
Abstract
The anterior capsulolabral complex including the anterior labrum and the capsular ligaments is an important structure that maintains stability of the shoulder joint. The labrum is attached to the glenoid rim, and the capsule is attached to the glenoid rim and to the glenoid neck. Anterior shoulder dislocations separate the capsulolabral complex from the anterior glenoid rim and glenoid neck. This can become a cause for traumatic anterior shoulder instability. 4
Although surgical procedures and tools including suture anchors have lowered postoperative recurrences, recurrence rates of instability in arthroscopic stabilization are still higher than those for open surgical stabilization. 15,16,18 Recently, Ahmad et al 2 claimed that from the research of the native glenoid insertion of the anterior-inferior capsulolabral complex, double-row repair of the capsulolabral complex re-establishes the native insertional footprint on the anterior inferior glenoid better than a single-row repair. Also, Lafosse et al 20 claimed that with the Cassiopeia double-row technique, a stronger and more stable footprint fixation of the capsulolabral complex seems to be possible, but this research had a very short follow-up.
Many authors advocate specific surgical techniques including repair of the labrum 1 to 2 mm onto the glenoid articular surface or at the articular edge. We do not think that repairing the capsulolabral complex at the glenoid articular surface induces a direct healing at the original footprint but rather a healing at the anterior glenoid bone surface. In re-creating the native structure, there has been a recent report that double-row labral repair techniques are superior to the existing single-row labral repair. 2 Despite the attention that has been paid to restoration of the capsulolabral complex anatomic insertion onto the glenoid, studies that compared the pressurized contact area and mean interface pressure at the anatomic insertion site between a single-row repair and a double-row labral repair have been uncommon.
The purpose of our study was to compare the mean and peak pressure, the contact force, and pressurized contact area at the anatomic insertion site of the capsulolabral complex between a single-row repair and a double-row labral repair technique. We hypothesized that a double-row labral repair will significantly increase the mean interface pressure and pressurized contact area between the capsulolabral complex and the insertion site when compared with a single-row repair technique.
Materials and Methods
Specimen Preparation
Thirty fresh-frozen cadaveric shoulders (mean age, 61 ± 8 years; range, 48-71 years) were used for this study. Institutional review board approval was acquired for the study. Specimens with abnormal bony lesions at the anterior glenoid rim and glenoid neck or specimens with abnormalities in the capsulolabral complex were excluded from the study. Our study did not investigate the anatomic insertion site of the capsulolabral complex microscopically, but all the specimens were classified as Eberly classification 10 type 1, which contains the capsular insertion on both the labrum and glenoid neck. All specimens were from male donors. They were stored at −20°C and thawed for 24 hours at room temperature before dissection. 19,34 The humerus, acromion, and soft tissue were removed, and the glenoid, labrum, and anteroinferior capsulolabral complex were preserved. From the level base of the coracoid process to the 6-o’clock position, the capsulolabral complex was dissected carefully from the glenoid (Figure 1). During the procedure, to minimize movement between the specimen and apparatus, the scapula was firmly fixed with the Ilizarov external fixator system (JOYM Co Ltd, Seoul, Korea) using the half-pins (Figure 2). Throughout the dissection and test, the specimens were protected from dehydration using saline-soaked gauze intermittently.
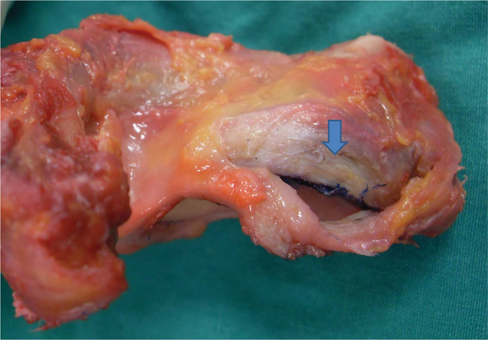
The anterior-inferior capsulolabral complex was carefully dissected off the glenoid. The arrow indicates the capsulolabral footprint.
