
Abstract
Background: Hip arthroscopy is an evolving surgical technique being performed in greater numbers because of advances in skill, improved technology, and increased demand. Identifying vascular safe zones using anatomic and intracapsular landmarks provides a valuable intraoperative guide to reduce the risk of damage to the femoral head blood supply during femoral neck osteoplasty and psoas tendon release.
Purpose: This series is presented to identify vascular safe zones for use in hip arthroscopy.
Study Design: Case series; Level of evidence, 4.
Methods: The authors analyzed 76 consecutive contrast-enhanced magnetic resonance scans obtained from patients with diagnosed femoral acetabular impingement. High-resolution 3-dimensional images were reconstructed to visualize the vasculature. The medial femoral circumflex artery (MFCA) course was traced from the anterior thigh to the femoral head. Specific attention was paid to its proximity to the psoas tendon at the site of release and the retinacular vessel course in relation to the femoral neck using a clock-face orientation.
Results: The MFCA was found inserting on the posterior superior femoral neck from the 10:30 to 12-o’clock position on the femoral neck shaft, just posterior to the lateral synovial fold, and progressed on the femoral neck via an average of 4 retinacular vessels (range, 2-6). Ninety-seven percent of vessels were posterior to the 12-o’clock position. The MFCA passes posteriorly a mean distance of 50% ± 8% between the lesser trochanter and inferior femoral head/acetabular junction, located a mean 15 ± 0.37 mm medial to the medial cortex of the femoral neck. The MFCA was within the middle third zone in 100% of the measurements.
Conclusion: The authors defined the following 2 safe zones: the femoral neck osteoplasty safe zone is on the anterior half of the femoral neck; the psoas tendon release safe zone is astride the middle third of the medial hip capsule (bordered by the lesser trochanter and inferior femoral head/acetabular junction).
Hip arthroscopy can be efficacious11,15,28,33,38 and have minimal surgical complications.19,21,23,32,40 It is growing in incidence and utility because of technique advances, improved technology, and increased demand. 2 Indications have also expanded from diagnostic arthroscopy to symptomatic labral debridement and repair, femoral and ace-tabular osteoplasty for patients with femoral acetabular impingement,24,39 and psoas tendon release for recalcitrant snapping hip syndrome.3,10,14,25,47
However, as with any surgical procedure around the hip, the tenuous blood supply to the femoral head can be compromised. The major blood supply to the femoral head in adults travels from the medial femoral circumflex artery (MFCA) to the retinacular vessels. ‖ The MFCA branches off the femoral profunda artery anteriorly and passes posteriorly between the psoas, the pectineus, and the obturator externus as it inserts posteriorly on the greater trochanter. The vessel enters the capsule on the posterior aspect of the femoral neck, giving off the retinacular vessels. These vessels then course on the posterior aspect of the femoral neck in the subsynovial layer and enter the femoral head. Damage to these vessels is known to cause avascular necrosis of the femoral head. 13 Thus, the hip arthroscopist must be cognizant of vessel proximity to avoid significant complications to femoral head perfusion.
References 6, 7, 17, 27, 30, 31, 35, 36, 42.
Much of our understanding of the blood supply is based on cadaveric studies.20,26,43 Gautier et al 17 described the precise vessel course as it specifically related to surgical hip dislocation and femoral acetabular impingement (FAI). Moreover, Lavigne et al 30 further documented the distribution of vascular foramen around femoral neck. Specifically addressing arthroscopic femoral cam osteoplasty, Sussmann et al 44 addressed the risk to the retinacular vessels using arterial dye perfusion. However, these previous studies have been limited by specimen selection, small subject sizes, and gross dissection.
The purpose of the current study is to apply findings from high-resolution, 3-dimensional, contrast-enhanced MRI in patients undergoing hip arthroscopy to identify vascular safe zones during hip arthroscopy using anatomic and arthroscopic landmarks. We traced the MFCA course from the anterior thigh to the femoral head. Specific attention was paid to its proximity to the psoas tendon at the site of release and the retinacular vessel course in relation to the femoral neck. Our findings may provide a valuable intraoperative guide to reducing the risk of damage to the femoral head blood supply during femoral neck osteoplasty and psoas tendon release.
