
Abstract
Among athletic populations, ankle sprain is the most common presenting injury, 5,13,14,19,25,30 accounting for 10% to 30% of all single-sport injuries. 3,13,19 Approximately 85% of ankle sprains involve the lateral ligamentous complex (ie, anterior talofibular, posterior talofibular, and calcaneofibular ligament), and the causes of this injury have been well described in the literature. 5,6,11,26,33 In contrast, syndesmotic and medial ankle sprains occur far less frequently and are diagnosed in only 10% to 15% of all ankle sprains 10,15 ; however, syndesmotic and medial ankle sprains have been reported to result in significantly greater time lost to injury and long-term disability. 11,15,17,18,24,31 Although our previous study focused primarily on lateral ankle sprain, 33 there are few data from large-scale (greater than 10 000 person-years at risk) population-based studies with corresponding athlete-exposure data regarding syndesmotic and medial ankle sprain incidence rates (IRs) and the associated risk factors. The purpose of this study was to estimate the rate of syndesmotic and medial ankle sprain injuries and identify risk factors associated with these injuries within the physically active cadet population at the United States Military Academy (USMA). Furthermore, this study will clarify the relationship between sex, level of competition, and type of sport and the incidence rate of syndesmotic and medial ankle sprain within this homogeneous cohort.
Methods
Study Design and Settings
This prospective cohort study was approved by our Institutional Review Board. The Cadet Illness and Injury Tracking System (CIITS) collects illness and injury data for all patient encounters at USMA treatment facilities. Additionally, CIITS provides patient demographic data and military-specific information for epidemiologic analysis. The CIITS database has previously been employed for the study of musculoskeletal injuries 33 and serves as a useful model for public health surveillance and epidemiologic research.
A longitudinal cohort study using injury data extracted from the CIITS was performed to examine the causes of syndesmotic and medial ankle sprain over a 4-year time period between 2005 and 2009 within the cadet population at the USMA. The population for this study included all cadets in attendance during the study period. The USMA cadets are required to meet their service’s physical induction standards when joining the military, which excludes from service those individuals with certain preexisting medical conditions to include potential causes for chronic ankle instability (eg, inadequate healing, poor rehabilitation, multiple recurrences after primary ankle sprain, heritable connective tissue or other genetic disorder, prior ankle surgery). All cadets are required to participate in intramural, club, or intercollegiate sports in each semester of their USMA attendance. Cadets also participate in Department of Physical Education courses and activities, some of which may be gender-specific, as well as the Army Physical Fitness Test. Mandatory military training occurs throughout the 48-month USMA experience. Furthermore, cadets participate in intensive physical training programs and field-training exercises. Because of USMA requirements, documented attendance is required for cadets at all places of duty to include athletics. Attendance is taken and reported for all sporting events, games, and practices. Exposure data are based on daily attendance data documented for every practice and game at the intramural, club, or varsity sport level. The data are reported on line through the USMA student information system, which then provides the athlete-exposure data for CIITS.
All cadets receive medical care through the closed health-care system at USMA, and all injuries are evaluated through its associated sports medicine and orthopaedic clinics. All injuries resulting in time lost to sports or activity and requiring presentation at a receiving clinic are documented in CIITS at USMA. Diagnoses are made by an orthopaedic surgeon, physician assistant, or certified athletic trainer based on patient history and physical examination. The West Point Ankle Grading System 15 was utilized for diagnosing type and severity of ankle sprain. Syndesmotic ankle sprain was diagnosed based on a history of external rotation or dorsiflexion injury, focal tibiofibular tenderness, positive special testing (external rotation stress test, squeeze test), or radiographic mortise widening. Medial ankle sprain was diagnosed by a history of eversion and dorsiflexion ankle injury, tenderness in the deltoid ligament distribution, and/or pain with passive external rotation. Body mass index (BMI) was calculated based on recorded height and weight.
