
Abstract
Background
Extramedullary cortical button–based fixation for distal biceps tendon ruptures exhibits maximum load to failure in vitro but cannot restore the anatomic footprint and has the potential risk for injury to the posterior interosseous nerve.
Hypothesis
Double intramedullary cortical button fixation repair provides superior fixation strength to the bone when compared with single extramedullary cortical button–based repair.
Study Design
Controlled laboratory study.
Methods
The technique of intramedullary cortical button fixation with 1 or 2 buttons was compared with single extramedullary cortical button–based repair using 12 paired human cadaveric elbows. All specimens underwent computed tomography analysis to determine intramedullary dimensions of the radial tuberosity as well as the thickness of the anterior and posterior cortices before biomechanical testing. Maximum load to failure and failure modes were recorded. For baseline measurements, the native tendon was tested for maximum load to failure.
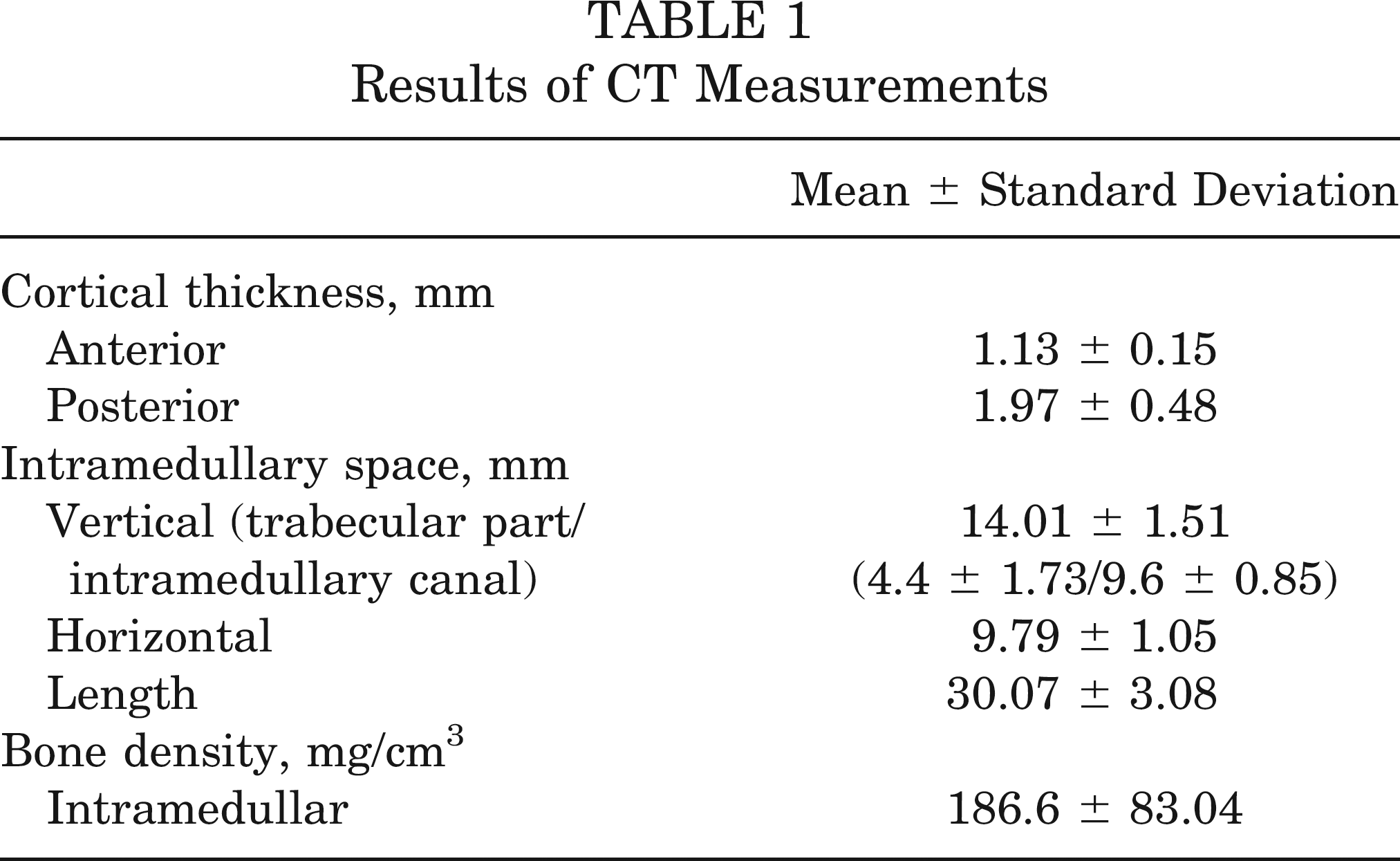
Results
The intramedullary area of the radial tuberosity provides sufficient space for single or double intramedullary cortical button implantation. The mean thickness of the anterior cortex was 1.13 ± 0.15 mm, and for the posterior cortex it was 1.97 ± 0.48 mm (P < .001). We found the highest loads to failure for double intramedullary cortical button fixation with a mean load to failure of 455 ± 103 N, versus 275 ± 44 N for single intramedullary cortical button fixation (P < .001) and 305 ± 27 N for single extramedullary cortical button–based technique (P = .003). There were no statistically significant differences between single intramedullary and single extramedullary button fixation repair (P = .081). The mean load to failure for the native tendon was 379 ± 87 N.
