
Abstract
Keywords
The posterior cruciate ligament (PCL) is the primary knee joint stabilizer and the principal restraint of posterior tibial translation. 14,18,23,24 Cases with PCL deficiency typically have posterior tibial sagging and knee instability. Definitive treatment for PCL injury remains controversial. Surgical reconstruction of the PCL is usually indicated in a PCL-deficient knee with symptomatic instability after rehabilitation. 14,22,23 Long-term results for various techniques with different grafts had remained unpredictable for PCL reconstruction. 19,24 Although controversy still exists for the optimal method of PCL deficiency, improved results after PCL reconstruction have been shown in recent studies. 2,16,17
Anterior cruciate ligament (ACL) reconstruction using semitendinosus and gracilis tendons with femoral knot/press-fit fixation without hardware was first proposed by Paessler and Mastrokalos. 26 This technique does not require hardware fixation; fixation is close to the native ACL attachment site, potentially resulting in enhanced healing due to optimal ample graft and bone contact. 25 This also prevents a windshield-wiper effect and synovial fluid ingress into the femoral tunnel. 25 A biomechanical study showed superior results when comparing this method with those that use hardware. 15
To enhance tendon-bone healing in ACL reconstruction, a periosteum-enveloped hamstring tendon was previously applied, and it achieved promising outcomes. 4 Because of its multipotent mesodermal cells forming osteogenic and chondrogenic tissue, a periosteum-enveloped hamstring tendon graft theoretically attains superior tendon-bone healing. 5
This study presents an arthroscopically assisted PCL reconstruction using femoral knot/press-fit technique with a periosteum-enveloped graft in tibial tunnel. We evaluated the results of patients with PCL ruptures who underwent PCL reconstruction using this unique technique.
Patients and Methods
From July 2003 to August 2007, 33 adult patients with isolated PCL reconstruction were enrolled in the study. They were surgically treated with non-hardware PCL reconstruction using femoral press-fit technique with periosteum-enveloped hamstrings tendon autograft on the tibial side. During the same period, another 30 patients were treated for PCL injury in our institute: 4 patients had combined medial collateral ligament injury and 26 had combined posterolateral complex injury. These patients were excluded from this study, to evaluate the PCL reconstruction results for isolated PCL tear with no other ligamentous injury. Before operation, we explained to patients the advantages, disadvantages, and technical difficulties of this hardware-free technique. All patients agreed to receive this procedure. The prospective data were retrospectively reviewed. The reviewing process was approved by Institutional Review Board of Wan-Fang Hospital.
The indication for PCL reconstruction in this manner was symptomatic PCL rupture with a positive posterior drawer test of at least 2+ (>1 cm). For patients with a 3+ drawer test (>1.5 cm), PCL reconstruction was immediately suggested. For those with a 2+ drawer test (>1 cm), 3 months of nonoperative treatment focusing on quadriceps strengthening was recommended. Only in those with unrelieved symptoms was PCL reconstruction suggested. In this study, there were originally 19 patients with a 2+ drawer test; after rehabilitation, 7 patients (36.8%) with unrelieved symptoms received PCL reconstruction, and the other 12 patients (63.1%) did not receive surgery.
Preoperatively, all patients were evaluated according to the International Knee Documentation Committee objective and subjective rating scale, as well as the Tegner and Lysholm rating scales. 9,20,29 Radiologic stability was evaluated by performing an instrumented laxity test using a Telos device (Telos Stress Device, Austin & Associates, Fallston, Maryland) at 90° of knee flexion and with a 150-N posterior load to the anterior aspect of tibia 10 cm distal to the medial joint line.
Surgical Techniques
Technique for Harvesting the Periosteum, Gracilis, and Semitendinosus Tendons
The patient was placed on an operating table in the supine position. After diagnostic arthroscopy, a horizontal incision of about 3 cm was made from 1.5 cm medial to the tibial tubercle, extending distally to harvest the graft and periosteum. The sartorius fascia, encountered after dissection, carried down through the subcutaneous tissue. The underlying semitendinosus and gracilis tendons were harvested using a tendon stripper, with the knee flexed and with traction applied on the grasping suture.
To harvest the periosteum, the subcutaneous soft tissue and fascia were split, exposing the anterior tibia distal to the pes anserinus. A 2- × 3-cm periosteum flap was harvested, which was divided into 2 flaps, each 2.0 × 1.5 cm.
Graft Preparation
The tendons were gently freed of muscle tissue at a workstation. The ends of each tendon were tied together in a simple knot. These knots were maximally tightened under cyclic manual loading. The knots were sutured with 4 to 5 stitches using No. 2 Ethibond (Ethicon, Somerville, New Jersey). Two 5-mm strips of Mersilene tape (Ethicon, Norderstedt, Germany) were passed around the knotted and looped end of each graft. For measuring of the diameter, the loops were then pulled, one after the other, through a measuring template in 1.0-mm site increments. To distinguish between the loops, Mersilene tapes for the semitendinosus tendon were marked, and the tape for the gracilis tendon remained unmarked.