Methods
After institutional review board approval was obtained, we performed a retrospective review of 76 patients with diagnosed FAI who underwent a delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) scan as part of the department's clinical protocol for FAI. The clinical protocol consists of indirect arthrography to assess labral and cartilage damage as well as dGEMRIC imaging to assess biochemical changes in articular cartilage. Image interpretation was via OsiriX (OsiriX Foundation, Geneva, Switzerland), an image processing application specifically designed for navigation and visualization of multidimensional DICOM (Digital Imaging and Communications in Medicine) images. Within this application, specialized 3-dimensional multiplanar reconstructions (0.62-mm cuts) were performed to allow accurate fine-cut high-resolution visualization of the hip vessel anatomy and manipulation along 3 rotations of axis. Measurements focused on the location of the MFCA in relation to the psoas tendon and the location of the retinacular vessel course on the femoral neck. Data were obtained by 2 orthopaedic surgery residents who received OsiriX training from a senior author (Y.J.K.) with extensive knowledge in MRI interpretation. Image interpretation was by 2 authors who independently reviewed and reached consensus on any differences. Interobserver and intraobserver variations were measured using a random sample of the study.
Magnetic Resonance Imaging
In all cases MRI was performed after intravenous gadolinium enhancement (indirect magnetic resonance arthrogram). Each patient received 0.4 mL per kg body weight of the Food and Drug Administration–approved contrast agent gadopentetate dimeglumine (Magnevist, Berlex Laboratories, Wayne, New Jersey) approximately 30 minutes before MRI.
Magnetic resonance images were obtained using a 1.5-T system (Avanto, Siemens Healthcare, Erlangen, Germany). A 3-dimensional isotropic true fast imaging with steady-state precession (true-FISP) sequence with water excitation for fat suppression (repetition time, 12.57 milliseconds; echo time, 5.48 milliseconds; field of view, 160 × 160 mm; flip angle, 30°; isotropic resolution, 0.63 mm; generalized autocalibrating partially parallel acquisition [GRAPPA] parallel acquisition technique [PAT] 2; single average) was selected.
MCFA Location at Psoas Tendon Release
The MFCA was first identified in the anterior thigh in the T1 fat-saturated coronal plane reformats (Figure 1A). Confirmation was made by identifying the psoas tendon, pectineus, and obturator externus muscles surrounding the vessel. Standardization of the coronal cut for measurement was made by using the cut 10 mm anterior to the most medial portion of the lesser trochanter. This was done to best replicate intraoperative visualization. We then selected the lesser trochanter, the inferior femoral head/acetabular junction, and the medial femoral neck cortex as reference points of measurements. All are readily visualized during both hip arthroscopy and intraoperative fluoroscopy. We made 3 separate distance measurements: MFCA to the lesser trochanter, MFCA to the inferior femoral head/acetabular junction at the medial synovial fold, and MFCA to the medial cortex of the femoral neck (Figure 1B). Both the distances from the lesser trochanter to the MFCA and the inferior femoral head/acetabular junction were taken as a percentage of the total distance from the lesser trochanter to the inferior femoral head/acetabular junction (Figure 1C). This percentage was taken to allow for a proportional assessment between the landmarks to facilitate the surgeon intraoperatively. Interobserver and intraobserver reliability of this percentage was measured. Using simple descriptive statistics, we calculated the mean percentages and their standard deviations to compose a psoas tendon release safe zone (Figure 1D).
