margin perpendicular to the joint line (g).
Radiographic measurements were made by 2 physicians: an orthopaedic surgeon who specialized in knee surgery and who was blinded from the study and a senior orthopaedic resident. Measurements were done at 2 times, 2 weeks apart, with the observers blinded to meniscus dimensions. An average of 5 measurements at each session was recorded to reduce the random errors.
Surgical Procedure and Anatomic Measurement of Lateral Meniscus
All total knee arthroplasties were performed with the standard incision and the standard medial parapatellar approach to the joint. After preliminary release of medial soft tissues, the anterior and posterior cruciate ligaments were excised. Ligamentous balancing was done, and an attempt was made to resect 10 mm of tibial bone distally from what was considered to be the intact articular surface, to achieve a surface that was perpendicular to the shaft of the tibia in the coronal plane, with a 7° posterior slope in the sagittal plane. Consideration was taken during anterior and posterior cruciate ligament removal not to injure the anterior and posterior bony attachments of the lateral meniscus. Proximal tibia bone cutting was also carefully performed. Saw cutting was done not to injure the lateral collateral ligaments and posterolateral structure, including the popliteus tendon. Every effort was taken to preserve the lateral meniscus.
Intraoperative measurements were taken right after the operation, when the samples were fresh. Nondigitalized Vernier calipers (Mitutoyo, Kanagawa, Japan) accurate to within 0.05 mm were then used to measure the meniscus dimensions. The anatomic measurements were done as suggested by Shaffer et al. 15 The AP length of the menisci was measured from the visible meniscosynovial junction anteriorly to the same junction posteriorly. The measurement was made at the site of the greatest dimension and parallel to the tibial intercondylar spines. The mediolateral width was determined by measuring from the peripheral edge of the lateral meniscus at midtibia to a line connecting the anterior and posterior meniscus horns. Care was taken to draw this line through the medial-most or lateral-most portion of the fibrocartilaginous meniscus rather than its root insertion (Figure 3). Two measurements were made of each lateral meniscus and the average was recorded.
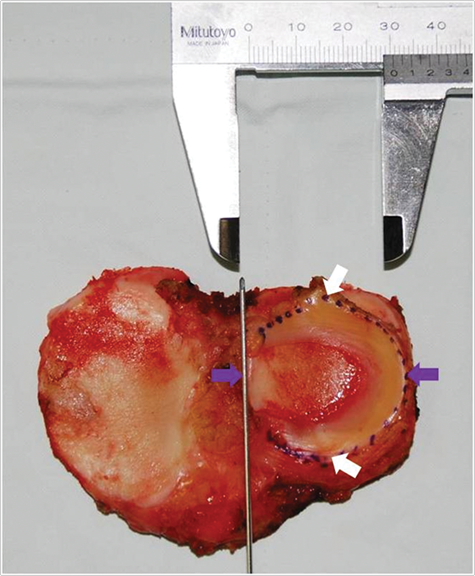
The methods of anatomic meniscal measurements were similar to those of Shaffer et al. 15 Surgical marking pen was used to outline the meniscosynovial junction for better photographic visualization. Nondigitalized Vernier calipers are shown measuring the mediolateral width of the lateral meniscus (purple arrows). To measure the anteroposterior length, the most anterior and posterior points were used (white arrows). A guide wire positioned directly over the meniscus horns facilitated a consistent landmark for measurement.
Statistical Analysis
Means, standard deviations, 90% confidence intervals were determined for each measurement. We also recorded the absolute value of deviation from the actual measurements of the tibial plateau, as well as the percentage error of the radiographic measurements (based on our method and Pollard’s). A positive value occurred when the image measurement exceeded the actual value, thus reflecting that the measurement was an overestimate of the meniscus size. A negative value occurred when the imaging measurement was less than the true value, thus indicating that the measurement was an underestimate. Paired t test was used to determine differences between anatomic and radiologic measurements.
