
Abstract
Shoulder pain after surgery for rotator cuff disease may be caused by failed tendon repair. The diagnostic algorithm for the painful shoulder includes an assessment with ultrasonography or MRI. Although there are numerous reports on retear rates,8,19,23,24,32,39 the survival probability of rotator cuff repairs has not been published in a time-dependent manner up to now.
A few studies have assessed the integrity of repaired rotator cuff tears at more than 1 time postoperatively. One short-term study 13 and one midterm study 16 support the hypothesis that most of the repair failures happen in the early postoperative period. The only long-term study that assessed the rotator cuff integrity of their study population at 2 times found an increment of retears between the third and the ninth postoperative year, 39 while other reports argue that the retear rate may decrease because of secondary healing of retears.16,23 Therefore, conflicting results exist with regard to the increment of retears over time. Moreover, it is not clear if reruptures happen at distinct periods of increased risk.
To analyze the survivorship of rotator cuff repairs, a prospective long-term diagnostic study was designed. We sought to make clinical and ultrasound assessments of the patients at 3 months, 6 months, and 1 year and then yearly until the final follow-up. It has been shown at our institution and by others5,18 that ultrasonography is able to distinguish full-thickness rotator cuff tears from intact rotator cuffs as precisely as MRI. We hypothesized that the majority of rotator cuff failures happen within the first 3 months postoperatively.
Furthermore, we hypothesized that the long-term development of clinical parameters such as pain, abduction force, range of motion (ROM) parameters, and activities of daily living is substantially determined in the early postoperative period. Our approach of repeated combined clinical and ultrasound assessments adds useful information to the controversial question of the clinical relevance of the postoperative cuff integrity.23,24,32,39
The purpose of the study was to describe the long-term survival probability of rotator cuff repairs with follow-up data up to 11 years. On the basis of our analysis, conclusions as to the optimum time for an assessment of the rotator cuff integrity can be drawn. Additional insight in the long-term development of shoulder scores of intact rotator cuff repairs, small reruptures, and large reruptures may improve patient counseling and assist in clinical decision making.
Methods
From January 1998 to October 2002, 180 consecutive patients underwent an arthroscopically assisted mini-open repair of the rotator cuff at 1 institution. The inclusion criterion for this prospective observational case series was a full-thickness superior or posterosuperior rotator cuff tear (supraspinatus or combined supraspinatus and infraspinatus). Patients with partial-thickness or irreparable full-thickness tears, subscapularis tear, labral injury amenable for surgical repair, symptomatic arthritis of the acromioclavicular joint, or previous surgery in the same shoulder were excluded.
By this method, 107 patients met the inclusion criterion. All patients gave informed consent to participate in a long-term study.
Description of Treatment or Surgery
All patients had pain for more than 5 months despite an appropriate trial of nonoperative therapy. There were no patients with a recent injury sustained less than 6 months before the time of initial physical examination and ultrasonography. The average duration of symptoms was 7 months. Surgery was performed between 30 and 72 days after first contact with the patient. Tears were diagnosed on clinical evaluation and ultrasound or MRI examination.
All patients were examined clinically 1 day before surgery. Results were documented with the use of the American Shoulder and Elbow Surgeons (ASES) and Constant score. All operative procedures were performed by 1 senior orthopaedic surgeon. Intraoperatively, the tear was judged irreparable if during the arthroscopy and after juxtaglenoid release of the cuff, the margins of the tendon could not be pulled laterally to the footprint. Surgery was performed with the patient in a beach-chair position.
Arthroscopically assisted mini-open repair was defined as a procedure in which a tendon release; inspection for comorbid pathologic changes such as labral detachment, synovial proliferation, tendinitis, or partial tears of the long head of the biceps tendon; a tendon debridement if the edges of the torn tendon were irregular; or a subacromial bursectomy or acromioplasty were performed arthroscopically. A multipolar electrocautery device was used to do a circumferential juxtaglenoidal release and a release of the rotator interval at the base of the coracoid.
The arthroscope was then removed and an incision less than 5 cm was made in a horizontal orientation along the lateral shoulder that included the previously made portal. This approach differed from a formal open rotator cuff repair because the deltoid was split bluntly in line with its fibers and without detaching it from its origin on the acromion. A self-retaining retractor was then placed, allowing direct visualization of the rotator cuff and the humeral head. Alternatively to an arthroscopic acromioplasty, bone spurs from the acromion were removed with a flat chisel and a rasp in 4 patients. The bone was resected until the undersurface of the acromion became flat. The coracoacromial ligament was released. The attachment of the deltoid muscle to the acromion was protected in all cases.
The border of the tear was defined as fully intact tendon or the rim of a full-thickness tear or the area where full thickness of the tendon end could be determined. Intratendinous midsubstance extensions of tears in the area of the conjoined tendon of the supraspinatus and the infraspinatus were added to the total tear size. The width of the tear was recorded in the parasagittal direction, perpendicular to the long axis of the cuff fibers. Retraction in the coronal oblique plane was documented as the maximum distance between the areas of the original tendon insertion to the free end of full-thickness tendon substance expressed in millimeters.
If the tear included the rotator interval and the long head of the biceps tendon was exposed with the subscapularis intact, the width of the rotator interval was added to the width of the tear. The tear was classified as crescent-shaped, L-shaped, inverse L-shaped, V-shaped, or U-shaped. The area was calculated according to Milano et al. 21
A transosseous repair was performed in the following manner. Braided nonabsorbable No. 2 suture material (Ethibond, Ethicon, Somerville, New Jersey) was placed through the tendon edges using a modified Mason-Allen suture. Holes were then made in the debrided footprint area and sutures were placed through these holes, pulling the free edge of the tendon over the footprint (Figure 1). A 2-row transosseous fixation technique was used to place the medial row of the holes at the articular margin and the second row as far lateral as possible. The articular side limb of each suture was pulled through the medial holes and the subacromial side limb through the lateral hole. The articular side limbs of 2 modified Mason-Allen sutures and corresponding lateral limbs were tied on the lateral side of the tuberosity in a horizontal orientation. A total of 2 to 3 sutures were used through 4 to 6 holes in the greater tuberosity. Thus, fixation stress was distributed over a maximal surface area to appropriately re-create normal tendon insertion anatomy. The deltoid split was then closed in a side-to-side manner and the skin was closed in a standard fashion.