The loop length after knotting should be equal to the bottleneck thickness, about 5 to 6 mm; plus the intra-articular graft length, about 35 to 40 mm; and the length in the tibial tunnel, about 30 to 35 mm. So ideally, the loop length after knotting totaled about 70 to 75 mm for the semitendinosus tendon and about 75 to 80 mm for the gracilis tendon. The gracilis loop must be longer than the semitendinosus tendon because the gracilis tendon knot will be proximal to the semitendinosus knot. Then, intra-articular portions of the graft between femoral and tibial openings were marked.
The previously harvested periosteum was securely wrapped and sutured around the tendon with a 3-0 Vicryl suture at the place in which the tendon graft neared the tibial tunnel opening (about 40-45 mm from knotted end) (Figure 1).
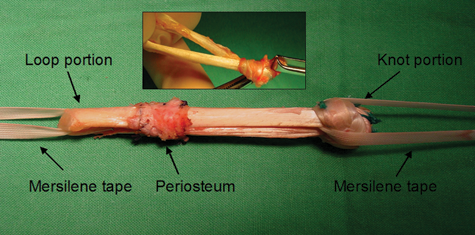
The ends of each tendon were tied together in a simple knot. The knot was sutured with 4 or 5 stitches using No. 2 Ethibond. The harvested periosteum was wrapped and sutured around the tendon.
Femoral Bottleneck Tunnel Preparation
Under arthroscopic visualization, the PCL disrupted stump was first debrided. The femoral remnant of the ligament was preserved where possible and only partially removed to improve visualization.
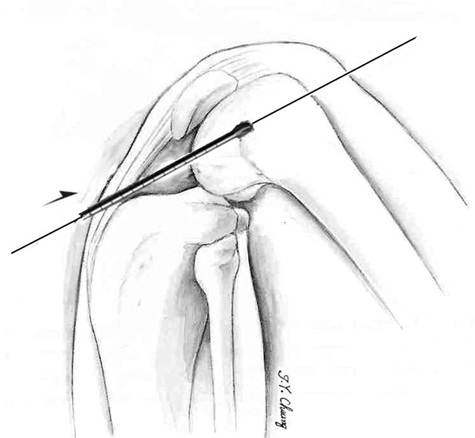
The knee was then flexed to 125°. Using an arthroscope inserted in the anteromedial portal, the surgeon passed a 2.2-mm Kirschner wire through the anterolateral portal and located it in the anterior portion of the PCL footprint at its femoral insertion. The goal of this procedure was to reproduce the anterolateral component of the PCL. The tip of the Kirschner wire was positioned over the anterior portion of the PCL femoral footprint, 10 mm from the articular edge of the medial condyle. The Kirschner wire was then advanced to the skin level and centered on the medial cortex of the medial femoral condyle. With use of the tip of Kirschner wire as a guide, a 2-cm longitudinal incision was made at the center of the outer surface of the medial femoral condyle. The vastus medialis obliquus was retracted superiorly, and the medial retinaculum was incised after the skin incision.
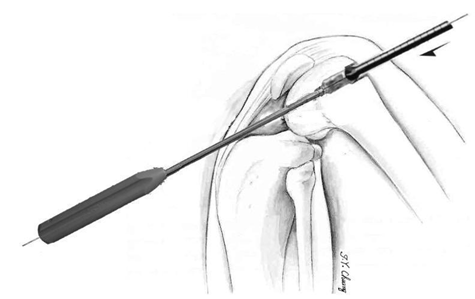
Under arthroscopic visualization, the Kirschner wire was overdrilled with a cannulated reamer from the anterolateral portal, matching the diameter of the 2 tendon parts of the periosteum-enveloped loops (commonly, 8-9 mm) (Figure 2). The cannulated reamer was reamed to a depth of 10 to 15 mm.
Under arthroscopic visualization, the Kirschner wire was overdrilled with a cannulated reamer from the anterolateral portal, matching the diameter of the 2 tendon parts of the periosteum-enveloped loops (commonly, 8-9 mm).