Data Acquisition and Outcome Assessment
Injury data were extracted from the CIITS database, and any ankle injuries were isolated. Injuries identified as syndesmotic or medial ankle sprains were subsequently analyzed for this study. Incident ankle sprains were defined as primary ankle sprains resulting in any time lost to sport and activity that occurred within the study period. Injuries sustained before the study period were not included as incident ankle sprains in this study. Subsequent repeat ankle sprains were also excluded in the calculation of incidence rates. Primary measured outcomes were the incidence of new ankle sprain per 1000 person-years at risk and the incidence of new ankle sprain per 100 000 athlete-exposures. A person-year or athlete-exposure is a unit expressing the cumulative observation time during which the population is at risk for injury. Person-years were defined as 1 cadet’s year-long exposure to at-risk activity at USMA. Athlete-exposures were defined as 1 cadet participating in 1 sports-related activity session (eg, game or practice). Incidence rate was calculated by dividing the total number of injuries observed in the population by a measure of person-time at risk to injury. While athlete-exposure to injury has commonly been used as a measure of person-time at risk in sports injury research, person-years at risk is a more widely used measure of exposure in population-based epidemiologic studies. 6,23 Data for person-time at risk to injury were collected as precisely as possible following the recommendations of Knowles et al. 23
Time lost to injury was used to evaluate the severity of ankle sprain injuries. Time lost to injury is the period of disability calculated from start and end dates on a standardized cadet medical excusal form, which determines physical limitations imposed by health-care providers for cadets during athletics and other physical training. When the physical profile is discontinued, this marks the full, unrestricted return to athletics and/or physical training irrespective of sport or level of activity. Severity of ankle sprain was measured by the extent of recorded time lost to injury using the definitions set forth by Powell and Barber-Foss 30 : minor (<8 days), moderate (8-21 days), or severe (>21 days).
Statistical Methods and Data Analysis
Using data extracted from the CIITS database, we calculated incidence rates with 95% confidence intervals (CIs) per 1000 person-years at risk and by sex, sport, and level of competition. When evaluating IRs by athlete-exposure, IRs with 95% CIs were also calculated per 100 000 athlete-exposures by sex, sport, and level of competition. Level of competition categories included involvement on an intercollegiate or intramural level. Intercollegiate sport categories included sports with both men’s and women’s athletic teams (basketball, cheerleading, team handball, lacrosse, rugby, soccer, track sports, volleyball), as well as single-gender athletic teams (men’s baseball, football, gymnastics, sprint football [player weight of 172 lb or less], ice hockey, and wrestling; women’s softball). Intramural sport categories include basketball, flag football, biathlon, boxing, combat grappling, football, orienteering, pass-n-go football, soccer, team handball, ultimate frisbee, and wrestling. Incidence rate ratios (IRRs) and respective CIs were calculated between male and female cadets, intercollegiate and intramural athletes, and men’s and women’s intercollegiate athletes involved in selected sports. Chi-square and Poisson regression analyses were used to examine the relationship between the variables of interest and the incidence of syndesmotic and medial ankle sprain. A Student t test was used to examine differences in mean values between groups, while a median 2-sample test was used to evaluate for differences in median values between groups. Analysis of variance and Scheffé post hoc analysis was used to evaluate the difference in BMI among injured and uninjured groups. All analyses were carried out using SAS (version 9.1.3, SAS Institute, Cary, North Carolina) with statistical significance set at P < .05 for all comparisons.
Results
During the 4-year study period, 1206 cadets sustained ankle sprains among an at-risk population of 20 336 person-years for an overall IR of 59.3 per 1000 person-years. Overall, 11.8% of all ankle sprains in the current study involved the syndesmotic or medial ligaments of the ankle. Eighty-five ankle sprains (6.7%) involved the syndesmotic ligaments for an IR of 4.8 per 1000 person-years. Medial ankle sprain accounted for 61 ankle sprains (5.1%), resulting in an IR of 3.5 per 1000 person-years.
