
Abstract
Background
Few data on shoulder arthropathy in patients undergoing arthroscopic repair for glenohumeral instability are available.
Hypothesis
Arthroscopic stabilization of Bankart lesions does not prevent the development of postoperative glenohumeral osteoarthritis.
Study Design
Case series; Level of evidence, 4.
Methods
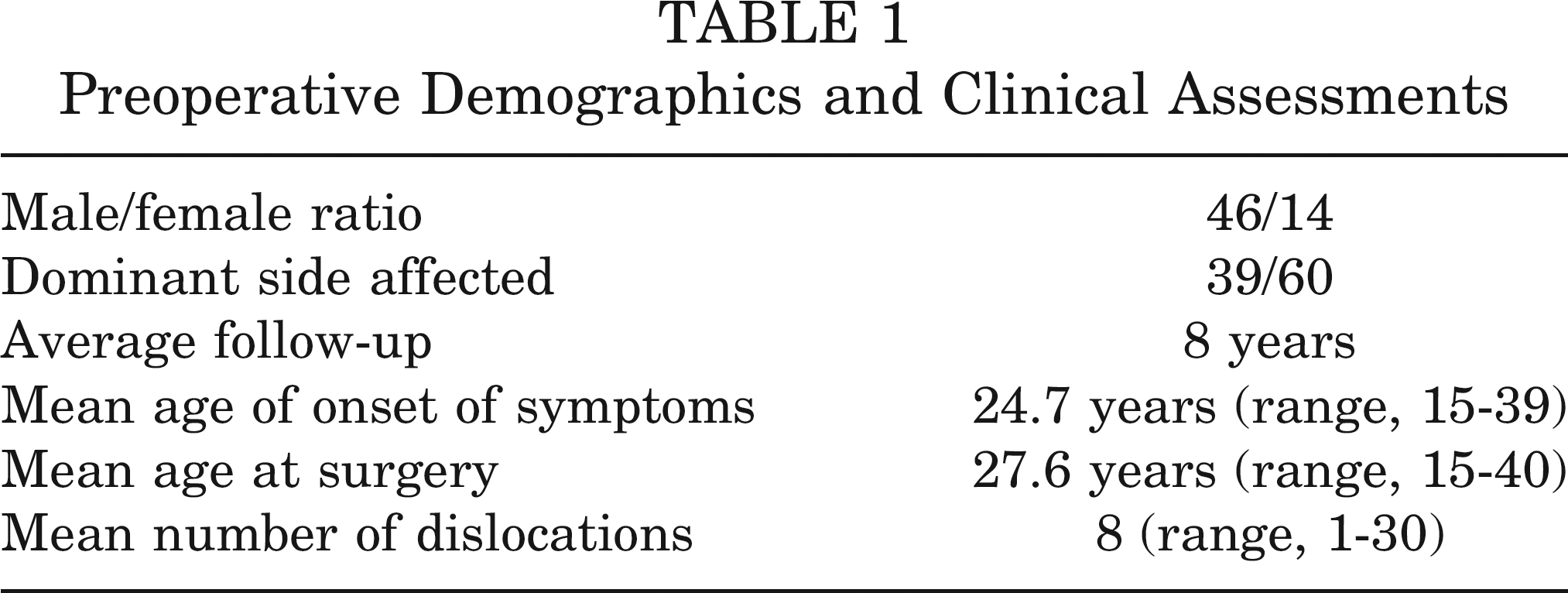
Clinical (Rowe and Constant scores) and radiographic preoperative and postoperative data from 60 patients who underwent arthroscopic Bankart repair were compared. Osteoarthritis was graded preoperatively and postoperatively with the Buscayret classification grading system. The average age at surgery was 27.6 years, and follow-up averaged 8.0 years.
Results
The postoperative incidence of osteoarthritis in patients with no preoperative degenerative changes was 21.8% (12 of 55 patients). The incidence of degenerative joint disease of the glenohumeral joint showed evidence of a statistically significant association with older age at first dislocation and at surgery, increased length of time from the first episode to surgery, increased number of preoperative dislocations, increased length of time from the initial dislocation until surgery, increased number of anchors used at surgery, and more degenerated labrum at surgery. A higher number of preoperative dislocations, a greater length of follow-up, and reduced external rotation in abduction influenced Rowe and Constant scores.
