
Abstract
Keywords
Meniscal tears requiring treatment are a common occurrence in sports traumatology. Past studies have established that the menisci play an important role in load distribution, joint lubrication, joint stability, and proprioception.1,2,21,24,25,31,32 Radial meniscal tears are common in young patients and are often combined with acute anterior cruciate ligament (ACL) ruptures. 7 Historically, radial tears extending to the rim have been believed to result in a reduction of meniscal hoop strength functionally equivalent to a total meniscectomy. 26 Partial meniscectomy to remove the damaged, unstable portion of the meniscus has been the gold standard of surgical treatment for radial meniscal tears.10,14 However, since multiple long-term clinical studies have identified a high risk of progression of knee osteoarthritis after meniscectomy,11,22 the importance of preserving meniscal tissue in the knee is now well established, and treatment of meniscal tears is directed toward preserving as much meniscal tissue as possible to prevent future degenerative disease.13,17,18,33,34,36,37 Several case series have been published describing different repair techniques. Van Trommel et al 35 repaired 5 radial tears of the lateral meniscus using outside-in sutures enhanced by fibrin clot. Noyes and Barber-Westin 28 repaired 4 cases of radial tear repairs using inside-out sutures. Choi et al 9 performed all-inside meniscal repairs in 14 cases of radial tears using a single horizontal absorbable suture. Most repair techniques discussed in previous studies utilized single-loop or double-loop sutures oriented parallel to the fiber direction of the meniscus tissue. However, Bedi et al 6 reported that inside-out double horizontal suture repair of a radial tear involving 90% of the width did not restore the location of the pressure peak to that of the intact knee.
Past studies thus raise concerns as to whether a single or double horizontal suture can provide primary stability. We hypothesized that our novel cross-suture technique would yield greater primary stability than the double horizontal suture technique. The objective of our study was to evaluate the biomechanical properties of our suturing method in repairing complete radial tears, comparing the cross-suture technique with the double horizontal suture technique under cyclic loading conditions.
Materials and Methods
We tested 40 fresh human lateral menisci from patients who underwent total knee arthroplasty (TKA) because of varus knee osteoarthritis. The TKA procedure included excising the meniscus in its entirety as close as possible to the capsular tissue. All the menisci in our study were from the lateral compartment and had no macroscopic signs of meniscal tear or degeneration, such as fibrillation or fragmentation.
The cross-suture group (group A) contained 20 menisci from 20 patients (17 women, 3 men) with a mean age of 75.9 years (range, 68-84 years). The double horizontal suture group (group B) contained 20 menisci from 20 patients (17 women, 3 men) with a mean age of 75.7 years (range, 70-84 years). The study was approved by the ethics committee of the university. All patients were informed of the purpose of the study and gave their written consent. After being harvested during the surgical procedure, the menisci were kept in saline solution and tested within 24 hours. We practiced each of the suture techniques in 5 menisci before starting the study to ensure consistency in the suture techniques. For all 40 menisci, we used a No. 15 scalpel to create a complete radial tear from the meniscal center to the rim in the middle third of the meniscus, in the process completely transecting the meniscus at the junction of the body and the posterior horn of the meniscus.
Suture Techniques
All menisci were repaired with the same suture material (2-0 Prolene, Ethicon Inc, Johnson & Johnson, Somerville, New Jersey), which consists of 2 straight suture needles at both ends of the thread. In each group, we oriented the 4 points of the suture as follows: 2 points 5 mm from the meniscal rim and 5 mm from the tear, and the other 2 points 10 mm from the meniscal rim and 5 mm from the tear (Figure 1).