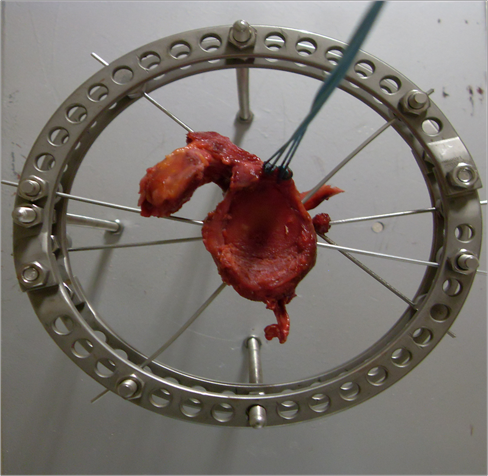
To minimize movement between the specimen and apparatus, the scapula was firmly fixed using the Ilizarov external fixator.
Pressure-Sensitive Film Preparation
Using pressure-sensitive films (Prescale Ultra Super Low Pressure Fuji Photo Film, Fuji Photo Film Co Ltd, Tokyo, Japan), the interface contact area and contact pressure between the capsulolabral complex and the insertion site were examined. The Prescale used in our study consisted of 2 sheets of A- and C-films, and the pressure sensitivity range is 0.2 to 0.6 MPa.
The A-film is coated with microencapsulated color-forming material, while the C-film is coated with color-developing material. When pressure is applied, the microcapsules break, and the color-forming material reacts with the color-developing material to generate color. The microcapsules are designed to react incrementally to the level of pressure; thus, the color density corresponds to the level of pressure.
In a pilot study, the footprint area of the capsulolabral complex averaged 0.9 × 3 cm. Therefore, a template was prepared beforehand to facilitate standardized insertion of the suture anchor systems. The pressure-sensitive films were cut to a size of 9 mm × 3 cm to match the capsulolabral footprint. Then, the film was placed under the prepared template so that we could prepare uniform and symmetric holes on both film sheets. The film was sealed within thin polyethylene sheets for use. During pilot studies, it was shown that the sealing method did not affect the sensitivity or repeatability of the pressure-sensitive film measurements. Before the first repair for each specimen, the pressure-sensitive film was fixed to the footprint interface on the glenoid bone using 2 small screws, 1 superiorly and 1 inferiorly (Figure 3). Immobilizing the pressure film ensured that it would remain at the same location throughout all experimental trials. We kept the film dry by continually using dry gauze and suction device to absorb the moisture from the capsulolabral complex and the glenoid bone. After insertion of the suture anchor systems, the film was inserted between the capsulolabral complex–glenoid surface interfaces. The sutures connecting the capsulolabral complex to the glenoid bone were carefully passed through the prepared holes to allow the best possible panoramic view of the contact pressure and pressure pattern.
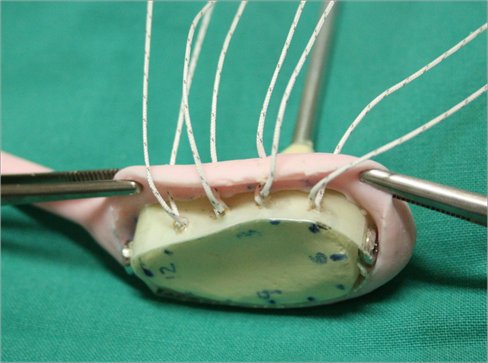
A model of the glenoid is used for illustrative purposes. Before the first repair for each specimen, the pressure-sensitive film was secured to the footprint interface on the glenoid bone.
In both groups, for further analysis, the film was left in place for 2 minutes before the removal of the pressure-sensitive film. Sutures were then carefully cut, and the 2 opposing pieces of film were separated immediately after testing, thus minimizing inadvertent imprint colorization after testing; digital images were created with a scanner. On the basis of the pressure-sensitive film dimensions, the defined footprint area was consistently 270 mm2 for all specimens.
