
Abstract
Patellar instability in the adolescent population is challenging because this condition is associated with various predisposing abnormalities. Successful surgical techniques used in adults may endanger the open growth plate when used in this population, so soft tissue procedures are more likely to be appropriate when significant growth remains. In the numerous soft tissue procedures described, several techniques are physis-sparing, such as vastus medialis plasty (VMP),1,15,25 medial patellofemoral ligament (MPFL) reconstruction without a bone tunnel created on the femoral side,4,8,10 semitendinosus tenodesis,5,12 medial retinaculum plication (MRP),2,11,13,14,27,29 lateral release, 7 and patellar tendon insertion transfer (Roux-Goldthwait technique).19,23 However, the clinical outcomes of these procedures on recurrent patellar dislocation in adolescents are still unknown because there are few studies found in the literature in this special cohort of patients, especially regarding studies of large series.
Clinically, we have been using MRP and VMP, as well as lateral release, as the main procedures in children and adolescents to treat recurrent patellar dislocation or instability. Open VMP is our traditional way of proximal realignment. Although it is invasive, we find its clinical results are acceptable. Arthroscopic MRPs have been reported for recurrent patellar dislocation with a cosmetic advantage,2,11,13,14,27,29 and are relatively new in our clinical practice. However, although minimally invasive, the imaging and functional outcomes of these procedures compared with open VMP were still unknown. The purpose of this study was to evaluate the imaging and functional results of arthroscopic MRP versus open VMP. Our hypothesis was that arthroscopic MRP could yield similar results to open VMP.
Methods
This was a prospective randomized comparative trial. With awareness of the limited number of patients who could be enrolled, we set α = .05, β = .8, and δ/σ = .75, to result in a supposed sample size of 29 in each group. Approval from our ethics committee was obtained regarding this comparative study and the supposed sample size. From March 2000 through October 2007, 60 pubescent patients with open epiphyseal plate were randomly divided into 2 groups through computer randomization to receive arthroscopic MRP and open VMP, respectively. At that time period, a total of 783 patients had been treated for recurrent patellar dislocation or instability in our institution by the senior author (J.Z.), including 656 adult patients and 127 skeletally immature patients. The indication for these 2 kinds of soft tissue adjustment or proximal realignment was the same—a patient having recurrent patellar dislocation with an open epiphyseal plate at both the distal femur and proximal tibia. Patients with an open epiphyseal plate at the distal femur and closed epiphyseal plate at the proximal tibia were considered near skeletal maturity and suggested to have an adult procedure. The prepubescent patients were excluded because of the incomplete ossification of the patella and femoral condyles, making CT evaluation of these structures difficult. All patients with previous surgery for patellar instability, and those with patellar or lateral femoral condyle fracture, were excluded. All patients were first advised to restrict their activity level and postpone the surgery to their adult age or near skeletal maturity, and underwent at least 6 months of nonoperative treatment. Those still having symptoms and unwilling to postpone the surgery were transitioned to operation. All patients had more than 2 episodes of dislocation and more than 1 episode required emergency hospital attendance for nonoperative treatment. The patients having 1 episode of dislocation followed by episodes of instability instead of dislocation were excluded because sometimes it was difficult to define whether the instability symptom was caused by real lateral translation of the patella or it was just a kind of “giving way,” a dysfunction of the whole knee joint attributable to various potential reasons. Patients having knee symptoms on the other leg were also excluded.
Before surgery, patellar apprehension, lateral translation grade (translation to 1/4, 1/2, 3/4, and 1 of the patellar width was documented as grade I, II, III, and IV, respectively; lateral translation greater than the whole patellar width was documented as grade V; lateral translation grade greater than III was considered as abnormal), and soft versus firm end point to lateral patellar translation in 30° of knee flexion were evaluated by the senior author. Radiographs, CT, and MRI were undertaken for all the patients. The patellar height was evaluated on the radiographic film according to the report by Koshino and Sugimoto. 17 Patellar tilt angle, congruence angle, lateral patellar angle, lateral translation, and tibial tubercle-trochlear groove (TT-TG) distance6,16,24 were evaluated on CT scan. Medial patellofemoral ligament sprain or tear, patellofemoral joint chondromalacia, or bone bruise were evaluated on MRI. The International Knee Documentation Committee (IKDC) subjective score, Kujala score, Lysholm score, and Tegner score were documented. Patients with a high-riding patella, such that the distal articular margin of the patella remained proximal to the proximal margin of the femoral trochlea in knee extension, were excluded from this study. (On the lateral view radiograph of the knee in extension, a line perpendicular to the long axis of the femur and tangential to the proximal posterior outline of the lateral femoral condyle was drawn. This line was defined as the proximal margin line of the trochlea in our clinical practice because we found it was sometimes difficult to identify the real proximal edge of the trochlea directly at the anterior side of the femur. We found that the distal edge of the articular surface of the patella remained distal to the proximal margin line of the femoral trochlea in most patients. It is normal for the patella not to fully engage the trochlea in full extension. However, it is not normal for the patella to stay totally proximal to or outside the trochlea in full extension.) Also excluded from the study were patients with supratrochlear spur or type D trochlear dysplasia,9,22 as well as patients with severe femoral anteversion or valgus knee. For these kinds of patients, the reason for exclusion was that additional surgeries in the future were suggested when growth stopped, and aggressive postoperative rehabilitation was not allowed, in contrast to those included.
Surgical Technique
Medial Retinaculum Plication
Surgery was carried out with the patient under general or regional anesthesia. The knee was examined and debrided through routine anterolateral and anteromedial portals. The arthroscope was placed in through the anterolateral portal to monitor the medial tightening. From outside the joint, an imagined irregular quadrangle was made over the medial retinaculum, with the medial patellar margin as the lateral side, a longitudinal line drawn across the adductor tubercle as the medial side, and 2 transverse lines at the level of the superior and inferior pole of the patella, respectively, as the superior and inferior sides. Then the quadrangle was transversely divided into 3 equal parts through 2 trisection lines (Figure 1A). A needle for epidural anesthesia was prebent to place 4 No. 2 Ethibond (Ethicon, Somerville, New Jersey) polyester threads through the medial side of the quadrangle into the joint and then out of the joint through the lateral side of the quadrangle, respectively, at the superior and inferior sides of the quadrangle, and the level of the 2 trisections (Figures 1B, 2A, and 2B). Through a 1-cm–long longitudinal incision made in the center of the quadrangle, dissection between the superficial fascia and medial retinaculum was performed, and the suture limbs were pulled out of the incision subcutaneously (Figure 1C). Then the lateral retinaculum release was performed through arthroscopic electrocautery or using a scissor while viewed through the anteromedial portal. With the knee at 45° of flexion and with medial pushing of the patella, the sutures were tied with SMC sliding knots to plicate the medial retinaculum (Figures 1D and 2C). At the end of the procedure, the knee was inflated with fluid and full correction of tracking was confirmed by inspection through the anterolateral portal (Figure 2D). Suction drainage was used.