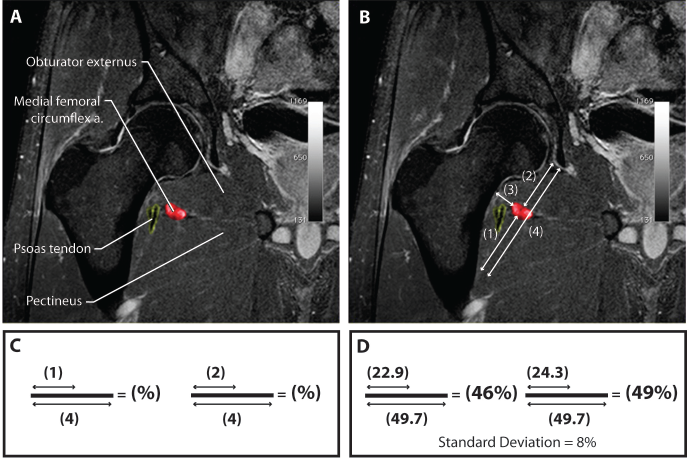
Summary of measurements for determining the psoas tendon release safe zone. A, coronal T1 fat-suppressed image of the hip identifying the medial femoral circumflex artery (MFCA; in red), its associated muscle borders, and the psoas tendon (outlined in yellow). B, measurements were made between the MFCA and intraoperative landmarks of (1) the lesser trochanter, (2) the inferior femoral head/acetabular junction, and (3) the medial cortex of the femoral neck. In addition the total distance from the lesser trochanter to the inferior femoral head/acetabular junction was measured (4). C, the distances from the MFCA to both the lesser trochanter and the inferior femoral head/acetabular junction were taken as a percentage of the total distance from the lesser trochanter to the inferior femoral head/acetabular junction. D, using the above results, in millimeters, of the measurements in (B) and (C), we calculated the percentages (means 6 standard deviations) to compose a psoas tendon release safe zone.
Retinacular Vessel Course along the Femoral Neck
Using the 3-dimensional isotropic True-FISP sequence, we centered our 3-dimensional imaging to rotate along the axis of the femoral neck, allowing for fine-cut manipulation in the axial, coronal, and sagittal planes from the greater trochanter to the femoral head, visualizing serial fine-cut sagittal reconstructions from the MFCA insertion at the greater trochanter (Figure 2). By exactly bisecting the femoral neck shaft axis, we were able to identify the course of the retinacular vessels along the femoral neck to where they enter the femoral head.
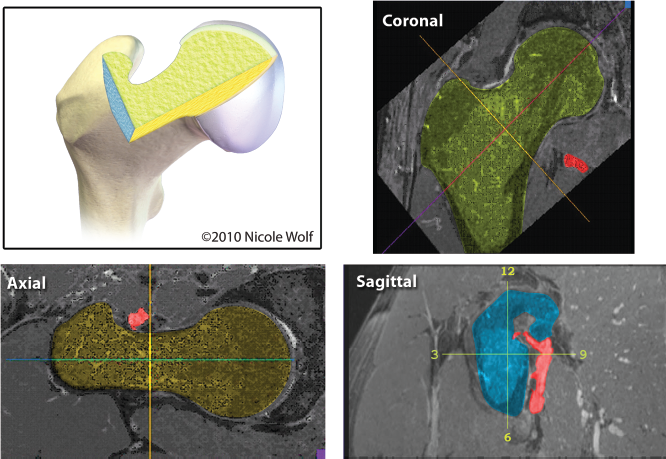
Using the 3-dimensional isotropic True-FISP sequence in the coronal, axial, and sagittal plane, we identify the medial femoral circumflex artery (MFCA) insertion on the femoral neck and follow the course of the retinacular vessels along the femoral neck axis using fine 0.66-mm cuts.
After establishing the correct imaging orientation, we identified the insertion of the MFCA onto the femoral neck (Figure 3). Using clock-face terminology to describe position, we defined our arthroscopic anatomic landmark as a line bisecting the femoral head and neck at the tip of the greater trochanter as the 12-o'clock position, with the anterior aspect defined as 3 o'clock and posterior as 9 o'clock. 30 The MFCA's insertion was recorded. The location of the lateral synovial fold was recorded. We followed the retinacular vessels medially and proximally along the femoral neck axis. The vessel number and clock location at the femoral head-neck junction were recorded where they dove subchondral (Figure 4). Interobserver and intraobserver reliability of the mean was measured. Using descriptive statistics, we calculated the mean percentages and their standard deviations to compose a femoral neck osteoplasty safe zone.
