
Abstract
The anterior cruciate ligament (ACL) is the most commonly injured ligament requiring surgery in the United States, with 250 000 ruptures and 100 000 surgeries per annum. 24 Despite the prevalence of ACL reconstruction, there is no universally agreed upon graft choice for this procedure. The 3 most common graft types are bone–patellar tendon–bone autografts (BPTB), quadrupled hamstring tendon autografts (HS), and allografts. Several series on ACL reconstructions have reported excellent outcomes in greater than 90% of patients.8,23 Bone–patellar tendon–bone autograft has long been considered the “gold standard,” with low failure rates. However, critics of BPTB autograft cite a high rate of donor site morbidity, potential risk of patellar fracture, larger scar, and long-term anterior knee pain.2,25 When both the gracilis and semitendinosus tendons are doubled to make a quadruple stranded graft, the hamstring autografts are biomechanically stronger than BPTB. However, historically, hamstring tendon fixation was subject to graft loosening and required more expensive implants with the potential for knee flexion weakness. 22 Recent literature would also suggest hamstring autografts have the highest rates of infection. 1 Allografts avoid the problems with donor site morbidity but may be associated with a higher failure rate and revision surgeries, particularly in younger, more active patients. 28
The current unstable economic and political environment suggests the need for an increasingly cost-conscious awareness among health care consumers. The orthopaedic surgeons’ effect can therefore be profound because they perform one of the most common surgeries in the health care industry. Thus, analyzing the most cost-effective method to treat this prevalent injury is a good starting point for curbing health care costs. Cost-effectiveness analysis (CEA; see Table 1) is a well-established tool to guide these decisions.10,14 Cost-effectiveness analysis enables one to compare the benefits and costs associated with different treatment paradigms to determine which treatment choice is ultimately most effective and least costly. In this study, CEA is used to analyze the different graft choices in ACL reconstruction to determine the most cost-effective graft. It is hypothesized that BPTB ACL reconstruction will be the most cost-effective method when compared with HS and allograft.
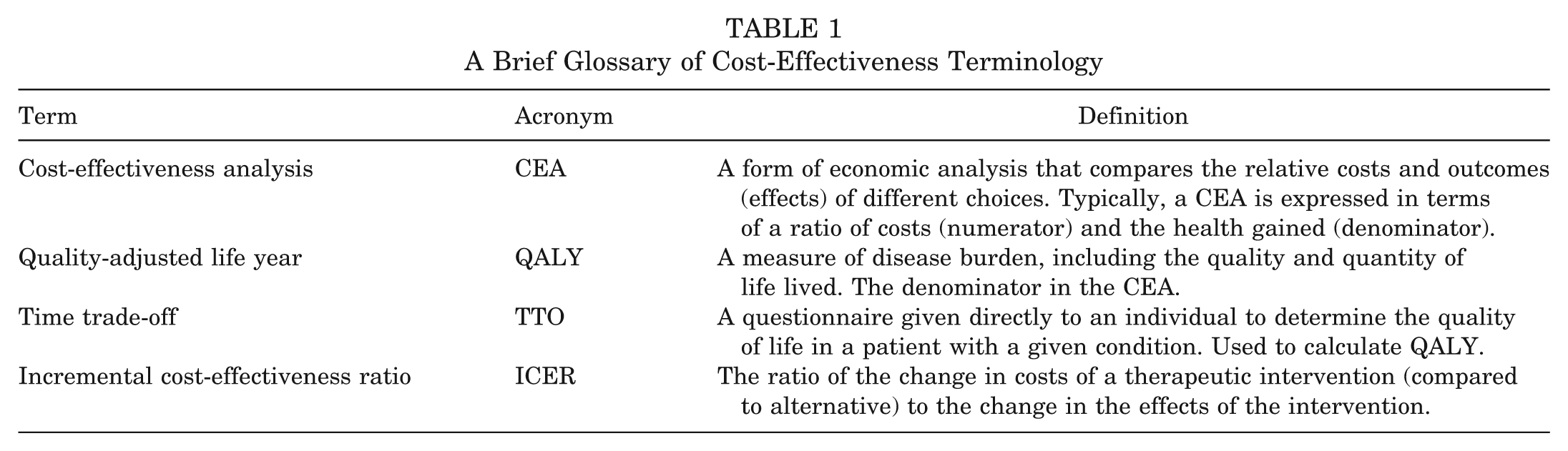
A Brief Glossary of Cost-Effectiveness Terminology
Methods
Model
Simple decision tree modeling is a well-accepted method to determine cost-effectiveness for intervention thresholds of strategies with outcomes that distribute over a defined period. 4 Therefore, a simplified decision tree model was used in this study to examine the cost-effectiveness of the 3 most common ACL reconstruction graft tissues: BPTB, HS, and allograft. The model was constructed using TreeAge software (TreeAge Pro Suite 2006; TreeAge Software, Inc, Williamstown, Massachusetts); a basic tree is available in Figure 1. 29 This model of ACL reconstruction branches into 3 strategies based on the 3 graft types. Each strategy then branches to different outcome states determined by the graft type: well, fracture, infection, looseness, knee pain, stiffness, and revision. The authors defined revision as any condition requiring a new revision of the ACL graft for any reason. Furthermore, the outcome states for individuals undergoing revision were (1) well after revision or (2) complication after revision. The authors assumed all patients underwent the same rehabilitation postoperative protocol regardless of the graft assignment.