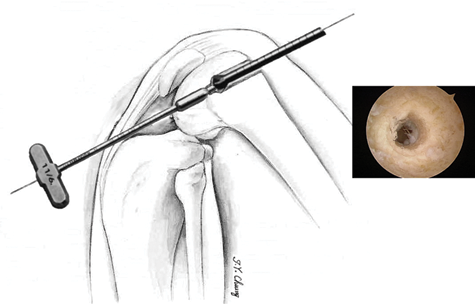
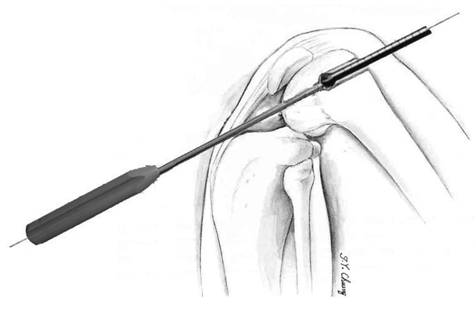
A stepped impactor 6/11 mm (barrel diameter, 11 mm; offset diameter, 6 mm) (Richard Wolf, Knittlingen, Germany) was inserted through the anterolateral portal. The 6-mm offset was stuck into the tunnel and held steadily. Under the guide of prepositioned Kirschner wire, the femoral tunnel was then created by the cannulated reamer. Starting outside, the tunnel was overreamed and stopped at the stepped impactor tip (Figures 3 and 4). Then, the reamer size was increased to match the diameter of knotted portion of the graft (usually to 13-14 mm). If the stepped impactor was unavailable, a cannulated handle could be used instead (2.8-mm-diameter handle of Corkscrew Suture Anchor, Arthrex, Inc, Naples, Florida) (Figures 5 and 6). Excess soft tissue and bone debris were removed from the tunnel. The edge of the articular opening of the femoral tunnel was smoothed by a rasp. A bottleneck-type tunnel was created; the tunnel integrity was then confirmed under arthroscopic visualization.
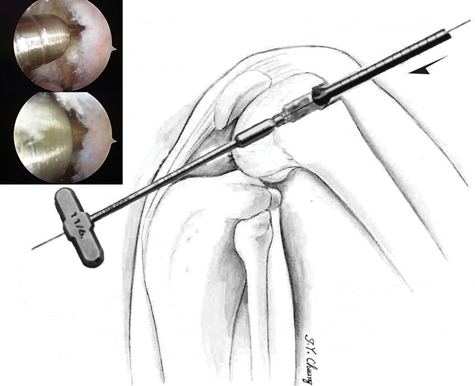
A stepped impactor was inserted through the anterolateral portal. The 6-mm offset was stuck into the tunnel and held steadily.
Under the guide of prepositioned Kirschner wire, the femoral tunnel was then created by the cannulated reamer. Starting outside, the tunnel was overreamed and stopped at the stepped impactor tip.
If the stepped impactor was unavailable, a cannulated handle could be used instead.
Starting outside, the tunnel was overreamed and stopped at the cannulated handle tip.
Tibial Tunnel Preparation
Under arthroscopic visualization, a supplemental posteromedial portal was created under direct visualization. After the tibial footprint was identified, an arthroscopic drill guide for the tibial tunnel was inserted through the anteromedial portal and directed over the distal and lateral portion of the tibial footprint of the PCL attachment. The drill angle guide was adjusted to 50°. After the tibial guide pin was placed, the tibial tunnel was then reamed with an 8- or 9-mm cannulated reamer, depending on the diameter of the 2 tendon parts of the periosteum-enveloped loops. The edge of the articular opening of tibial tunnel was also smoothed by a curved rasp. A looped steel wire was passed outside-in through the tibial tunnel and pulled by a Kelly hemostat outward from the anteromedial portal. Finally, this looped steel wire was passed inside-out through the femoral tunnel externally by a Kelly hemostat.
Graft Passage
The Mersilene tapes on the 2 grafts were secured to the prepositioned looped steel wire. To avoid tearing out of the grafts’ periosteum, the wire and tapes were gently and carefully drawn through the medial aspect of the knee through the intercondylar notch and out to the entrance of the tibial tunnel. The gracilis loop with the thin knot followed the semitendinosus loop. The 2 loops were pulled firmly. A sudden jerk indicated that the semitendinosus knot had reached the step in the tunnel—the bottleneck. Before fixing the tibial side, the knee was manipulated through a range of motion 20 times. Several flexion and extension cycles were performed for stress relaxation of the viscoelastic properties of the tendon graft. To anchor the knots, maximum traction was applied to both loops while the knee was fully flexed. Moreover, the graft was checked arthroscopically to ensure proper placement of the graft and no impingement of the ACL.
Fixation of Tibial Site
A 4.5-mm drill hole was made 1 cm distal to the tibial end of the tunnel. A bone bridge was created by tunneling under the bone with a right-angle clamp. A No. 2 Ethibond suture was passed from the tibial tunnel opening by this right-angle clamp. The Mersilene tapes were separated and secured to the No. 2 Ethibond. The Mersilene tape strips were pulled under the bone bridge by this No. 2 Ethibond.
The knee was then flexed at a 70° angle, and an anterior drawer force was applied to the proximal tibia. The normal step-off should be recovered between the medial femoral condyle and the medial tibial plateau after manual reduction. Maximum traction was exerted on the Mersilene tapes, and the semitendinosus tape ends were first tied with 4 knots. Stability was confirmed manually; then, the tapes of the second loop (gracilis) were tied using the same procedure (Figure 7).
A sterile dressing was applied after closure of the incision. The knee was then placed in a knee brace and locked in full extension.