Conclusion
Double intramedullary cortical button fixation provides the highest load to failure in the specimens tested.
Clinical Relevance
Double intramedullary cortical button fixation provides reliable fixation strength to the bone for distal biceps tendon repair and potentially minimizes the risk of posterior interosseous nerve injury. Further, based on a 2-point-fixation, this method may offer a wider, more anatomic restoration of the distal biceps tendon to its anatomic footprint.
Keywords
Distal biceps tendon rupture typically occurs in middle-aged male patients who suffered an acute trauma with massive eccentric loading of the biceps brachii. In the past few decades, the incidence of this injury has increased from 3% to 10%.13,35 For pathogenesis, focal degenerative processes caused by hypovascularity within the tendon and mechanical impingement on the biceps tendon during forearm rotation continue to be cited in the literature as the reason for rupture at the tendinous insertion at the radial tuberosity. 37 Furthermore, the abuse of steroids and nicotine has been discussed to cause the tendon tear.30,35 Operative repair of these injuries has shown improved functional elbow outcome compared with nonoperative treatment.4,16,31
Currently, anatomic reinsertion of the biceps tendon to the radial tuberosity has been recognized as the treatment of choice to restore normal flexion and supination strength.23,34,39 Because of the increased risk of hetero-topic ossification or radioulnar synostosis using the “classic” or “modified” 2-incision technique,6,11 the 1-incision technique for distal biceps tendon repair has become more popular in recent times.7,29 Via a single anterior approach, a variety of surgical repair techniques using suture anchors, interference screws, and cortical fixation buttons have shown both good clinical results and near preinjury strength of forearm supination and elbow flexion.12,14,15,19,20,28 For fixation to the bone, the construct with the strongest biomechanical data is a titanium extra-medullary cortical fixation button (“EndoButton technique”), which is anchored to the tendon by sutures and deployed on the posterior cortex of the proximal radius.21,22,26 The strength of this construct may allow earlier, more aggressive protocols for postoperative rehabilitation. Possible gap formations using a double- or single-fixation method for distal biceps repair are controversially discussed in the current literature. The “EndoButton technique” may provide minor displacement of the repair and is able to maintain bone-tendon continuity because of its intramedullary placement of the restored tendon. 40 However, this cortical button–based technique cannot restore the anatomic footprint of the distal biceps tendon and furthermore runs the risk of posterior interosseous nerve (PIN) injury as well as loss of motion attributable to het-erotopic ossification.1,3,32
The purpose of the present study is to demonstrate the new technique of intramedullary cortical button fixation (Biceps-button, Arthrex, Naples, Florida) for distal biceps tendon repair and to evaluate this procedure with respect to fixation strength to the bone versus the standard extramedullary cortical button–based technique. Our hypothesis is that double intramedullary cortical button fixation will provide superior loads to failure when compared with the traditional single extramedullary cortical button–based technique.
Materials and Methods
Specimens
A total of 24 Thiel-preserved 42 cadaveric radii (harvested from 12 paired elbows), with complete soft tissues removed except of the distal biceps tendon, were used for this study. The mean age was 79 years (range, 65-96 years). The radii with the attached tendon were all cut to a consistent length of 10 cm from the proximal head.
Computed Tomography Measurements
All specimens were scanned on a clinical 256-slice multi-detector CT (Brilliance iCT, Philips Healthcare, Hamburg, Germany) before biomechanical testing. Three hand-drawn regions of interest (ROIs) that delimited the trabecular bone of the radial tuberosity were placed in the proximal, central, and distal tuberosity to determine thicknesses of anterior and posterior cortex (Figure 1). The intramedullary dimensions of the radial tuberosity were defined by the vertical diameter including trabecular bone and the horizontal diameter. The length of the tuberosity was appointed by its distance from proximal beginning to distal ending. The measured data were averaged from the 3 ROIs. To validate the influence of bone quality and the measured failure strengths between repair groups, the bone mineral density of the radial tuberosity was defined by simultaneously using a phantom provided by the manufacturer of the scanner and consisting of water- and bone-equivalent solid materials (0 and 200 mg/cm3 calcium equivalent).