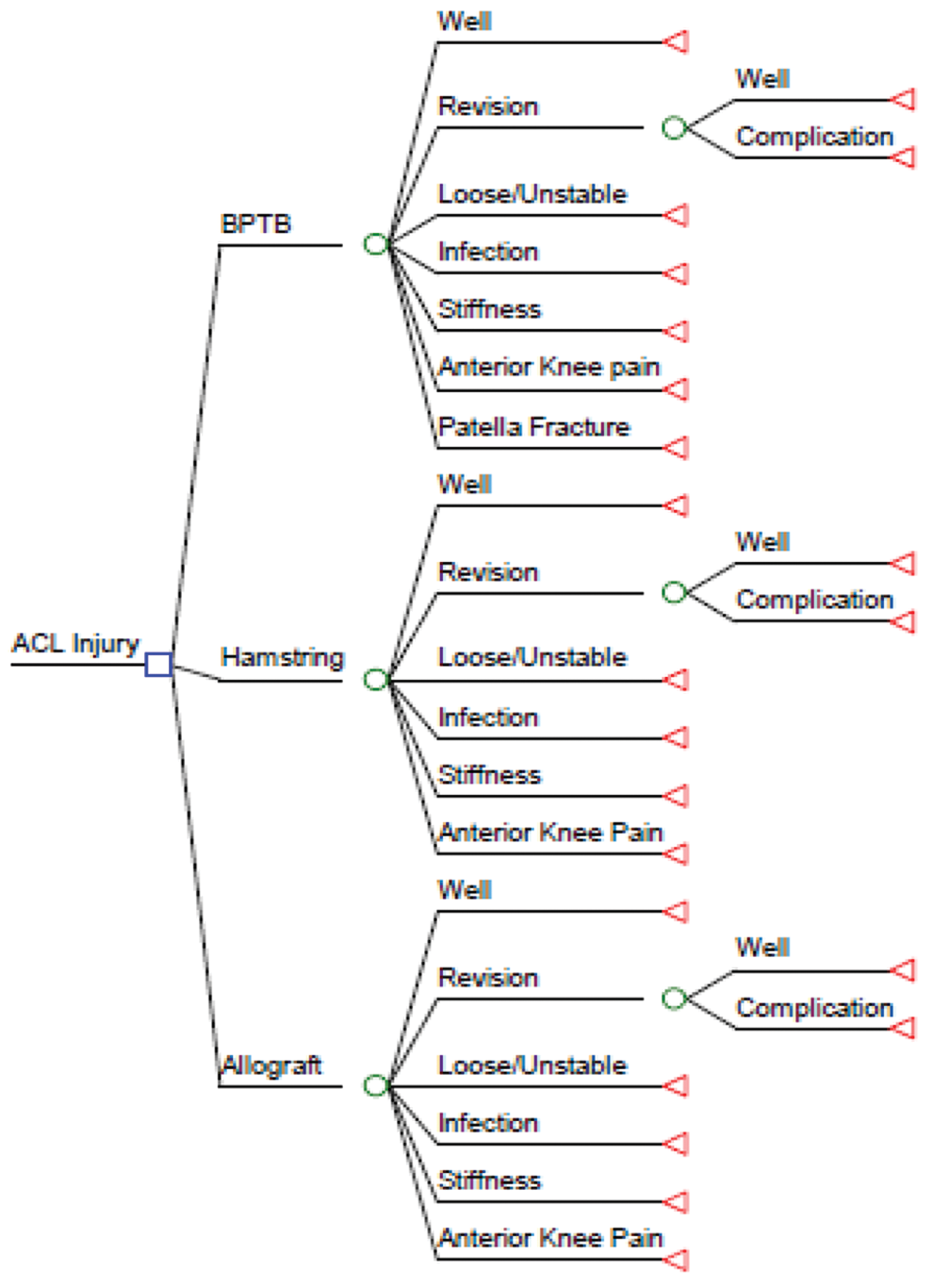
A simplified decision tree showing the 3 strategies and the associated outcome states from each strategy. The probability, utilities, and costs of each outcome state were measured using author data, estimated from the available literature or estimated using author assumptions. ACL, anterior cruciate ligament; BPTB, bone–patellar tendon–bone autograft.
To calculate the cost-effectiveness, a theoretical group of patients was put through the model. Theoretical patients were divided equally among the 3 treatment strategies and then distributed to an outcome state according to the occurrence rates found in the literature. Both societal costs and health state utility scores were calculated for each specific treatment strategy and are described in detail below.