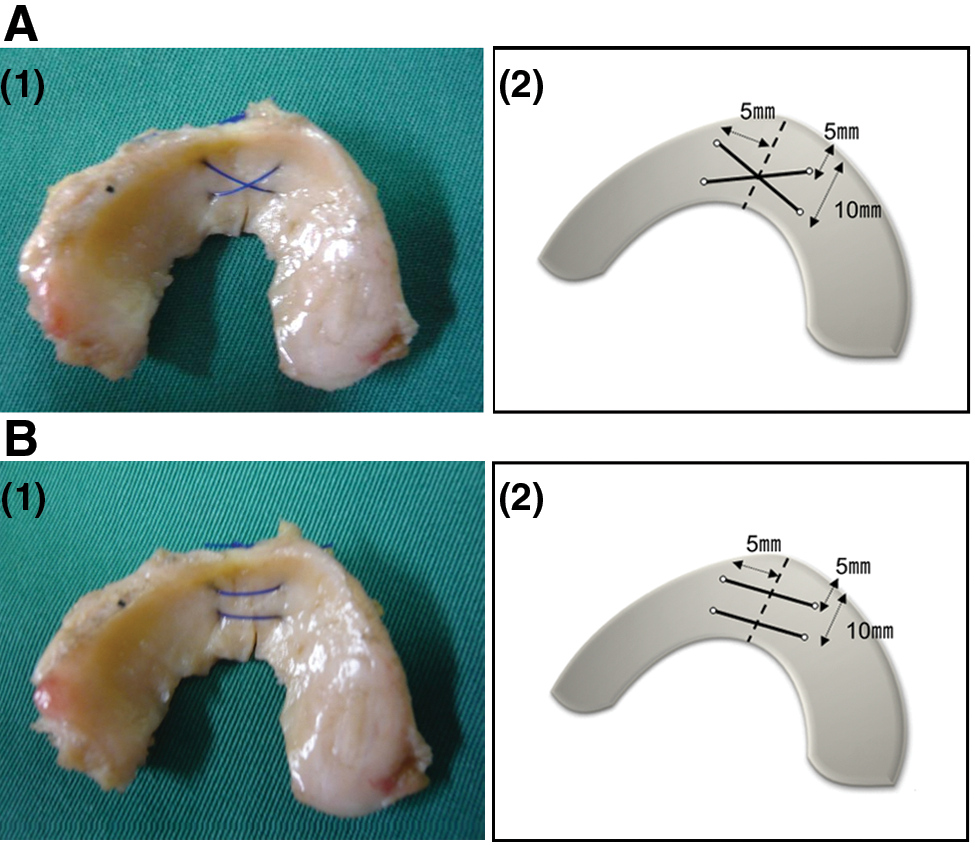
Group A: (1) Cross-suture technique. (2) Suturing cross over the 4 points: 2 points 5 mm from the meniscal rim and 5 mm from the tear, and the other 2 points 10 mm from the meniscal rim and 5 mm from the tear. Group B: (1) Double horizontal suture technique. (2) Suturing parallel to the 4 points: 2 points 5 mm from the meniscal rim and 5 mm from the tear, and the other 2 points 10 mm from the meniscal rim and 5 mm from the tear.
In the cross-suture group (group A), we repaired the meniscal tear by suturing 2 stitches that crossed over each other at the tear (Figure 1). We repaired the menisci in group B by the standard double horizontal suture technique with parallel sutures 5 mm and 10 mm from the meniscal rim (Figure 1). All sutures in both groups were secured by 3 knots at the lateral edge of the menisci.
Cyclic Load Testing
We loaded the specimens onto a universal testing machine and clamped the peripheral sections of the repaired meniscus with custom-made tissue clamps (Figure 2). Furthermore, we stitched baseball sutures through both ends of the meniscus using 4-0 Ethibond (Ethicon Inc, Johnson & Johnson) and securely fastened them to the clamps to prevent slippage. We performed a pilot study in 5 menisci of each suture technique to ensure that no rotation or slippage occurred between the meniscus-clamp interfaces during the procedure.