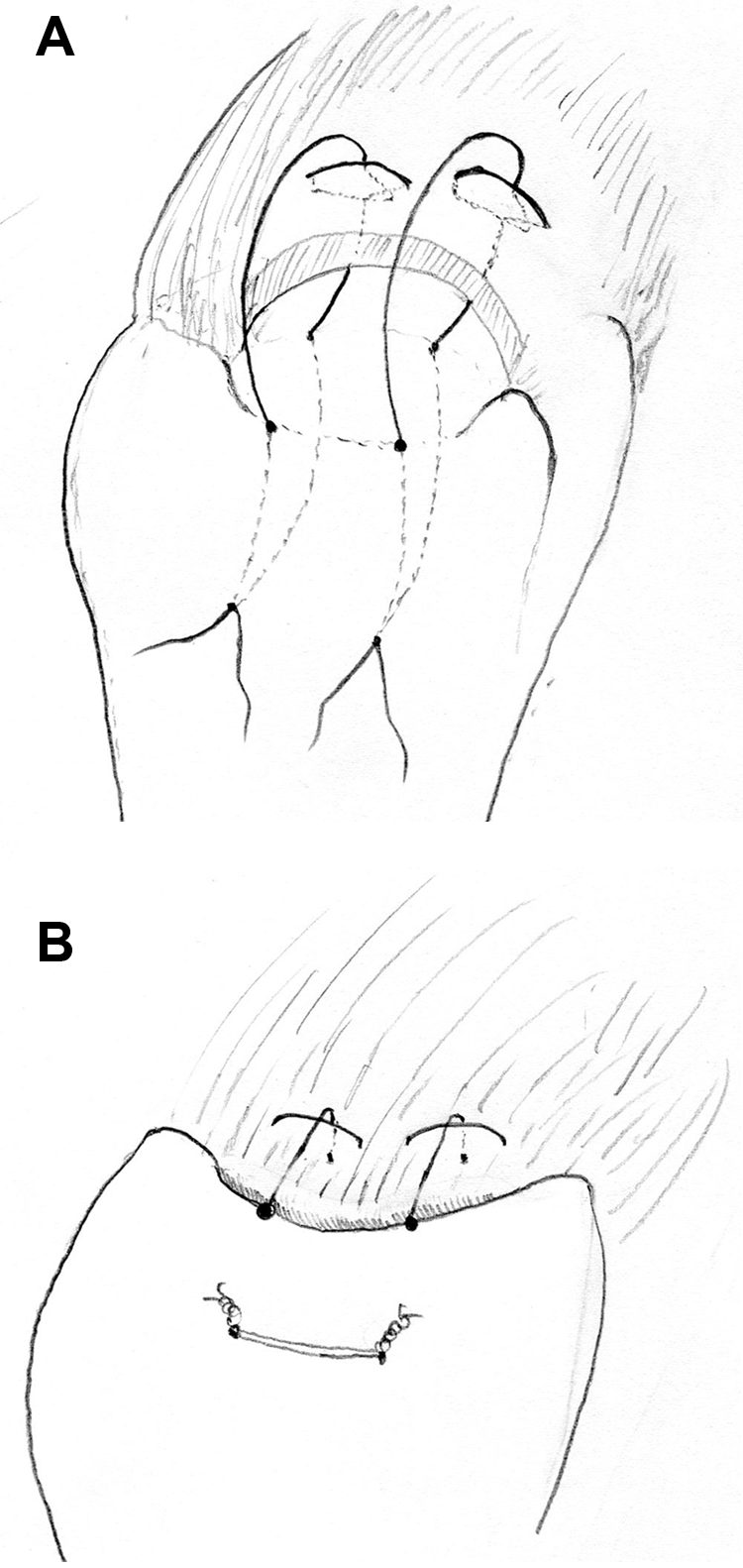
Line drawing of the transosseous double-row repair technique using a modified Mason-Allen stitch.
Postoperative Management
After the rotator cuff repair, patients were placed in an abduction pillow. The total length of immobilization was 6 weeks. Passive exercises started on the first postoperative day, active-assisted ROM exercises were started at 4 weeks, and active ROM exercises at 6 weeks. The patients were encouraged to begin ROM exercises for the elbow, wrist, and cervical spine from the first postoperative day. Light resistive exercises started at 3 months and resistive exercises progressed until full strength returned, usually at 4 to 6 months. The pace and vigor of the therapy were dictated by size of the tear and the amount of tension in the repair. At 6 months, the patient was released to unrestricted activities of daily living and began sport-specific training if indicated.
Description of Follow-up Routine and Outcome Measures
Complications were recorded following the summary of Williams. 36
All clinical follow-up examinations were done by resident orthopaedists who were blinded for ultrasound, MRI, and surgery findings. Of the scheduled follow-up examinations in the 95 patients with long-term follow-up, 5.6% of the appointments were not met by the patients for various reasons. All missed follow-up examinations were after the third year postoperatively.
Patients were evaluated preoperatively and at each follow-up examination with the ASES score, which consists of the activities of daily living score (ADL) and the visual analog scale (VAS) pain score. The Constant-Murley scoring system 4 was used in all follow-up assessments but the postoperative strength was not included in the evaluation before 6 months. Range of flexion and of abduction was determined as the angle between the humeral shaft and the midthoracic line with a goniometer and the patient seated. External rotation was measured with the arm at 0° of abduction with a goniometer. Internal rotation was measured as an unassisted movement by use of the thumb as a pointer against the anatomic landmarks. Patients reaching the lateral aspect of the thigh scored 0 points. Patients reaching behind the buttock were allotted 2 points; the sacroiliac joint, 4 points; the level of the waist, 6 points; the 12th thoracic vertebra, 8 points; and the interscapular level, 10 points. Shoulder strength measurements were done with a fixed spring balance and standardized test position. 1 The Constant raw score was then normalized on the basis of values that take into consideration age and sex-related changes. 17 The normalized Constant score according to Katolik et al 17 is calculated as follows: normalized score = (raw score/normal score) × 100. The normal score for the denominator of the equation can be determined from the values in Table IV of the article by Katolik et al.
Sports activities were assessed. Activity levels were rated both as premorbid activity level and activity level at 7 years postoperatively. The work of Iannotti et al 14 was used as a guideline. Sedentary activity was defined as no sport participation and general lifting activities not exceeding 6 to 7 kg. Low activity was defined as participation in light recreational activities such as gardening, stationary biking, golf, or other activities that do not cause repetitive stress or involve lifting of more than 10 to 15 kg. In these activities, most movements are performed below shoulder height.
Moderate activity was defined as regular participation in moderate-stress recreational sports such as racket sports, landscaping, swimming, yoga, or metal work, with potential for repetitive stress or lifting of 20 to 30 kg. In these activities, occasional overhead movements were performed. Strenuous activity was defined as regular participation in contact sports such as team handball or basketball at a competitive level. In these activities, regular overhead movements were performed including chopping wood or dirt shoveling or weight machines that impose repetitive stress, and include heavier lifting of more than 30 to 50 kg. Activity level was defined on the basis of the most strenuous work or leisure activities that the patient performed on a regular basis.
Each follow-up also included an ultrasound examination. Sonograms were performed and evaluated by an orthopaedist who had conducted more than 1200 examinations during a 4-year period.
Follow-up examinations were at 3 months, 6 months, 1 year, and every year until final follow-up.
In 94 of the 95 patients with long-term follow-up, MRI of the shoulder was done at an average of 5 years postoperatively (range, 1-7 years) to validate the ultrasonographic findings. In 1 patient, a second-look arthroscopy was used to validate the ultrasound assessment. The interval between the MRI assessment and the respective ultrasonography used for correlations averaged 2 weeks (range, same day to maximum 12 weeks).
Assessment of Sonograms
Ultrasonography thermal paper images of each patient were reviewed retrospectively and independently by 2 radiologists who were blinded to the patient’s current scores and clinical findings at follow-up. All images were then rereviewed jointly to achieve consensus. When a consensus could not be reached between reviewers, the real-time impression found by the sonographist was used as the final arbiter.
A questionnaire was completed noting the presence of an intact cuff or a full-thickness tear according to established criteria.26,35 Each radiologist also recorded whether the sonogram was diagnostic, suboptimal but diagnostic, or nondiagnostic. Nondiagnostic pictures were excluded. In 38 of 939 follow-up examinations (4%), the sonographic pictures were regarded as nondiagnostic.
Ultrasonography
Ultrasonograms were obtained with a real-time 7.5- to 10-MHz linear array transducer on a Sonoline G20 machine (Siemens, Erlangen, Germany). Images of the supraspinatus tendon were made with the shoulder extended, the elbow flexed, and the hand placed behind the back on the contralateral iliac wing. This position was necessary to expose as much of the supraspinatus tendon as possible from under the acromion. At first, the transducer was oriented perpendicular to the supraspinatus tendon, approximately 45° between the coronal and the sagittal plane defined as the parasagittal plane. It was moved anterior to posterior to visualize the subscapularis, supraspinatus, and infraspinatus tendons. The transducer was then rotated 90° to examine the tendons in a longitudinal plane (coronal-oblique plane). The examination technique included static and dynamic portions.
Criteria for Ultrasound Diagnosis of Rotator Cuff Tears
Rotator cuffs were either scored intact or a diagnosis of full-thickness tear (rerupture) was made. Criteria for a rerupture were (1) a hypoechoic zone that extended through the entire substance of the cuff, (2) a segmental or complete loss of rotator cuff substance with visible margins of a tear, (3) nonvisualization of the cuff tissue, or (4) if a focal depression was present into which the deltoid muscle could be compressed manually to separate the torn ends.26,30,35
A focal heterogeneous hypoechogenicity (distinct mixed hyperechoic and hypoechoic defect) in the rotator cuff substance, which is a sign of a partial-thickness tear, was classified as a rerupture.