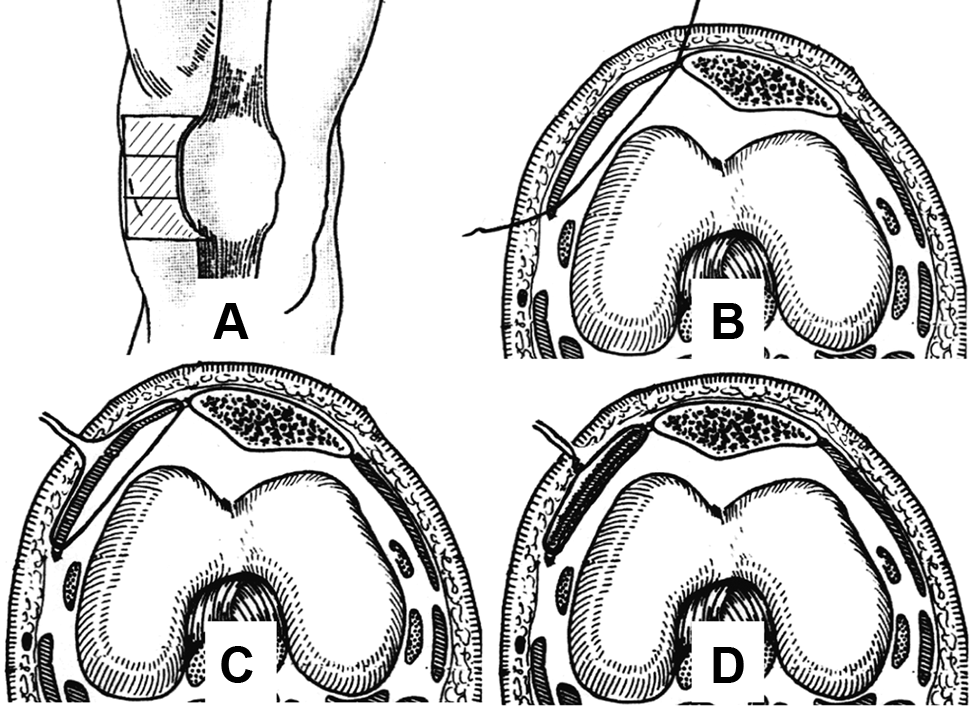
The technique for medial retinaculum plication: (A) to-be-plicated medial irregular quadrangle; (B) suture placement; (C) suture pulling-out; (D) plication by tying suture.
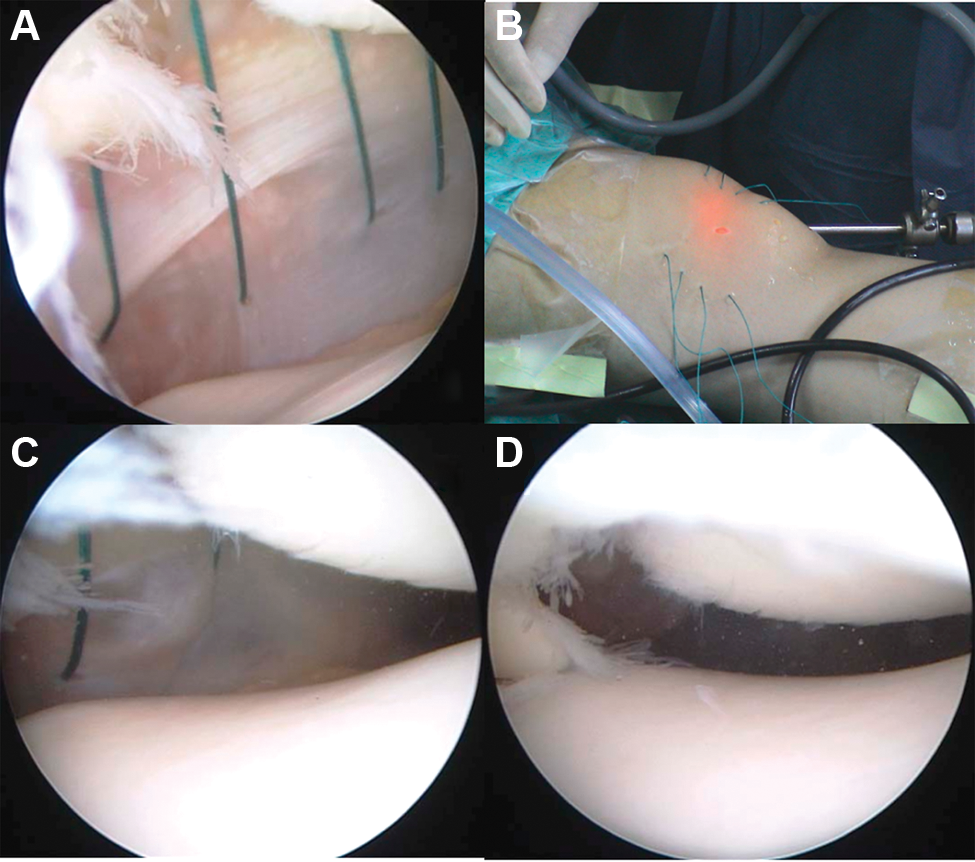
Clinical photographs of medial retinaculum plication (MRP): (A) arthroscopic view of suture placement; (B) outside view of suture placement; (C) laterally deviated patella before MRP; (D) neutralized patella after MRP.