Event Probabilities
Model probabilities were derived from the literature, as shown in Table 2. As a base model from literature review, we assumed 8.6% of allografts, 1.9% of BPTB, and 4.9% of HS required revisions.3,11 The authors assumed that failure meant that that the ACL required complete revision of the ACL graft with or without staged bone grafting. Baseline infection rates were estimated from the published literature and were 0.44%, 0.49%, and 1.4% for allografts, BPTB, and HS, respectively. 1 Loosening was defined as a positive postoperative pivot shift, and the rates of loosening were 24%, 19%, and 24%, for allografts, BPTB, and HS, respectively.2,26 Knee pain was defined as patellofemoral anterior knee pain, not pain with kneeling, and was 11%, 22%, and 13% for allografts, BPTB, and HS, respectively.2,26 Patellar fractures were assigned only to the BPTB group and were estimated at 0.2% from the literature. 18 The authors assumed that all revisions had an equivalent rate of complication regardless of the primary procedure.
Baseline Variables, Sensitivity Analysis Ranges, Sources, and Level of Evidence a
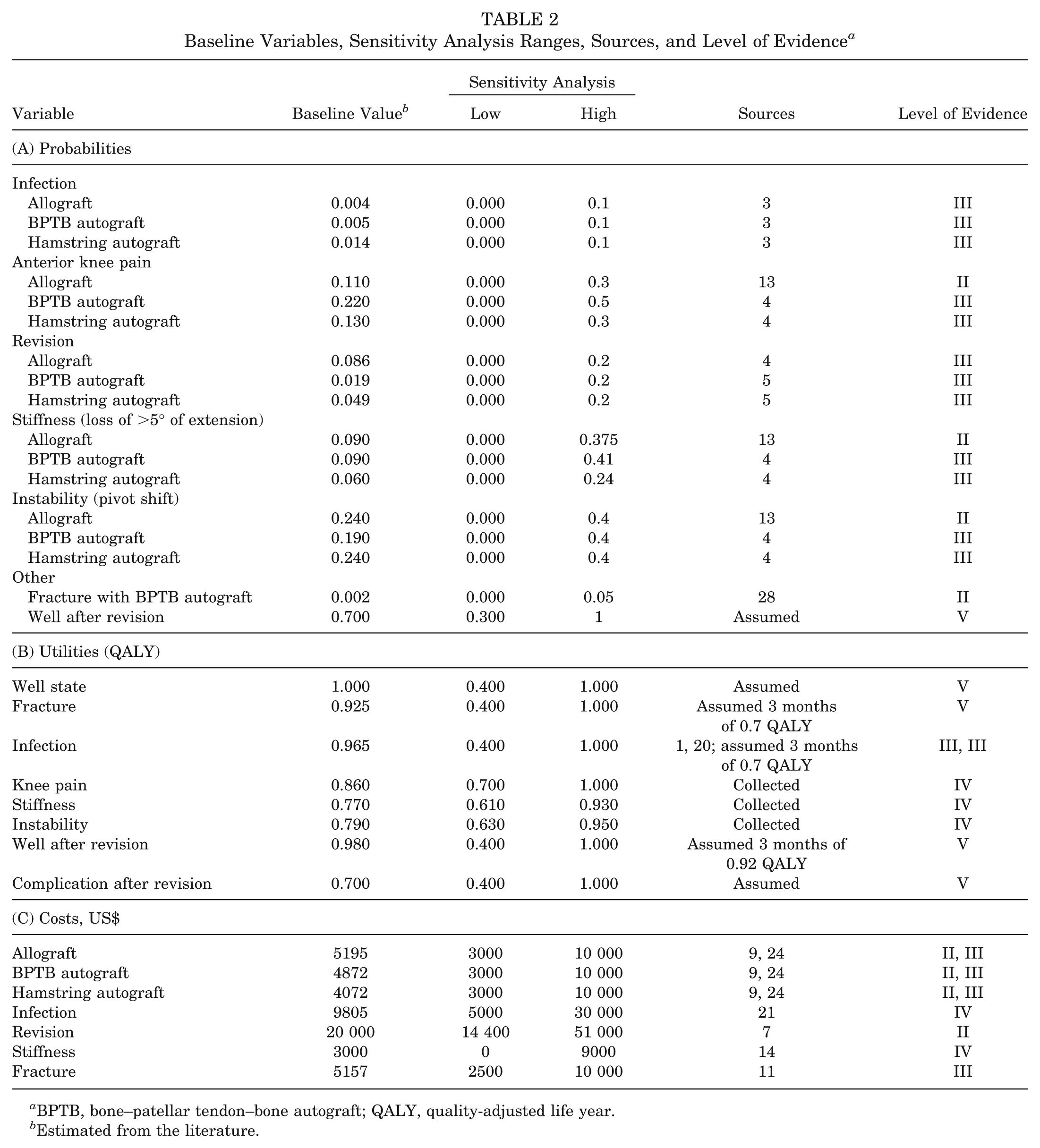
BPTB, bone–patellar tendon–bone autograft; QALY, quality-adjusted life year.
Estimated from the literature.