Measurement of Retears
The anterior-posterior width (base of tear) and the mediolateral depth (height of tear) of the cuff retear were measured and for simplification a U-shaped tear was assumed. The area was then considered as rectangular (area = base × height). At the time of their sonographic detection, reruptures were classified as less than 2 cm2 or larger than 2 cm2.
Magnetic Resonance Imaging
Magnetic resonance investigations were done on a Magnetom Expert Plus 1.0-T MRI unit (Siemens) using a paracoronal fat-suppressed inversion recovery sequence (repetition time [TR], 4500 ms; echo time [TE], 30 ms; inversion time [TI], 150 ms), a paracoronal T1-weighted spin-echo sequence (TR, 459 ms; TE, 12 ms) and a parasagittal T2-weighted turbo spin-echo sequence (TR, 3800 ms; TE, 96 ms). The paracoronal sequences were oriented parallel to the direction of the supraspinatus muscle and tendon; the parasagittal plane was oriented perpendicular to the latter ones. The studies were archived in the hospital picture archiving and communication system (PACS).
Magnetic resonance imaging findings were independently measured on screen by 2 radiologists who were uninformed about the clinical outcome and the sonographic evaluation. Tendon signals were interpreted in consensus by the same 2 radiologists. The results of the consensus session were used for further evaluation. Using the classification of Sugaya et al, 29 number designations from 1 to 5 were assigned: type 1, repaired cuff appeared to have sufficient thickness compared with normal cuff with homogeneously low intensity on each image; type 2, sufficient thickness compared with normal cuff associated with partial high-intensity area; type 3, insufficient thickness with less than half the thickness when compared with normal cuff, but without discontinuity, suggesting a partial-thickness delaminated tear; type 4, presence of a minor discontinuity in only 1 or 2 slices on both oblique coronal and sagittal images, suggesting a small full-thickness tear; and type 5, presence of a major discontinuity observed in more than 2 slices on both oblique coronal and sagittal images, suggesting a medium or large full-thickness tear.
For MRI, the interobserver agreement between the 2 observers was calculated first including all 5 bands of the Sugaya classification and secondly differentiating intact (Sugaya 1-2) versus ruptured (Sugaya 3, 4, and 5) cuff. Comparing MRI results with consensus ultrasound only, the categories “intact” and “ruptured” were used for calculating the agreement.
Statistical Methods
Continuous data usually show skew distributions and are thus described with median, minimum, and maximum. Categorical data are described with absolute frequencies and percentages. Differences between groups for continuous data were tested by the nonparametric Wilcoxon rank-sum test. Paired data are tested by Wilcoxon signed-rank test. Categorical data are tested with the χ2 test. The Fisher exact test was used in case of sparse data. For ordinal data, a trend version of the χ2 test was used. Furthermore, the normalized Constant score at 84 months was modeled by a linear regression model with gender, age, preoperative tear size, and rerupture size within 6 months (none/<2 cm2/>2 cm2) as independent factors. Some analyses were only performed excluding traumatic reruptures, where measurements from the time of the diagnosis of a traumatic rerupture were censored and not included in the subsequent analysis.
Survival probabilities for the rerupture-free time were presented graphically with life tables, and group differences were tested with the log-rank test.
Interobserver agreement and agreement between MRI and ultrasound measurements were assessed by Cohen kappa and corresponding 95% confidence intervals (CIs) were given. A weighted-kappa version was used in case of an ordinal assessment score.
All P values given are 2-sided and P ≤ .05 was considered significant. Calculations were performed with the statistical software packages SAS (Version 9.2, SAS Institute Inc, Cary, North Carolina) and SPSS (Version 17.0, SPSS Inc, Chicago, Illinois).
Results
In this prospective study, 107 patients were enrolled with a median follow-up of 96 months (minimum, 6 months; 25th percentile, 84 months; 75th percentile, 120 months; maximum, 132 months). The average patient age of the 65 men and 42 women was 59.5 ± 9.2 years (range, 37-77 years).
A minimum follow-up time of at least 7 years and a maximum time of 11 years was achieved in 95 patients. Twelve patients were lost to follow-up in the first 7 years: 2 patients had a pacemaker implanted and could not have MRI; 3 patients moved away and could not be seen for the sequential ultrasonography; 3 patients died from causes unrelated to the shoulder surgery; 1 patient had a stroke with residual weakness on the operated upper extremity; and 3 patients underwent rerepair of the tendon, which was regarded to bias the clinical result profoundly and were thus censored at the time of rerepair.
Complications
The most frequent complication was a rerupture of the rotator cuff in 35 of 107 patients (33%). Three patients underwent rerepair of the tendon effect, as mentioned above. Of the remaining 32 patients, 6 patients (18.7%) had an arthroscopic debridement at 1 to 6 years after the initial surgery. The rationale to do a debridement rather than a rerepair was the rigid retraction of the reruptured tendon in these cases. Two kinds of complications were observed in 8 patients of the intact tendon group (8 of 63). Four of 8 patients had postoperative stiffness for more than 3 months. Of these, 1 patient had a second arthroscopic surgery and in the other 3 cases, nonoperative treatment resolved the problem. The other 4 had a subacromial impingement, which was resolved in 1 case by subacromial corticosteroid injections and in 3 cases by arthroscopic removal of subacromial scar tissue and bursitis. Altogether a second arthroscopy was done in 6.3% (4 of 63) of the patients in the intact tendon group within the first 2 years after initial surgery.
The interobserver agreement for the MRI assessment of the structural integrity of the cuff shows that MRI yields highly reproducible results for cuff integrity in our postoperative patients.
The interobserver reliability for the Sugaya classification (types 1-5) revealed a substantial agreement with a weighted kappa of 0.72 (95% CI, 0.63-0.80). Differentiating intact (Sugaya 1-2) versus ruptured (Sugaya 3-5) cuff, there was an almost perfect agreement, with a kappa of 0.91 (95% CI, 0.82-0.99).
Moreover, ultrasound proved to be very reliable with regard to the detection of ruptured versus intact rotator cuff repairs. Both investigators of MRI scans had good agreement of their results with the consensus ultrasound. Observer 1 had a kappa of 0.90 (95% CI, 0.81-0.99); observer 1 graded 4 cases type 3 (Sugaya) with MRI that were graded intact in ultrasound. Observer 2 had a somehow lower agreement, with kappa 0.81 (95% CI, 0.69-0.93); observer 2 graded 2 cases type 4 and 6 cases type 3 (Sugaya) with MRI that were graded intact in ultrasound.
At 3 months postoperatively, 75.7% of the patients showed intact rotator cuffs (26 reruptures within 3 months), and 71.9% were still without rerupture at 6 months postoperatively (there were 4 more ruptures between 3 and 6 months). All of these early reruptures were atraumatic failures that can be addressed as insufficient healing.
Five traumatic reruptures occurred later on: 1 rerupture accompanied by pain after a tennis match was detected around the 2-year assessment, and 4 reruptures attributable to slips and falls on the operated shoulder occurred between 3 and 5 years postoperatively. After a follow-up time of 84 months, 66.9% of the patients were rupture-free (Figure 2).