Conclusion
The number of anchors used and the state of the labrum are the most important factors associated with a higher risk of radiographic degenerative changes. Longer follow-up investigations are needed to draw meaningful conclusions.
Arthroscopic Bankart repair and open procedures for post-traumatic, recurrent, unidirectional shoulder instability produce comparable outcomes.4,9,14 Although arthroscopic surgery results in less morbidity, shorter surgical time, improved cosmesis, and less postoperative pain, open procedures may still be superior in terms of long-term stabil-ity,11,20 despite their possible association with a higher incidence of glenohumeral arthropathy. 27 Almost all the data relating to glenohumeral arthropathy associated with shoulder instability repair were studied before the development of arthroscopic techniques, but the lack of long-term follow-up data did not allow determination of whether arthroscopic shoulder repair 16 affects the incidence of shoulder osteoarthritis (OA). In this investigation, we wished to define the arthrogenic factors that correlate with the development of degenerative changes in patients who had undergone arthroscopic Bankart repair. We also report on postoperative clinical success rates and clinical outcomes using the Constant and Rowe scores, and range of motion (ROM) assessment.
Materials and Methods
Patient Population
The present investigation is a retrospective analysis of prospectively collected data on 72 consecutive patients who presented to our institution to undergo arthroscopic Bankart repair for unilateral anteroinferior shoulder instability during the period 1996 to 2005. Patients were eligible for participation if the following inclusion criteria were met: (1) recurrent (2 or more), unidirectional, anterior dislocation or subluxation, unresponsive to non-operative treatment; (2) had been diagnosed on clinical grounds and through MRI; and (3) had been operated by the same fellowship-trained surgeon. Patients with multidirectional instability, prior surgery on the affected or con-tralateral shoulder, contralateral shoulder instability, severe preoperative shoulder OA, and preoperative radio-graphic diagnosis of bony Bankart lesion and Hill-Sachs defect were excluded from the study. We also excluded patients with superior labrum anterior and posterior (SLAP) lesions and/or lesions of the biceps tendon.
Of the 72 dislocations, all had a Bankart lesion on arthroscopic assessment; in 62 (86%) of the patients, the recurrent anterior dislocations had been documented at least twice by plain radiography. In the remaining 10 patients (14%), the shoulder had always reduced spontaneously before radiographs could be performed, but the history of trauma and the intraoperative findings confirmed a Bankart lesion. Fifty-nine (82%) of the original dislocations had been produced by a definite injury, and 13 (18%) by a normal movement of the arm.
The patients were assessed at baseline immediately before the index operation, and postoperatively at 2 years and at a minimum 5-year follow-up. Clinical and operative details were thoroughly recorded for each patient. The scientific and ethical contents of this study were in compliance with guidelines by our institutional review board.
Operative Treatment
All surgical procedures were performed by a single experienced board-certified fellowship-trained orthopaedic surgeon (F.F.). All patients received a general anesthetic and were placed in the lateral position. An arthroscopic Bankart repair was performed in all 72 patients (72 shoulders). A diagnostic arthroscopy was performed to evaluate the presence of any lesions, and a 3-portal technique was used. At the index procedure, all patients had a Bankart lesion, approximately between 1 and 2 o'clock and 5 and 6 o'clock (in the right shoulder). Bankart lesions were classified as type I (robust labrum), type II (thinned labrum), or type III (absent labrum), according to the thickness of the labral tissue. 10 The shoulders were operated on with suture technique. 2
Initially, the bone bed on the glenoid neck was prepared using a motorized bur, until a bleeding surface was produced. In patients with type I and II labrum, capsular plication was accomplished by sutures passed through the labrum and capsular tissue. This construct acts as a neo-labrum, reduces intra-articular volume, increases tension, and decreases joint instability. If a type III labrum was present, suture anchors were inserted in the glenoid rim to perform a capsular shift. Metal or bioabsorbable suture anchors were placed and sutures were passed for the Bank-art lesion. Metal anchors (2.4-mm Fastak, Arthrex, Naples, Florida) single-loaded with No. 2 Ethibond (Ethicon, Somerville, New Jersey) sutures were used from 1995 to 2003 (43 patients), while bioabsorbable anchors (3.0-mm BioFastak, Arthrex) double-loaded with No. 2 FiberWire (Arthrex) sutures were used from 2004 on (29 patients). Depending on the size of the lesion, a median of 2 anchors (range, 1-4) were used, beginning at the 5-o'clock position inferiorly and then progressing superiorly. After capsulo-labral complex repair, the construct was assessed for persistent significant capsular laxity by evaluating the presence of an easy drive-through sign and the volume of the capsule after inflating the glenohumeral joint. Eighteen of 72 patients (25%) underwent anteroinferior laser capsular shrinkage as an additional procedure to address residual capsular redundancy in the period from 1996 to 2005.