Repair Technique
Two types of repair were performed on each specimen: (1) a single-row repair and (2) a double-row repair. During pilot studies, these 2 repair constructs did not compromise the capsulolabral complex or glenoid bone for the other construct, and pressure-sensitive film impressions were not confounded by the order in which these 2 constructs were performed. Nevertheless, the repair sequence was performed randomly. We used 5.5-mm Bio-Corkscrew suture anchors (Arthrex, Naples, Florida) loaded with No. 2 FiberWire (Arthrex) for all repairs. A single-row repair technique was performed with one suture limb of each Bio-Corkscrew suture anchor (Arthrex), and a double-row repair technique was performed with the other suture limb. One suture limb was cut after tying, and the other unused suture limb was used to perform the other repair technique. All the measurements were made with calipers to standardize the technique for each specimen.
Bio-Corkscrew suture anchors (Arthrex) were placed on the articular margin at the 5:30, 4:30, 3:30, and 2:30 clock positions. All the holes were placed at a 45° angle relative to the glenoid surface. 6,21 If the attachment of the labrum was extended up the superior glenoid without a sublabral foramen, an additional fourth suture anchor was inserted at the 2:30 clock position. Because none of the specimens had sublabral foramen, all cases used 4 suture anchors. To simulate an arthroscopic setting, all anchor system insertion steps, as well as suture passing, were performed with instruments for arthroscopic repair (Spectrum Tissue Repair System, ConMed Linvatec, Largo, Florida).
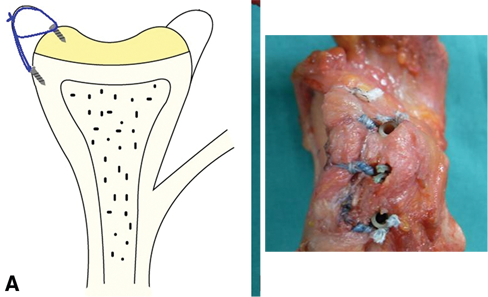
For a single-row repair, the sutures were then passed through 1 cm of the capsulolabral complex using the Spectrum Tissue Repair System (ConMed Linvatec) from an approach inside the capsule as would be done in the arthroscopic setting. All knots were tied first by use of an arthroscopic sliding-knot technique (SMC knot) followed by 3 half-hitches on alternating posts. To standardize tension for the repair, no less than 4 kg of tensile force was used to secure each knot. This was measured by a tensiometer. A single surgeon carried out all repairs (Figure 4).
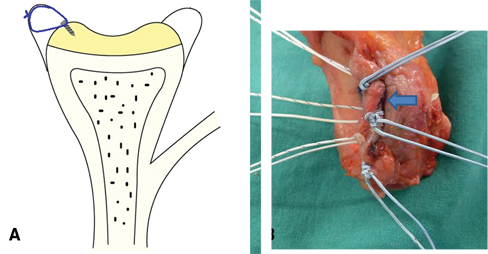
A, schematic line drawing of the single-row repair in axial view. B, the gross specimen shows the uncovered capsulolabral footprint as indicated by the arrow.
For a double-row repair, holes to insert 2.9-mm PEEK PushLock (Arthrex) were made in a similar manner to the standard suture anchor repair, on the edge of the glenoid articular surface at the 5:30, 4:30, 3:30, and 2:30 clock positions. Both limbs of the suture in the anchor were passed through the capsulolabral tissue again with the Spectrum Tissue Repair System (ConMed Linvatec) from an inside approach similar to the arthroscopic situation. The knot for a double-row repair was created as in the single-row repair technique. From each corresponding medial Bio-Corkscrew anchor (Arthrex), the suture limbs were loaded into a PushLock (Arthrex). By use of a tensiometer (Arthrex), a minimum 4 kg of tension was gauged for these suture limbs passing through the suture loop in the PushLock (Arthrex); to simulate the technique clinically, the tensiometer was not used during PushLock (Arthrex) impact, and therefore, the minimum of 4 kg was an estimate, consistent with the amount of tension used clinically. A PushLock (Arthrex) was inserted into the predrilled hole with a mallet and countersunk approximately 1 mm to prevent formation of proud knots (Figure 5). In addition, the procedure was performed using an arthroscopic knot-tying technique with the use of an arthroscopic knot pusher.