Vastus Medialis Plasty
This was a modification of the Insall technique. A 6-cm longitudinal skin incision along the anterior midline of the knee was made from the level of the superior pole of the patella to the midpoint of the patellar tendon. Dissection between the shallow and deep fascia layers was performed to make the skin window movable. Through this mobile skin window, lateral retinaculum release from the lateral side of the tibial tubercle to 2 cm proximal to the patella was first performed. Then the direction of the lateral release was changed to along the lateral side of the vastus lateralis. The connection of the vastus lateralis to the patella was kept as much as possible for fear of quadriceps weakness. The lateral release line was kept 5 mm from the lateral side of the patella and patellar tendon to leave a soft tissue margin for holding sutures from the transferred vastus medialis in later procedures. The vastus medialis, along with the anteromedial capsule, was released from the medial side of the patella and patellar tendon. As a proximal extension of the medial release, a 3 cm long incision between the rectus femoris and vastus medialis tendon was made (Figure 3A). The synovium and fat layer under the vastus medialis and medial capsule were removed with an arthroscopic shaver. The released medial muscle–capsule structure was transferred laterally over the patella, and sutured to the lateral margin of the patella and patellar tendon (Figure 3B). The incision was closed, leaving suction drainage in place.
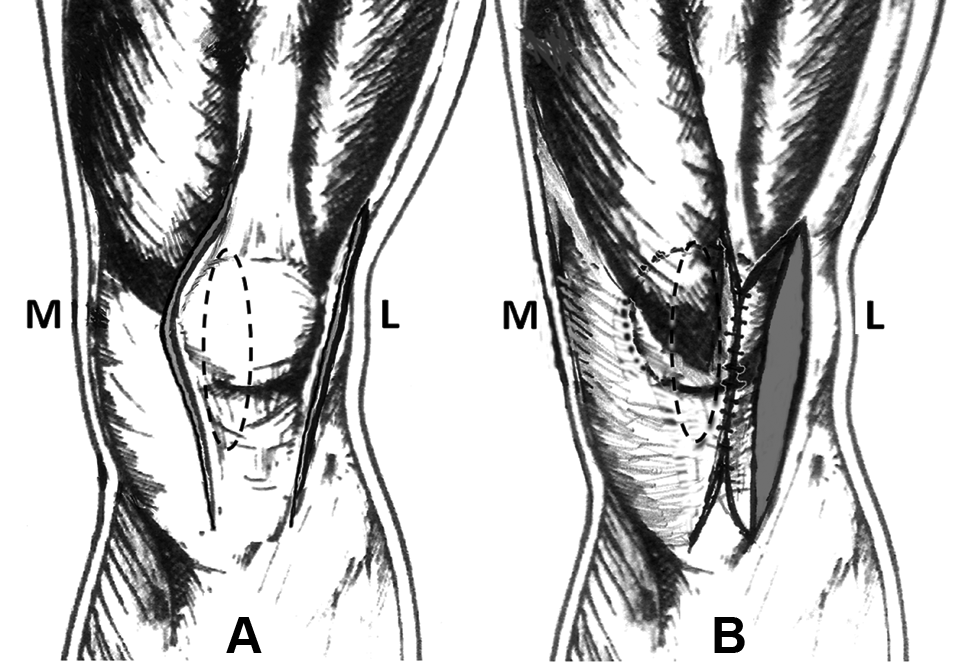
Technique for vastus medialis plasty: (A) lateral (L) and medial (M) release; (B) transfer of the vastus medialis–capsule structure to the lateral margin of the patella and patellar tendon.
Postoperative Treatment
The drainage was removed within 2 days and the patient was discharged from the hospital. The 2 groups followed the same rehabilitation protocol. A hinged brace was used for 6 weeks and locked in extension while walking. Partial to full weightbearing was allowed immediately after operation. Range of motion exercise began immediately, but knee flexion angle was restricted to 45°, 90°, and 120°, respectively, in the second, fourth, and sixth weeks after operation. Straight-leg raising, vastus medialis exercises, and proprioception training started 6 weeks after operation; running and agility training began from the fourth month.
The patients were followed up at 3, 6, 12, and 24 months and CT examination was taken immediately after operation and at 12 and 24 months postoperatively to evaluate the position of the patella. The function of the knee was evaluated at 24 months postoperatively according to the IKDC, Kujala, Lysholm, and Tegner rating scales. For those who underwent operation more than 3 years previously, a correspondence, e-mail, or telephone review was conducted to evaluate the latest patellar stability status.
CT Imaging Evaluation
The CT scan was taken in a 2-mm–thick slice. In the CT images before and after operation, the congruence angle, the lateral patellar angle, patellar tilt degree, and the lateral patellar translation were measured. The images were measured using Digimizer software (version 3.1.2.0, MedCalc Software, Mariakerke, Belgium). Because the depth of the trochlear groove, the anterior prominence of the medial and lateral femoral condyles, the width of the patella, and the tilt of the lateral facet of the patella changed in different CT cuts, we set up 2 cuts as the standard image for measurement. The proximal standard image (PSI) was the cut through the widest level of the patella to define the transverse axis, lateral facet, lateral edge, and posterior apex of the patella (Figure 4). In case the width measurement results of the patella were the same in a series of cuts, the most proximal one that cut through the thickest part of the patella was used as the PSI. The distal standard image (DSI) was the cut in which the medial facet of the femoral trochlea was most prominent to define the apex of the trochlear groove, the sulcus angle, the lateral femur line, and the anterior and posterior tangential line of the femoral condyles (Figure 4). In case the prominence of the medial femoral condyle was the same in a series of cuts, the most distal cut was used as the DSI. Measurements were usually done by copying the reference point or line from the PSI into the DSI, instead of overlapping the 2 images. The congruence angle was measured using the posterior apex of the patella in the PSI and the sulcus angle in the DSI (Figure 5A). The lateral patellar angle was measured using the lateral facet line of the patella in the PSI and the anterior tangential line of the femoral condyles in the DSI (Figure 5B). The patellar tilt was measured using the transverse axis of the patella in the PSI and the posterior tangential line of the femoral condyles in the DSI (Figure 5C). The lateral patellar translation was measured by the lateral edge of the patella, transverse patellar axis in the PSI, and the lateral femoral line in the DSI (Figure 5D). The TT-TG was measured by using the most proximal cut through the tibial tubercle and the DSI.