Costs and Discounting
Costs were estimated from multiple sources, as shown in Table 2. The authors considered only the direct operative costs and additional direct postoperative rehabilitation or indirect societal or patient costs. The cost of allograft was estimated at $5195, BPTP was $4872, and HS was estimated to be $4072.7,21 The cost of patellar fracture was estimated from National Transportation Safety Board (NTSB) research on reconstruction of particular fractures after motor vehicle collisions at $7541. 9 The cost of treatment for an infection after primary ACL reconstruction, $9805, was estimated as requiring one debridement and retention of the primary ACL graft as a large series of infected ACL graft showed retention as the most common outcome. 30 This cost included the irrigation and debridement costs of $3675 and the hospital admission and antibiotics cost of $6140. 20 Costs associated with stiffness were estimated at $3000 based on the average number of physical therapy appointments in patients with stiffness as their primary complaint (unpublished data, J. Genuario and T. Schlegel, 2010). Other costs were obtained from the available published literature. The cost of revision ACL reconstruction was estimated at $20 000 using an academic medical center’s actual cost data from the published literature. 5 Furthermore, the cost for revision was assumed to be the same irrespective of the graft chosen for the primary procedure. All values were US dollars and were not discounted since the cycle time was 1 year.
Event Utilities
The utility assignments for the outcome states were estimated using a time trade-off (TTO) method with subjects in a sports medicine clinic. Patients were given each of the outcome states and instructed to estimate how much time the participant would give up in the well state, 1.0, to avoid being assigned the poorer outcome. The utility state of well was estimated at 1 quality-adjusted life year (QALY). The end point for all the utility values was 1 year after ACL reconstruction.
Analysis
The authors assumed that a cost-effective strategy had an incremental cost-effectiveness ratio of less than $50 000. This is a ratio of the incremental cost and the incremental effectiveness over the least costly strategy. It is recognized in cost-effectiveness literature that a strategy is deemed cost-effective if it has an incremental cost-effectiveness ratio (ICER) of less than $50 000. 12
Each variable underwent sensitivity analysis testing the ICER of each strategy within a range of values. The range for most variables was wide to be sensitive to any change in the model outcome. The sensitivity ranges and the ICER ranges for each variable are available in Table 2. Two-way sensitivity analyses were also performed to vary 2 variables at once. At each analysis point, a decision was made based on a monetary benefit of $50 000/QALY. The outputs are a graph with the area under the isocurve as the collection of values, which make that strategy the preferred strategy.
Results
The base model showed that HS was both the least expensive graft with an average cost of $5373 and most effective at 0.912 QALY. The BPTB cost, on average, was $207/case more than HS with an effectiveness of 0.966 QALY. Allografts were the most costly ($1585/case additional to HS) and least effective (0.904 QALY). As such, in the baseline case, HS dominated both BPTB and allograft (less costly and more effective). The baseline analysis is available in Table 3 and Figure 2.
Baseline Cost-Effectiveness Analysis Results a
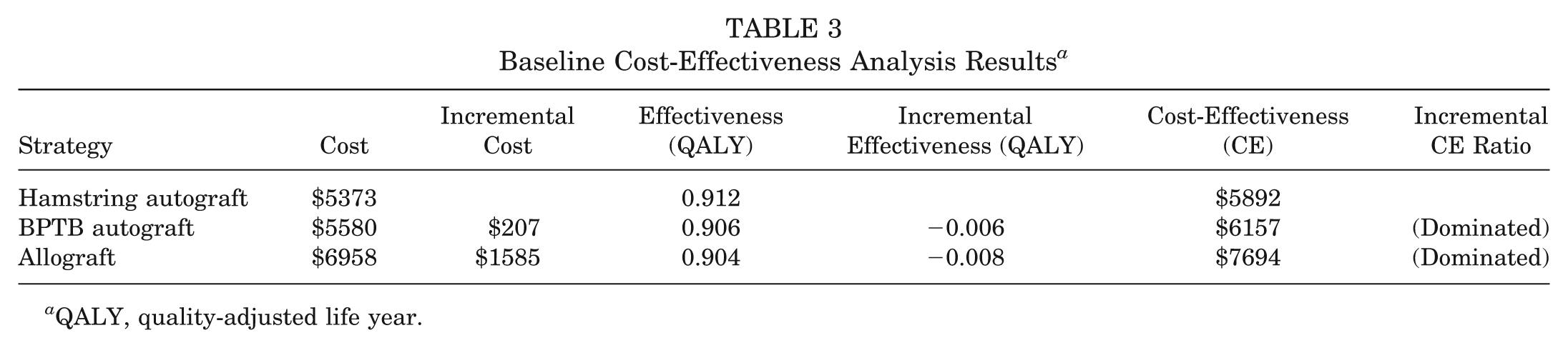
QALY, quality-adjusted life year.