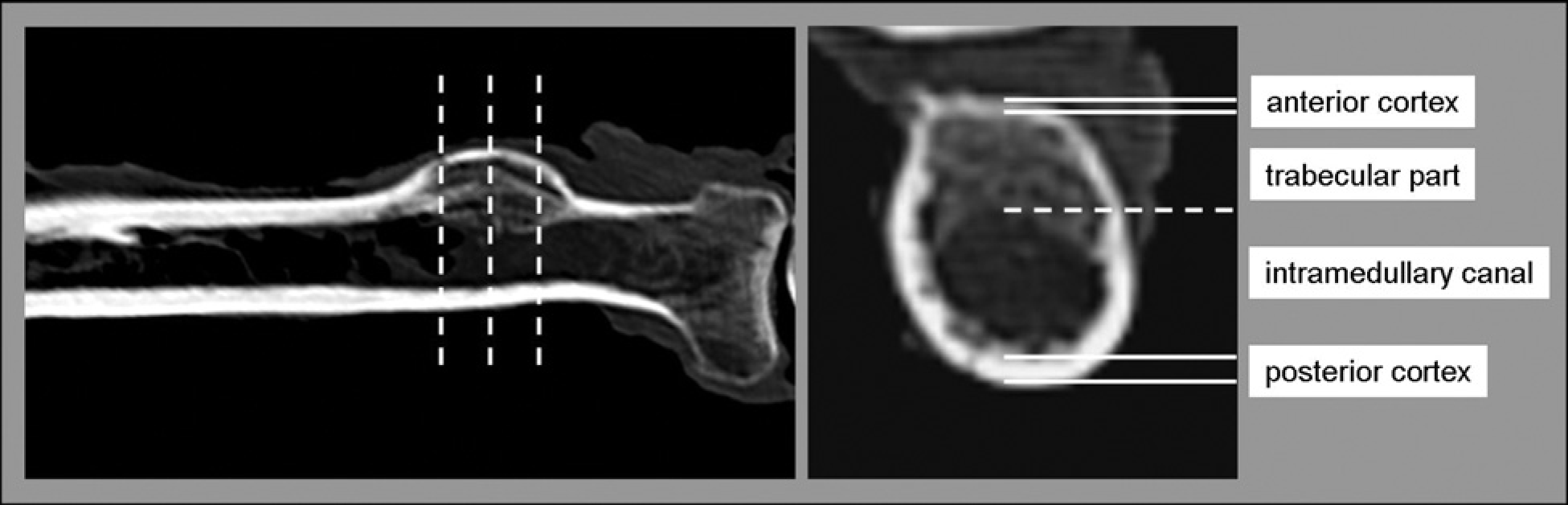
Radiologic scheme with dashed lines indicating the regions of interest (ROIs) for CT measurements of the radial tuberosity (left). Axial CT scans were taken to determine cortical thicknesses and intramedullary space (right). Sagittal images were used to measure the length (not shown).
Biomechanical Testing
For baseline measurements of fixation strength of the native tendon to the bone, 20 specimens with intact distal biceps tendon were loaded to failure. Four specimens with previously damaged tendons were excluded from the study.
Each radius was securely fixed in a custom-made angle-adjustable apparatus that was mounted on a materials testing machine (Zwick 2.5 TN, Zwick/Roell, Ulm, Germany). The native biceps tendon was tightened in a liquid nitrogen cryoclamp at the musculotendinous junction 7 cm from the osseous insertion. The tension vector was oriented at 45° to the radial shaft to simulate the in vivo direction of pull of the biceps tendon more precisely (Figure 2). A preload of 5 N was applied to precondition the construct and warrant a consistent starting point. Afterward, the load to failure was performed with an extension rate of 4 mm/s according to previous published studies.21,25,33 Maximum load of failure and mode of failure for each specimen were recorded.

Setup for biomechanical testing on servohydraulic machine.
After the complete dissection of the residual distal biceps tendon fibers of its osseous insertion, all specimens (12 pairs of radii) could be reused for repair testing. No irregularities or previous lesions of the radial tuberosity were detected. According to their age, gender, and bone mineral density, specimens were matched for 2 groups of 12 specimens each for biomechanical testing. For the different repair techniques, we alternated right and left elbows with each successive pair of radii.
To figure out if the number of the implanted buttons (1 or 2) or their location to corresponding cortices will result in higher failure strengths, we first tested the single intramedullary cortical button technique in 12 specimens. Afterward the same radii were carefully examined for integrity of the posterior cortex and reused for single extra-medullary cortical button–based repair.