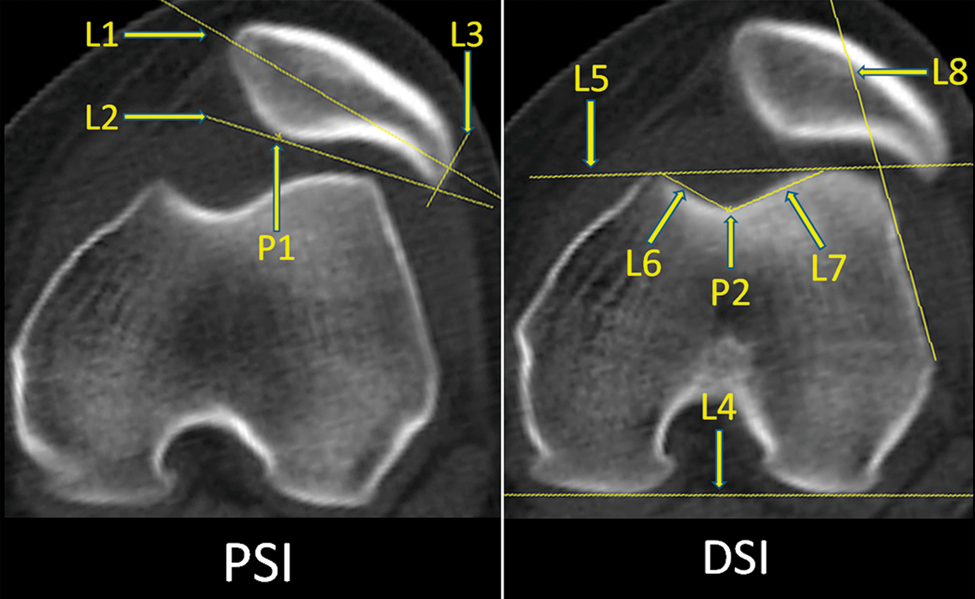
Proximal standard image (PSI) of the patella in CT examination, which cut through the widest and thickest level of the patella. L1, the transverse axis; L2, lateral facet; L3, lateral edge; P1, posterior apex of the patella. Distal standard image (DSI) of the patella in CT examination, which cut through the most prominent and distal level of the medial femoral condyle. P2, the apex of the trochlea groove; L4, the posterior tangential line of the femoral condyles; L5, the anterior tangential line of the femoral condyles; L6 and L7, the sulcus angle; L8, the lateral femur line.
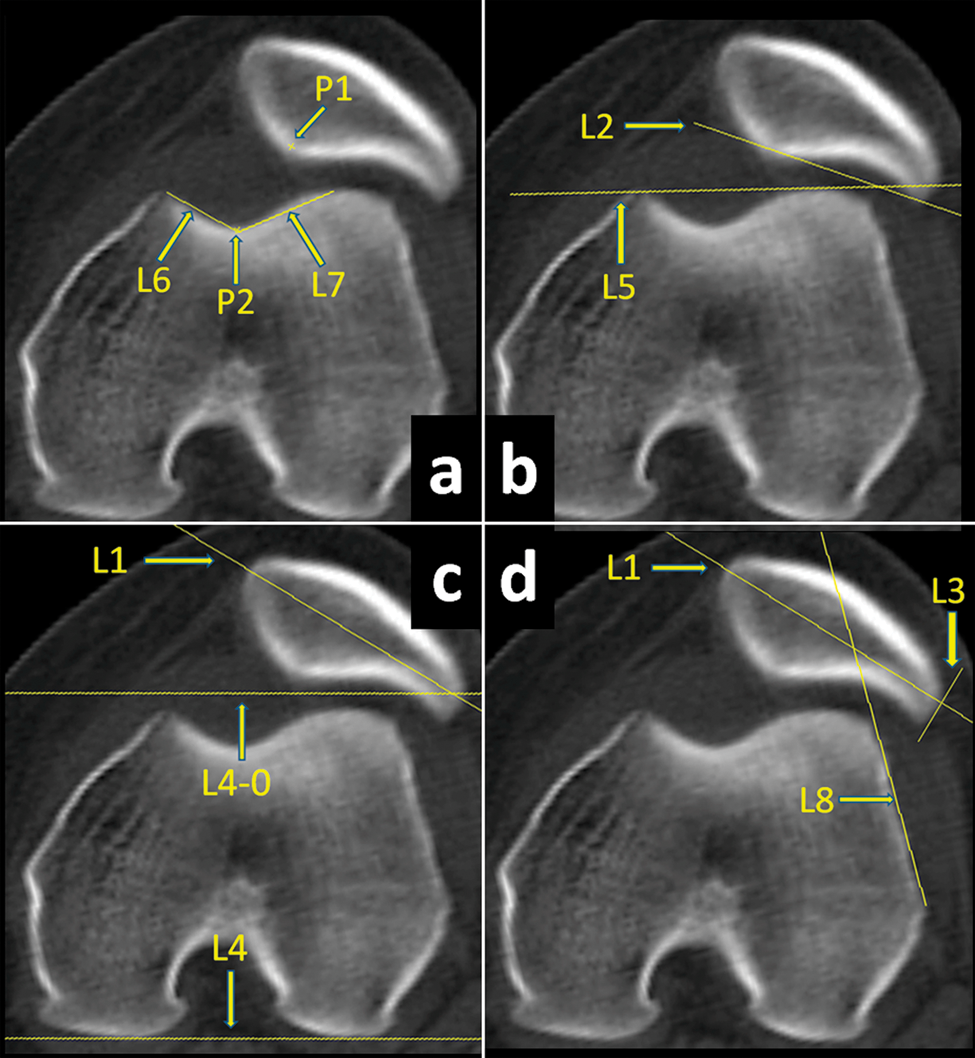
(A) Measurement of the congruence angle. P1, posterior apex of the patella in the proximal standard image (PSI); P2, L6, and L7, the sulcus angle in the distal standard image (DSI). (B) Measurement of the lateral patellar angle. L2, the lateral facet line of the patella in the PSI; L5, the anterior tangential line of the femoral condyles in the DSI. (C) Measurement of the patellar tilt. L1, the transverse axis of the patella in the PSI; L4, the posterior tangential line of the femoral condyles in the DSI; L4-0, a parallel line to L4. (D) The lateral patellar translation was measured as the distance between the 2 cross points of L3 (the lateral edge of the patella) and L8 (the lateral femoral line) on L1 (transverse patellar axis).