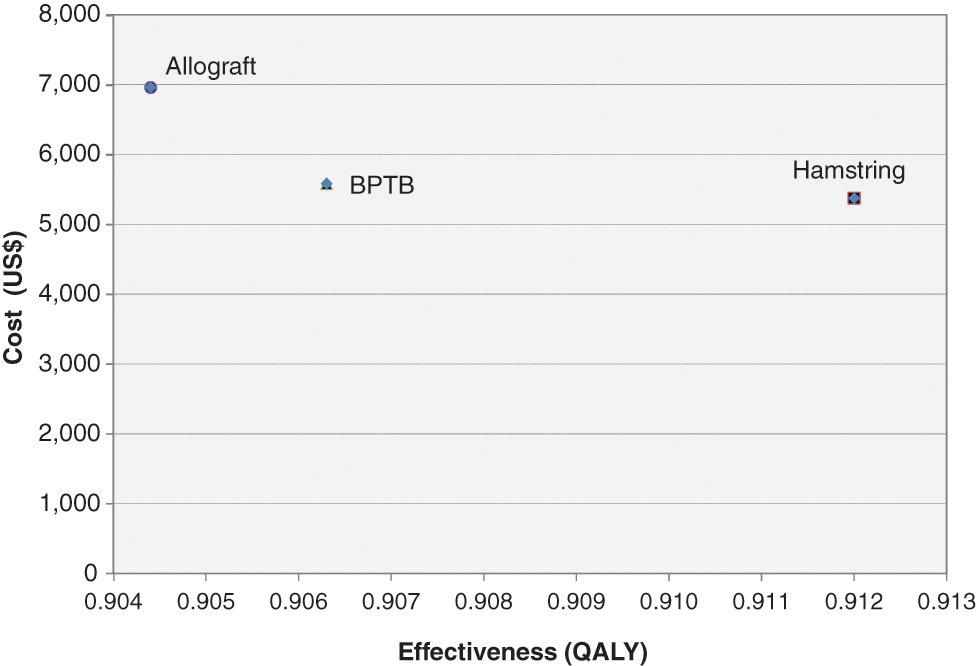
The baseline cost-effectiveness analysis. Hamstrings had the lowest cost and were most effective. Bone–patellar tendon–bone autograft (BPTB) cost slightly more and was slightly less effective. Allograft was the most expensive and the least effective. QALY, quality-adjusted life year.
All variables in the model were analyzed using a sensitivity analysis over their plausible range with significant variables reported in Table 4. When the costs of the grafts and complications were analyzed using a sensitivity analysis, the cost of each graft and the probability of complications all had influence on the cost-effectiveness of each strategy. The baseline cost of surgery for HS ACL reconstruction was assumed to be $4072. If it was increased to $4600, then BPTB became a cost-effective treatment. If the cost of BPTB could be reduced to less than $4380 (baseline $4872), then it would become cost-effective (Figure 3). Decreasing the cost of allograft to $4000 (baseline $5195) did not affect the preferred treatment strategy. A 2-way sensitivity analysis on the cost of HS and BPTB is available in Figure 4.
Significant Variables a
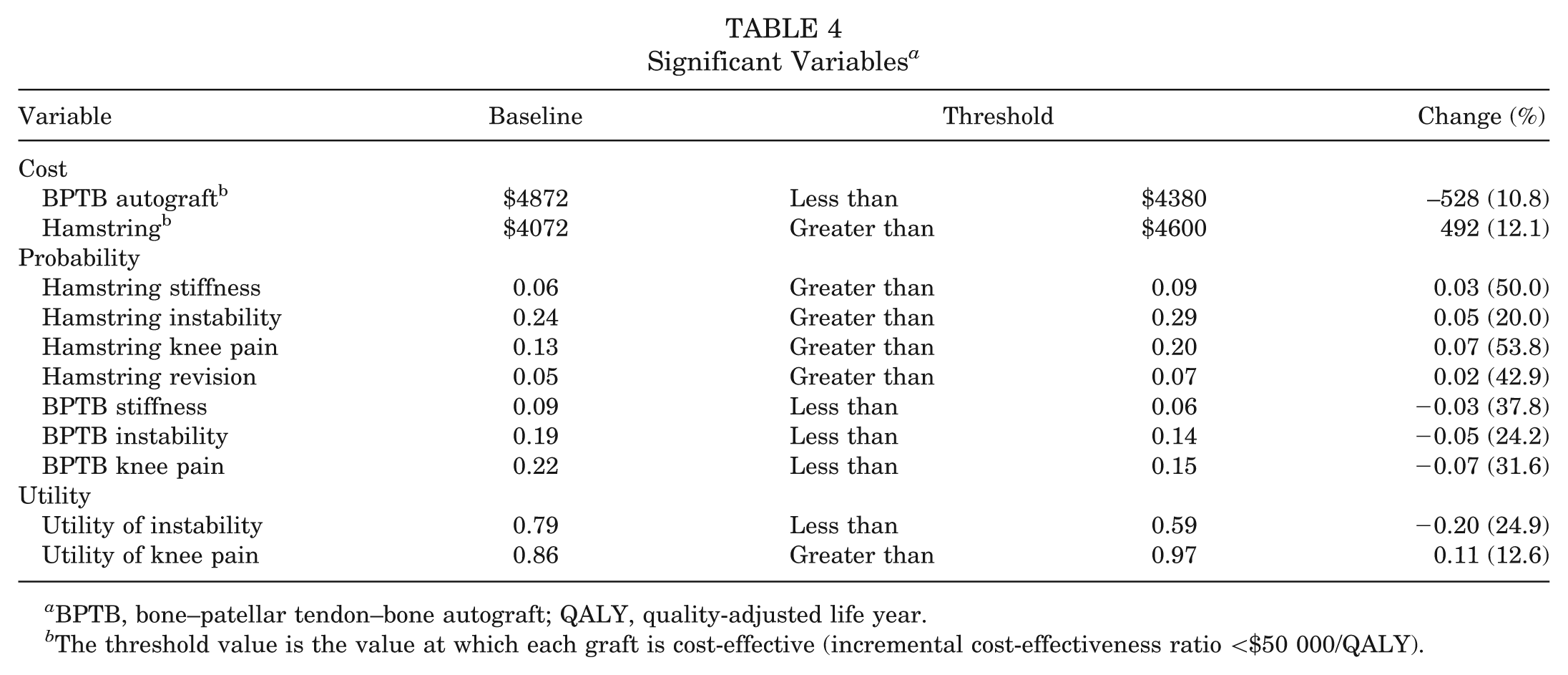
BPTB, bone–patellar tendon–bone autograft; QALY, quality-adjusted life year.