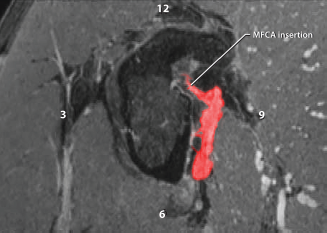
In this sagittal 3-dimensional isotropic True-FISP sequence, the insertion of the medial femoral circumflex artery (MFCA) onto the femoral neck is identified using the clock-face orientation. This is illustrated as a line bisecting the femoral neck axis at the tip of the greater trochanter as the 12-o'clock position, with the anterior aspect defined as 3 o'clock, and posterior as 9 o'clock.
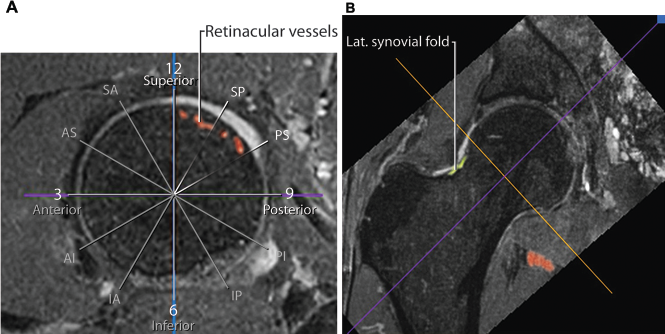
A, in this sagittal 3-dimensional isotropic True-FISP sequence, the femoral neck axis is bisected at the femoral head-neck junction with the clock-face orientation superimposed. The retinacular vessels traced off the medial femoral circumflex artery (MFCA) insertion are seen in the posterosuperior region diving subchondral. B, the coronal plane illustrates the lateral synovial fold is slightly anterior to the vessels identified in the orthogonal sagittal plane.
Results
Patients
Seventy-six hip magnetic resonance arthrogram studies of 76 patients were reviewed in this study. The average age was 30 years (range, 13–54 years). There were 36 male and 40 female patients. This sample size and distribution was sufficient to allow for the mean measurements 62 standard deviations to be incorporated into clinically relevant safe zones.
Psoas Tendon Safe Zone Release
The MFCA lies directly medial to the psoas tendon sheath between the lesser trochanter and the anterior hip capsule at the acetabulum. We observed an average MFCA location 15 mm medial to the medial cortex of the femoral neck. The MFCA's average distance from the lesser trochanter was 22.9 ± 5 mm, and the inferior femoral head/acetabular junction was 24.3 ± 5 mm (Figure 1D).
The MFCA measured at a mean distance of 46% between the lesser trochanter and 49% from the inferior femoral head/acetabular junction. The standard deviation was 8% (Figure 1D). Using interclass correlation, the interobserver variability was 0.8; the intraobserver reliability was 0.7.
By incorporating the means and 2 standard deviations each way (ie, 49 + 16 = 65, 49 – 16 = 33), the vessels were located at 33% to 66% of the distance between the lesser trochanter and the inferior femoral head/acetabular junction. To translate the percentages into a safe zone area, we divided the distance between the lesser trochanter and inferior femoral head/acetabular junction distance into thirds, correlating to the borders of the medial capsule. The MFCA vessel was reliably located within the middle third. This middle-third zone captured 100% of our measurements.
Femoral Neck Safe Zone
The MFCA was found inserting on the posterior superior femoral neck medial to the greater trochanter at an arc from the 10:30 to 12-o'clock position on the femoral neck shaft (mean, –20° [11:15 o'clock]), just posterior to the lateral synovial fold (mean, –18°), and progressed medially via an average of 4 retinacular vessels (range, 2–6) on the posterior superior femoral neck in the same 10:30 to 12:00-o'clock arc (–20° ± 10° [11:15 o'clock ± 45 minutes]) before diving subchondrally at the head-neck junction (Figure 4). Using interclass correlation, the interobserver variability was 0.8; intraobserver reliability was 0.7. Ninety-seven percent of vessels were posterior to 12 o'clock.