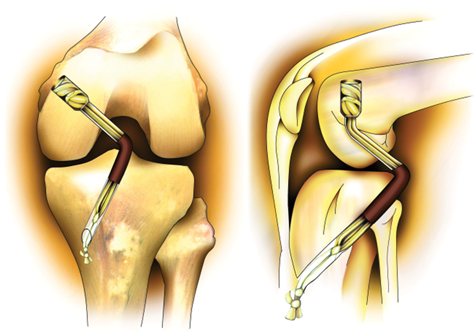
The Mersilene tape strips were pulled under the bone bridge with No. 2 Ethibond. Maximum traction was exerted on the Mersilene tapes, and the semitendinosus tape ends were first tied with 4 knots. Stability was confirmed manually; then, the tapes of the second loop (gracilis) were tied.
Postoperative Rehabilitation
A pillow was placed underneath the tibia while the patient was resting to support posterior subluxation of the tibia. Full weightbearing exercise was allowed as tolerated with the brace locked in full extension. A brace was used for 3 months. The knee was fixed in extension for 4 weeks. At 4 weeks, protected range of motion was allowed from 0° to 60°. At 8 weeks, range of motion was progressed to 90°. At 12 weeks, the brace was unlocked, and establishing a normal gait was stressed. Closed chain kinetic exercise was also initiated. Finally, the patient was allowed to return to normal daily activities after 6 months and to sporting activity after 9 months (Figure 8).

Anteroposterior and lateral radiographs demonstrated the femoral and tibial tunnel without hardware.
Follow-up Assessment
Outcome assessments were standardized and conducted prospectively by research assistants to effectively audit the results of the procedures. Clinical evaluations of knee function and stability were performed preoperatively and last follow-up after more than 2 years postoperatively. All the results of these assessments were rated according to the guidelines of the International Knee Documentation Committee. 9 Patients were assessed with the following criteria: patient subjective assessment, presence of any symptoms, activity level, range of motion, degree of laxity, patellofemoral crepitus, donor site morbidity, radiographic findings, and functional test. Tegner score was used to evaluate the activity level of the preinjury, preoperative, and postoperative periods. 29 Lysholm knee score was used to evaluate subjective symptoms, including presence of a limp, use of support, evidence of joint locking, knee instability, joint pain, swelling, and impaired squatting and stair-climbing ability preoperatively and postoperatively. 20
Radiologic stability was also evaluated by performing an instrumented laxity test using a Telos device (Telos Stress Device, Austin & Associates) at 90° of knee flexion and with a 150-N posterior load to the anterior aspect of tibia 10 cm distal to the medial joint line.
Thigh atrophy was defined as the difference in thigh circumference between the operated and nonoperated knee at a point 10 cm proximal to the superior pole of the patella. The Cybex 340 dynamometer (Cybex, New York, New York) was used to measure extensor muscle strength. Peak extension torque and side-to-side ratio were measured.
Statistical Analysis
The Wilcoxon signed rank test was used to compare Lysholm scores and ligament laxity measurements between preoperative and follow-up measurements. The level of statistical significance was set as P < .05.
Results
Twenty-nine patients with complete follow-up documentation for a minimum of 2 years were included in the outcome analyses. Four patients could not complete regular follow-up evaluation because of a move abroad (n, 1), a move to another city (n, 1), or other trauma that made assessment difficult (n, 2). Other trauma included a contralateral femoral shaft fracture (due to another motorcycle accident 13 months after PCL surgery) and an ipsilateral open ankle fracture (after another motorcycle accident 18 months after PCL surgery). The mechanisms of injury included 17 motorcycle accidents, 6 motor vehicle accidents, 3 falls on the knee, and 3 sports injuries. There were 20 men and 9 women, and the mean age at the time of surgery was 31.5 years (range, 18-45 years). The interval between injury and operation was 2 to 25 months, with a mean of 4.3 months. There were 16 patients (55%) who accepted surgery from 4 weeks to 3 months after injury and 11 (38%) who accepted surgery from 3 months to 1 year after injury. Average follow-up time was 35.4 months (range, 24-60 months).
Eleven knees had combined meniscal tears (6 medial, 5 lateral). Meniscus repair was performed in 2 cases and partial meniscectomy in 9 cases. Articular cartilage damage was identified in 4 patients. For femoral chondral defects of less than 2 cm2, microfracture was performed. For patients with partial-thickness chondral lesion, abrasion chondroplasty was performed. Three patients underwent microfracture procedures, and one received abrasion chondroplasty to smooth irregular surfaces.
Tegner Score
Preinjury, preoperative, and postoperative activity levels were graded according to the Tegner scoring system. The average preinjury score was 5.9 (range, 3-9), decreasing to 2.9 preoperatively (range, 2-5) and increasing to 5.2postoperatively (range, 2-9). Among 11 patients participating in competitive sports (preinjury score >6), 9 (81%) returned to their preinjury scores after surgery during the follow-up. There were 2 judoists and 1 rugby player, who suffered a PCL injury during a game. These 3 athletes returned to their competitive sports about 1 year after surgery.