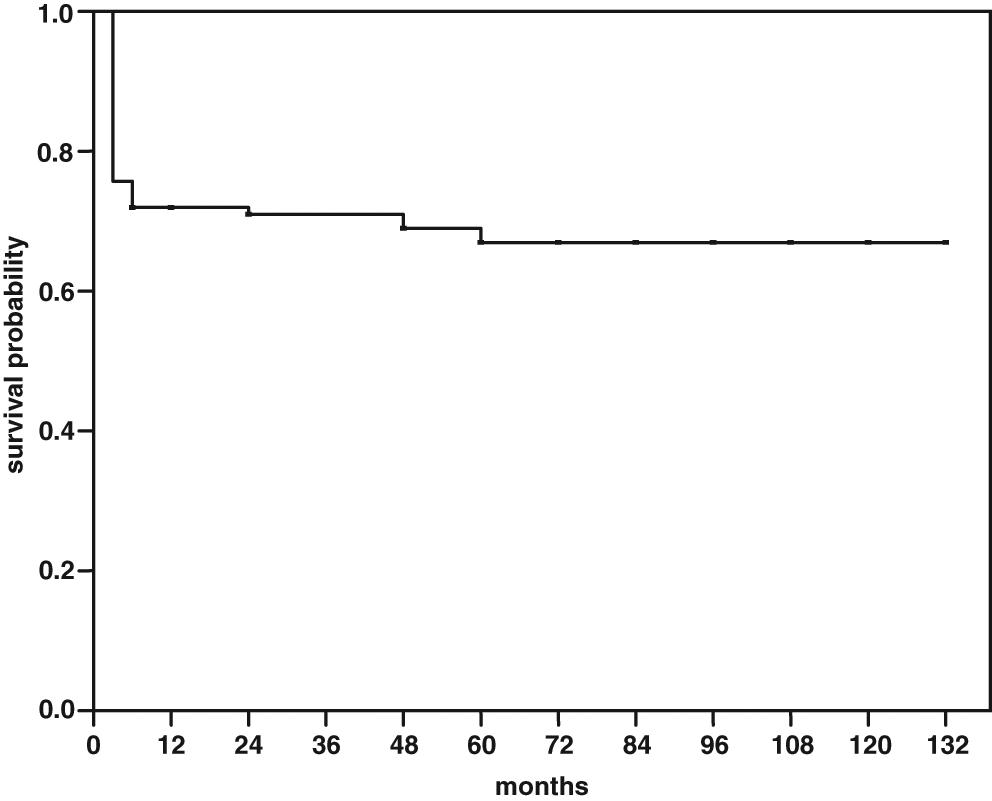
Survival probabilities for rerupture-free time after rotator cuff repairs of 107 patients. Ultrasound assessments were done at 3 months, 6 months, 1 year, and then annually.
Overall Results
The overall rerupture rate was 33%. The overall Constant score (n = 95) improved significantly (P < .0001) from a baseline median of 45 points (range, 28-78 points) to 86 points (range, 36-98 points) at 84 months. After 1 year, the median Constant score had increased to 83 points. The overall ASES score (n = 95) improved significantly (P < .0001) from a baseline median of 40 points (range, 10-67 points) to 95 points (range, 30-100 points) at 84 months. The biggest increase was observed within the first year (median ASES score after 12 months: 92 points). The overall pain score (n = 95) (VAS, 0-10) improved significantly (P < .0001) from a baseline median of 6 (range, 3-10) to 0 (range, 0-7) at 84 months (1-year median of 1 [range, 0-7]).
Assessment of medical comorbidities, body mass index, and smoking habits did not show statistically significant differences between patients with and without retears during follow-up (see Table A in the Appendix, available online at http://ajs.sagepub.com/supplemental/).
At 84 months (Table 1), patients with a healed tendon showed significantly higher Constant scores (P < .0001), VAS pain scores (P < .0001), ADL (P < .0001), strength (P < .0001), ASES scores (P < .0001), and normalized Constant scores (P < .0001), when compared with patients with retears. In addition, measures for flexion (P < .0001), abduction (P < .0001), external rotation (P < .0001), and internal rotation (P < .0001) were significantly better in patients with intact repairs when compared with those with failed repairs (Table 1).
Analysis of Subcategories: Intact Rotator Cuffs Versus Retears a
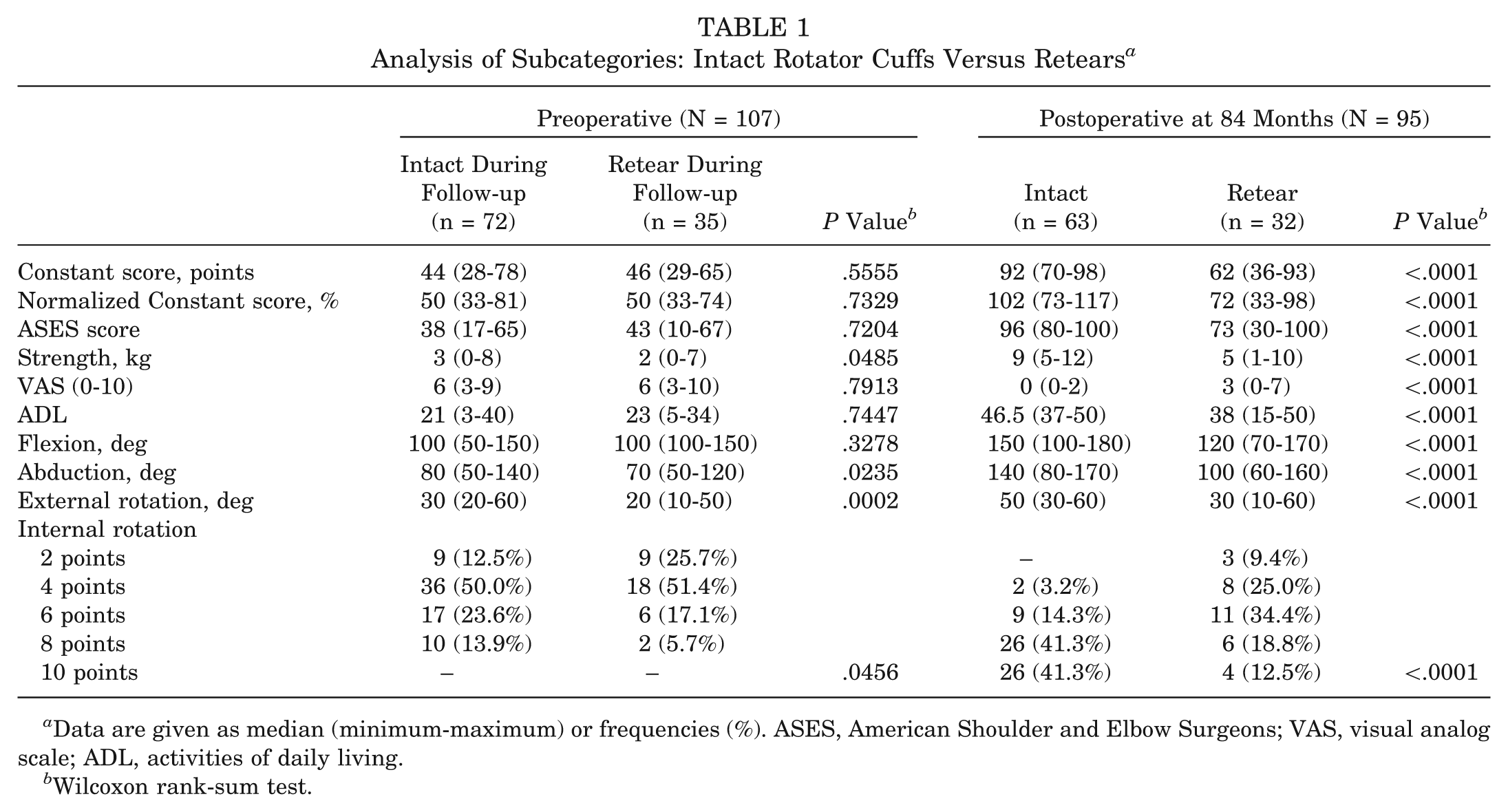
Data are given as median (minimum-maximum) or frequencies (%). ASES, American Shoulder and Elbow Surgeons; VAS, visual analog scale; ADL, activities of daily living.
Wilcoxon rank-sum test.
At 84 months (Table 2), the activity level of patients with healed tendons was significantly higher than the activity level of patients with retears.