For single intramedullary fixation, 1 button was placed in the center of the radial tuberosity ridge. The Arthrex Bicepsbutton is an implantable titanium suture button that measures 2.6 × 12 mm and provides 2 suture holes. By comparison, an EndoButton measures 4 × 12 mm. Sethi et al 38 were the first who reported the use of the Bicepsbutton for distal biceps repair performing the so-called tension slide technique.
The double intramedullary cortical button fixation was performed in the same manner as single intramedullary fixation. To introduce the buttons into the intramedullary canal, the 3.2-mm drill was performed in an angle of 60° inclined to the radial head only into the anterior cortex. The proximal drill hole was positioned to the proximal beginning of the tuberosity ridge in each specimen to ensure a consistent implantation. After drilling, the button was passed through the anterior cortex and flipped with a button inserter (Arthrex). To prevent the buttons from interfering with each other inside the medullary canal, a custom-made parallel drill guide with defined 12-mm distance was used (Figures 3 and 4).
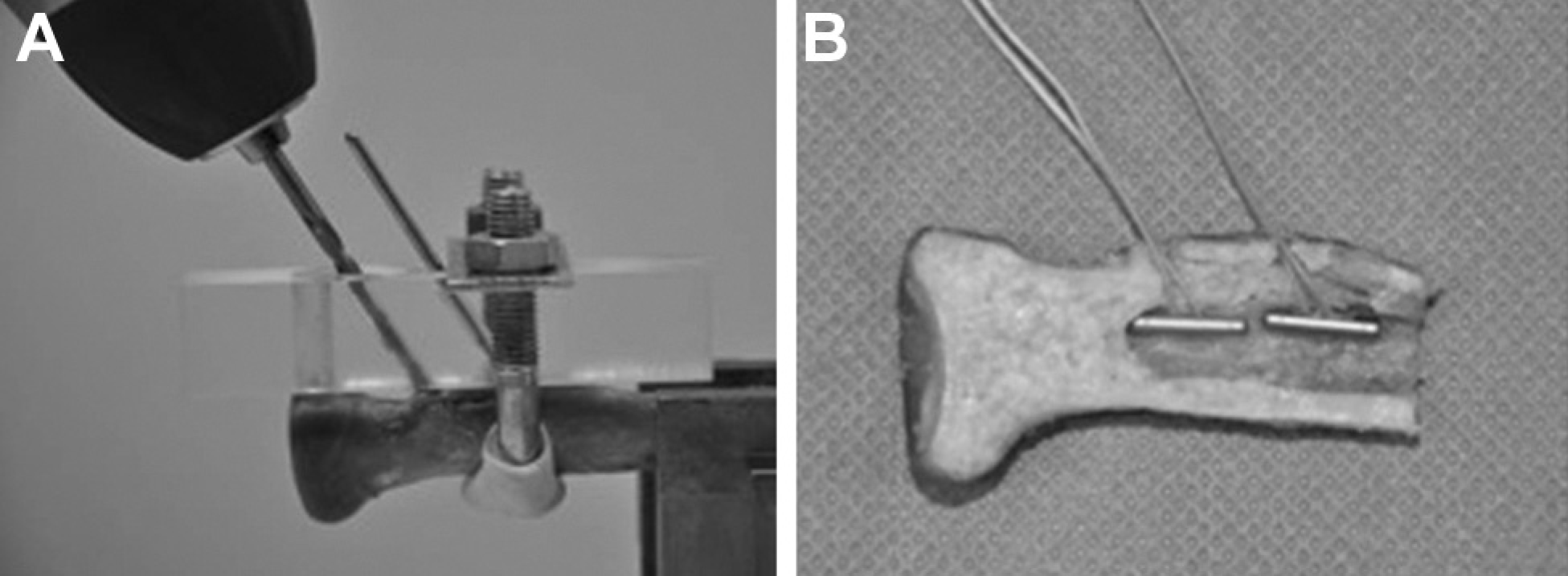
Parallel drill guide for double intramedullary cortical button implantation with a defined angle of 60° and 12-mm distance between drill holes (left). Sagittal cross-section of the radius with 2 intramedullary implanted Bicepsbuttons (right).