Lysholm Knee Scores
Preoperative and final follow-up Lysholm scores averaged 58.5 ± 5.2 (range, 46-70) and 94.2 ± 4.1 (range, 63-98), respectively. Twenty-seven patients (93.1%) achieved good or excellent results; 1 was graded as fair (73 points); and 1 had poor results (63 points) (Table 1). There is significant statistical difference in Lysholm scores between preoperative and final follow-up evaluation (P < .01, Wilcoxon signed rank test).
Lysholm Knee Scores
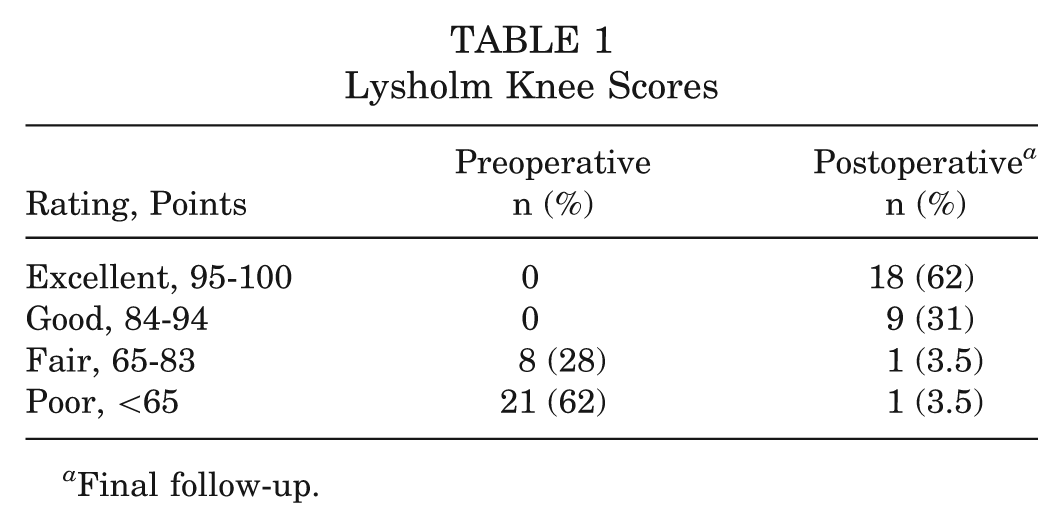
Final follow-up.
International Knee Documentation Committee Scores
Knee Function by Patient Subjective Assessment
Preoperative assessment showed that, by their self-assessment, 11 patients (38%) had an abnormal status and 18 (62%) had severely abnormal status. At final follow-up after reconstruction, 21 patients (72%) subjectively rated their knee function as normal and 6 (21%) as nearly normal.
Symptoms
Two patients (7%) reported pain during moderate or strenuous activities, and 1 (3.5%) reported swelling during moderate or strenuous activity. Moreover, 2 patients (7%) displayed symptoms of partial giving way during moderate or strenuous activities, and 1 (3.5%) reported occasions of full giving way during moderate or strenuous activities.
Range of Motion
At the last follow-up, 27 (93%) patients were rated as normal status. One patient (3.5%) with a 12° flexion deficit and one (3.5%) with a 5° extension deficit were rated as nearly normal status.
Ligament Laxity
All the patients received stress radiography evaluation to evaluate the posterior knee laxity. Preoperatively, the average posterior displacement using stress radiography was 13.7 ± 2.1 mm (7 to 15 mm). The average posterior displacement at last follow-up was 4.8 ± 1.1 mm (3 to 9 mm). There was a significant difference between preoperative and postoperative evaluation (P < .01) (Table 2).
Posterior Knee Instability Before and After Reconstruction
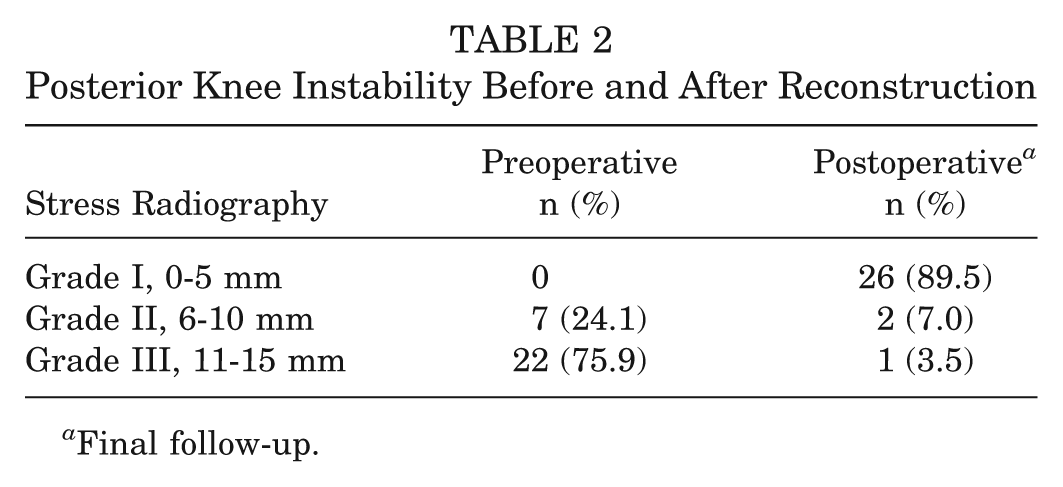
Final follow-up.