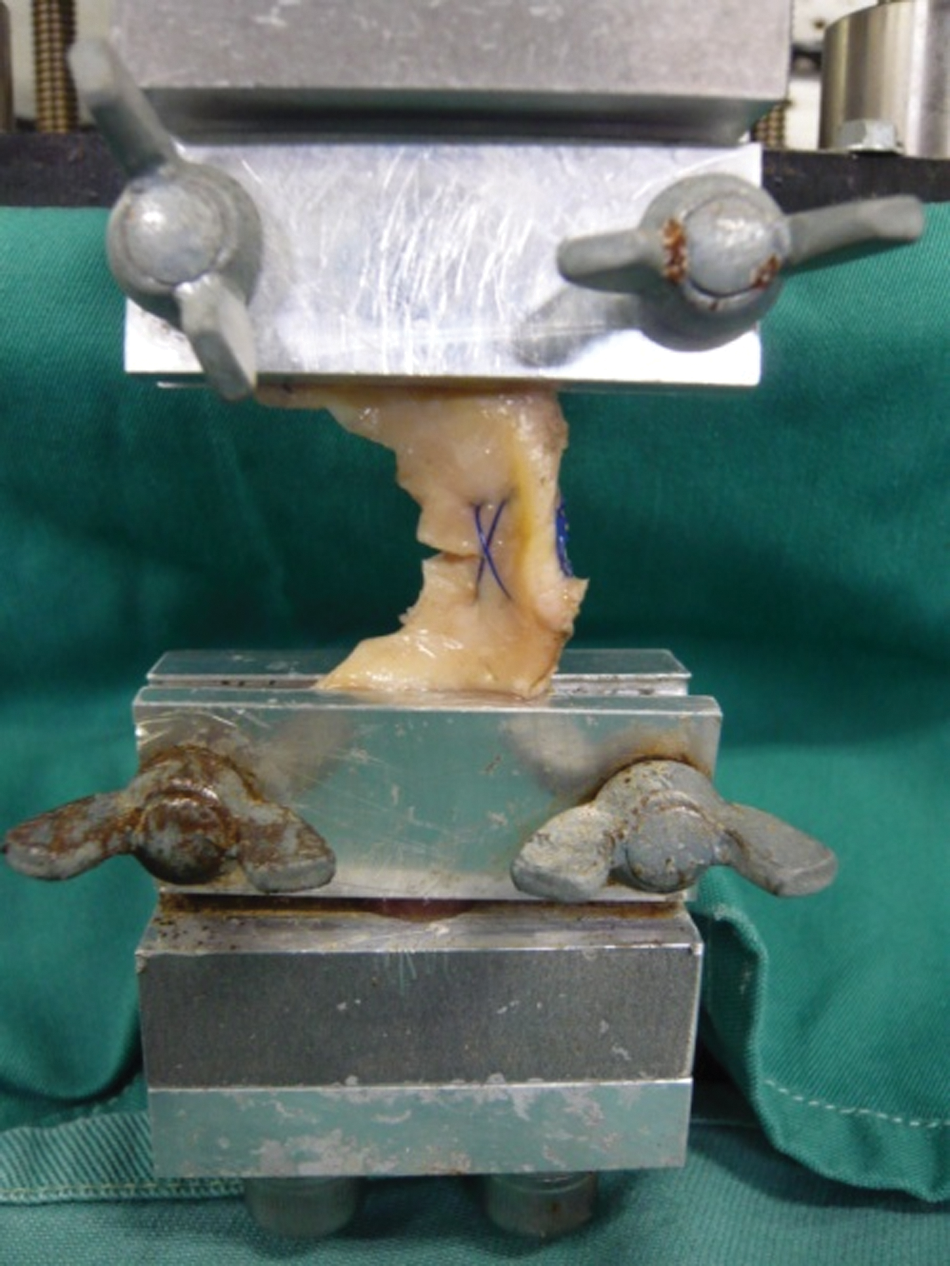
Two custom-made tissue clamps hold the specimen in place during cyclic load testing.
Testing was performed at room temperature, and samples were kept moist using normal saline to prevent desiccation. The specimens were cyclically preconditioned between 5 and 30 N at 1 Hz for 500 cycles at a displacement rate of 5 mm/min in accordance with the testing conditions that other researchers have described in previous studies.4,8,20
Load-to-Failure Testing
All repaired menisci in each group survived the 500–cycle loading protocol. Load-to-failure testing was immediately performed after the cyclic load testing. Load and elongation were continuously recorded with a computer. Displacement was defined as the distance between the 2 meniscus clamps and was measured after 500 cycles and after load-to-failure testing. Stiffness was calculated from the linear region of the load displacement curve during load-to-failure testing. Mode of failure was determined by visual inspection.
Statistical Analysis
We used the Student t test for statistical analysis of the results, setting the level of significance at P < .05.
Results
Ultimate Failure Load
The cross-suture technique specimens had a significantly higher failure load than did the double horizontal suture technique specimens (P < .05) (Table 1).