The threshold value is the value at which each graft is cost-effective (incremental cost-effectiveness ratio <$50 000/QALY).
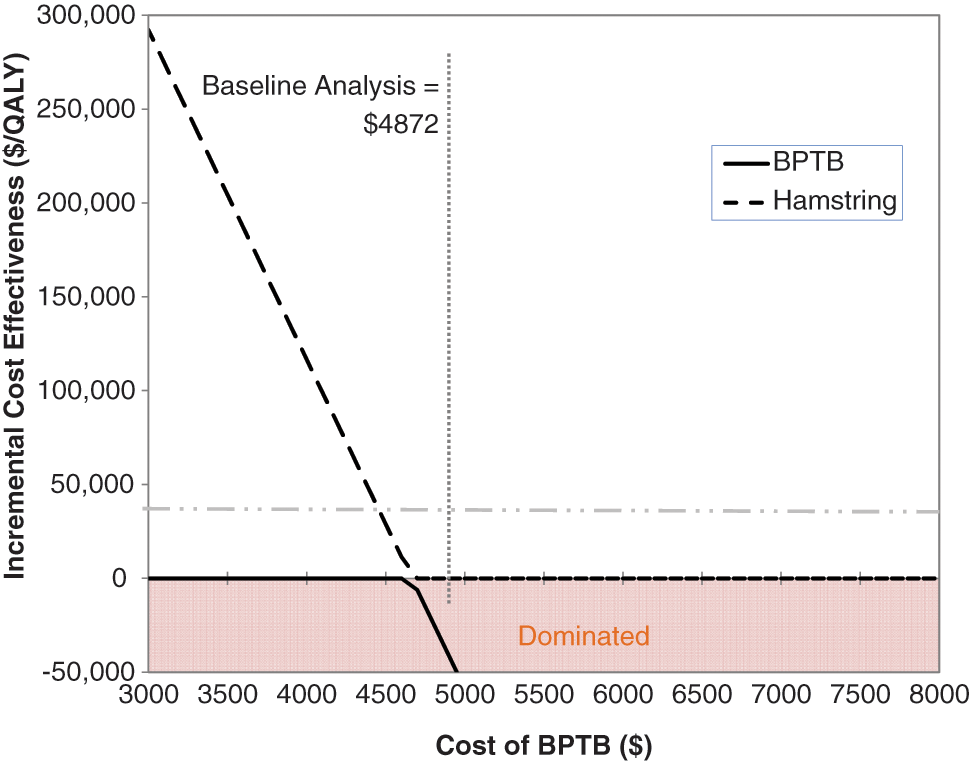
Sensitivity analysis on the cost of bone–patellar tendon–bone autograft (BPTB) autograft. The baseline cost of BPTB autograft was $4872. If the cost of BPTB was greater than $4380, then it became a dominated strategy.
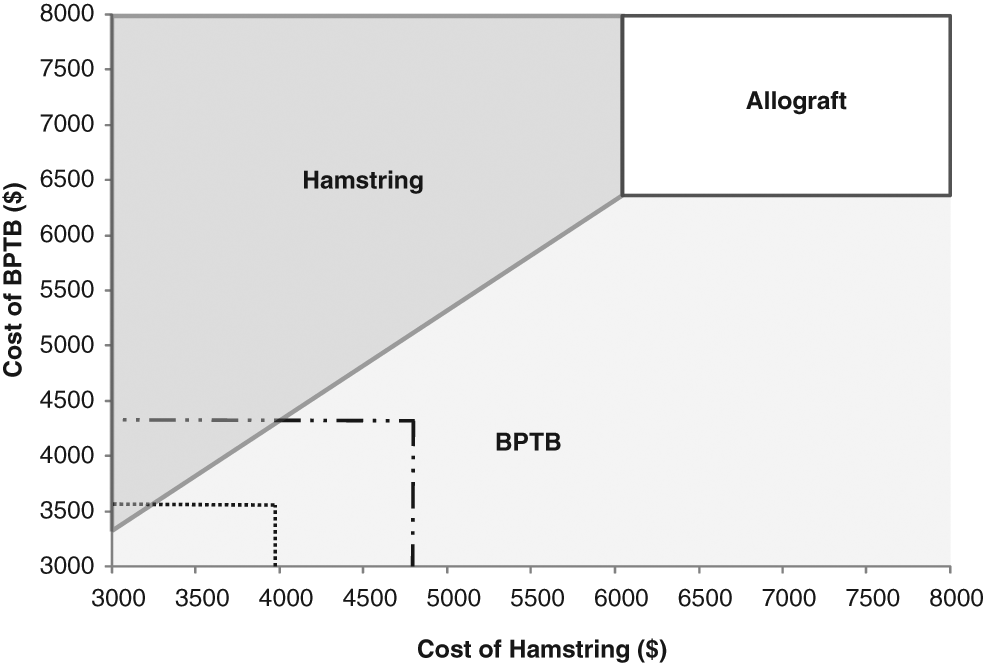
A 2-way sensitivity analysis using the cost of bone–patellar tendon–bone (BPTB) autograft and the cost of hamstring grafts. The 3 areas labeled by the graft are the sets of cost that make that variable the most cost-effective option. The small dotted lines demonstrate that if the cost of BPTB autograft is equivalent to hamstring, then it is more cost-effective then hamstring.