Activity
Regarding preinjury activity level, 20 patients participated in strenuous and moderate activities. After injury, 21 were able to participate in only light or sedentary activities. At last follow-up, 26 patients (89.7%) returned to the same preinjury daily activity and sports activity. Two judoists and 1 rugby player returned to the competitive activity 1 year after surgery.
Patellofemoral Crepitus
Patellofemoral crepitus with mild pain was noted in 1 patient, and patellofemoral crepitus with moderate pain occurred in 1 patient.
Donor Site Morbidity
Twenty-seven patients (93%) had no residual discomfort at the donor site. Two (7%) sustained some numbness or irritation at the donor site.
Radiographic Findings
Normal radiography in the joint space was noted for 28 patients (96.5%). One patient (3.5%) was noted to have minimal deterioration on radiographs.
Functional Test
Twenty-two patients (76%) achieved a single-legged hop distance on the injured leg that was 90% or more of that achieved with the noninjured leg. Five patients (17%) achieved a distance of 76% to 89%, and 1 patient (3.5%) could only achieve hops of less than 50% of the distance.
Overall Rating
Overall, 26 patients (89.7%) were assessed as normal or nearly normal according to International Knee Documentation Committee criteria (Table 3).
International Knee Documentation Committee Scores After Minimum 2 Years Postoperatively a
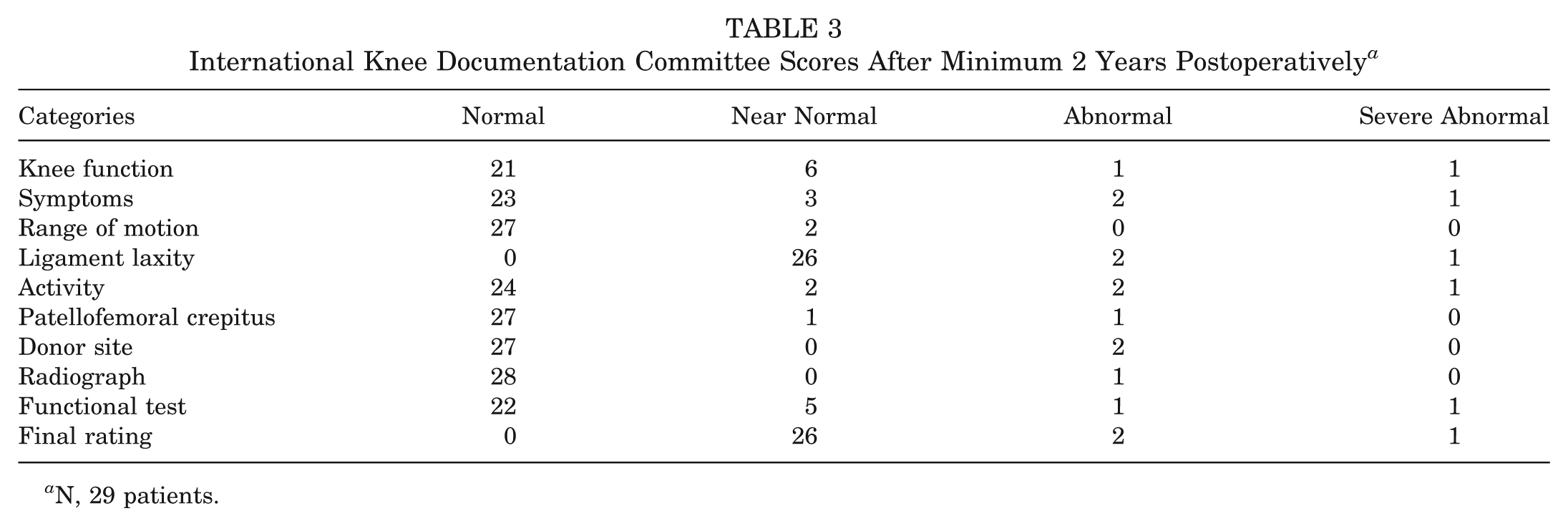
N, 29 patients.