Rehabilitation
Postoperatively, the patients wore a sling for 4 weeks and were allowed free flexion and internal rotation from the first postoperative day. At 4 weeks, patients were cleared for free ROM in all directions, and strengthening exercises were started. All patients had regained full functional stability in the operated shoulder at 6 months.
Outcomes Assessment
Imaging. All patients received standard radiographs in 2 planes of the affected shoulder, performed preoperatively, at 2 years, and at a minimum 5-year follow-up. Pre-operative and postoperative radiographs were reviewed and compared by a single independent radiologist not involved in the initial management of patients. For radio-graphic analysis of degenerative changes, imaging findings were staged according to the Buscayret 5 classification. Stage 1 consists of osteophytes measuring less than 3 mm in the greatest diameter; stage 2 consists of osteo-phytes measuring between 3 and 7 mm in the greatest diameter, with slight glenohumeral joint irregularity; and stage 3 consists of osteophytes measuring more than 7 mm in the greatest diameter, with narrowing of the gle-nohumeral joint and sclerosis. Osteophytes may be located on the humerus, the glenoid, or both. Stage 4 consists of complete obliteration of the glenohumeral joint space with or without osteophytes (stage 4 was included with stage 3 in the original classification system). Stages 1 through 3 do not involve complete obliteration of the gleno-humeral joint space. Specific observations were made for the presence of preoperative degenerative changes, progression of changes on the postoperative radiographs in patients with evidence of preoperative arthropathy, and development of changes on the postoperative radiographs in patients without preoperative disease.
Clinical Assessment. Clinical functional evaluation was carried out preoperatively, postoperatively at 2 years, and at latest follow-up at a minimum of 5 years from the index operation by a single trained examiner (R.P.) not involved in the clinical management of these patients. The clinical assessments were performed according to the Constant 8 and Rowe 30 scores. Stability was assessed using the apprehension test, and the results were graded in 3 categories, as normal, discomfort in maximum external rotation without signs of subluxation, and signs of subluxation with muscular contraction. 12 Patients with signs of subluxation who reported 1 or more frank dislocations or had a history of a minimum of 1 episode of “dead-arm syndrome” during the follow-up period were classified as a failure in terms of stability. Measurements of ROM were performed using a goniometer. External rotation was measured with the arm at 90° of abduction, and active and passive ROM of the operated shoulder were compared with the contralateral side. Preoperatively and at the last follow-up, patients were asked to classify their activity level as overhead activity, contact sports, sports without overhead activity, or sedentary activity.
Statistical Analysis
The outcome scores were analyzed using t tests and repeated-measures analysis of variance (ANOVA). The mean scores of the outcome measures were determined and compared at baseline and at 2-year and minimum 5-year postoperative periods. Analyses of variance with pairwise comparisons (1-way ANOVA) and Bonferroni corrections were performed to determine statistically significant differences in Rowe scores,
30
Constant scores, and ROM measures (external rotation in 90° of abduction) from baseline to 2 years and at a minimum of 5-year follow-up. The Mann-Whitney Houston pair test was used to compare follow-up related outcomes. Linear regression analysis was used to correlate the number of preoperative dislocations, time from injury to surgery, time of follow-up, and external rotation in abduction to long-term functional scores. Logistic regression was used to assess the effect of age at the first dislocation occurrence and at surgery, the number of dislocations, the number of anchors placed, the time from the first dislocation to surgery, the length of follow-up, and the status of labrum on the last follow-up clinical and imaging outcomes. Moreover, the relationship between limitation in range of movement and incidence of long-term degenerative OA was tested at the last assessment. Odds ratios were calculated to investigate whether the number of suture anchors used and reoperation may be involved in the development of degenerative changes. To assess the association between long-term imaging findings and concomitant surgical procedure (laser capsular shrinkage), odds ratios were calculated. Finally, the correlation between ROM and the scales used for evaluation was assessed. The SPSS software package, version 11.0 (SPSS Inc, an IBM Company, Chicago, Illinois) was used. A P value
Results
Sixty (46 men, 14 women) of the 72 patients were reviewed at a minimum follow-up of 5 years (mean, 8 years; range, 5-12 years) from the index operation. Twelve patients could not be located for final follow-up, although preoper-ative and intraoperative findings were available.