Activity Level a
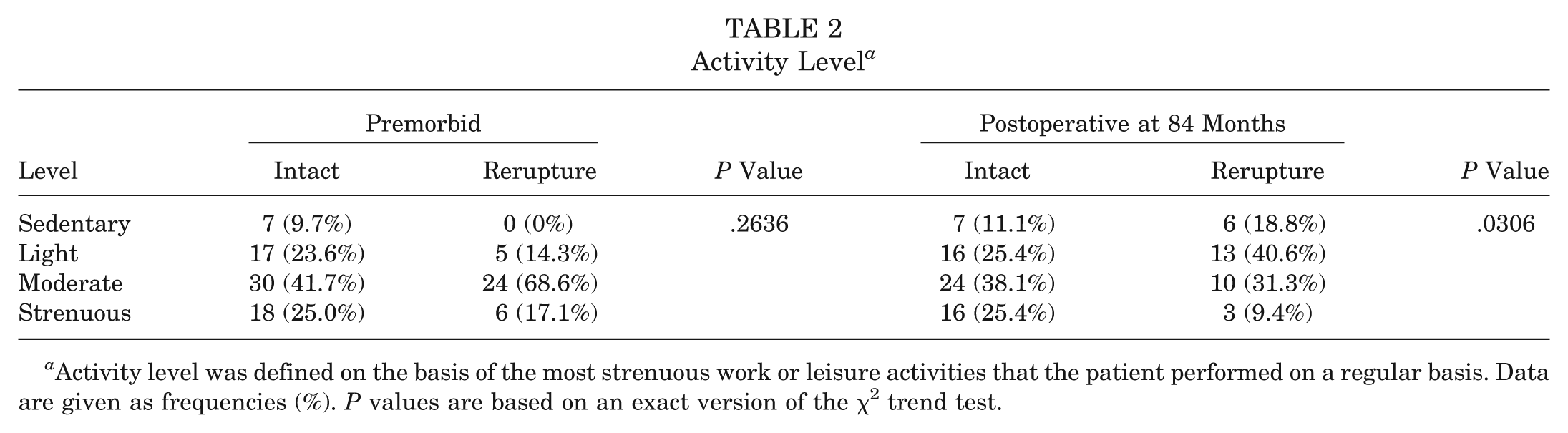
Activity level was defined on the basis of the most strenuous work or leisure activities that the patient performed on a regular basis. Data are given as frequencies (%). P values are based on an exact version of the χ2 trend test.
Patient Age and Rerupture Rate
The rerupture rate is slightly increased with patient age at first rupture (P = .5132). In the group of patients younger than 65 years (n = 77), the rerupture rate was 31.3% at 84 months. In the group older than 65 years (n = 30), the rate was 37.9%.
Preoperative Tear Size and Rerupture Rate
At 84 months, 86.3% of the patients with a preoperative tear size of less than 500 mm2 (n = 53) were still intact, whereas only 47.9% of the patients with a preoperative tear size bigger than 500 mm2 (n = 54) were still intact at 84 months (P < .0001).
Preoperative Tear Size and Clinical Parameters
Preoperative tear size did correlate with both the postoperative Constant raw score and the normalized Constant score at 84 months (n = 95). The bigger the tear size, the lower were the measured scores (rS = −.43 [P < .0001] and rS = −.36 [P = .0004], respectively). However, this correlation vanishes if patients with and without reruptures were analyzed separately. Therefore, patients with larger tears had a higher probability for retears and thus for decreased Constant raw scores and normalized Constant scores.
Analysis of the Subgroups of Patients With Atraumatic Failures
No significant differences in the ASES ADL subscore were observed between intact repairs and both <2 cm2 and >2 cm2 reruptures at 3 months and 6 months postoperatively (Figure 3). At 2 years and at 7 years postoperatively, reruptures >2 cm2 scored significantly worse than intact repairs, whereas reruptures <2 cm2 showed a marginally significant difference from intact repairs at 2 years and no significant difference from intact repairs at 7 years postoperatively (see Table B, available online).
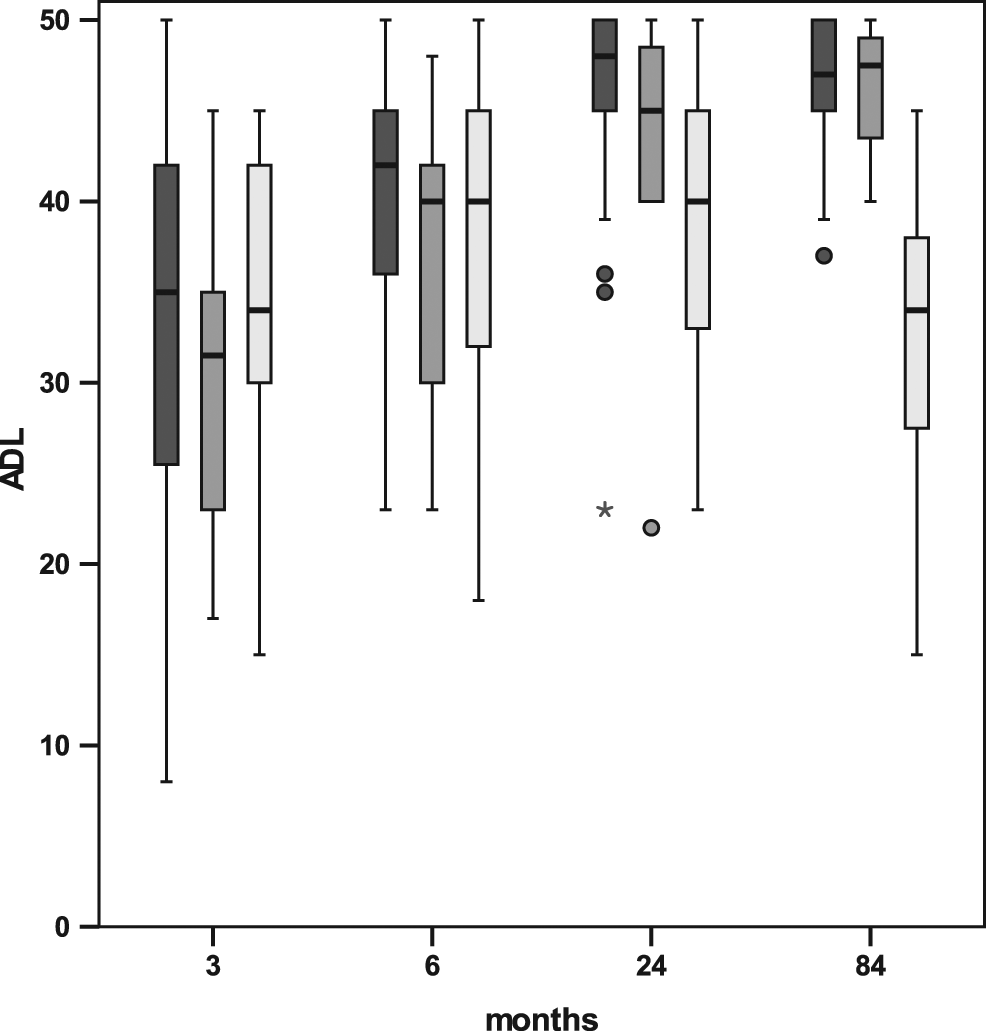
Distribution of activities of daily living (ADL) scores for intact (dark gray), reruptures <2 cm2 (medium gray), and reruptures >2 cm2 (light gray) at selected time points. At 24 months, reruptures >2 cm2 were significantly different from intact repairs with P < .0001, whereas for reruptures <2 cm2, differences are smaller (P = .0734). At 84 months, reruptures >2 cm2 remain significantly different from intact repairs (P < .0001), whereas reruptures <2 cm2 are similar to intact repairs (P = .8135).
The comparison of the ASES subscore for pain (VAS) showed that at 3 months postoperatively, patients with intact repairs and both <2 cm2 and >2 cm2 reruptures were not significantly different. However, at the 6-month, 2-year, and 7-year follow-ups, both kinds of reruptures could be clearly distinguished from intact repairs (Figure 4).