Among the cadets with ankle sprains, 46 (54%) with syndesmotic ankle sprains and 45 (74%) with medial ankle sprains had available time-loss data. Severity of syndesmotic ankle sprains was classified as minor (<8 days time lost) in 19 cadets (41.3%), moderate (8-21 days time lost) in 19 cadets (41.3%), and severe (>21 days time lost) in 8 cadets (17.4%). Similarly, medial ankle sprains were classified as minor in 23 cadets (51.1%), moderate in 18 cadets (40.0%), and severe in 4 cadets (8.9%). Syndesmotic ankle sprain resulted in longer time lost to injury (median, 10.5 days; mean, 13.9 days; range, 3-53 days) than medial ankle sprain (median, 8.0 days; mean, 10.7 days; range, 1-38 days) (P = .11).
Sex
During the study, male cadets sustained 73 syndesmotic and 58 medial ankle sprains for respective IRs of 4.9 per 1000 male person-years and 3.9 per 1000 male person-years. Fifteen female cadets sustained 12 syndesmotic and 3 medial ankle sprains for respective IRs of 4.6 per 1000 female person-years and 1.2 per 1000 female person-years. When compared with females, male sex was associated with higher rate of medial ankle sprain (IRR 3.37; 95% CI: 1.05, 10.74), but not of syndesmotic ankle sprain (IRR 1.06; 95% CI: 0.58, 1.95).
Women with syndesmotic ankle sprains had higher average time lost to injury (n = 7; median, 12.0 days; mean, 18.3 days; 95% CI: 7.3, 28.7) than men (n = 39; median, 10.0 days; mean, 13.4 days; 95% CI: 9.5, 17.2). Conversely, men with medial ankle sprains had higher average time lost to injury (n = 42; median, 8.0 days; mean, 11.1 days; 95% CI: 7.18, 13.8) than their female counterparts (n = 3; median, 4.0 days; mean, 5.0 days; 95% CI: 0.9, 9.3); however differences in time loss between men and women failed to achieve statistical significance for both syndesmotic (P = .31) and medial (P = .24) ankle sprains (post hoc power = .367). Similarly, no statistically significant differences were detected by sex and distribution of severity of injury for syndesmotic (P = .16) and medial (P = .19) ankle sprain.
Incidence by Sport