The demographic features of the patients who returned for the last follow-up are listed in Table 1.
Preoperative Demographics and Clinical Assessments
Clinical Outcomes
Recurrence of instability had been experienced by 10 (16.6%) of the 60 patients. Five patients with no preoperative hyperlaxity or positive examination for multidirectional instability complained of repetitive subluxation after surgery, and 5 reported a frank redislocation. The recurrences occurred within the first 2 postoperative years in almost all patients. Two or more episodes of instability were reported by 9 of these 10 patients (5 subluxations and 4 redislocations), and 5 of these 10 patients had undergone additional surgery to manage the recurrent instability.
At the latest follow-up, the results in the shoulders evaluated were graded as excellent, good, or poor using the Rowe score grading system. Forty-five of 60 (75%) were graded as excellent; 12 (20%), good; and 3 (5%), poor. Postoperatively, Rowe scores were significantly improved (P
Clinical Assessment at 2 Years and Minimum 5-year Follow-up a
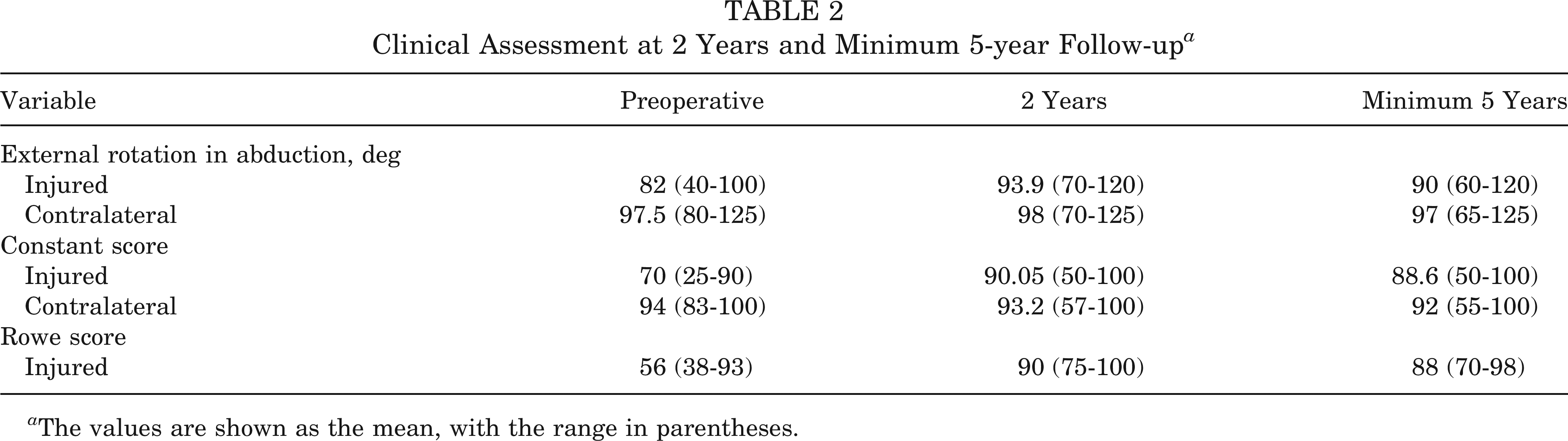
The values are shown as the mean, with the range in parentheses.
Linear regression analysis revealed that a higher number of preoperative dislocations, increased interval between surgery and time of follow-up, reduced external rotation in abduction, and additional surgery are the best predictors of decreased long-term Rowe 30 and Constant 8 scores. Time from onset of symptoms to surgery, age at onset of symptoms, and age at surgery did not influence clinical scores. There was evidence of a statistically significant association between external rotation in abduction and number of preoperative episodes of instability.