The reliability of each radiologic measurement was assessed with the intraclass correlation coefficient, which quantifies what proportion of difference is due to measurement variability. The intraclass correlation coefficient can assume any value from 0 to 1, where >.80 represents good agreement; between .60 and .79, moderate agreement; and <.59, poor agreement. In both cases, all values showed good reliability (Table 1).
Interobserver and Intraobserver Error of Measurement: Intraclass Correlation Coefficients a
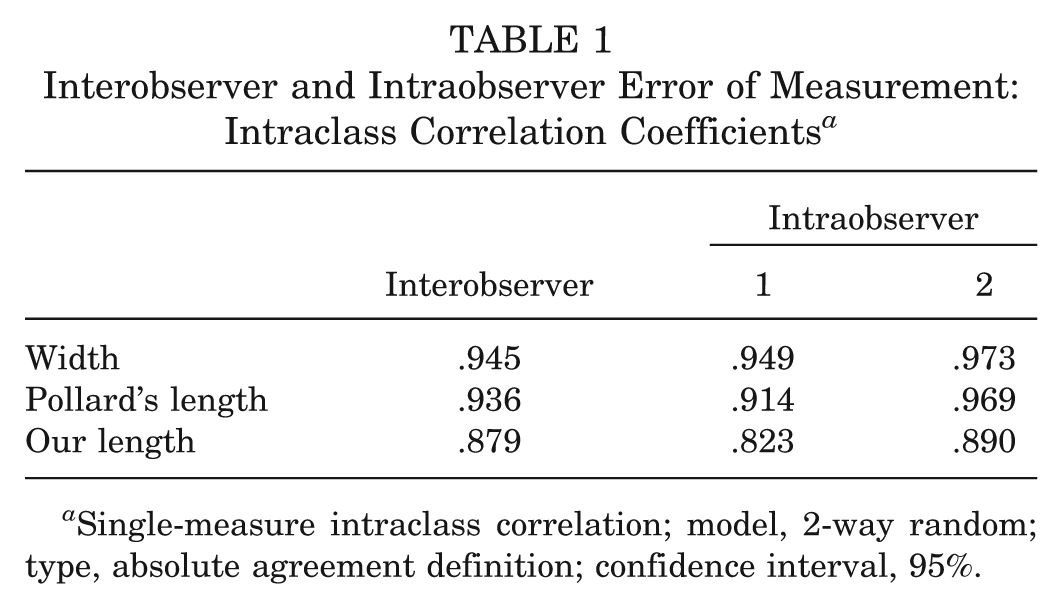
Single-measure intraclass correlation; model, 2-way random; type, absolute agreement definition; confidence interval, 95%.
Accuracy reflects how closely the imaging measurements corresponded to the actual measured dimensions of the meniscus. We examined the frequency with which each width and length imaging measurement fell within 10% of the actual anatomic dimensions for each of the 25 menisci. If radiographic measurement was within 90% to 110% of the anatomic measurement, we classified it as accurate. All radiologic measurements were tested for normality using Shapiro-Wilk W test.
The measurements of the menisci were plotted against the tibial plateau dimensions to determine correlation between the values. Simple linear regression analysis was used to derive a formula for calculating a predicted value for each meniscal dimension based on the appropriate tibial plateau dimensions. This was repeated for each radiologic measurement. In addition, a simple linear regression analysis between the anatomic width and length was done. Pearson χ2 test was used to determine statistical value.
All statistical analyses were performed with SPSS version 12.0 (SPSS Inc, Chicago, Illinois) and Analysis Excel 2007 (Microsoft Corp, Redmond, Washington). P ≤ .05 was considered significant.
Results
The Pollard dimensions were generally larger than our measurements. Table 2 shows the mean anatomic meniscal dimensions and radiologic plateau measurements (with standard deviations); the absolute difference and the percentage differences are also shown. The radiographic measurements for width, our length, and the modified Pollard length were within the confidence interval (90%), whereas the Pollard length was outranged; the paired t test also showed a significant P value. All radiologic measurements were in normal distribution (P > .05, range .053 to .495) (Figure 4).