Double-row repair schematic (A) and gross specimen (B), allowing visualization and understanding of the way the sutures are passed and tied in the double-row repair construct. The gross specimen (B) shows that the footprint coverage was superior in the double-row repair than the single-row repair (Figure 4B).
Pressure-Sensitive Analysis and Statistical Method
Digital images of each pressure-sensitive film imprint were scanned and stored with a Fuji Film Prescale Pressure Densitometer (FPD-8010E, Fuji Photo Film Co Ltd). Statistical analysis was performed using SPSS software (version 13.0, SPSS, Chicago, Illinois). Mean interface pressure, mean pressurized contact area, and contact pattern were examined for each of the 2 groups. Each of the single- and double-row repair percentage value of restoration of the native capsulolabral complex footprint surface area was calculated based on a defined footprint area of 270 mm2 (9 mm × 3 cm). These data were analyzed using the paired 2-tailed Student t test, and the level of statistical significance was defined as P < .05.
Results
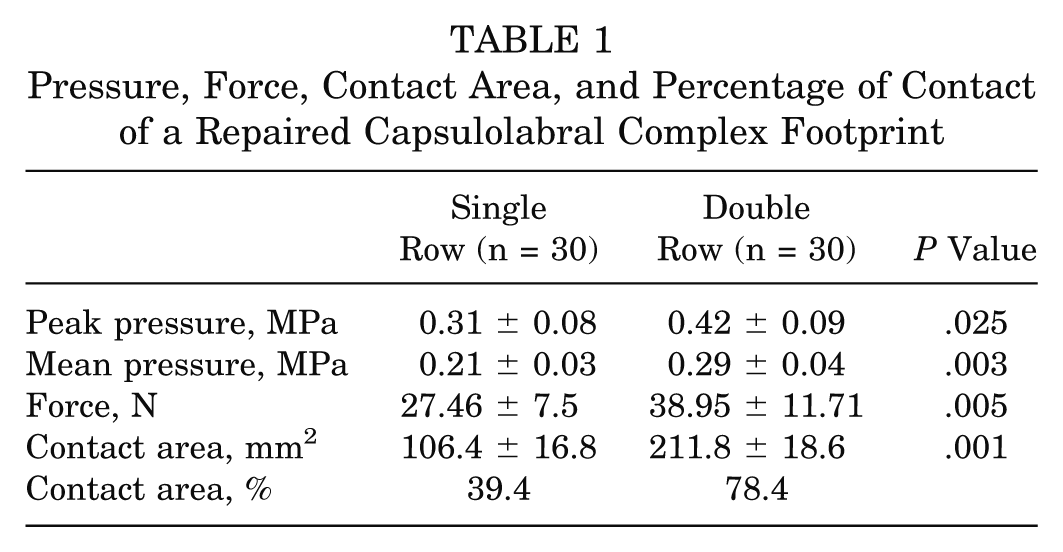
Contact of the capsulolabral complex to the anatomic insertion area was superior in the double-row repair compared with the single-row repair. The peak pressure of the single-row repair was 0.31 ± 0.08 MPa, while for the double-row repair, it was 0.42 ± 0.09 MPa (P = .025) (Table 1). The mean interface pressure exerted over the insertional footprint area by the capsulolabral complex was greater for the double-row repair technique (0.29 ± 0.04 MPa) than for the single-row repair technique (0.21 ± 0.03 MPa) (P = .003) (Table 1). The interface contact force of the single-row repair was 27.46 ± 7.5 MPa, whereas the double-row repair was 38.95 ± 11.71 MPa, and this difference was significant (P = .005) (Table 1). The mean pressurized contact area between the capsulolabral complex and footprint was also significantly greater for the double-row repair technique (211.8 ± 18.6 mm2, 78.4% footprint) compared with the single-row repair technique (106.4 ± 16.8 mm2, 39.4% footprint) (P = .001) (Table 1).