Imaging Assessment
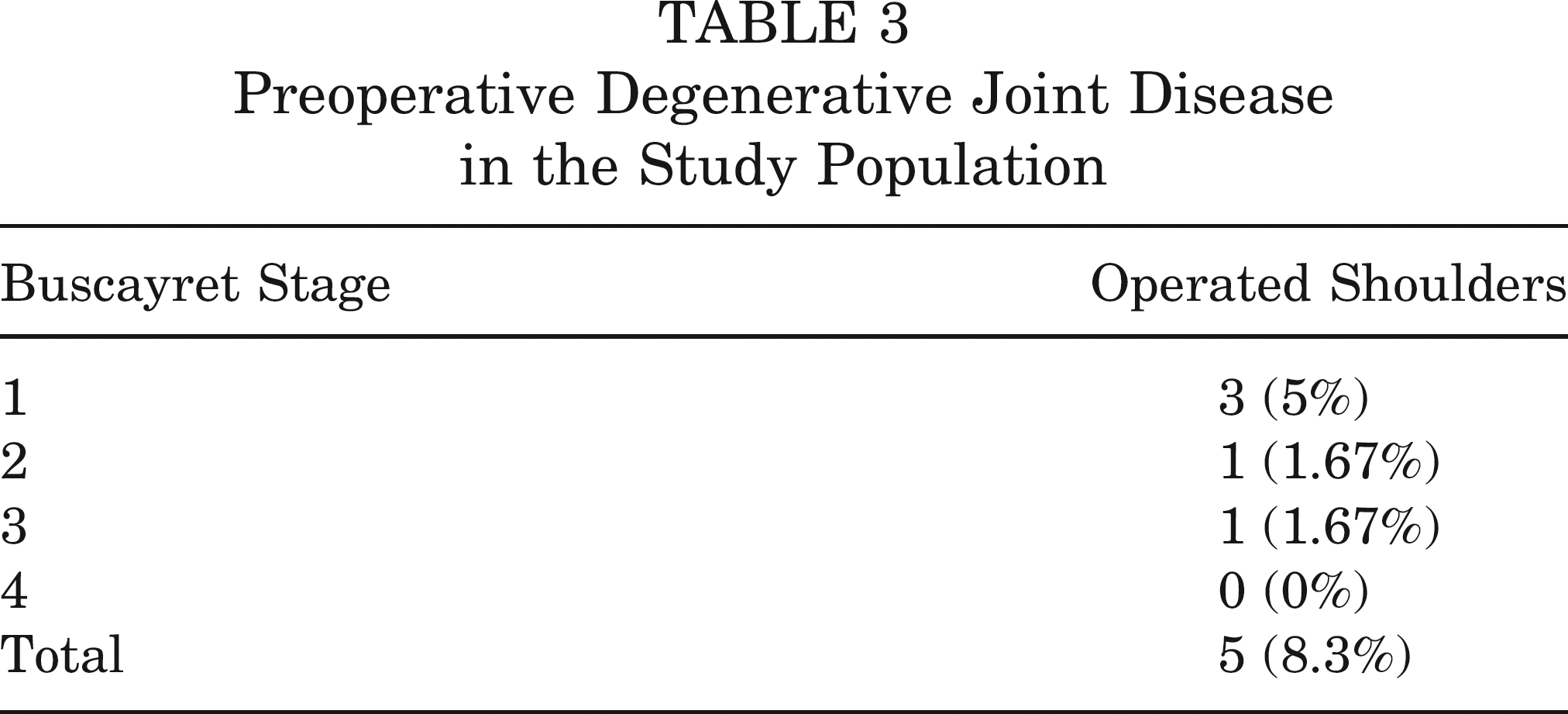
Preoperative and postoperative radiographic findings of all 60 patients were available. Comparing preoperative and minimum 5-year follow-up examinations, significantly degenerative changes were found at the latest follow-up (P < .05). At the intermediate follow-up, of the 5 (8.3%) patients with preoperative degenerative changes, 3 had no evidence of progression (Table 3), and 2 had 1-stage progression. Of the 55 (91.7%) patients without preoperative changes, 5 (10%) developed changes at 2-year review (Table 4), including 2 patients graded as stage 1, 2 as stage 2, and 1 as stage 3. At the last