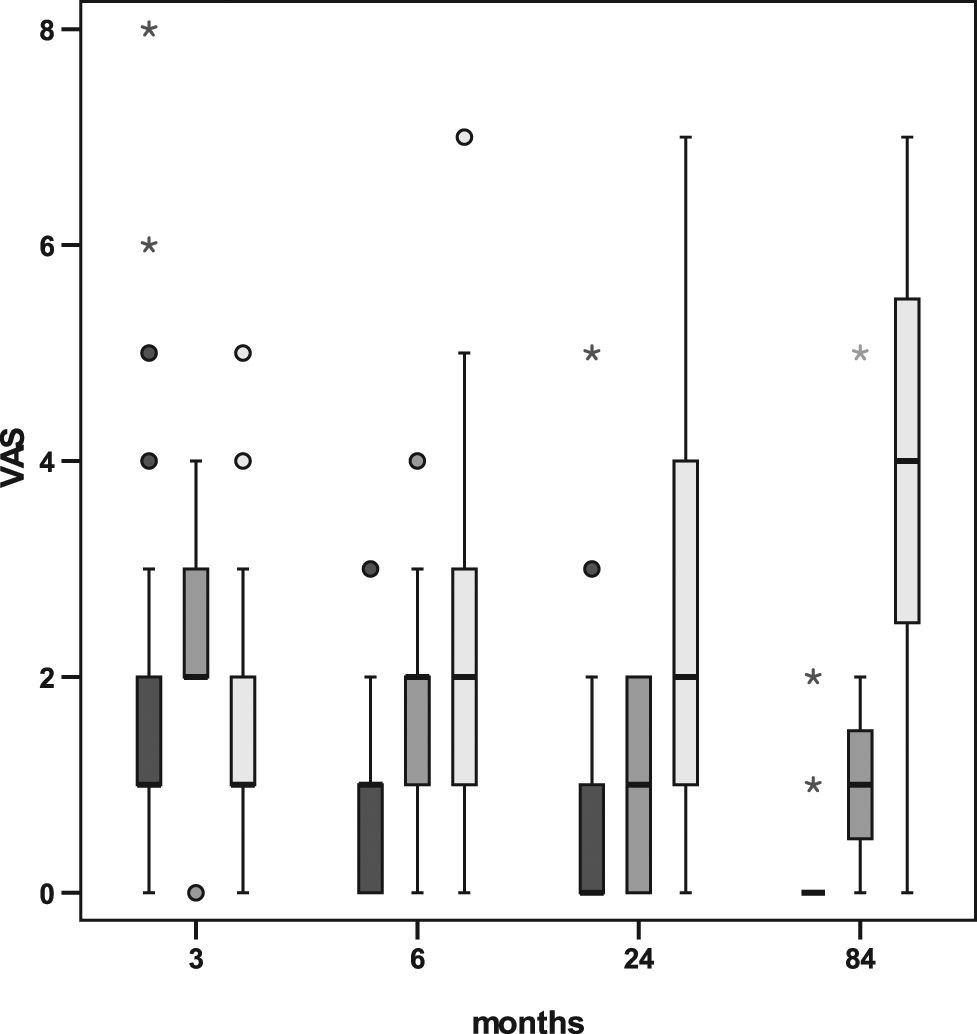
Distribution of pain scores for intact (dark gray), reruptures <2 cm2 (medium gray), and reruptures >2 cm2 (light gray) at selected time points. At 6 months, reruptures <2 cm2 and reruptures >2 cm2 were significantly different from intact repairs, with P = .0261 and P = .0013, respectively. At 24 months, reruptures <2 cm2 and reruptures >2 cm2 were significantly different from intact repairs, with P = .0180 and P <.0001, respectively. At 84 months, reruptures <2 cm2 and reruptures >2 cm2 were significantly different from intact repairs, with P = .0007 and P < .0001, respectively.
Differences between intact repairs and reruptures were more pronounced in the normalized Constant score (Figure 5, and Table B [available online]) than in the 2 ASES subscores, showing that reduced strength of abduction and ROM are indicators for a rerupture in our patients. When modeling the normalized Constant score at 84 months by a multiple linear regression with age, gender, and preoperative tear size as independent factors, then only the preoperative tear size was significant (P < .0001), similar to univariate results. However, if rerupture at 6 months and size (none/<2 cm2/>2 cm2) were added to the model, then preoperative tear size lost its significance and rerupture size is the only significant factor (P < .0001). The nonsignificant P value for preoperative tear size can be explained by the strong association between preoperative tear size and rerupture size (as discussed above). Thus the knowledge of preoperative tear size contributes no relevant additional information to predict the normalized Constant score at 84 months, as soon as the occurrence of an atraumatic rerupture and its size (usually within 6 months) is known.
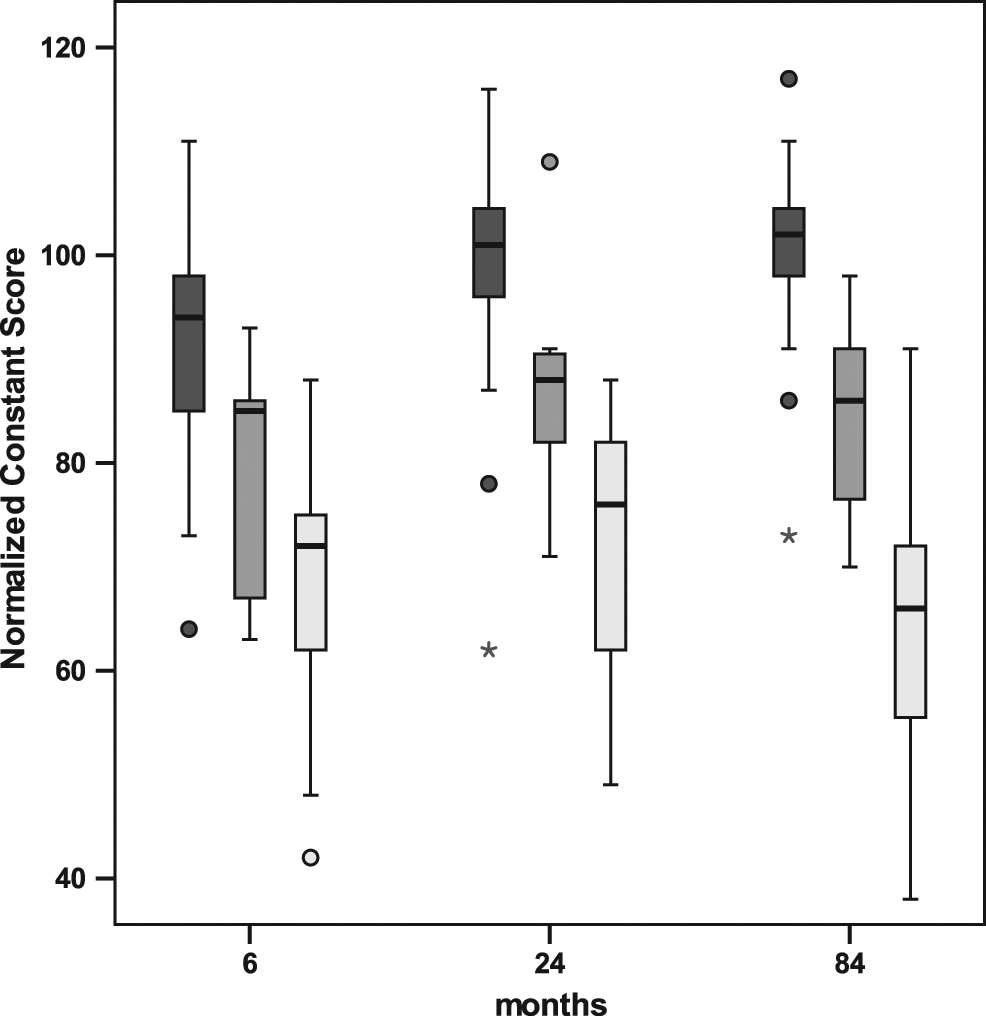
Distribution of normalized Constant scores for intact (dark gray), reruptures <2 cm2 (medium gray), and reruptures >2 cm2 (light gray) at selected time points. At 6 months, reruptures <2 cm2 and reruptures >2 cm2 were significantly different from intact repairs, with P = .0012 and P < .0001, respectively. At 24 months, reruptures <2 cm2 and reruptures >2 cm2 were significantly different from intact repairs, with P = .0006 and P < .0001, respectively. At 84 months, reruptures <2 cm2 and reruptures >2 cm2 were significantly different from intact repairs, with P < .0001 for both.