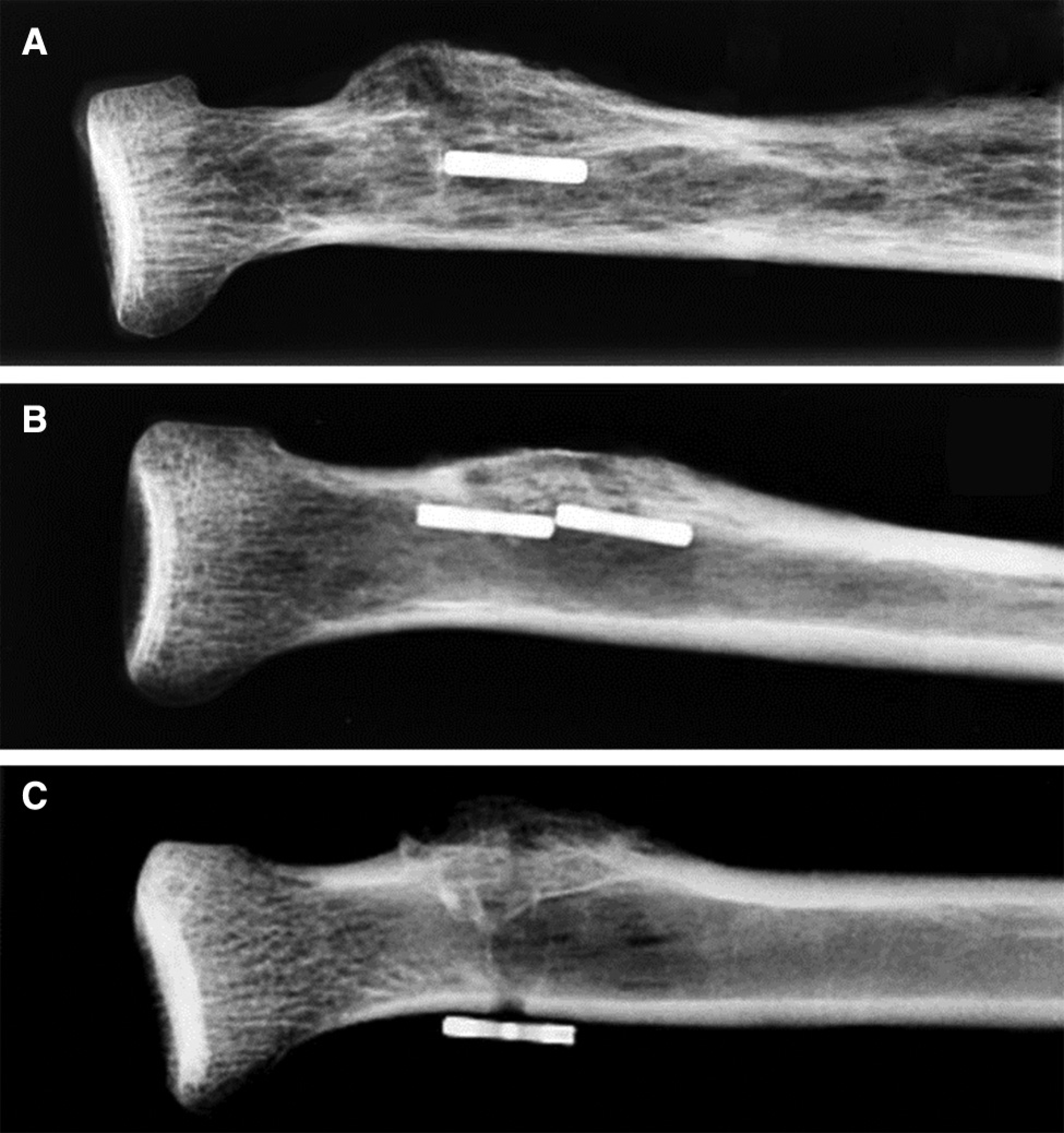
Radiographic controls for the different repair techniques: A, single intramedullary cortical button fixation; B, double intramedullary cortical button fixation; and C, single extramedullary cortical button–based technique.
For single extramedullary cortical button–based repair, 1 Bicepsbutton was passed and flipped on the posterior cortex of the radius via a 3.2-mm drill hole according to the manufacturer's instructions.
All buttons were single-loaded with No. 2 FiberWire nonabsorbable suture (Arthrex). The sutures were mounted in an axial tension device by securely knotting them to the testing system. We used the same testing setup with a 45° tension vector to the long axis of the radius as described above for the native tendon. All repair groups were loaded to failure with an extension rate of 4 mm/s consisting of a preload of 5 N. Again, maximum load of failure and mode of failure for each specimen were recorded.
Statistical Analysis
Statistical analysis was performed using PASW software, Version 18.0.2 (SPSS Inc, Chicago, Illinois). Data were presented as mean ± standard deviation. The comparison between the different repair groups and the values of native tendon were done using Friedman or Wilcoxon signed-rank test where appropriate. A pretesting power analysis revealed a minimum of 11 specimens per group to achieve statistical power of .80. A difference in load to failure of 20% was set as clinically important difference a priori. Subject to a standard deviation of 94 N, a paired t test was considered to be sufficient to detect a 20% difference between repair techniques. All analyses were done using a 2-sided .05 level of significance.