follow-up, all patients with preoperative degenerative changes showed signs of progression, and 12 patients with no preoperative degeneration had degenerative changes (Table 4). Additionally, patients with a higher number of dislocation episodes before the surgery were more likely to develop evidence of arthropathy (P
Preoperative Degenerative Joint Disease in the Study Population
Postoperative Progression of Degenerative Joint Disease in Operated Shoulders Without Preoperative Degenerative Joint Disease a
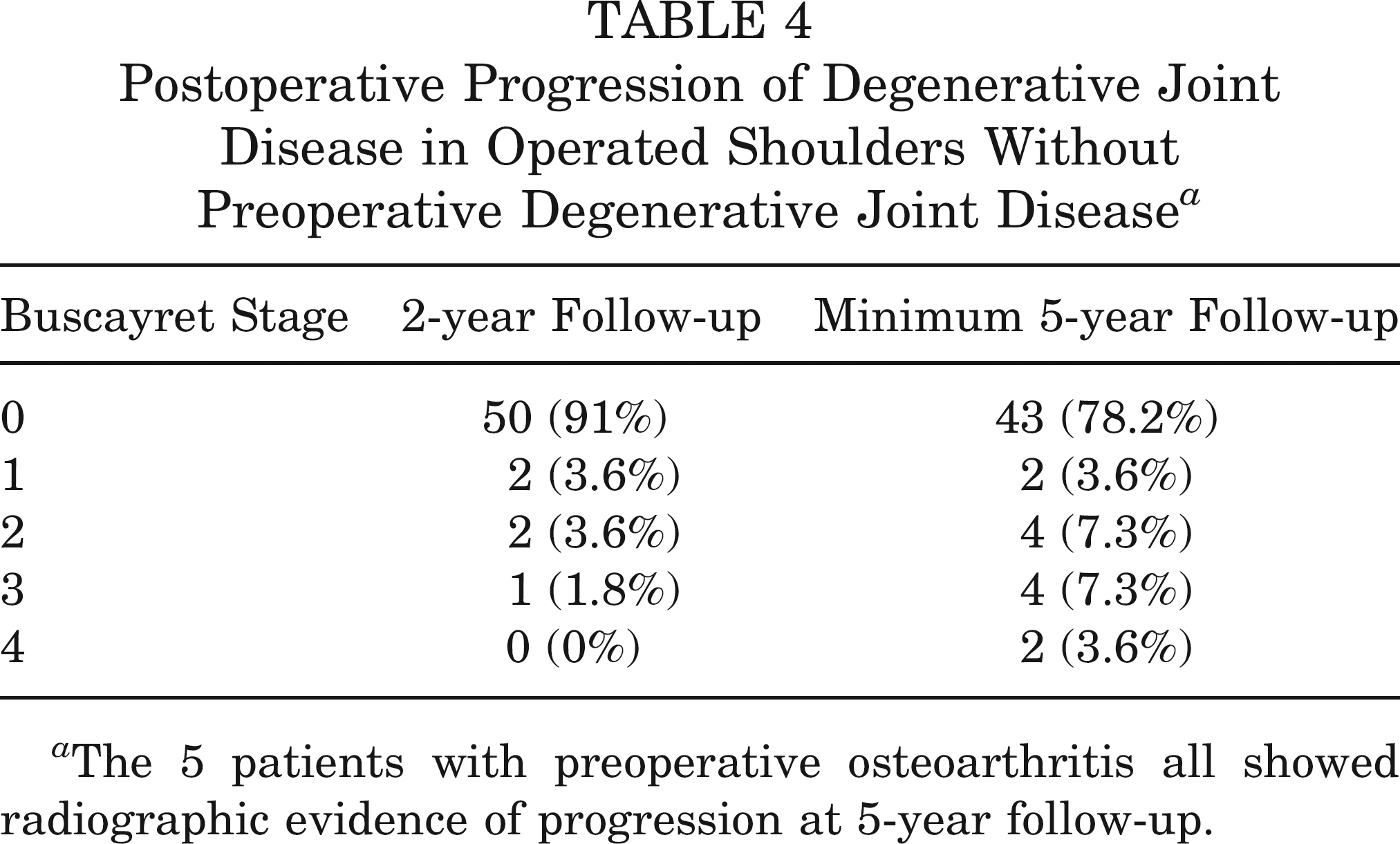
The 5 patients with preoperative osteoarthritis all showed radiographic evidence of progression at 5-year follow-up.