Varying the complication rates for all 3 graft types also affected the preferred treatment strategy. The baseline rate of instability after allograft was 24%. If this rate could be reduced to 5%, then allograft would be cost-effective. The BPTB became a cost-effective reconstructive method if the rate of anterior knee pain was reduced below 15% (baseline 22%) or if the rate of postoperative instability was less than 14% (baseline 19%). In addition, if the rate of instability after HS surgery was greater than 29% (baseline 24%) or if the revision rate became greater than 7% (baseline 4.9%), then BPTB became an incrementally cost-effective strategy. If the rate of anterior knee pain post-BPTB surgery was above 22% (baseline 13%), then BPTB became a cost-effective treatment.
A 2-way sensitivity analysis comparing the revision rates for allograft and BPTB is available in Figure 5. Using data analyzed by Kaeding et al 15 from the Multicenter Orthopaedic Outcomes Network (MOON) study, the revision rates for each graft type were plotted against each other. Their analysis created a model dependent on age and graft type. Various ages are labeled in Figure 5.
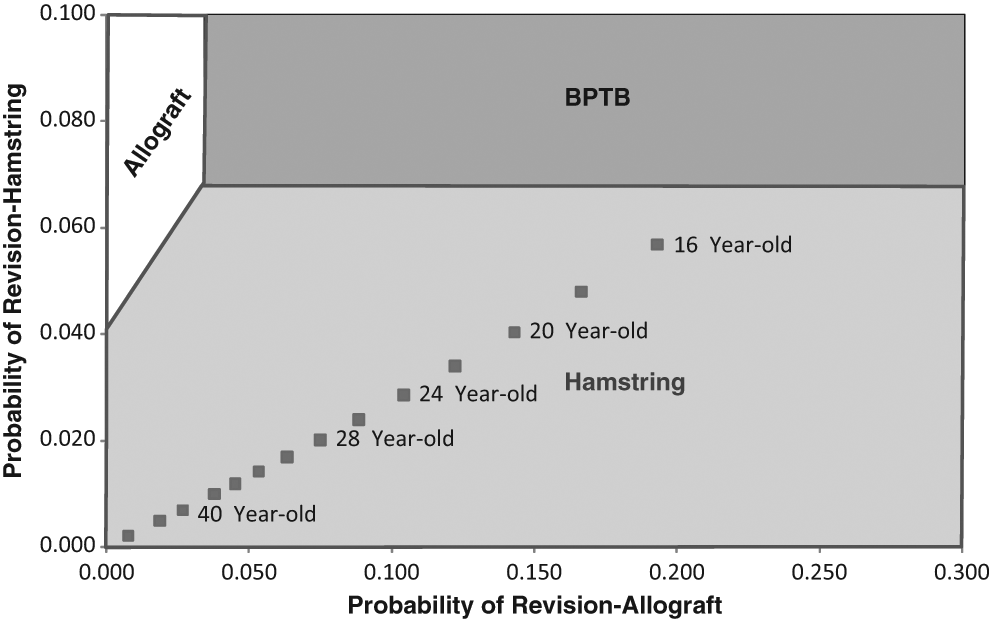
A 2-way sensitivity analysis of the probability of revision of allograft vs hamstring. Overlaid on the cost-effectiveness is the outcome data from the Multicenter Orthopaedic Outcomes Network (MOON) study on revision rates of allograft and hamstring by age. BPTB, bone–patellar tendon–bone autograft.
If the probability of anterior knee pain was above 43% for both autograft options, then allograft became a cost-effective graft choice (Figure 6).