Of all syndesmotic sprains, 81% occurred during sports activity, with 54% sustained during intercollegiate athletics; whereas 64% of medial ankle sprains occurred with sports activity and 38% were sustained during intercollegiate athletics. The IRs of syndesmotic and medial ankle sprain in select intercollegiate sports are listed in Table 1. In intercollegiate athletics, sprint football (52.25), team handball (34.72), soccer (men’s, 30.5; women’s, 6.54), and basketball (men’s, 24.75; women’s, 6.74) had the highest rates of syndesmotic ankle sprain per 100 000 athlete-exposures. Rugby (men’s, 16.56) and gymnastics (men’s, 14.04) had the highest rates of medial ankle sprain per 100 000 athlete-exposures.
Incidence Rates of Syndesmotic and Medial Ankle Sprain in Selected Intercollegiate Sports
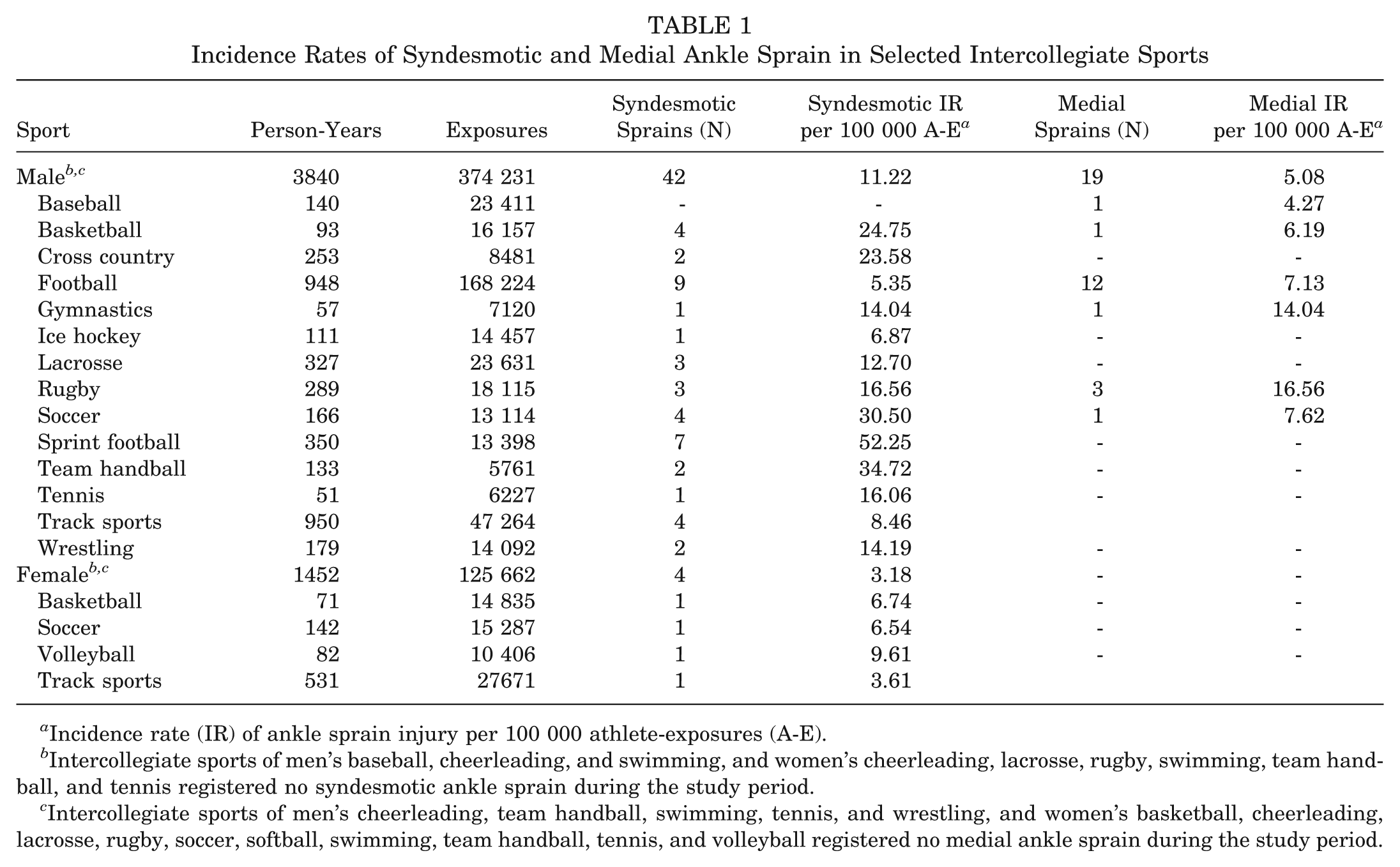
Incidence rate (IR) of ankle sprain injury per 100 000 athlete-exposures (A-E).
Intercollegiate sports of men’s baseball, cheerleading, and swimming, and women’s cheerleading, lacrosse, rugby, swimming, team handball, and tennis registered no syndesmotic ankle sprain during the study period.
Intercollegiate sports of men’s cheerleading, team handball, swimming, tennis, and wrestling, and women’s basketball, cheerleading, lacrosse, rugby, soccer, softball, swimming, team handball, tennis, and volleyball registered no medial ankle sprain during the study period.
Overall, the syndesmotic ankle sprain IRR in male athletes participating in all intercollegiate sports was over threefold greater than that of female participants (IRR 3.53; 95% CI: 1.26, 9.83) Similarly, when evaluating only those sex-matched athletes involved in intercollegiate basketball, soccer, and track sports, men also had higher rates of syndesmotic sprain than their female counterparts (IRR 3.53; 95% CI: 0.75, 9.90), although this did not reach statistical significance. A further detailed subanalysis of syndesmotic ankle sprain IRR by sport and sex was unable to be performed because of the low numbers of syndesmotic and medial sprains when they are categorized by each individual sport.