Discussion
On the basis of our data, we define the following safe zones: the femoral neck safe zone is on the anterior half of the femoral neck (Figure 5), and the psoas tendon release safe zone is astride the middle third of the medial hip capsule (bordered by the lesser trochanter and inferior femoral head/acetabular junction) (Figure 6).
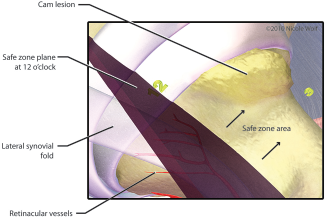
An anterolateral portal perspective on the femoral neck safe zone with labeled anatomic and intracapsular landmarks. The femoral neck safe zone is on the anterior half of the femoral neck.
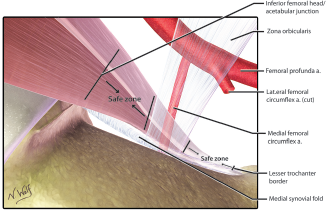
An anterolateral portal perspective of the psoas tendon release safe zone with labeled anatomic and intracapsular landmarks. The psoas tendon release safe zone is astride the middle third of the medial hip capsule (bordered by the lesser trochanter and inferior femoral head/acetabular junction).
These vascular safe zones use anatomic and intracapsular landmarks to provide a valuable intraoperative guide for avoiding damage to the femoral head blood supply during hip arthroscopy, particularly during femoral neck osteoplasty and psoas tendon release.
Femoral cam osteoplasty on the anterior femoral neck is safe from femoral head perfusion disruption. However, performing osteoplasty on the posterior superior aspect of the femoral neck should be done with caution as the retinacular vessels are likely to course within this region. We recommend using the tip of the greater trochanter or the lateral synovial fold as intraoperative landmarks. A significant majority of the retinacular vessels can be found posterior to these structures (some or all retinacular vessels course superficially and medially on the femoral neck to within very close proximity to the chondral junction of the head). We did find a small portion of retinacular vessels on the anterior femoral neck. However, they were a small minority and always had 1 or more concurrent vessels coursing on the posterior femoral neck. We predict the femoral head blood supply is not dependent on each vessel and that damage to a small portion of the vessels would be clinically insignificant.
Recently, Scher et al 41 reported a case of femoral head osteonecrosis after arthroscopic psoas tendon release and femoral neck osteoplasty. Before this, there were no reports of avascular necrosis of the femoral head as a complication of hip arthroscopy.8,9,21,23,24,29,38 However, given the significant morbidity potential, we believe an anatomic awareness during hip arthroscopy is important. We believe the wide arborization of the retinacular vessels at the femoral head/neck junction may protect from iatrogenic injury during osteoplasty. One would need to debride extensively posterior or lateral to disrupt head perfusion. The vessel arborization medially at the head-neck junction is in contrast to the vessel laterally at the piriformis fossa, where intramedullary nails, femoral neck fractures, acute and surgical dislocations, and hip resurfacing techniques have been shown to cause avascular necrosis. ¶ Thus, the risk of osteonecrosis elevates with progressive lateral or posterior osteoplasty. 21
References 4, 5, 7, 13, 16, 18, 34, 36, 37, 46.
The results of our study are in close concordance with the findings reported by Lavigne et al 30 showing that the anterior aspect of the femoral neck-head junction is essentially free of retinacular vessels. However, a subtle difference in the definition of the femoral head clock-face (12 o'clock in relation to the femoral axis as compared with the tip of the greater trochanter) should be recognized. Furthermore, they identified a greater number of vascular foramina encompassing the entire femoral neck using loupe magnification and lateral retinacular vessel foramina included, while our results focus on the MFCA and associated branches with a focus on intraoperative surgical decision making. Our findings are also in agreement with those of Sussmann et al, 44 where arthroscopic femoral osteoplasty in a 150° anterior arc demonstrated no vascular injury using arterial dye injection in a cadaver model, and identified an average of 3 vessels in the posterosuperior femoral head-neck junction.