Results
Computed Tomography Measurements
Table 1 summarizes the results of radial tuberosity dimensions with respect to cortical thickness, intramedullary space, and bone mineral density. There were significant differences in thickness for the anterior and posterior cortex between the defined ROIs (P < .001). The mean difference between the posterior and the anterior cortical thicknesses was 0.84 ± 0.33 mm with a mean anterior cortical thickness of 1.13 ± 0.15 mm and a mean posterior cortical thickness of 1.97 ± 0.48 mm. No significant differences were seen in cortical thicknesses and bone mineral density between repair groups (P > .05).
Results of CT Measurements
Biomechanical Testing
For the native biceps tendon and for all repair techniques, the maximum load to failure was considered when the testing machine stopped at a drop in force of 50% from the applied maximum force (Fmax 50%). The recorded Fmax was equated with the maximum load to failure.
All native tendons ruptured step-by-step at the bone-tendon interface starting from the distal part of the osseous insertion. No bony avulsion of the osseous insertion or failure between the tension device and the tendon were observed in specimens tested. We found a mean failure strength of the native biceps tendon of 379 ± 87 N, which was significantly higher than the single intramedul-lary (275 ± 44 N; P = .001) and single extramedullary (305 ± 27; P = .035) cortical button fixation (Figure 5). Mean maximum loads to failure for double intramedullary cortical button fixation were 455 ± 103 N, which was not significantly different when compared with the native tendon (P = .201).
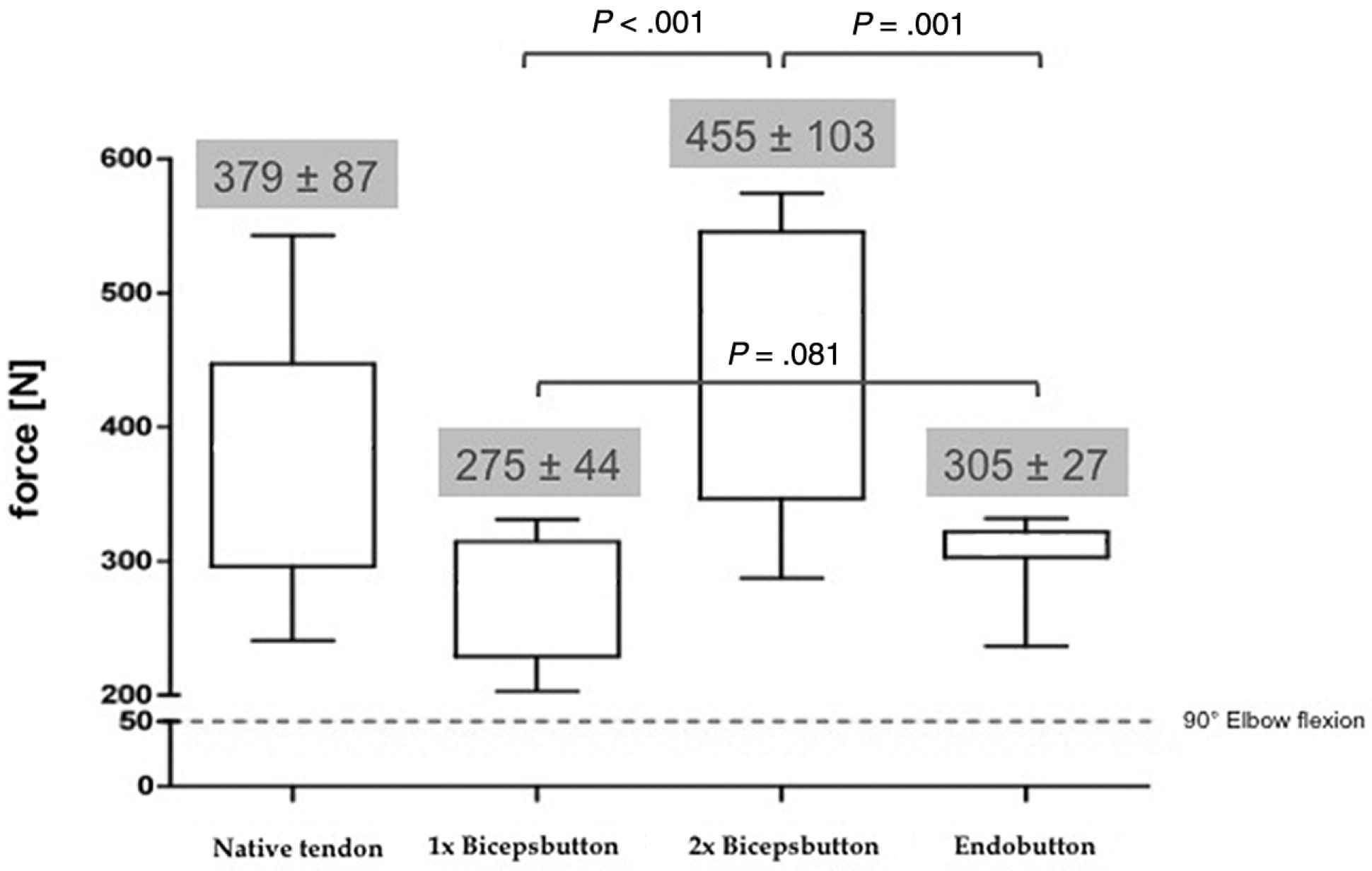
Maximum loads to failure ± standard deviation for native tendon and repair techniques. EndoButton = single extramedullar cortical button-based repair. A value of 50 N on average (dotted line) indicates the physiologic force to flex the elbow at 90° against gravity.