Level of Competition
Intercollegiate athletes, when compared with intramural athletes, had significantly higher syndesmotic ankle sprain IRRs per 1000 person-years (IRR 20.95; 95% CI: 8.95, 59.05) and per 100 000 athlete-exposures (IRR 2.41; 95% CI: 1.03, 5.65). Additionally, intercollegiate athletes, when compared with intramural athletes, had a sevenfold increased IRR of medial ankle sprain per 1000 person-years: 7.42 (95% CI: 3.12, 17.64). However, when expressed according to athlete-exposure, there were no significant differences between intercollegiate and intramural athletes in IR of medial ankle sprain (Table 2).
Incidence Rate Ratios of Syndesmotic and Medial Ankle Sprain Among Intramural and Intercollegiate Athletes
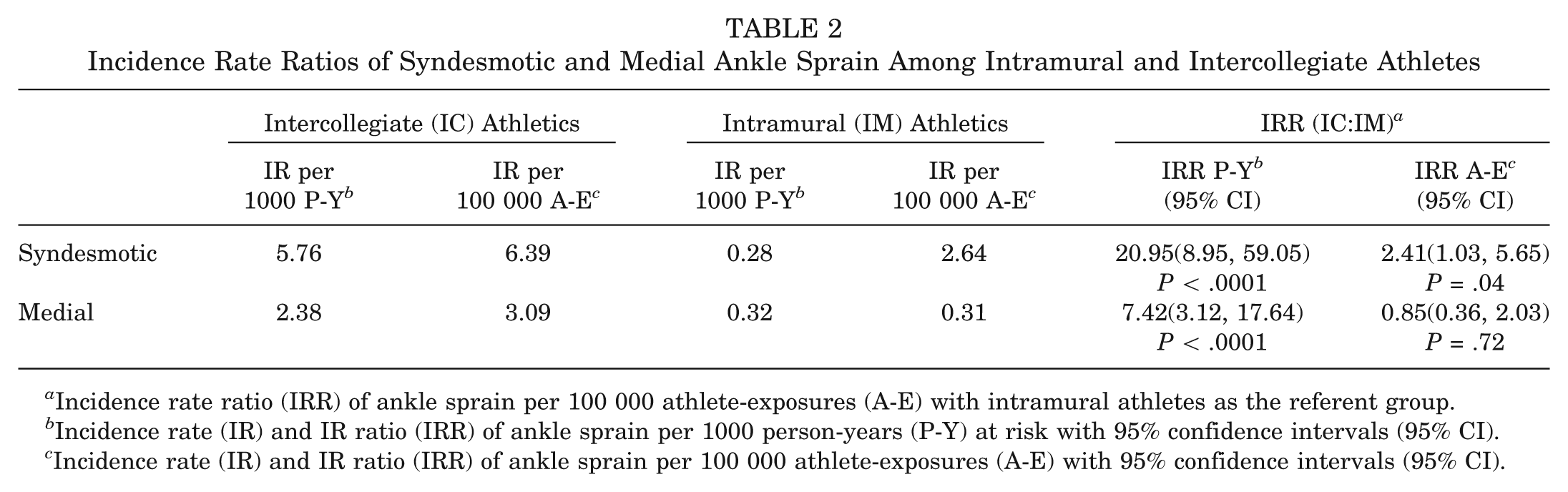
Incidence rate ratio (IRR) of ankle sprain per 100 000 athlete-exposures (A-E) with intramural athletes as the referent group.
Incidence rate (IR) and IR ratio (IRR) of ankle sprain per 1000 person-years (P-Y) at risk with 95% confidence intervals (95% CI).
Incidence rate (IR) and IR ratio (IRR) of ankle sprain per 100 000 athlete-exposures (A-E) with 95% confidence intervals (95% CI).