Logistic Regression Analysis: Arthrogenic Factors
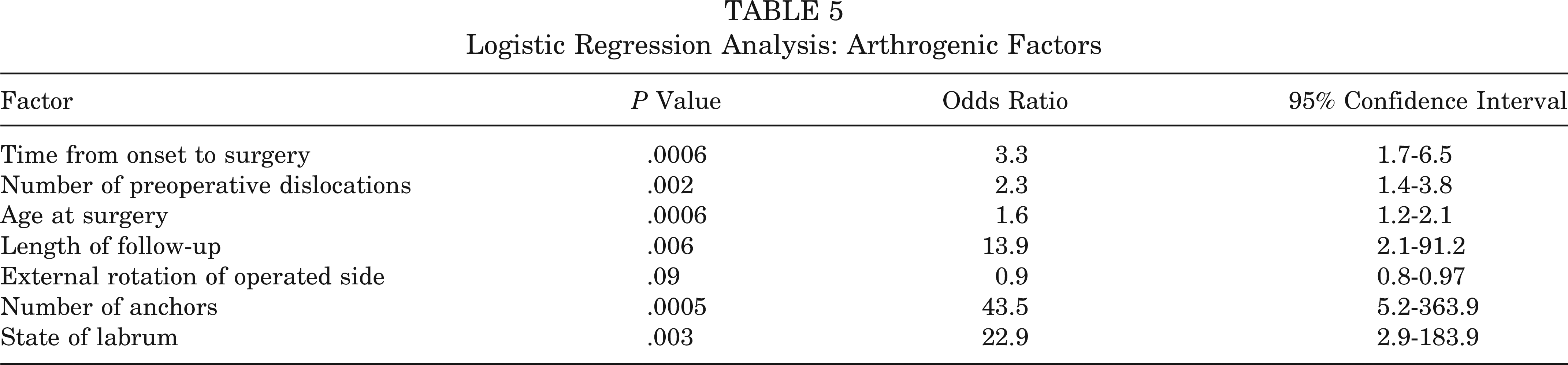
In the subgroup of patients with stage 3 or 4 glenohumeral osteoarthritic changes, the proportion of male patients and operations on dominant shoulders was slightly higher. Patients with radiographic signs of OA had lower Rowe scores (average 82) than patients with no changes (average 92), but the difference was not statistically significant (P = .237). The average of 91 in patients with no evidence of shoulder arthropathy was significantly different from the average 77.8 Constant-Murley score in patients with degenerative joint disease at imaging (P < .001). Logistic regression analysis revealed that a higher number of pre-operative dislocations, increased age at onset of symptoms and age at surgery, higher time from occurrence to surgery, more than 3 anchors, and state of the labrum are all factors associated with a higher risk of radiographic degenerative changes (Table 5).
Discussion
This study demonstrates that arthroscopic Bankart reconstruction using suture anchors resulted in increased postoperative radiographic degenerative changes compared with preoperative assessment. In the current study, of the 60 patients evaluated at the last follow-up, 12 had developed glenohumeral OA in the long term. Failure occurred in 10 of 60 operated patients (16.6%). Five patients complaining of repetitive atraumatic subluxations improved after muscle strengthening exercises without need for surgery; 5 patients experienced frank posttrau-matic dislocation after postoperative trauma similar to the trauma that produced the initial dislocation. After resistive exercises for the shoulder muscles, these patients had further recurrences during the ensuing years and required surgery.
Anterior shoulder instability is a well-established source of glenohumeral arthropathy, 22 and shoulder stabilization does not prevent an increase in degenerative changes. However, the nonoperative management of recurrent shoulder instability will also result in long-term radiographic degeneration. The high incidence of degenerative changes after surgery for recurrent anterior dislocation has been shown in medium- and long-term studies. § All recurrence data, ranging from 55% to 63%, come from studies with follow-up longer than 10 years reporting on patients operated on with open procedures such as Latarjet, Putti-Platt, and Bankart reconstruction.1,15,19,29,32 On the other hand, little has been reported on occurrence of OA after minimally invasive procedures for repair of shoulder instability. Occurring in 12 patients without preoperative imaging signs, the incidence of long-term OA was higher compared with previous studies reporting on OA after arthroscopic repair of shoulder instability.5,26 Furthermore, the patients with preoperative signs of mild degeneration on plain radiographs showed further degenerative changes over the time.
References 1, 17, 18, 24, 25, 29, 32, 33.