Results of Anatomic and Radiologic Measurements
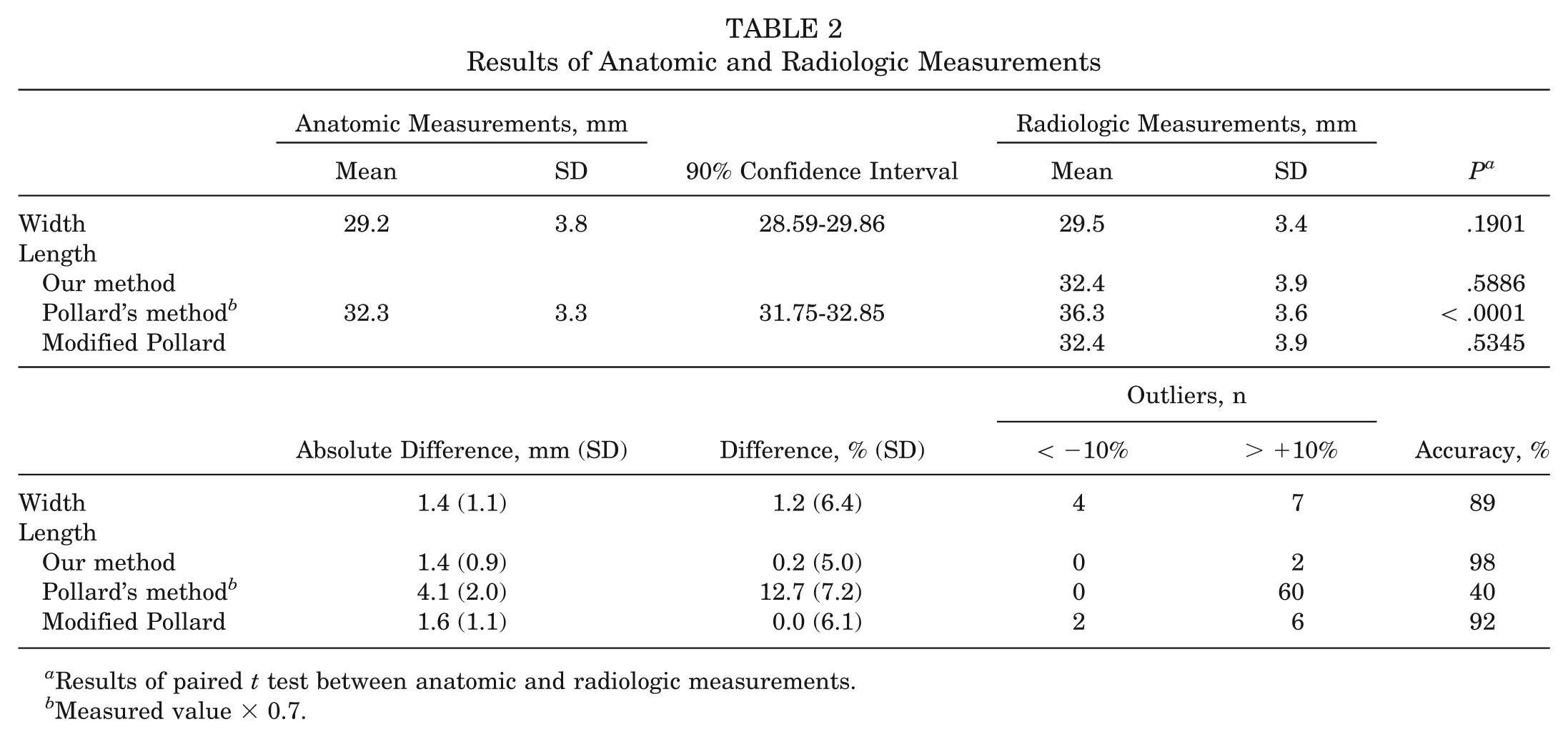
Results of paired t test between anatomic and radiologic measurements.