Body Mass Index
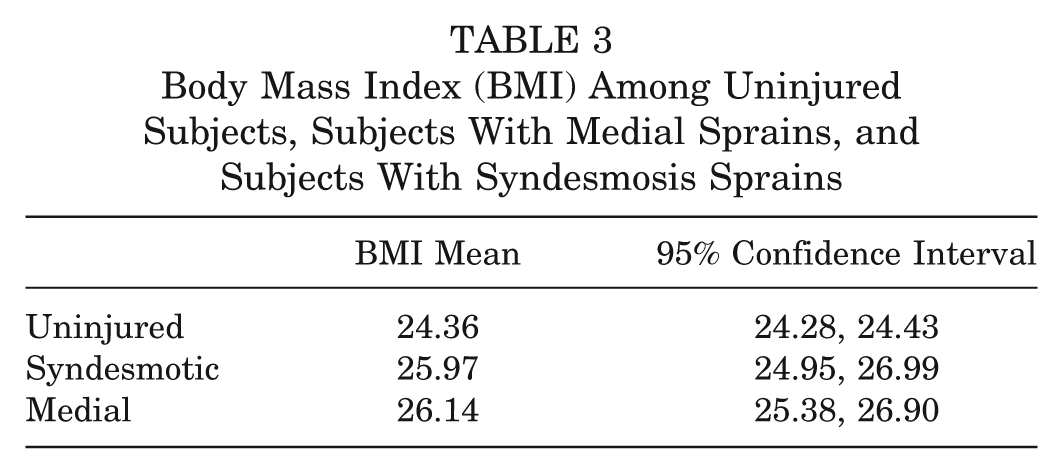
Analysis of variance revealed a significant main effect for BMI by group (F 2,5381 = 24.96, P < .001). Scheffé post hoc analysis revealed that patients with medial (P < .001) and syndesmotic (P < .001) ankle sprains had significantly higher BMI than those who did not sustain ankle sprain injuries (Table 3). The mean difference in BMI between the uninjured and those with medial and syndesmotic ankle sprains was 1.61 and 1.79, respectively. Inadequate power existed for subgroup analyses by gender.
Body Mass Index (BMI) Among Uninjured Subjects, Subjects With Medial Sprains, and Subjects With Syndesmosis Sprains
Discussion
In this longitudinal cohort study with over 20 000 person-years at risk, we found that sex, level of competition, and athlete-exposure to selected sports were factors associated with sustaining a syndesmotic or medial ankle sprain in USMA cadets. Syndesmotic and medial ankle sprains typically account for 10% to 15% of all ankle sprains. 10,15 In our cohort, syndesmotic and medial ankle sprains accounted for 11.8% of all ankle sprains during the study period, with syndesmotic sprains representing 6.7% and medial sprains accounting for 5.1% of all ankle sprains. As noted above, this is consistent with the available literature 10,15 ; however, no prior studies have formally established the incidence rate of these injuries in active cohorts with associated athlete-exposure data. In the current study, the IR of ankle sprain in the USMA cadet population was 59.3 per 1000 person-years, with syndesmotic and medial ankle sprains accounting for 4.8 and 3.5 per 1000 person-years, respectively.
Our results revealed an overall increased risk for sustaining medial ankle sprain injury in male cadets when compared with their female counterparts, with an IRR of 3.37 (95% CI: 1.05, 10.74). However, no differences were noted among intercollegiate athletes. Conversely, while no statistically significant differences were detected in syndesmotic ankle sprain IR by sex in the overall cadet population, sex was a significant risk factor when considering intercollegiate athletes. When IRs were calculated using athlete-exposure as a more precise measure of person-time at risk, male intercollegiate athletes experienced a three-fold increase in the rate of syndesmotic ankle sprain than their female counterparts. Prior studies have reported a possible association between female sex and lower extremity injury. 4,6,21,22 However, few known studies to date have evaluated the epidemiologic risk factors for syndesmotic and/or medial ankle sprain. Hosea et al 20 reported no statistically significant differences in the incidence of syndesmotic ankle sprain among male and female athletes involved in basketball. Conversely, when considering all male and female intercollegiate sports, male intercollegiate athletes experienced an IR of syndesmotic sprain that was 3.5 times higher than their female counterparts per 1000 person-years. Logically, one would conclude that this is attributable to the effect of the weight that football injuries, which accounted for 35% of all syndesmotic sprains, have on the overall incidence rates for males. However, when considering those intercollegiate sports with equal male and female involvement, the male predominance did not reach significance, likely because of the relatively small number of observed injuries in this subgroup analysis. Further large-scale, prospective studies are needed to better clarify the role of sex in syndesmotic and medial ankle sprain, especially in athletic cohorts.