The preoperative measurement of the CT images was done by the senior author, and the postoperative measurement of the CT images was done by an author who was blind to the group membership of the patients.
Statistical Analysis
The measurement data of the 2 groups in preoperative examination and at each time of follow-up were compared using the Student t test, and the enumeration data of the 2 groups were compared using a χ2 test, both with .05 as significant level. Comparisons were performed between the measurement and enumeration data of each pair of preoperative and 24-month time points using paired Student t tests and χ2 tests, with .05 as significant level. In each group, the F test was first performed regarding the CT measurement result. When a significant difference was found through the F test, multiple comparisons for analysis of variance (ANOVA) between the results at each pair of time points were performed through the Student-Newman-Keuls q test. The significance level was set at .05 in the ANOVA. SPSS software (version 14; SPSS Inc, Chicago, Illinois) was used for the statistical analysis.
Results
The same surgeon performed all the operations and performed the preoperative and postoperative clinical examinations. Twenty-eight patients in the MRP group and 26 patients in the VMP group were completely followed for 2 years. Three patients were lost to follow-up because of broken contact. One was excluded because of missing the 1-year follow-up. The other 2 were excluded because they were unwilling to take the final CT examination at 2 years.
The final follow-up time was 56.8 ± 21.5 months (range, 24-92 months) and 59.1 ± 24.7 months (range, 24-88 months), respectively, in the MRP and VMP groups. In the MRP group, the ages of the patients at the time of surgery were 12 to 19 years, the duration of dislocation was 4 to 39 months, and the number of dislocations was 2 to 4 times. In the VMP group, the ages of the patients were 13 to 18 years, the duration of dislocation was 6 to 34 months, and the number of dislocations was 2 to 5 times. There were no statistical differences between the preoperative data of the 2 groups regarding gender, age, side of the knee, duration, and numbers of dislocation (Table 1).
Demographic Data of the Patients a
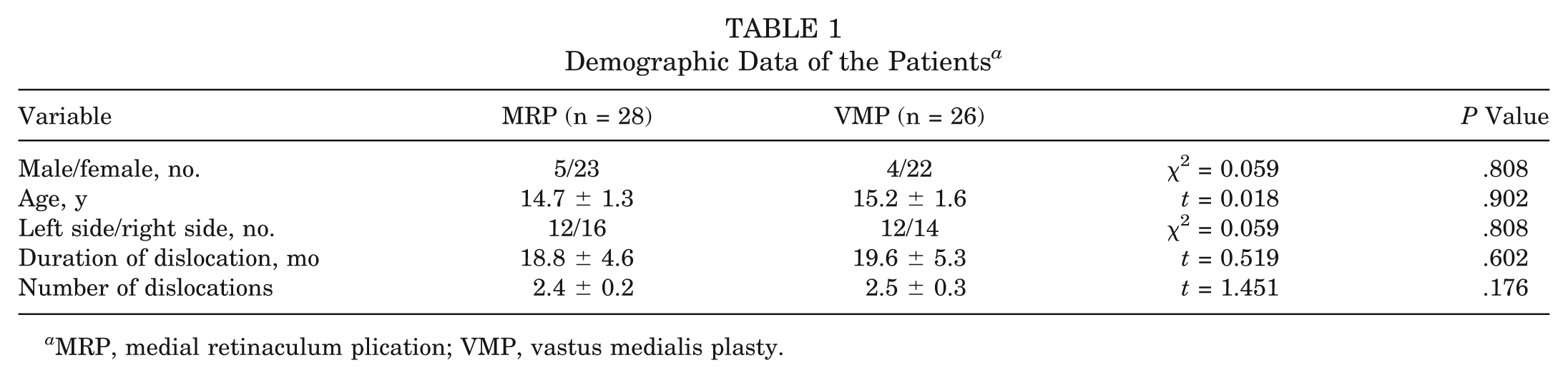
MRP, medial retinaculum plication; VMP, vastus medialis plasty.
There were also no statistical differences between imaging data of the 2 groups regarding the PT:FT (patella-tibia distance to femur-tibia distance) ratio, TT-TG distance, chondromalacia, and bone bruise in the patellofemoral joint (Table 2).
Preoperative Imaging Data a
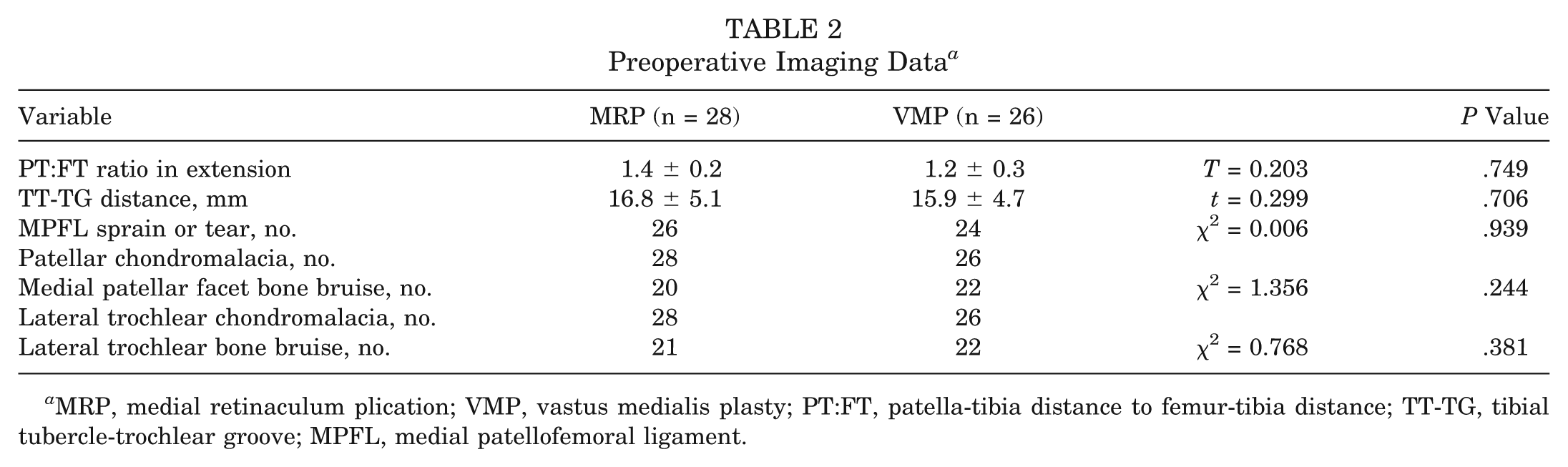
MRP, medial retinaculum plication; VMP, vastus medialis plasty; PT:FT, patella-tibia distance to femur-tibia distance; TT-TG, tibial tubercle-trochlear groove; MPFL, medial patellofemoral ligament.