Measured value × 0.7.
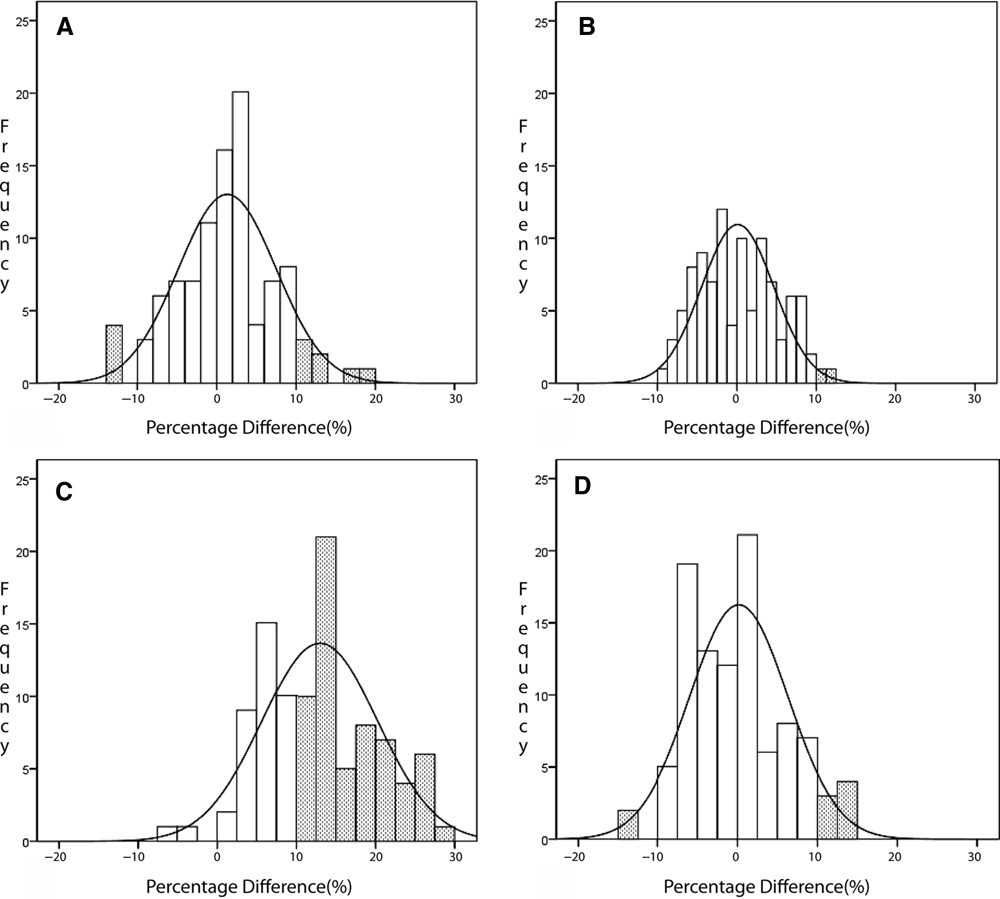
Histogram of each measurement. Percentage difference is shown on the x-axis and the number of measurements on the y-axis. All measurements were in normal distribution. Notice the outliers (<−10% and >10%) in the dotted box of each measurement. A, width (P = .495); B, our method (P = .230); C, the conventional Pollard method (P = .053); D, the modified Pollard method (P = .057).
With respect to accuracy, which represents the frequency of measurements that fall within 10% of the actual measurements, our method was superior to the Pollard method. The accuracy of our length was 98% whereas for the Pollard method it was 40%. The number of outliers—that is, those outside 10%—was 2 (2%) for our method and 60 (60%) for Pollard’s method (Table 2, Figure 4).