For all reconstruction techniques, we found the highest loads to failure for double intramedullary cortical button fixation (455 ± 103 N) (Figure 5). This was significantly higher than for single intramedullary (275 ± 44 N; P < 0.001) and single extramedullary (305 ± 27 N; P = .001) cortical button techniques. No significant differences, however, were seen between the single intramedul-lary and the single extramedullary cortical button fixation (P = .081).
Button pullout, bony avulsion, or suture breakage were defined as repair failure for all specimens. Of 12 specimens with single or double intramedullary cortical button fixation, 7 of each group had a button pullout with fracture avulsion of the anterior cortex at the osseous bridge between the implanted buttons and 5 failed because of suture breakage at the knot side. The extra-medullary cortical button–based technique failed by suture breakage at the knot side in 11 of 12 specimens. No suture breakage at the button side was observed. In only 1 specimen, a fracture avulsion was observed at the posterior cortex.
Discussion
In 1941, Dobbie 9 recommended nonoperative treatment of distal biceps tendon ruptures and noted that it is “impractical and unwise to select a procedure more difficult, dangerous and time consuming when the same result can be obtained with less effort and without risk of serious complications.”
Over time, numerous studies have revealed superior results in functional outcome after surgical repair when compared with nonoperative treatment. 4 , 8 , 16 The 2-incision technique, initially described by Boyd and Anderson 6 in 1961 and modified by Morrey et al, 31 has popularized the anatomic method of tendon repair, which means the reattachment of the distal biceps tendon to its anatomic footprint at the radial tuberosity. Because of the availability of improved fixation devices in the late 1990s and early 2000s, the anterior limited single-incision approach was favored by upper extremity surgeons in an effort to avoid neurovascular complications and to minimize the risk of heterotopic ossification. 11 , 34 Anchor-based repair techniques have been the most widely used in recent years and most authors have reported excellent clinical results., More recently, extramedullary cortical button–based repair has proven to provide the highest fixation strength to the bone in several biomechanical studies when compared with other single-incision techniques.21,22, 40
Bain et al 3 were the first to report on single-incision extramedullary cortical button fixation for repair of distal biceps tendon ruptures (EndoButton, Smith & Nephew, Andover, Massachusetts). The authors reported excellent results in a series of 12 patients but raised the question of risk of PIN damage during the procedure. Depending on the direction of the tunnel through the posterior cortex, the average distance to the PIN varied between 8 and 14 mm. Greenberg et al 14 reported a minimum distance of 7 mm to the PIN for EndoButton-assisted repair of distal biceps tendon ruptures.
The hypothesis of our study was that intramedullary cortical button fixation biomechanically provides superior loads to failure when compared with the traditional single extramedullary cortical button–based technique, but has a decreased risk for potential injury of the PIN.
In the first part of this in vitro investigation, a CT analysis of all specimens was performed to determine cortical thicknesses and intramedullary dimensions of the radial tuberosity. We found that the anterior cortex was significantly (P
The main purpose of this study was to evaluate the new repair technique of double intramedullary cortical button fixation with respect to fixation strength to the bone when compared with the standard single extramedullary cortical button–based technique.
During biomechanical testing, we performed the loading force at an insertion angle of the fixation device of 45° to better approximate the pull of the biceps muscle in vivo. Krush-inski et al 24 reported a mean angle of insertion of the distal biceps tendon of 45° when the elbow was flexed at 30°. We found mean maximum loads to failure for the native biceps tendon of 379 N. These findings are similar to data published by Krushinski et al. 24 We found higher failure loads for the native tendon (379 N) when compared with the single intramedullary cortical button fixation (275 N; P = .001) and the single extramedullary cortical button–based repair (305 N; P = .035). We assume that our biomechanical setup with a tension vector oriented at 45° to the radial shaft is responsible for these findings. Concerning the failure mode of the native tendon with a step-by-step rupture of the tendon, a “partial rupture model” was created that was probably able to maintain the applied tension force and finished in higher failure loads.