Pressure, Force, Contact Area, and Percentage of Contact of a Repaired Capsulolabral Complex Footprint
Analysis of contact patterns revealed spot welds around the insertion points of each suture anchor in both groups. The pressure around the insertion of each suture anchor was higher than in the space between the suture anchors as represented by the color density in both groups. Although the single-row repair group showed high pressure onto the articular surface of the glenoid and low pressure distribution on the anterior glenoid neck, in the double-row repair group, there was a broad distribution of pressure on the anterior glenoid rim as well as on the anterior glenoid neck (Figure 6).

Imprints for the single-row repair technique (A) and double-row repair technique (B). The pressure around the insertion of each anchor system was higher than in the area between the anchor systems in both groups. The contact pattern between the anchors was increased by the double-row technique, resulting in more footprint coverage.
Discussion
Studies about restoration of the capsulolabral complex to the insertional footprint area and comparison of its restoration either by single- or double-row repair have been rare. Surgical treatments for anterior shoulder instability are either open surgical stabilization or arthroscopic stabilization of the detached capsulolabral complex. 9,13 Open surgical stabilization reattaches the capsulolabral complex to the anterolateral glenoid rim and the capsule to the anterior glenoid neck. This enables fixation and reattachment of the capsulolabral complex close to its original anatomic insertion site. However, current arthroscopic stabilization techniques focus on re-creating the labral bumper effect by locating the suture anchor on the glenoid articular surface when suturing the capsulolabral complex, but in fact, the capsulolabral complex is fixed to the anterior glenoid articular surface and reattached along the anterior glenoid rim as a thin line.
It has been described that, even though most rotator cuff repair techniques cannot restore the original insertion site, the recent double-row repair technique makes it possible to restore the native insertional footprint nearly completely. 11,21 Also, recently, several authors are designing ways to cover the anatomic footprint area of the rotator cuff and to increase contact pressure and contact areas between the bone and the tendon. 5,22,27
Similar to rotator cuff repair, although the rate is low, a major complication of postoperative capsulolabral complex repair is recurrence of the instability. The recurrence rates after arthroscopic shoulder stabilization with suture anchors have been reported to be 0% to 13%. 1,7,12,24 Many authors recommended a special surgical technique including repair of the labrum 1 to 2 mm onto the glenoid articular surface 26,32 or at the articular edge, 17,23 which is thought to create a neolabrum, improve concavity compression, and increase glenohumeral stability. To facilitate healing of the capsulolabral complex to the anterior glenoid bone, preparation of the anterior glenoid bone is performed with bur, shaver, or rasp. 7 However, with this technique, the suture anchors set the suture on the articular surface of the glenoid. As can be seen in Figure 4, the single-row repair technique fails to fix the capsulolabral complex to its native footprint onto the anterior glenoid. In contrast to Figure 4, Figure 5 shows that the double-row repair technique has an advantage in the restoration of native footprint area. The current arthroscopic single-row repair technique may not create an adequate environment to facilitate the healing of the tendon on the footprint area, and the technique might be the reason for the recurring symptom.
Ahmad et al 2 reported that the single-row repair re-created 42.3% of the native footprint surface area while the double-row repair re-created 85.9% in their study to evaluate the normal glenoid insertional anatomy of the anterior-inferior capsulolabral complex and to compare the ability of a single-row repair and a double-row suture bridge repair to restore the insertional anatomy. Also, Ahmad et al 2 argued that double-row repair of the capsulolabral complex re-establishes the native insertional footprint on the anterior-inferior glenoid better than a single-row repair.