Safe psoas tendon release can be performed astride the middle third of the medial hip capsule. Performing a release in the middle-third region risks damage to the MFCA. The MFCA is at the medial border of the psoas tendon sheath, which is only a mean 15 mm off the bone cortex.
Surgical psoas tendon release is infrequent, and most commonly indicated for recalcitrant internal coxa saltans. 45 Moreover, failure to address a tight psoas tendon during hip arthroscopy is an identified factor in revision hip arthroscopy. 19 There are 3 techniques described in the literature: arthroscopic iliopsoas tendon release through the central compartment at the reflection of the rectus femora's head and acetabular rim while the leg is in traction through the anterior portal with anterolateral visualization 12 ; an arthroscopic psoas tendon release from the peripheral compartment at the femoral head, proximal to the zona orbicularis and anterior to the medial synovial fold insertion while the leg is out of traction and flexed 30° through the anterior portal with anterolateral visualization 47 ; and an endoscopic iliopsoas tendon release at the lesser trochanter insertion, with the leg externally rotated and flexed 30°, with 2 additional portals. 25 The proximity of the MFCA in relation to these aforementioned techniques is illustrated in Figure 7. Our study results demonstrate the iliopsoas release from the central compartment is furthest from the MFCA, yet the muscle belly is directly lateral to the femoral nerve, artery, and vein at this level. While there is no reported difference between the transcapsular and endoscopic iliopsoas tendon release, 22 both techniques are potentially within millimeters of the MFCA, and the risk further potentiated with the heat of a radiofrequency tissue ablator device. An awareness of the MFCA location using landmarks will be a valuable tool for the arthroscopist.
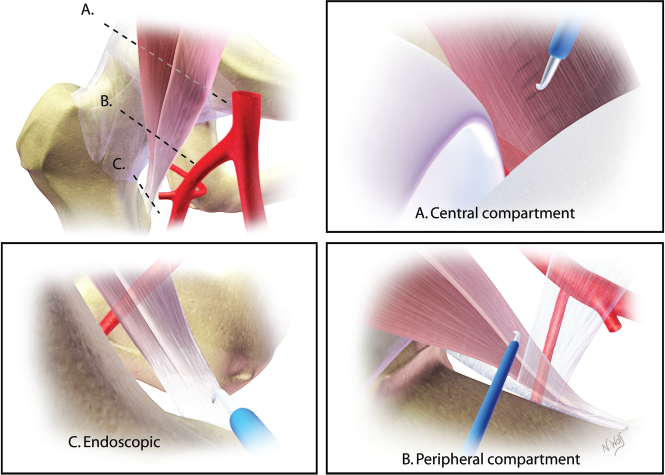
The proximity of the medial femoral circumflex artery in relation to the 3 described techniques for psoas tendon release (dotted lines), with the associated arthroscopic perspective: A, central compartment release; B, peripheral compartment release; C, endoscopic lesser trochanter release.
One strength of this study is the application of high-resolution imaging with 3-dimensional manipulations to simulate surgical scenarios and permit the identification of anatomic and arthroscopic landmarks to address a surgical risk. Moreover, this design allows for highly accurate measurements and can be performed on individuals preoperatively (software is commercially available at minimal to no cost). Our study sample were all patients with FAI and thus represents the population undergoing hip arthroscopy, resulting in strong external reliability, and with a large enough sample to develop statistically supported conclusions.
There are several limitations to this study. The safe zones are not guarantees and do not account for statistical outliers. In addition, we cannot account for the dynamic environment of the operating room where capsular pressurization, leg positioning, and patient positioning may be additional variables. We cannot provide a recommendation for avoiding vascular injury when performing cam osteoplasties on posterior-superior lesions. It is important to note that our safe zones are intended for visual estimates during surgery.
Conclusion
A surgeon needs to be aware of the location of the blood supply to the femoral head to avoid significant complications during hip arthroscopy. This is particularly relevant in femoral osteoplasty for cam impingement on the femoral head/neck and for psoas tendon release. This study demonstrates the blood supply is at theoretical risk during these interventions. However, by using defined anatomic landmarks as a guide, one can minimize complications by operating within these safe zones.