Buscayret et al 5 demonstrated that 5 factors potentially correlate to the development of preoperative OA after an anterior instability episode: the age at the time of the initial instability episode, tears of the rotator cuff, bony glenoid lesions, humeral head impaction fractures, and the time interval from the first instability episode to surgical stabilization. In the present study, preoperative degenerative changes were present in 5 of 60 patients, and the strict selection of patients with isolated Bankart lesions did not allow us to analyze preoperative contributing factors. We performed logistic regression analysis to investigate the factors involved in the development of long-term shoulder OA after arthroscopic management of isolated Bankart lesions. Several factors had been already identified in previous studies,5,6 but additional variables such as the state of the labrum, number of anchors, and type of anchor sutures used were included in the statistical analysis. Multiple factors were identified as contributing to postoperative OA.
As previously demonstrated, higher age at surgery was a predictor of shoulder OA. 6 In accordance with Buscayret, the number of instability episodes is statistically associated with development of postoperative OA, and the interval from the first instability episode to the surgery may predispose to development of degenerative changes. These findings suggest that earlier surgery could be useful to prevent further episodes and subsequent degenerative changes. Interestingly, degenerative changes occurred in shoulders with a median of 4 anchors placed, and a higher number of anchors predisposed to long-term OA (OR, 43.5; P = .0005). Unfortunately, the number of patients with comparable extent of Bankart lesions did not allow us to analyze statistically the role of the extent of damage in the development of degenerative changes. However, after arthroscopic assessment of the labrum, a shoulder with a more degenerated labrum (types II and III) is significantly more likely to develop degenerative changes in the long term (OR, 22.1; P = .003). No association was found between the findings at imaging and the use of metal or bioabsorbable implants (OR, 1; 95% CI, 0.18-5.46), the long-term effects of which are yet to be established.3,23 With regard to metallic suture anchors, the causative factor for arthropathy is presumed to be incorrect placement of the hardware. 28 Bioabsorbable anchors may cause cartilage damage, initiating the causal pathways involved in the development of destructive degenerative changes after shoulder arthroscopy. 31 To avoid repetitive cartilage scuffing, proper positioning of the anchors should be performed as soon as the trocar and cannula trajectory is optimized. 31
Buscayret et al 5 found a relationship between the limitation of external rotation and OA, but it was impossible to determine whether the limitation of external rotation is cause or effect of glenohumeral OA. In the present study, although external rotation of the operated shoulder was reduced compared with the contralateral side, this limitation was less than after open surgery, and a high participation rate in overhead or contact sports was recorded. This limitation in motion was not associated with imaging degenerative changes. The Constant 8 score was able to discriminate between the patients with radiographic changes and those without.
The postoperative recurrence of instability did not seem to be relevant for development of marked degeneration (OR, 1.0; 95% CI, 0.139-7.63; P = 1.0).
We are fully aware of the fact that 14 of our 60 patients underwent capsular shrinkage in addition to Bankart repair. We point out that patients undergoing additional capsular shrinkage had a 3.1 OR for developing postoperative OA compared with the other patients. In concert with other authors,7,13,21 we have now ceased using capsular shrinkage. Although our results did not reach statistical significance, we believe that capsular shrinkage is likely to be an independent risk factor for developing OA after Bankart repair. Unfortunately, the size of our cohort precluded further statistical analysis.
We point out that when a logistic regression analysis is performed in studies including fewer than 500 patients, the OR values are overestimated. The wide CIs, including 1, bear witness to the variability of the sample, a consequence of the fact that although this is a relatively large study in this specialized field, the total number of patients is still short of 500.
A major strength of the present study is the strict inclusion and exclusion criteria, allowing us to include only patients with isolated Bankart lesions, excluding patients with associated lesions. A single experienced surgeon performed all procedures, while an independent assessor performed all postoperative assessments. The small number of patients with radiographic evidence of degenerative status makes statistical analysis of the data difficult. A control study of patients with recurrent anterior shoulder instability not treated by surgery would be helpful in assessing the degree of degenerative changes found at long-term follow-up. Given the study design, it was not possible to ascertain whether the findings at final follow-up were a consequence of the original injury or were a result of the index operation. Despite these limitations, factors influencing shoulder imaging and clinical outcomes follow in the repair of a Bankart lesion.
Conclusion
In unstable shoulders undergoing arthroscopic repair of Bankart lesions, the overall clinical results were satisfactory in the medium to long term. Although multifactorial pathways have been recognized as contributors to degenerative changes after arthroscopic management, 31 the number of anchors used and state of the labrum are the most important factors associated with a higher risk of radio-graphic degenerative changes. However, as the prevalence and progression of shoulder arthropathy might continue to increase over time, there is a need for longer follow-up investigations.