Instead of computer digitalization as used in the study of Ahmad et al, 2 our study directly measured interface pressure and contact area and observed contact pattern using pressure-sensitive film. In our study, the double-row repair had significantly higher interface pressure and contact area than the single-row repair. Re-creations of the defined insertion footprint areas based on pressure-sensitive film dimension were 39.4% for the single- and 78.4% for the double-row repair group. Also, for contact patterns, the single-row repair produced the shape of a thin line distributed along the anterior glenoid rim, and the double-row repair revealed a wide band distributed along a significant glenoid bony surface. These findings suggest that the double-row repair technique does restore a greater percentage of the anatomic footprint than the single-row repair. Also, the double-row repair will optimize the potential for healing by improving restoration of insertional contact for capsulolabral repairs when compared with the single-row repair.
Current arthroscopic single-row repair techniques advocated by many authors have been reported with excellent outcomes. 3,7,12,18,28 However, this technique has been noted for a high recurrence rate in athletes or people enjoying sports that require physical contact and in reoperation cases. 8,29 Thus, to those whose group is at risk of recurrence with single-row repair, it may be more beneficial for them to be repaired with the double-row repair technique. Also, in severely injured cases such as adherent anterior labroligamentous periosteal sleeve avulsion (ALPSA) lesion and Bankart lesion with severe displacement and retraction, the double-row repair might be more effective than the single-row repair for improving healing characteristics.
This study has some weaknesses. First, this is a cadaveric study, which does not give biological information of healing. Differences may exist between ex vivo and in vivo studies. Through in vivo observation, it is necessary to confirm that the double-row repair actually increases contact area and interface pressure between the capsulolabral complex and the glenoid bone. Second, this study only offered time zero information in an ex vivo model. Characteristics of contact may change depending on the angle of motion, after repair is done. As a result, studies about real-time measurement of pressure distribution in the double-row repair are needed. Third, because our study used pressure-sensitive films for evaluation, it was impossible to evaluate using arthroscopic repair technique. Instead, we used open surgical stabilization with use of instruments for arthroscopic repair. Fourth, although great care was taken to minimize interference when preparing holes in the film, some artifacts were unavoidable during the process. Also, a few more limitations can be found with Fuji film. 14,25,30 A shortcoming of the film is that it is effective only within a certain range of pressure. Pressures lower than the film range will not be detected, which will cause the actual contact area to be underestimated. Pressures that exceed the film range will saturate the film and underestimate the actual maximum pressure. Also, pressure-sensitive film irreversibly records all pressure contributions over time. 31,33 With pressure-sensitive film, the measurement does not account for any decrease in contact area or pressure that may occur from the time of repair to the time of measurement due to, for example, tendon or suture creep. The colorization of the film is cumulative (does not diminish with decreases in contact), and therefore, the area and pressure measurements may tend to be overestimated when using pressure-sensitive film. 14,31
Although the double-row repair has greater interface contact area and pressure, applying it to the actual clinical setting requires critical discussion. When applied to the clinical setting, low pressure between the glenoid bone and the capsulolabral complex can result in separation of the repaired interface. On the other hand, high pressure may cause disturbance of the vascularization in impaired tissue healing. Thus, studies about possible generation of overtension, which may disturb vascularization, are needed.
It is our conclusion that the double-row repair is better for restoration of the insertion site by open surgical stabilization than arthroscopic stabilization. Lafosse et al 20 described a double-row repair named Cassiopeia double-row technique, but to insert into the exact position of the medial suture anchors, it is essential to make a very inferior and medial anterior portal above the subscapularis tendon. When using this portal, the neurovascular structures are potentially more at risk. It may also result in high cost due to more suture anchors used. However, it should also be noted that because of arthroscopy’s inherent advantages over open surgical stabilization, a technique of double-row repair of the capsulolabral complex using an arthroscopic technique should be developed in the future.
Conclusion
The results of this study show that the double-row repair has significantly greater mean interface pressure and pressurized contact area at the insertion site of the capsulolabral complex than the single-row repair. Also, the contact pattern between the anchors could be increased by the double-row technique, resulting in more footprint coverage than is observed for single-row techniques. Therefore, the double-row repair may have an advantage over the single-row repair to restore the native footprint area of the capsulolabral complex.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.