The rates of syndesmotic ankle sprain are variably described with reported cumulative incidence rates from 1% to 16% of all ankle sprains. 10,15,18 To our knowledge, this is the first study to specifically document the rate of syndesmotic ankle sprain incurred by participation in over 15 different intercollegiate sports within a single cohort. In the current study, syndesmotic ankle sprains account for 6.7% of all ankle sprains, with approximately 81% during sports activity and 54% during intercollegiate athletics. Male intercollegiate athletes in sprint football, team handball, soccer, and basketball had the highest IR of syndesmotic ankle sprain, with football accounting for 35% of all syndesmotic ankle sprains in intercollegiate sports. Among female sports, intercollegiate volleyball had the highest syndesmotic ankle sprain IR, followed by basketball and soccer. Previous studies 11,12,18,28,34 have described a higher incidence of syndesmotic ankle sprain during football, ice hockey, wrestling, rugby, and lacrosse, with an external rotation injury the most commonly reported mechanism. 17,28 These high-risk sports involve frequent player-to-player contact and cutting movements that result in significant rotational strain at the ankle and secondary syndesmotic injury.
Furthermore, syndesmotic ankle sprains resulted in an average time loss of 13.9 days (median, 10.5 days; range, 3-53 days), which was higher than time lost to either lateral or medial ankle sprains. Our previous study of lateral ankle sprains in the same cohort resulted in a mean of 8.1 days lost to sport. 33 In the current study, the time lost to injury is on the lower end of that reported in previous studies (range, 13.4-55 days). 12,17,18,28,32,34 This may be a function of limited time-loss reporting as only 46 of 85 (54%) syndesmotic injuries had available time-loss data. Intercollegiate athletics impose significant physical demands because of its high level of competition and greater exposure to at-risk activity. However, only 15 of 46 intercollegiate athletes with syndesmotic ankle sprains (34.7%) had available time-loss data, thus contributing another potential source of sample bias to the calculation of time lost to injury.
We found that BMI was higher in athletes sustaining medial and syndesmotic injuries compared with the uninjured cohort. While this has been reported as a risk factor for lateral ankle sprain, 33 we are not aware of this as a reported risk factor for medial or syndesmotic sprains.
Medial ankle sprain has been the subject of few studies, and little is known about its contributory risk factors. In the current study, medial ankle sprain accounted for 5.1% of all ankle sprains, with 64% of injuries during sports activities and 38% during intercollegiate athletics. Men’s rugby, gymnastics, and soccer had the highest IR of medial ankle sprain. Sprains involving the deltoid ligament most commonly arise from excessive eversion or dorsiflexion, and can occur with both contact and noncontact athletics. In their evaluation of foot and ankle injuries during competitive soccer, Giza et al 16 demonstrated that eversion ankle sprains occurred most commonly during a lateral contact injury to the weightbearing ankle. Similarly, abnormal landing and push-off mechanics may also contribute to medial ankle sprain. Furthermore, Fallat et al 10 indicated that while pure medial or eversion ankle sprains are rare, the deltoid ligament can be involved in up to 32.9% of all ankle sprains. In the current study, medial ankle sprain also resulted in greater time lost to injury than previously reported. 33 However, only 45 of 61 (73%) medial ankle sprains had time-loss data available, and this could similarly limit the interpretation of this result.