For the different fixation techniques tested, double intramedullary cortical button fixation had superior failure strengths compared with single intramedullary cortical button fixation (455 N vs 275 N; P
There are several biomechanical studies in the literature testing different fixation techniques. Greenberg et al 14 evaluated the pull-out strength of extramedullary cortical button–based fixation, suture anchors, and transosseous tunnels. In this study, the pull-out strength of the “EndoButton technique” was significantly higher than the bone tunnels and suture anchors. Kettler et al, 21 Mazzocca et al, 26 and Spang et al 40 also confirmed superior loads to failure for extramedullary cortical button–based fixation when compared with suture anchors and interference screws. Our findings for extramedullary cortical button–based repair compare favorably to studies cited above with respect to mean failure strengths.
Our study, however, is to our knowledge the first that also tested single and double intramedullary cortical button fixation.
The results for double intramedullary cortical button fixation were significantly higher when compared with single intramedullary and single extramedullary cortical button fixation. One might argue that 2 devices are stronger than 1 because of load sharing. We therefore also tested single intramedullary and single extramedullary cortical button fixation. Interestingly, there was no significant difference between these 2 groups (275 N vs 305 N; P = .081), although the anterior cortex was significantly thinner than the posterior (1.13 mm vs 1.97 mm; P <.001). This can be explained by compression of cancellous bone, which may increase the intramedullary resistance and differences in the different failure modes between intramedullary and extramedullary button placement. In both repair groups with intramedullary button fixation, 7 of 12 specimens failed by bony avulsion at the tuberosity ridge. We speculate that this is caused by the difference in thickness of the cortex of the anterior and posterior walls of the radial tuberosity. On the other hand, suture breakage at the knot side was the predominant mode of failure for the single extramedullary cortical button-based technique. Green-berg et al 14 reported a mean pull-out strength for an extra-medullary cortical button–based reconstruction of 584 N, which was distinctly higher than failure loads we saw in our study for all repair groups (455 N, 305 N, 275 N). This may have been associated with different sutures (No. 5 Ethibond) used in their testing model or differences in the cadaveric specimens.
Current anatomic studies described the distal tendon unit as 2 distinct parts, 1 each from the long and short heads of the biceps muscle with different insertion areas at the distal and proximal part of the tuberosity as well as different functional parts for elbow flexion and supination.2,10 Using a 2-point fixation principle, the double intramedullary cortical button fixation may provide a wider, more anatomic repair.
There are some limitations of our study. The tested human cadaveric radii, harvested from the institutional anatomic institute, were embalmed in the technique described by Thiel. 42 The mechanical properties of cortical bone are altered by this preservation method similar to other storage methods. 43 Stefan et al, 41 in a recently published study, reported that Thiel fixation increases the plastic energy absorption, whereas formalin as well as alcohol-glycerine fixation decreases the plastic energy absorption. Furthermore, the mean age of our cadaveric specimen, 79 years, was significantly older than the typical age for distal biceps ruptures (40s and 50s), but comparable with the specimen age in other studies.5,18,24,25 It is possible that in younger cadavers with better bone quality, the failure mode might change with fewer bony avulsions. This may be especially relevant for intramedullary placement where this was the predominant failure mode.
We only evaluated the fixation strength to the bone for maximum loads to failure of the different techniques tested. For that reason, linear load to failure instead of cyclic loading was applied as described in previous publications.14,21
Finally, the 12 cadavers for single cortical button repair (intra- and extramedullary) were used twice. We do not believe that this influenced our results because of the failure mode, which was suture breakout in 11 of 12 cases for the secondarily tested extramedullary cortical button repair. Using the same specimen may also be seen as a strength of the study because it limits the variance of bone quality, which could have biased our results.
For clinical use, the intramedullary positioning of the buttons may prevent the PIN injury as an iatrogenic complication because the posterior cortex at the bicipital tuber-osity remains intact. Depending on the drill trajectory for an extramedullary cortical button fixation and the position of the button itself to the posterior cortex, the PIN is placed at significantly increased risk for injury.14,36 Similarly, anchor-based repair techniques may also place the PIN at a theoretic risk, if the posterior cortex is cracked by the drill or the anchor itself.
In conclusion, double intramedullary cortical button fixation provides significantly higher loads to failure than single intramedullary or extramedullary cortical button reconstruction in a biomechanical setup. These findings have encouraged us to use this technique for distal biceps tendon repairs with a more aggressive rehabilitation protocol.