Thigh Muscle Atrophy and Muscle Strength
Twenty-three patients (79.3%) revealed less than 10 mm of difference in thigh circumference between their reconstructed and nonreconstructed limbs. Six patients had more than 10 mm of difference. Cybex dynamometer studies revealed that 21 patients (72%) achieved recovery of the extensor muscle strength in the reconstructed knee to >90% of normal knee strength, and 6 (21%) patients recovered to 80% to 90%. A statistically significant difference by the Wilcoxon signed rank test existed in thigh girth difference and extensor strength ratio before and after reconstruction (Table 4).
Thigh Muscle Atrophy and Extensor Muscle Strength a
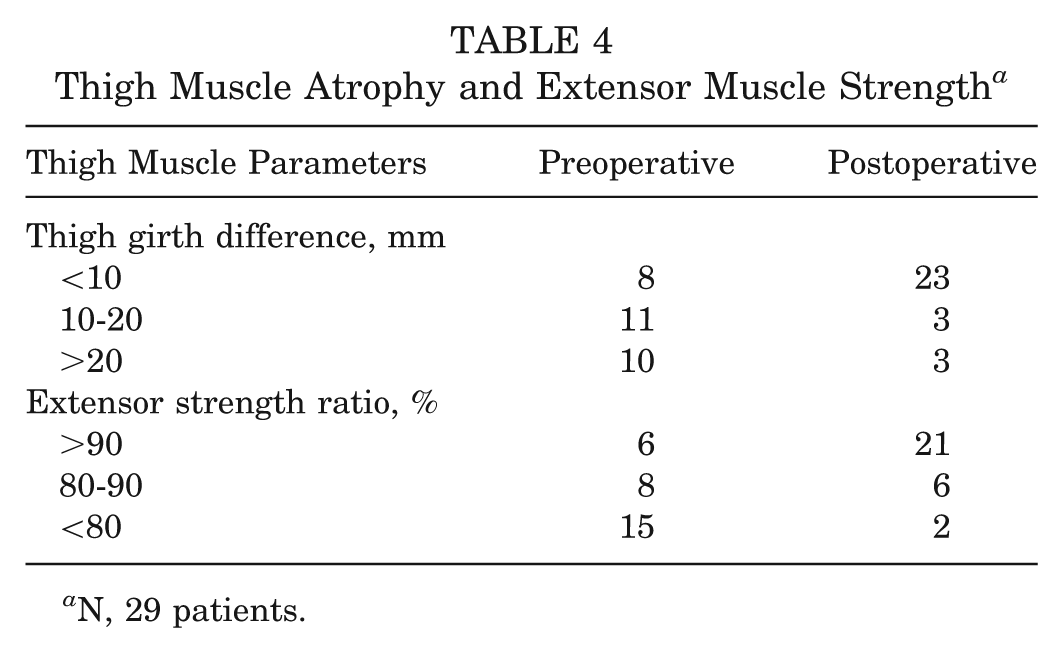
N, 29 patients.
Complications
One patient had superficial wound infection at the surgical incision after operation, which was resolved after oral antibiotic use for 1 week. One complained of numbness around the original tibial incision. The patient with a poor result was a 24-year-old man who sustained persistent knee pain, frequent knee instability during daily activity, and a side-to-side difference of 14 mm. This patient sustained graft rupture according to MRI examination.
Discussion
Although clinical and scientific research continues to be the focus in PCL reconstruction, controversy remains because a procedure that fully restores posterior stability is lacking. Surgical options for PCL reconstruction include arthroscopic transtibial reconstruction, double-bundled reconstruction, and arthroscopically assisted tibial inlay reconstruction. Graft options are also controversial and include autologous bone–patellar tendon–bone, quadriceps tendon-bone, hamstring tendons, and allogenic Achilles tendon or bone–patellar tendon–bone grafts. #
The outcome of the transtibial tunnel method for PCL reconstruction with hamstring tendons may be affected by the following factors: uncertain tendon-bone healing, undetermined windshield wiper effect between tendon and tunnel, unknown effect by femoral turn of graft, and use of different fixation devices. Furthermore, high local tissue stresses borne by the graft as it passes around the acute angle over the posterior tibia can generate graft abrasion, thinning, and permanent graft elongation, which is in turn manifested by increased posterior knee laxity. 1 Although an inlay technique can avoid the stress effect of an acute turn, this technique has the disadvantages of an unsightly scar after posterior arthrotomy, long surgical time, and a steep learning curve. 6-8,18
For ACL reconstruction, knots with the press-fit technique for the femoral fixation of hamstring tendon grafts were first introduced by Paessler and Mastrokalos. 26 This technique, which was used in 915 patients, showed a low rate of postoperative morbidity. Paessler and Mastrokalos 26 claimed that “waterproofing” of the bone tunnels led to less postoperative bleeding and swelling. There was no widening of the femoral tunnels and little widening of the tibial tunnels. The femoral fixation of hamstring grafts was close to the insertion site of native ACL, which is biomechanically sound and avoids the bungee effect. 25,26 Additionally, this approach is hardware-free, thereby reducing the use of expensive devices and avoiding problems such as allergic reaction, artifacts in MRI, and complications during revision surgery. 25,26
In a previous biomechanical study for ACL reconstruction, a robotic/universal force-moment sensor testing system was used by Kilger et al 15 to compare the knee kinematics of the intact, ACL-deficient, EndoButton-reconstructed, and knot/press-fit-reconstructed knee. The load at failure of the knot/press-fit complex was found to be 540 ± 97.7 N, and the stiffness, 37.8 ± 9.6 N/mm. The authors concluded that the knot/press-fit technique is a reliable alternative for the femoral fixation of hamstring tendon grafts in ACL reconstruction. 15
However, this hardware-free technique for ACL reconstruction has problems. A frequently encountered problem is that hamstring graft length is insufficiently long. Special instruments, such as a complete set of stepped impactors, were required to create a bottleneck femoral tunnel. Nevertheless, widening of the tibial tunnel in a long-term follow-up of ACL reconstruction occurred clinially. 26