The correlation of our method for measuring lateral meniscal length was better than the method proposed by Pollard. There was a moderate to good correlation between anatomic meniscal dimensions and radiologic plateau dimensions for our lateral meniscal width (R 2 = .790) and our lateral meniscal length (R 2 = .823). In contrast, there was fair correlation for Pollard’s lateral meniscal length (R 2 = .660) (Figure 5).
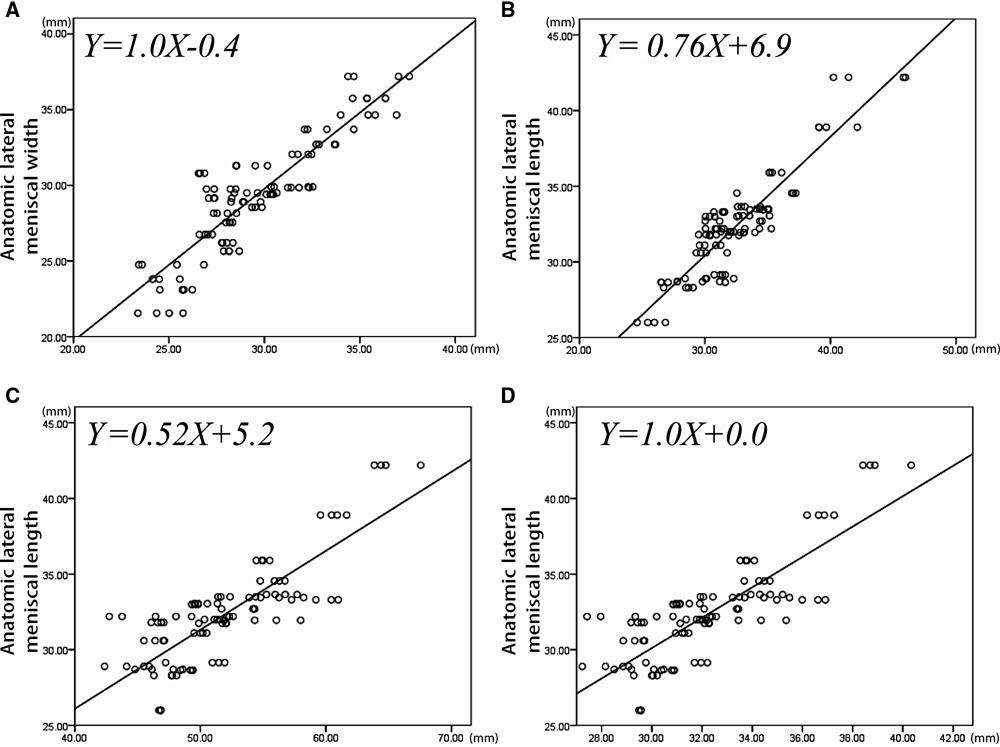
The simple linear regression lines with radiologic measurements (in millimeters) on the x-axis and anatomic measurements (in millimeters) on the y-axis. A, width (R 2 = .790); B, author’s method (R 2 = .823); C, the conventional Pollard method (R 2 = .660); D, the modified Pollard method (R 2 = .660). The modified Pollard method refers to the following equation: anatomic length = 0.52 × plateau length (according to the Pollard method) + 5.2.
Because the accuracy of Pollard’s method of measuring the length of lateral meniscus was low (40%), we tried to determine the best-fit equation for predicting meniscal size from Pollard’s method of bone size, and the equation was as follows:

and not as Pollard et al 9 suggested:

Based on this equation—namely, the modified Pollard method—the percentage difference decreased, and the accuracy increased to 92% (Table 2).
There was a poor correlation between the anatomic width and length dimensions (R 2 = .425, p = .241).
Discussion
This study compared current methods of radiographic meniscal allograft sizing 9 with our proposed method. Based on a strict protocol for radiographic imaging, the accuracy (ie, within 10% of the anatomic dimensions) of our method and Pollard’s for length was 98% and 40%, respectively. The main strength of this study is that all meniscal samples were measured in fresh state.