Clinical Examination
Apprehension Test
Before surgery, all the patients showed positive apprehension test. After surgery, more patients in the MRP group showed a positive apprehension test at each time of follow-up compared with the VMP group, although no statistically significant differences were found between the 2 groups. Two years after surgery, 42.9% of the patients in the MRP group and 26.9% of patients in the VMP group showed positive apprehension test. There was a statistically significant difference between the preoperative and final examination in both groups (see Appendix 1, available in the online version of this article at http://ajs.sagepub.com/supplemental/).
Lateral Patellar Translation Grade
Before surgery, all patients showed abnormal lateral quadrant translation. Three months after surgery, 21 of the 28 patients (75%) in the MRP group and 23 of the 26 patients (88.5%) in the VMP group showed normal lateral quadrant translation grade. However, more patients showed abnormal results over time in both groups. There was no statistically significant difference between the 2 groups at each time of follow-up. In each group, statistically significant differences were found between the preoperative and final examination (see Appendix 2, available online).
Firm End Point in Lateral Translation
Before surgery, no patient showed a firm end point in lateral patellar translation examination. Twenty-four months after surgery, 10.7% of the patients in the MRP group and 42.3% of the patients in the VMP group showed a firm end point. There were statistically significant differences between the 2 groups at the 24-month follow-up. Regarding the preoperative and final results, no statistically significant difference was found between them in the MRP group, but a statistically significant difference was found in the VMP group (see Appendix 3, available online).
CT Examination
The measurement results of the congruence angle, lateral patellar angle, and patellar tilt angle were similar before operation. Immediately after operation, the degree of these 3 angles returned to a similar range in both groups (see Appendix 4, available online). The VMP group showed significantly greater lateral patellar angle and lesser patellar tilt angle, which may indicate more medial soft tissue tightening in this group. The VMP group showed statistically significantly better measurement results since the 3-month follow-up regarding the 3 angles when compared with the MRP group.
In each group, statistically significant differences (P < .05) were found in the F test regarding the congruence angle, lateral patellar angle, patellar tilt angle, and lateral patellar translations. Accordingly, multiple comparisons were performed between the results at each pair of time points through a Student-Newman-Keuls q test.
In the MRP group, significant deterioration of the patellar position or rotation regarding these 3 angle degrees was found in the ANOVA at the 12-month time points compared with these data at the 0-month time point, but not at the 24-month time point compared with the 12-month time point. Regarding the preoperative and 24-month results, no statistically significant difference was found between them in the ANOVA (see Appendix 4) and paired t test (Table 3).
Paired t Test Between the Preoperative and 24-Month Data in CT Examination a
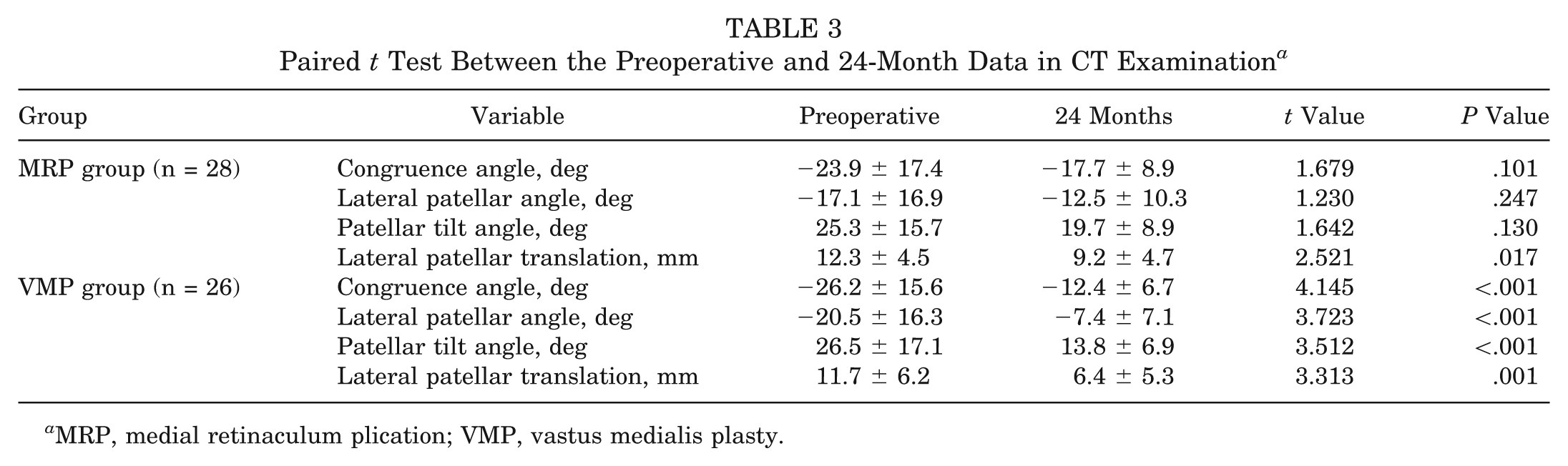
MRP, medial retinaculum plication; VMP, vastus medialis plasty.