Our technique combined a knot/press-fit femoral fixation to PCL reconstruction with a periosteum-enveloped hamstring tendon to fill the tibial tunnel opening. Thus, the femoral tunnel opening is filled with tendon knots, and the tibial tunnel opening is filled with the periosteum-enveloped tendon. This dual waterproof construction can prevent some synovial fluid from entering both bone tunnels, creating a theoretically better environment for tendon bone healing. Intensive contact between the tibial tunnel and periosteum-enveloped graft introduces quick and complete graft incorporation; this phenomenon also occurs between the femoral tunnel and graft knots. Additionally, the periosteum contains multipotent mesodermal cells that form osteogenic and chondrogenic tissue, which is in turn beneficial for tendon-bone healing. 5 Periosteum has an added advantage in decreasing the tendon abrasion that occurs over the posterior tibia and the effect of acute turns.
The short length of the hamstring tendon was noted in the technique. Although not confirmed, the graft length does not appear to affect outcomes if good initial fixation and improved tendon bone healing are achieved. Further biomechanical and histologic investigation should be conducted to elucidate this issue. When a complete set of specially designed instruments is not available, a femoral bottleneck tunnel can be created using traditional instruments for ligament reconstruction in this revised procedure.
The clinical results of various PCL reconstruction methods were reported in several articles. ** But there were few studies regarding the outcomes of PCL reconstruction for isolated PCL injury. According to the International Knee Documentation Committee scale for PCL reconstruction after isolated PCL injury, the percentage of normal and nearly normal results were 61% in the study of Garofalo et al 11 ; 79% in the study of Mariani et al 21 ; 94.7% in the study of Chen and Gao 2 ; 100% in the study of Sekiya et al, 27 considering activity level of acute and subacute group; 85% and 91% in the study of Chen et al 3 with quadriceps tendon and hamstring tendon autograft, respectively; and 60% in a 6- to 12-year follow-up study of Hermans et al. 13 The clinical outcomes in this study after hardware-free PCL reconstruction introduced a satisfactory return of function and improvement in symptoms and were in line with these reports in the literature.
Irrespective of the fixation method cited in this study, favorable results were affected by other important factors, including a technically sound single tunnel for anterolateral bundle, an isolated PCL injury, and early reconstruction of grade 3 posterior drawer cases. In the studies of Hermans et al 13 and Harner et al, 12,27 acute and subacute reconstructions also had statistically significant better subjective outcomes than did chronic reconstructions with regard to the time between injury and surgery.
Certain weaknesses of the present study should be noted—the first of which are the lack of a control group and the relatively small number of patients. However, postoperative recurrence of instability in this selected group of patients was not common, and it would have been impossible to collect a number of patients large enough to randomize into 2 groups. Moreover, this knot/press-fit technique was unique in tibial side fixation, which made it not possible to compare with other techniques with hardware. Second, there was not any objective proof to support some of our claims, such as dual waterproof construction or avoidance of abrasion over the posterior tibial turn. Further histologic study should be conducted to elucidate this point. Third, biomechanical studies have been conducted that show favorable results in only ACL reconstruction; further biomechanical studies should be conducted for PCL reconstruction. Finally, the periosteal envelope should ideally be placed on both the femoral and tibial sides to achieve waterproof construction and increased graft healing. But in this knot/press-fit technique, the amount of periosteum from the incision of the tibial side was not enough to wrap both sides unless the tibial incision had been extended.
Conclusion
Without using hardware, this technique was applied for PCL reconstruction and might be a reasonable alternative to other popular techniques for fixation of the hamstring tendons for PCL reconstruction. This approach needed no hardware and might be beneficial in MRI interpretation and revision surgery. Further histologic and biomechanical research is needed to determine knot/press-fit fixation in the PCL and the potential clinical benefits of using periosteum within the tibial tunnel in PCL reconstruction.