The cause of variability experienced by the sizing methods based on the radiographic parameters is likely multifactorial, including radiographic errors in magnification, erroneous identification of bony landmarks, and difficulty in differentiating between the soft tissue–bone interface. 5,9,15 Shaffer et al 15 compared the results from true AP and lateral films with those obtained from knees with 15° of internal and external rotation and found that rotation significantly increased the errors. It is therefore important to take the preoperative radiograph in a strict manner. By tilting the radiographic beam caudally about 5° to 10° in taking the lateral radiograph, we were able to identify each plateau cortical margin. In addition, by following the lateral plateau margins, we could identify the transition points from plateau to each anterior and posterior slope. Although a validation study is lacking regarding which anatomic areas of the lateral tibia plateau these transition points are actually indicating, the reproducibility of these points are proved by high intraclass and interclass correlation coefficient values (Table 1).
The goal of meniscus transplantation techniques should be to replace a meniscus of the same size as the original tissue; therefore, accurate and reproducible sizing methods are essential to the overall success of the meniscal transplant. Several studies have emphasized the importance of accurate meniscal allograft sizing. Haut et al 5 emphasized the importance of transverse and cross-sectional meniscal parameters in determining the contact pressure distribution on the tibia plateau with their algorithm. In a sheep study, Lazovic et al 7 showed that implanting an incongruous graft or nonanatomic positioning of the insertional ligaments led to increased degenerative changes within the animals’ knees. In a biomechanical study using cadaver knees, Sekaran et al 13 showed that malpositioning of the tunnel for the posterior horn bone plug of a medial meniscal transplant—by as little as 5 mm away from the point of insertion of the original meniscus—caused a significant increase in the maximum contact pressures within that compartment of the knee. In another biomechanical study using cadaver knees, Dienst et al 2 proposed that the mismatch on graft selection should be less than 10% of the size of the original meniscus.
Meniscus-sizing studies in human beings have been performed by Pollard et al and others. 5,8,9,15 The study by Pollard et al 9 established a correlation between bony landmarks and meniscal tissue size. 9 A tantalum powder–cyanoacrylic paint was applied to 21 cadaveric specimens (12 female, 7 male, and 2 unknown sex), and radiographic measurements were compared with caliper measurements of the tissue. Lateral meniscal width equaled the distance from the peak of the lateral tibial eminence to the lateral periphery of the tibial metaphysis. On lateral films, the lateral meniscal length was 70% ± 8% of the sagittal length of corresponding tibial plateau dimension. However, measurement errors by these predictive criteria showed a standard deviation ranging from 7.4% to 8.4%. This transposed to a largest possible error of 2.9 mm for lateral meniscal width and 3.2 mm for lateral meniscal length. Our results regarding the sagittal length of lateral meniscus interpreted by Pollard’s method were quite different. The measurements under strict radiographic protocol, as in our study, reproduced the relation between the anatomic and radiographic measurements of tibial plateau according to their protocol, which resulted in the following equation—anatomic length = 0.52 × plateau length (according to the Pollard method) + 5.2—and not as they suggested (anatomic length = 0.7 × plateau length). When based on the conventional Pollard method, the accuracy was 40%. In contrast, when the modified Pollard method was used (anatomic length = 0.52 × Pollard’s plateau length + 5.2), the accuracy increased to 92%. There may be a couple of reasons for this. First, the recruited meniscal samples were from an Asian population. The dimensions could be different from the Western population. Second, the technique of obtaining the implant view was strict in our case, and every effort was made to obtain the desired radiograph. This could have resulted in the difference.
Haut et al 3,5,6 described the importance of not only the transverse meniscal measurements but also the cross-sectional dimensions. They recommended MRI as a better imaging modality than radiography for predicting the cross-sectional parameters. But from a practical point of view, contralateral MRI has its limitations in predicting the demanded meniscal dimensions, and tissue banks may not provide the precise transverse, cross-sectional size-matched allograft. Despite the lack of 3-dimensional parameters, radiographic measurements may have a role in reproducing accurate transverse dimensions.