In the VMP group, significant deterioration of the patellar position or rotation regarding these 3 angle degrees was found in the ANOVA at the 12-month time point compared with those data at the 0-month time point. At the 24-month time point, only the lateral patellar tilt angle showed significant increase compared with the 12-month time point. Statistically significant differences were found regarding the preoperative and 24-month results in both the ANOVA (see Appendix 4) and paired t test (Table 3).
Before surgery and immediately after operation, similar lateral patellar translations were found in the 2 groups. At 12 and 24 months after operation, the VMP group showed significantly less lateral translation of the patella. In both groups, a significant increase was found in the ANOVA at the 12-month time point compared with the 0-month time point, but not at the 24-month time point compared with the 12-month time point. Regarding the preoperative and 24-month results, a statistically significant difference was found in both groups in the ANOVA (Appendix 4) and the paired t test (Table 3).
Functional Outcome
Before operation, there were no significant differences between the 2 groups regarding the IKDC subjective score, Lysholm score, Kujala score, and Tegner score. Significant differences were found between the 4 scores of the 2 groups 24 months after operation. Regarding the preoperative and final rating outcome of the 4 scores, statistically significant improvements were found in both groups (Table 4).
Functional Scores a

MRP, medial retinaculum plication; VMP, vastus medialis plasty; IKDC, International Knee Documentation Committee.
Comparative results between preoperative and final follow-up data.
Recurrence Rate
The recurrence of patellar dislocation or instability was documented at the 2-year follow-up in both groups. Twenty-two of the 23 patients in the MRP group and all 23 patients in the VMP group having undergone surgery at least 3 years earlier received another review through telephone call, correspondence, or e-mail regarding their recurrence of dislocation or instability as the final follow-up. In summary, the 2- to 7-year follow-up showed that 5 patients (17.9%) experienced episodes of redislocation and 14 patients (50%) experienced only instability (the patella did not clearly dislocate and require a reduction maneuver) in the MRP group, and 2 patients (7.7%) experienced episodes of redislocation and 5 patients (19.2%) experienced only instability in the VMP group (see Appendix 5, available online). Three of the redislocated patients in the MRP group underwent reoperation 3 to 6 years after the first operation, with 2 having MPFL reconstruction and 1 having simultaneous MPFL reconstruction and tibial tubercle medialization. The 2-year and 2- to 7-year follow-up results show no statistically significant differences between the patient numbers of redislocations but show statistically significant differences between the total patient numbers regarding dislocation and instability.
Discussion
Studies on physis-sparing procedures in dedicated cohorts of patients with open growth plates are few in the current published data. One study of a large cohort of children is about the treatment of primary dislocation. 21 The report by Deie et al 8 is the only one found about recurrent dislocation of the patella in children, but in too small a cohort (6 knees in 4 patients).
We chose pubescent patients in this study mainly because the patella and femoral condyles of the patients in this growing stage were almost fully ossified, making evaluation and measurement of these structures more accurate. On the contrary, although we also use these 2 methods for prepubescent patients, it is very difficult to make measurements because the patella and femoral condyles are not fully ossified. In adult patients, we depend mainly on MPFL reconstruction instead of MRP or VMP to treat recurrent patellar instability or dislocation. Therefore, we chose patients of this special age stage for this study.
In previous reports, the data were always gathered at 1 final follow-up, a 1-time evaluation. However, patellar dislocation may be a developing condition either before or after surgery, so the 1-time final follow-up may not reveal the real face of this condition, and we suppose that multiple sequential evaluations may reflect its hidden characteristics. With regard to the correction of the lateral tilt and deviation of the patella, the change of the static position of the patella may reflect the condition in a better way. Therefore, we wanted to know if the correction of the position of the patella can be maintained after operation, and through this method we wanted to evaluate the effectiveness of the surgical procedures. To our knowledge, no multiple sequential evaluations of the surgical results, especially regarding the corrected patellar position, can be found in previous reports.
There were several physis-sparing procedures reported to treat recurrent patellar instability or dislocation. The Roux-Goldthwait procedure realigns the distal extensor mechanism by transferring the lateral part of the patellar tendon at the tibial insertion to the medial side. 23 This procedure does not increase the medial restraint of the patella and attenuates the patellar tendon. In the semitendinosus tenodesis procedure, the proximal end of the semitendinosus tendon is released and its distal insertion is left intact. The tendon is tethered to the patella and its free end is sutured back to itself. This procedure is really an augmentation of the medial patella–tibial ligament instead of the MPFL.5,12 The adductor magnus transfer procedures release the proximal end of the adductor magnus tendon, leave the distal attachment intact, and transfer the free end into the patella. The path of this new structure is like the MPFL.4,8 However, because this structure is inserted proximal to the anatomic femoral insertion of the MPFL, it may cause flexion restriction when it is too tight or unsatisfactory patellar restraint when it is too loose.
Arthroscopic proximal realignment is also physis-sparing. Regarding proximal realignment of the patella in chronic cases, some authors reported enlarging the medial retinaculum defect, or incising or releasing the lax and redundant medial capsule in a longitudinal way at first and then reopposing the separated retinaculum through plication or imbrications.2,13,27 Some authors reported just plicating the lax retinaculum without predivision.3,14 Halbrecht 11 reported plicating the lax medial retinaculum with preshaving or thermal shrinkage of the soft tissue to increase healing response.
Lateral quadrant translation and end-point examination in this study showed increasing number of patients regaining soft end-point and abnormal lateral translation grades in both groups a long time after operation. Apprehension testing also showed increasing numbers of patients regaining a positive apprehension test. These phenomena may indicate that these 2 methods are not reliable enough to create a long-lasting medial restraint for the patella. No statistically significant differences found between the 2 groups regarding the apprehension and lateral quadrant translation tests may be attributable to the inaccuracy of these kinds of clinical tests.