Discussion
Rotator cuff repair is a successful surgical method that provides significant pain relief and improvement of the ROM of the shoulder in the majority of patients. However, a recent review of the literature shows that important differences in clinical outcomes likely exist between patients with healed and nonhealed rotator cuff repairs. 28 Reruptures probably impair several clinical parameters of the shoulder. ‖ Interestingly, it is not known whether failures of the repair occur randomly over time or at time periods of increased risk. Moreover, the long-term postoperative development of clinical parameters of intact rotator cuff repairs compared with different sizes of repair failures are ill defined. We sought to determine the Kaplan-Meier function for reruptures of rotator cuff repairs over a maximum of 11 years. In addition, we compared the clinical development of patients with intact repairs and reruptures <2 cm2 and larger reruptures.
This is the first long-term survivorship analysis of rotator cuff repairs. Our data show that reruptures did not occur in an evenly distributed pattern over time. The great majority of reruptures (74% [26 of 35]) occurred within the first 3 months. This finding supports the notion that failure to heal is the main contributor to repair failures. Four of the 35 reruptures (11%) were detected during the active rehabilitation program between the third and the sixth month. We regard these also as nonhealed tendons, as no trauma was evident in the anamnesis. A single tendon defect of approximately 40 mm2 was detected at the 2-year follow-up and probably happened during a tennis match followed by pain and transitional weakness to lift the arm. Eight patients reported a slip and fall on their arm during follow-up and were subsequently seen for a sonographic control. Four of these patients had a traumatic rerupture (11% [4 of 35]). A few studies have addressed healing rates of a single patient series at different time points. Our results are supported by a study by Huijsmans et al, 13 who found that 56% of failures occurred within 3 weeks after surgery and 44% happened between 3 weeks and an average of 22 months. Similarly, Nho et al 23 reported that 100% of reruptures in their patients occurred within the first 3 months postoperatively during an observation period of 2 years. On the other hand, a significant rate of late reruptures has also been described in the literature. Zumstein et al 39 noted that the rerupture rate increased from 37% to 57% at 3.1 and 9.9 years, respectively. Our data suggest a much less dynamic change of the repair integrity after the second postoperative year, which is in accordance with a study by Gerber et al, 11 who evaluated 12 patients at 1 to 2 years and later than 2 years postoperatively. The authors state that “neither healing of a retear nor the presence of an additional retear were observed during this interval.” Secondary healing of reruptured tendon repairs have rarely been observed. Jost et al 16 reported, for a postoperative period of 3 to 7.6 years, that of 20 reruptures, 8 healed, 7 became smaller, 2 remained the same in size, and 3 enlarged in size. We found enlargements of rerupture tear sizes in the majority of cases but only a single case of tendon healing in a small rerupture of 9 mm2 (Table 3). A statistically significant increase in the mean size of the recurrent defect has been reported in the series of Dodson et al. 6 Our data do not support the notion that tendon repair defects may heal with an incremental rate within the first 2 years postoperatively. 23
Development of Retear Size
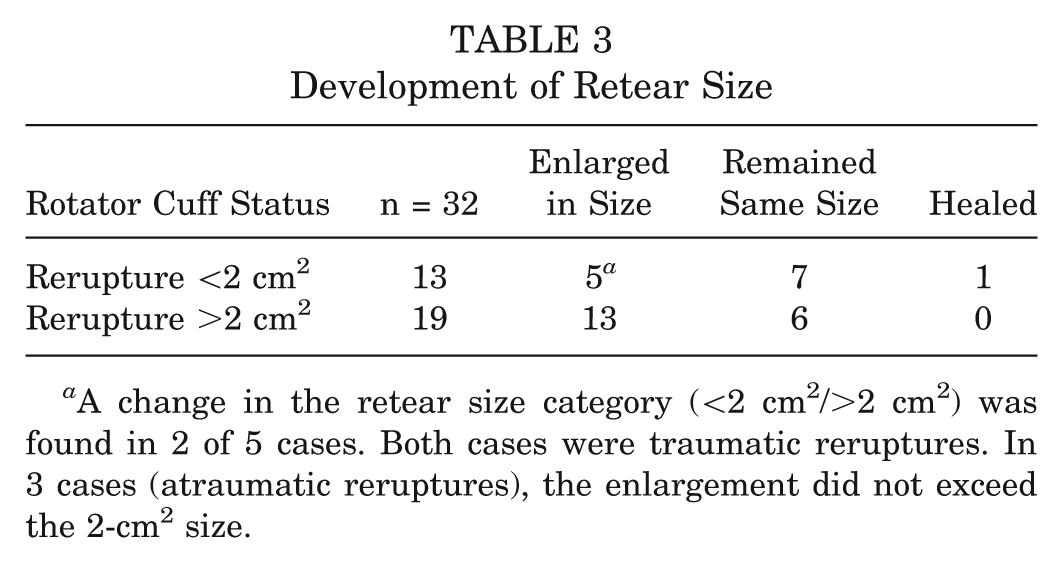
A change in the retear size category (<2 cm2/>2 cm2) was found in 2 of 5 cases. Both cases were traumatic reruptures. In 3 cases (atraumatic reruptures), the enlargement did not exceed the 2-cm2 size.
The overall clinical results of our study resemble those of previously published reports on mini-open techniques.25,27,33 We too identified preoperative risk factors for an unfavorable outcome or a retear such as preoperative tear size2,10 and age. 32 Similar to others, we found that the overall results of the Constant score and the ASES score did not deteriorate from the first year of follow-up to the final follow-up.9,25 We have used the arthroscopically assisted mini-open repair technique, but in a recent meta-analysis on arthroscopic versus mini-open rotator cuff repair by Morse et al, 22 no difference in clinical outcomes between the 2 techniques was found. In addition, one of the studies that were included in the review by Morse et al reported a comparison of rerupture rates between all-arthroscopic versus mini-open rotator cuff repair. 31 The authors showed that no difference in recurrent defects was found on ultrasound at an average follow-up of 38.9 months (27% in the mini-open group versus 24% in the all-arthroscopic group). In comparison, the rate of recurrent defects in our study was 29% after 3 years.
Although repair integrity and functional outcome have been assessed together in numerous studies, ¶ a suggested correlation between the 2 parameters is still under discussion. Discrepancies between the studies have been explained by factors such as cohort numbers, evaluation of the size of the retear, imaging modalities, follow-up time, or scoring instruments, whether including abduction strength like the Constant score or not.
Several studies support our findings that patients with healed tendons can be clinically distinguished from patients with retears by the use of the Constant score,2,7,10,13,15,20,39 the ROM measurements,3,10,11,13,19,23,39 and the ASES score. 12 In particular, intact repairs have been reported to result in better forward flexion 19 ; forward flexion, external rotation, internal rotation, and abduction 39 ; forward flexion and external rotation 23 ; or significantly better forward flexion, external rotation, and abduction 10 ; forward flexion11,13; and forward flexion and external rotation 3 than failed repairs. However, a recent review article 28 on the comparison of healed versus failed rotator cuff repair describes the Constant score to be a better indicator for a rerupture than the ROM measurements. The ASES score seems to be the least valuable tool in differentiating structural results of rotator cuff surgery clinically. 28
Our study found that the size of the retear, the 2 scores that we used, and the time at which the clinical assessments were done were of importance to reveal a correlation between the anatomic and the functional outcome.