Ultimate Failure Load, Stiffness, and Displacement of Meniscal Repair Devices After 500 Cyclic Loading Between 5 and 30 N
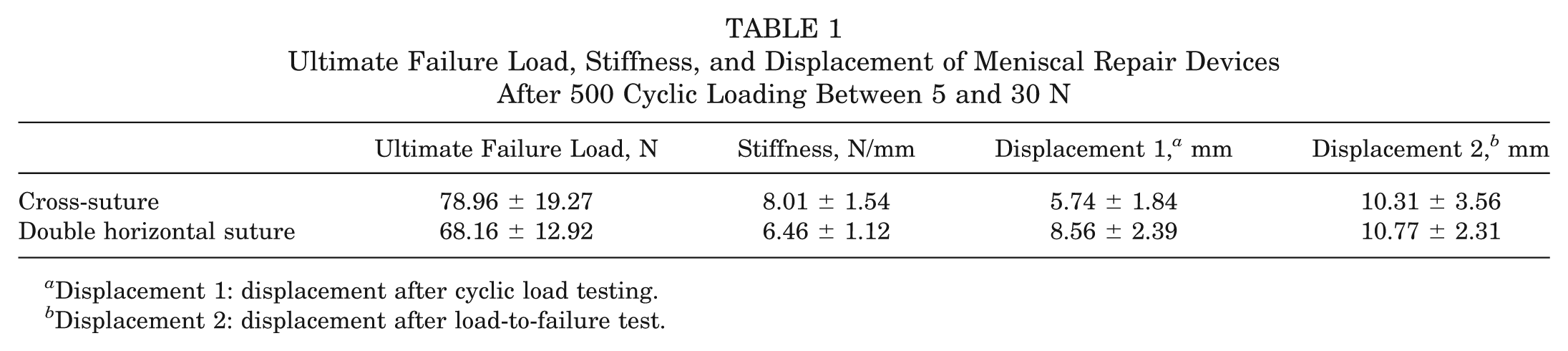
Displacement 1: displacement after cyclic load testing.
Displacement 2: displacement after load-to-failure test.
Stiffness
The cross-suture technique specimens had significantly greater stiffness compared with the double horizontal suture technique specimens (P < .05) (Table 1).
Displacement
Immediately after starting the cyclic loading, a gap between the meniscal margins could be seen. At the end of the 500–cycle loading protocol, group A had a significantly lower displacement than group B (P < .05). No significant difference in displacement between group A and group B was observed after load-to-failure testing (P > .05) (Table 1).
Failure Mode
In each group, most of the specimens failed by tissue failure, with only a few specimens failing by a suture rupture. In group A, 17 of the specimens failed by tissue failure, and 3 failed at the knot. In group B, 18 of the specimens failed by tissue failure, and 2 failed at the knot.
Discussion
Radial tears of the menisci are relatively common. Magee et al 23 reported a 14% incidence of radial tears among 200 patients who underwent arthroscopy. Among these cases, the most frequent location was the midbody of the lateral meniscus.
Preserving meniscal anatomic structures whenever possible is important. Collagen fibrils in the main portion of the meniscus are oriented in a circular direction that transforms joint stress on the meniscus into circular stress. 30 Because radial tears extending to the meniscal rim that completely transect the collagen fibrils lead to loss of hoop strain, the goal for repairing complete radial tears is to restore the hoop strain.
Although multiple case reports regarding the repair of radial meniscal tears have been published,9,12,16,27,28,35 few biomechanical studies have been performed on radial tear repairs. Herbort et al 16 conducted a biomechanical study analyzing the outcomes of complete radial meniscal tears that were repaired at different distances from the meniscal rim and tear edges with different numbers of sutures. Their analysis found that double horizontal suture techniques closer to the meniscal rim had stronger structural properties than single suture techniques on tears more distant from the meniscal rim.
However, uncertainty persists as to whether employing double horizontal suture techniques to repair complete radial tears can actually provide sufficient fixation strength to withstand physiological cyclic loading in vivo. Bedi et al 6 performed a cadaveric study and reported that partial meniscectomy led to further increase in contact pressure transmitted to the medial tibial plateau under physiological loads. Furthermore, double horizontal suture repair of a 90% tear did not restore the location of the pressure peak compared with the intact knee. Their measurements of the magnitude and location of peak contact pressure did not show any differences between a radial tear and the double horizontal suture repair. These findings suggest that menisci repaired by the double horizontal suture technique cannot play a role in load distribution because of gap formation under physiological loads. Therefore, we hypothesized that the cross-suture could achieve superior primary stability compared with the double horizontal suture.