The level of competition is commonly implicated as a risk factor for ankle sprain or other lower extremity injury. We found that intercollegiate athletes had over a twofold increased rate of syndesmotic ankle sprain when compared with intramural athletes while controlling for athlete-exposures. To our knowledge, only 1 prior study has attempted to evaluate the role of the level of competition on the IR of syndesmotic ankle sprain. Hosea et al 20 evaluated 1052 ankle injuries among an at-risk population of 11 780 intercollegiate and high school basketball athletes, and showed that male and female intercollegiate athletes involved in basketball incurred a twofold increased risk of ankle injury than their high school counterparts. When considering only syndesmotic ankle injuries, they demonstrated that men and women participating in intercollegiate basketball had a relative risk of 6.29 and 4.20 when compared with their high school counterparts, respectively. However, no statistical analysis was performed and a total of only 14 syndesmotic injuries were recorded. Other studies focusing on the broader incidence of ankle sprain by level of competition have been inconclusive 7,9,27,29 and do not stratify incidence according to lateral, medial, and syndesmotic ankle sprain. The reasons for increased risk of syndesmotic ankle sprain associated with intercollegiate level of competition in this study are likely multifactorial. We propose that higher intensity of competition, more aggressive player-to-player contact, limited rest period, 1 higher match exposure, 2 and greater risk-taking behavior 8 account for this trend with intercollegiate athletics; however, further study is required to clarify the role of these factors and their association with ankle sprain injuries to the syndesmotic and medial ligaments.
The CIITS is an established model for the epidemiologic surveillance of athletic injuries. The strengths of this study include its large, athletic population (greater than 20 000 person-years at risk) and the corresponding athlete-exposure data captured within USMA’s closed health-care system. This closed cohort serves as an ideal setting for the evaluation of the incidence and risk factors for syndesmotic and medial ankle sprain. However, as with any database study, we acknowledge certain inherent limitations. First, we are unable to exclude all cadets with a history of ankle sprain because of limited patient history. To control for recurrence, all cadets with subsequent sprains during the study period were not included in our calculations of incidence, and any cadet with prior recorded sprain during attendance at USMA or antecedent history of ankle instability were excluded at the onset of this study. Second, multiple health care providers were involved in the evaluation and treatment of cadets, as well as the coding of patient encounters in the CIITS. As a result, this may decrease the accuracy of the diagnosis of syndesmotic and/or medial ankle sprain due to limitations in interobserver reliability. Because of the limited number of observed medial and syndesmotic ankle sprains among men and women during the study period, and the degree to which time-loss information was available within the cohort, it is possible that observed differences by sex failed to reach statistical significance because of inadequate statistical power. On the basis of a post hoc power analysis, we would have needed complete time-loss data for 136 men and women with medial and syndesmotic ankle sprains (total N = 544) to attain 80% power. In addition, the time-loss data were incompletely documented and limit the effect of our data. Routine MRI and/or arthroscopy was not used to confirm the diagnosis in this study. Despite these limitations, the data from this longitudinal cohort study represent the first known estimates of the incidence of syndesmotic and medial ankle sprain in physically active and athletic populations and can guide strategies for risk reduction and injury prevention in at-risk groups.
Conclusion
Syndesmotic and medial ankle sprains account for 11.8% of all ankle sprains in a young, athletic population. Male sex, higher level of competition, and exposure to selected sports are important risk factors for syndesmotic and/or medial ankle sprain. The intercollegiate sports of football, team handball, basketball, and soccer have the highest rates of syndesmotic ankle sprain, while intercollegiate rugby, gymnastics, and soccer had the highest rates of medial ankle sprain.
Footnotes
Acknowledgements
The authors thank Julia Bader, PhD for her assistance with statistical analysis. Thanks also to Tim Kelly, ATC, and his staff in the Department of Intercollegiate Athletics at USMA; Ms Karen Peck, ATC, and her staff in the Department of Physical Education at USMA; and LTC Parry Gerber, PT, PhD, and his staff in the Keller Army Hospital Physical Therapy Department for their contributions to the ongoing injury surveillance efforts at USMA. The authors also recognize and thank the cadets at the USMA for their participation in this study and their commitment to serve their nation.
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of Defense or United States government. The authors are employees of the US government.
The authors declared that they had no conflicts of interest in their authorship and publication of this contribution.