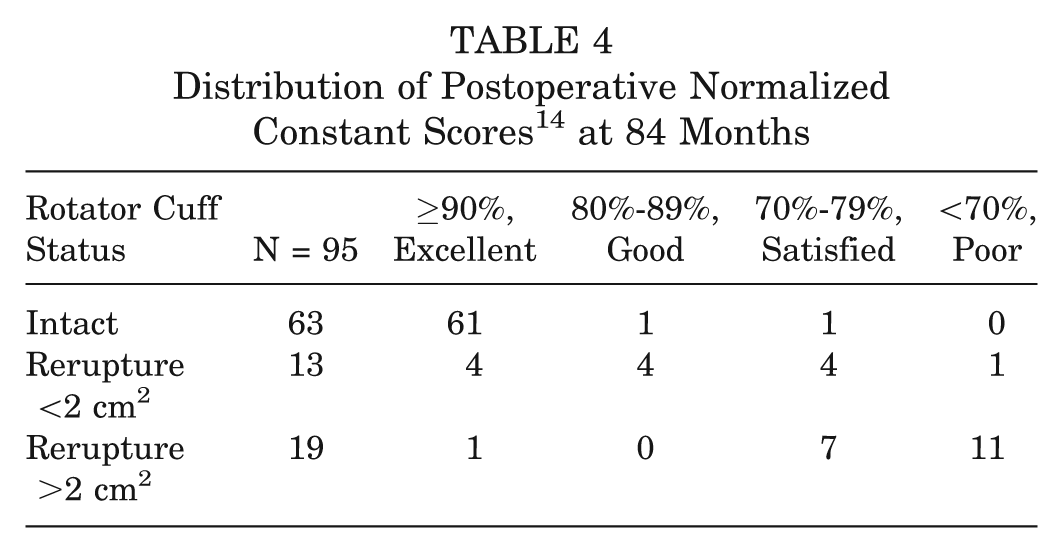
Multivariate analysis showed that patients with a healed tendon at 6 months can expect excellent normalized Constant scores at 84 months (Table 4, Figure 5).
Distribution of Postoperative Normalized Constant Scores 14 at 84 Months
Long-term Survey of Reported Pain (VAS) in Intact Repairs Versus Patients With a Rerupture a
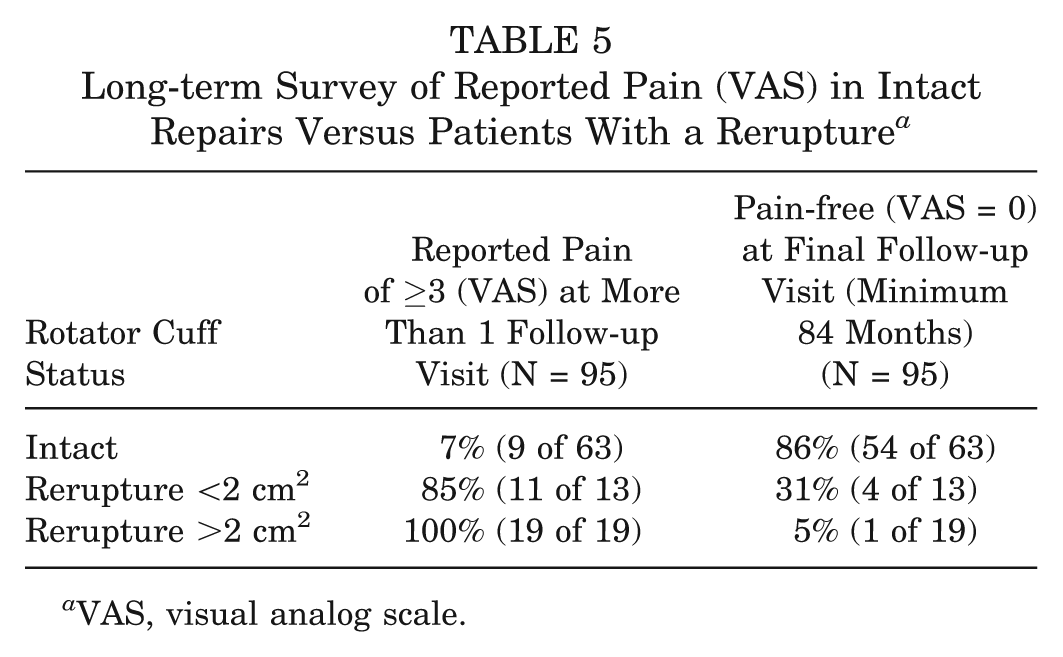
VAS, visual analog scale.
Of note, patients with supraspinatus tendon defects <2 cm2 resemble patients with intact repairs in several parameters. Except for a small statistical difference in the ADL subscore (of the ASES score) at 24 months, we found no significant differences with regard to the ADL between these 2 groups. In addition, differences in the VAS pain subscore (of the ASES score) were small. Importantly, these differences increased only marginally over time. A comparison of our data with the literature is limited by the lack of retear size evaluations in many reports. Our results are consistent with those of Dodson et al, 6 who proposed that patients with recurrent defects can remain asymptomatic over the long term but will predictably lose strength in the involved extremity. Similar to our findings, the category pain has been observed to correlate with the size of the retear.10,15 In addition, pain has frequently been observed to be different between intact rotator cuff repairs and failed repairs.10,19,23 Interestingly, 85% of the patients with reruptures <2 cm2 reported pain of more than 3 (VAS) at more than 1 follow-up, compared with only 7% of patients with intact rotator cuffs (Table 5). This finding shows that the quality of life in terms of pain is better evaluated with multiple assessments than with a single follow-up investigation. In contrast, Oh et al 24 have shown in a single clinical and structural evaluation at 19 months that patients with recurrent tendon defects had higher ASES scores and lower VAS pain scores than patients with intact repairs. Of note, our patients with intact repairs did show better Constant scores than patients with reruptures <2 cm2. This finding is explained by the differences in the abduction force observed by others2,6,10,13,15,29,39 and by us, especially after the second postoperative year.
In summary, patients with a recurrent tendon defect <2 cm2 at 6 months can expect their shoulder to perform well with occasional episodes of pain and slight impairment of the abduction force (Table 4). Clinical parameters in these patients remained stable over several years.
In contrast, patients with tendon defects >2 cm2 showed clinically relevant differences from intact cuffs in almost all parameters. Some authors have noted this correlation between the functional results and the integrity of the cuff. # Our data support the notion that the retear size is of critical importance for the long-term outcome. Moreover, an incremental impairment in all parameters was observed over the years. Whereas at the 3-month follow-up, no differences to intact cuffs were seen with regard to the ADL, ASES, and pain scores, only the difference in the ADL score remained nonsignificant up to the second-year follow-up. We explain this finding by the pain-relieving effect of the subacromial bursectomy, which is known to diminish over time.9,37 The negative effect of larger reruptures is underlined by the finding that only 5% of these patients were pain-free at the final follow-up, compared with 31% in the group with small reruptures and 86% of patients in the intact group (Table 5). Patients with reruptures >2 cm2 at 6 months showed relevant pain relief for up to 2 years. However, these patients had to cope with impairment of pain and function afterward (Table 4). Rerepairs or arthroscopic debridements were more frequent in these patients.
There are limitations to our study. Of the scheduled follow-up, 5.6% of the appointments were cancelled by the patients. However, only a single missed follow-up assessment occurred in the first 6 months postoperatively, which is the most critical phase for a rerupture. Second, the radiologic consensus session regarded 4% of the sonograms to be nondiagnostic. Although 3 of the 3-month follow-ups were nondiagnostic, the 6-month sonograms were diagnostic in these cases. A second surgery (arthroscopic debridement) was done in 19% (6 of 32) of the patients with a failed repair but in only 6% (4 of 63) of the patients in the intact tendon group. This should bias patients with reruptures in favor of those with an intact rotator cuff mainly with regard to the reported pain scores. Another potential limitation of the study is the open nature of the repairs, which might make the results less generalizable. However, a recent meta-analysis on all-arthroscopic versus mini-open rotator cuff repair, 22 as well as the study by Warner et al 34 and a study on the comparison of recurrent defects between the 2 surgical techniques, 31 showed no difference in clinical outcomes or rerupture rates.
Conclusion
The great majority of recurrent tears occurred in the first 3 months after surgical repair. Most retears appear to be a failure to heal rather than re-tearing after healing.
The parameters “recurrent tear” as well as “healed tendon” at 6 months postoperatively were predictors for the clinical outcomes at 7 years. This finding is useful for patient counseling. Efforts to improve healing during the first 3 months postoperatively should be made.
Footnotes
Acknowledgements
The authors thank Michelle Epstein, PhD, for editorial assistance during manuscript preparation and the reviewers for their helpful comments and suggestions.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.