The primary stability of meniscal repair for a complete radial tear is a key factor in determining success of the repair. To reduce the risk of suture rupture or tissue failure, we focused on the orientation of the sutures relative to the meniscal tear and particularly the relationship between the orientation of the sutures and the orientation of the collagen fibers. For example, several studies that have examined repair techniques for longitudinal meniscal tears have determined that the vertical suture technique provides superior ultimate strength over the horizontal suture technique, findings that have contributed to establishing vertical suturing as the gold standard for longitudinal meniscal fixation.3,5,15,19
Similarly, it is suggested that the superiority of the cross-suture technique in the ultimate failure load and stiffness derives from the ability to capture a greater proportion of the semicircular-oriented meniscal collagen fibers because the direction of the sutures is oblique to the meniscal collagen fibers rather than parallel to the fibers, as is the case with the double horizontal technique.
Displacement after 500 cyclic loading was significantly smaller in the cross-suture technique than that in the double horizontal suture technique. These results suggest that cross-suturing reduces the likelihood of a subsequent “cheese-cut” tissue failure.
Cyclic loading protocols are thought to more closely imitate the usual loads to which the repaired menisci are subjected in vivo. In our study, we used a protocol similar to what previous researchers have used in their meniscus studies: 500 cycles between 5 and 50 N. Biomechanical testing was performed using a slow loading rate to simulate the stresses to which the meniscus might be subjected during early postoperative rehabilitation exercises and activities of daily living such as slow-speed walking, stair climbing or descending, and squatting. The loading range was selected to simulate known medial meniscal loads during the application of forces equivalent to a clinical examination under both ACL-intact and ACL-deficient conditions. 29 However, pretest experiments in our laboratory found that setting the upper limit at 50 N led to very high rates of failure, making meaningful comparisons of study groups difficult. We therefore confined our testing of the study specimens to 500 cycles between 5 and 30 N.
Our study was limited by our decision to use human lateral menisci, taken from patients who received TKA. As a result, these human lateral menisci differed to some degree from each other with respect to degenerative changes, shape, thickness, and stiffness despite our efforts to select cases in which the cartilage and meniscus were well preserved in the lateral compartment. Before our human study, we tested porcine menisci, but their smaller size and greater thickness compared with human menisci made it difficult to load porcine menisci onto our cyclic testing machine. To our knowledge, our study is the first biomechanical study examining repair techniques for radial meniscal tears using fresh human menisci. Indeed, because previous studies have often used porcine or cadaveric menisci, one of the aims of our study was to collect data on fresh human menisci.
Another limitation to our study was that we used a nonphysiological method of loading. Our setup was a “worst case scenario” test, whereby the load is applied parallel to the axis of meniscal sutures and perpendicular to the tears. The real in vivo forces might be more complex, but the real forces are still unknown. We considered the main affecting force is the tensile force in radial tears and minimized the disruptive factors, such as shearing forces. The cross-suture group still had an average displacement of 5 mm after cyclic loading, which would not be conducive to clinical healing. However, we proved that the cross-suture technique could get more superior stability than the double horizontal suture technique in vitro. After this, the clinical relevance of this biomechanical study is important. Clinical and animal studies with appropriate controls are recommended to validate our findings in vivo and to determine the biological sequelae of the cross-suture technique under clinical conditions. Nonetheless, the significant improvement in biomechanical properties that we observed in conjunction with the minor modification in the technique of reorienting the sutures from parallel to cross still should provide encouragement for surgeons to consider utilizing the cross-suture technique in their clinical practice. In fact, this technique does not require any significant modification from the horizontal double suture in the arthroscopic surgical maneuvers.
Conclusion
Our study findings indicate that cross-suturing significantly improves the structural properties of complete radial meniscal repairs and appears to improve primary stability of the repaired meniscus compared with double horizontal suture techniques. Our new method for repairing radial tears could be a promising solution in both young and active patients.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.