Axial view radiographic examination is a traditional way to evaluate the lateral translation or tilt of the patella. The Merchant view 20 is taken in 45° of knee flexion and the Laurin view 18 is taken in 20° of knee flexion. In the axial view, the most prominent point of the femoral condyles, the shallowest point of the trochlear groove, and the widest point of the patella are outlined simultaneously, although they may not be on the same level along the femoral axis. However, although the trochlear groove can be clearly outlined, the patellar facet cannot be clearly outlined because of the overlapping of the facet shadow. Also, the patellar tilt cannot be evaluated because the posterior aspect of the femoral condyles cannot be revealed in the axial view. In CT examination, the femoral trochlea and the patellar facet can both be clearly outlined, to make measurement easier and more accurate. However, because the most prominent point of the femoral condyles, the shallowest point of the trochlear groove, and the widest point of the patella are usually not on the same level along the femoral axis, we cannot use 1 cut to match the axial radiographic view. Measurements were made by overlapping different cuts or using special software. From another point, CT images taken in full extension are different from the axial view radiograph in 20° or 45° of flexion. It is only when they are taken at the same flexion degree that measurement results on the CT images and the axial view radiograph can be compared, especially regarding the sulcus angle.
Although static position of the patella can be evaluated on an axial view radiograph or CT image, it does not represent the stability status of the patella. A laterally deviated patella with a low lateral translation grade and firm end point may be more stable than a neutralized patella with high lateral translation grade and soft end point. Thus, to evaluate the functional status of the patella regarding its stability, both the static position of the patella and its dynamic status, the extent of possible lateral translation should be taken into consideration. Clinical examination is one way to evaluate the potential lateral translation. In this study, the apprehension test, lateral quadrant translation and end point were checked, although clinical examinations regarding the grade and end point of lateral patellar translation are rough and examiner-dependent. Quantitative measurement of the lateral motion limit of the patella with or without stress radiography may be more accurate,26,28 but the device and the method used in this kind of measurement still need to be validated.
Measurements on CT images showed correction of patellar malposition by the increase of the congruence angle and the decrease of lateral patellar translation, and showed correction of patellar malrotation by the increase of the lateral patellar angle and decrease of the patellar tilt angle. However, deterioration of the correction was found in both groups. Deterioration of the corrected position of the patella may primarily be caused by insufficient restraint of the patella by the operated medial soft tissue structure. It may also be attributable to predisposing factors such as the abnormal quadriceps angle after patellar position correction and the abnormal TT-TG distance in this group, as well as other factors such as femoral sulcus and lateral femoral condyle dysplasia, although patients with severe sulcus dysplasia were excluded from this study.
From another aspect, the results of MRP depend on the extent of contracture of the plicated medial retinaculum. Through contracture, the plicated medial retinaculum can form a stiff soft tissue structure to retain the patella in the corrected position. However, if there is not enough contracture, the patella may return to a malposition because of the laterally deviated pulling of the quadriceps. Moreover, because most patients in this study had hyperlaxity, plication may be less likely to result in medial retinaculum contracture. As for the VMP group, although overlapping of the medial muscle–capsule structure across the patella may increase medial restraint of the patella, there is still a lack of direct restraint because the ruptured MPFL was not reconstructed. There were no statistically significant differences between the preoperative and final follow-up results in the paired t test regarding the congruence angle, lateral patellar angle, and patellar tilt angle in the MRP group, which implies that MRP is not a reliable technique regarding the maintenance of the correction of the patellar position and rotation.
In the MRP group, although no statistically significant improvement of the patellar position and rotation were found in the CT evaluation, statistically significant functional improvement was found regarding the IKDC, Kujala, Lysholm, and Tegner scores. Functional improvement may be attributable to other factors that may alleviate the symptoms, such as deinnervation of the patella through lateral release.
The statistically significant higher recurrence rate of instability or dislocation in the MRP group indicate that this less invasive technique is unreliable to treat recurrent patellar dislocation in adolescents compared with open VMP. Vastus medialis plasty seems to drastically alter the forces applied to the patella, and the altered forces may adversely influence the patellofemoral pressure distribution and cause future cartilage degeneration. However, we found that the medial soft tissue structure was still often not strong enough to control the corrected position of the patella during operation as well as in follow-up. We did not find evidence of adverse patellofemoral pressure.
Regarding MRP, the recurrence rate in this study was relatively high compared with previous reports, at 17.9% (5 of 28 patients). In a 2-year follow-up, Halbrecht 11 found no redislocation in 26 patients (29 knees) who underwent arthroscopic all-inside medial reefing and lateral release for patellar instability. In a 12- to 26-month follow-up, Haspl et al 13 found no recurrence of subluxation or luxation in 17 patients who underwent plication of the medial patellar retinaculum and release of the lateral patellar retinaculum for patellar instability, acute patellar luxation, or recurrent patellar luxation. In a 1- to 7-year follow-up, Yamamoto 29 found only 1 redislocation in 30 cases that underwent arthroscopic repair of the medial retinaculum and capsule for acute patellar dislocations. Regarding the VMP, the recurrence rate in this study was also relatively high compared with previous reports, at 7.7% (2 of 26 patients). Scuderi et al 25 followed 21 patients (26 knees) who underwent VMP for patellar dislocation for 2 to 9 years and found that only 1 patient (3.8%) experienced redislocation.
The high recurrence rate found in this study may be attributable to patient selection. The recurrence of patellar dislocation is related to the postoperative activity level and may be more likely to happen if the patients more often take part in high-level activities. In other words, one way to prevent redislocation is to restrict activity. In this study, the patients included had high preinjury sports activity levels, were eager to return to sports activities, and were unwilling to postpone their surgery to adult age. Furthermore, the patients had no symptoms on the other leg. Thus, after operation they were allowed and encouraged to take part in high-level sports as early as possible. This rehabilitation protocol may reveal the unsatisfying aspect of the procedures and result in comparatively higher recurrence rates.
These 2 procedures are mainly used in adolescents; we found in our clinical practice that adult MPFL reconstruction results in better patellar stability than either of these 2 procedures. Accordingly, patients near skeletal maturity were advised to have an adult procedure.
This was neither a single- nor a double-blinded study, which might result in bias. The clinical examination, especially the lateral translation grade and end-point examination, were examiner-dependent and may be inaccurate, so the results might not be so reliable regarding the differences between the 2 groups. Bias may have also existed in the measurement of the CT images. The number of the patients was limited. One additional weakness of this study is that we did not evaluate the possible remaining growth of the patients.
Conclusion
Medial retinaculum plication is a less reliable technique for recurrent patellar dislocation compared with VMP with regard to the maintenance of the corrected position of the patella, functional recovery, and prevention of recurrence.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.