Regardless of how accurate average measurements may be, they may not be suitable if individual measurements significantly stray from the mean. In trying to better understand this, we sought to determine how many meniscal measurements fell within what we defined as an acceptable margin of error. In recognizing that the tolerance of inaccuracy in meniscus implantation is not surely known, we variably set the margin at 10% of either the width or the length of the actual anatomic dimensions for each of the 25 lateral menisci. Using this criterion, we were surprised to find that the studied radiographic measurements were particularly accurate. The accuracy rate was 98% in measuring the length of lateral meniscus. The reasons for increased accuracy compared with previous reported radiographic studies 5,8,9,15 may lie with the strict imaging and measuring techniques and the freshness of the meniscal samples.
It is surprising that the radiographic width measurement had a relatively low accuracy (89%). Four (4%) samples were below 10% and 7 (7%) samples were more than 10% of actual anatomic meniscal size. Although the percentage difference (1.22% ± 6.36%) in our results is compatible with the values previously reported 9 (standard deviation, 8.4%), the margins of outliers of over 10% may well not be acceptable. There should be further studies regarding the measurements of bony landmarks for width to increase accuracy.
One other point should be noted. Practically, in imaging studies of the meniscus-deficient knee, radiographic imaging or MRI is used to estimate meniscal size based on an established anatomic relation between the tibial plateau and the meniscus, which is then compared with donor cadaver measurements of the meniscus obtained by the tissue bank. 8,9,15 Because of a lack of a standardized protocol for meniscal measurement, tissue banks employ their own protocols to determine meniscal size, based on internally derived, unpublished, and often proprietary data. 15 In surgical practice of meniscal allograft transplantation, it is common to interpret the desired meniscal size by measuring the width or the length alone, not simultaneously. The relation between the width and the length, as shown in our values of anatomic measurements, has poor linear correlation (R 2 = .425, P = .241). It is therefore important to measure both the width and the length and prepare the allograft for proper sizing.
The measurement error of the measuring tool should be discussed. The measurement accuracy of the manual Vernier caliper was 0.05 mm, whereas the dimensions of the lateral meniscus were 29.2 ± 3.8 for the width and 32.3 ± 3.3 for the length. Accuracy was defined as those measurements that fell within 10% of each meniscal dimension, and 10% refers to about 2.5 to 3.5 mm. Consequently, large dimensions are more precise, and small dimensions may hold errors. Despite relative possibilities of variability, the measuring tool was acceptable, with high intraclass correlation coefficient values (Table 1).
Limitations of the study might be found in the demographic data of our specimens. First, all our specimens were from Asian patients with a mean age of 74.1 years. Second, even with strict indication of mild to moderate degenerative changes of the examined tibia plateaus, osteoarthritic change—including medial tibia depression and osteophyte formation—could have affected the measurements. Third, there might be bias as a result of age, given that meniscus transplantation is performed in young patients. Another limitation is the relatively small number of examined samples. However, the accuracy of the described radiographic method was statistically significant, and we have no reason to doubt the method or expect that increased numbers of tested specimens would result in less accuracy. The most important limitation is that clinical results are lacking as based on the mentioned measuring method. Meniscal allograft transplantation study with long-term follow-up is necessary.
Further study regarding the mentioned radiographic measuring method of lateral meniscus should be undertaken with the young cadavers and ipsilateral/contralateral MRI. Radiographic study regarding the medial meniscal measurements should also be undertaken.
Footnotes
Acknowledgements
We thank Ms Min-Jung Lee for her assistance with the statistical assessment of the data and the illustrations. We also thank Mr Jai-Hoon Yoo and Ms Young-Ok Woo for their assistance.
The authors declared that they had no conflicts of interest in their authorship and publication of this contribution.