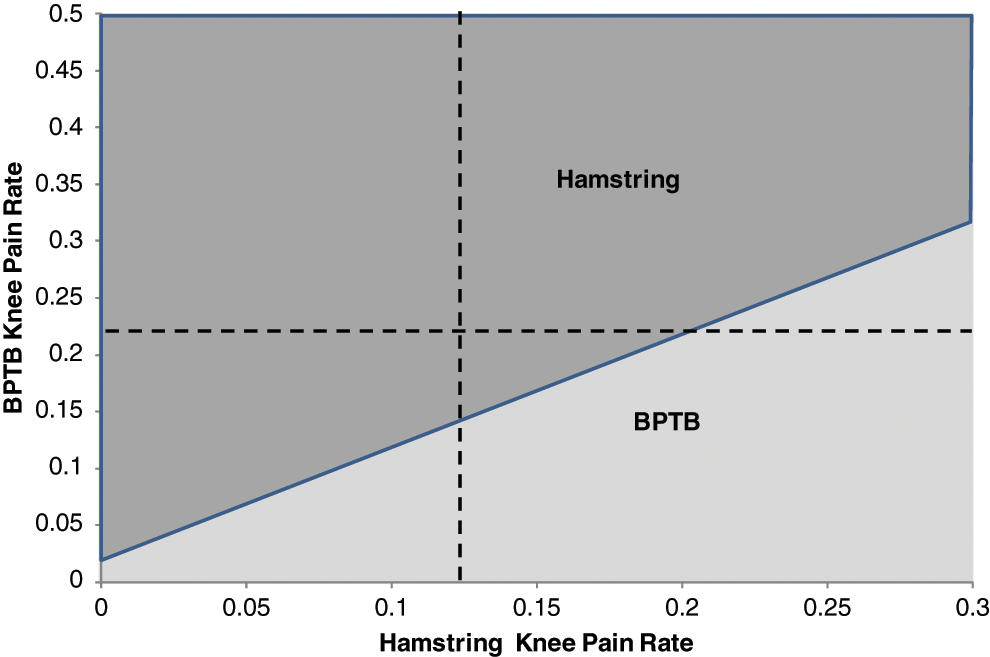
Sensitivity analysis on rate of knee pain of hamstring and bone–patellar tendon–bone (BPTB) autograft.
Discussion
Using the tool of cost-effectiveness analysis and the best evidence currently available, autograft hamstring ACL reconstruction is the most effective and least expensive graft choice. Both BPTB and allograft reconstructions were dominated by HS.
In 2005, Cole et al 6 estimated just over a $1000 increase in expenses associated with autograft ACL reconstruction as compared with allograft reconstruction. The increased expenditures associated with the graft were secondary to the increase in operating room (OR) time, anesthesia time, a higher probability of overnight stay, and an increase in postoperative pharmacy needs (narcotics). However, more recent data with modern block techniques show no increase in overnight stays, and the small increase in OR time is more than offset by the $1300 increased supply costs in allografts, making autografts significantly less expensive. 7 Nagda et al 21 also recently looked at the cost difference between auto- and allografts. They evaluated primarily BPTB and reached the same conclusion that the increased supply cost outweighs the salvaged OR time in allograft. However, this analysis used higher total OR costs than Cooper et al, 7 resulting in a baseline increased cost of BPTB as compared with HS. The use of a 2-way sensitivity analysis on costs (Figure 3) allows examination throughout plausible ranges. Even if the costs of BPTB were assumed to be lowered to the same as HS or, vice versa, the costs of HS were assumed to be raised to be equal to BPTB, BPTB would still become an incrementally cost-effective strategy, as demonstrated in Figure 4 with the dashed lines.
The probability of anterior knee pain both in BPTB and HS autografts drove the model. If the rate of anterior knee pain after BPTB could be reduced from 22% to less than 15%, then BPTB would become a cost-effective treatment choice. This scenario may be the case in a young patient with a pristine patellofemoral compartment who would possibly be at a lower risk of patellofemoral symptoms postoperatively. On the contrary, if the rate of postoperative anterior knee pain was above 43% after autograft surgery, then allograft would become cost-effective (Figure 6). This scenario may play out in a patient with significant underlying patellofemoral arthrosis, predisposing the patient to postoperative symptoms.
Postoperative knee instability also predicted the optimum graft choice. If the rate of instability after HS surgery was increased above 29% (baseline 24%), then BPTB was cost-effective. It has been surmised and recently shown by Kim et al 16 that generalized joint laxity, including knee hyperextension, has a higher failure rate secondary to laxity in HS as compared with BPTB. For the clinical scenario of a young hyperextensible female, BPTB may be a cost-effective graft choice secondary to the higher rate of postoperative knee laxity seen in HS.
Utility health states were obtained directly from patient interviews using TTO questionnaires. In 1998, Mohtadi 19 developed a quality-of-life outcome measure for patients with chronic ACL-deficient knees. Using his validated questionnaire, he determined a health state quality of life for chronic knee instability of 79 out of 100. The TTO data resulted in a similar utility of 0.79 for knee instability in a similar patient cohort, indicating baseline reliability from our collected utility states. Nevertheless, varying the utility values in the sensitivity analysis had no effect on the preferred strategy.
Data from the MOON study group suggest patient-specific variables such as age and activity level affect rates of failure based on graft type. A 2-way sensitivity analysis was performed by plotting the revision rates for both allograft and autograft (Figure 5). Using these revision rates by age demonstrates that HS autografts remain the favored cost-effective strategy throughout all ages evaluated. In older adults, the Marx activity score is lower and the revision rate is therefore lower. 15 In a 35-year-old patient, the relative difference in revision rates between allo- and autografts becomes smaller, such that many surgeons use allografts in this patient population. However, despite this sentiment, the model suggests that HS remains the most cost-effective treatment strategy.
Ultimately, decision analysis is limited by the variables inserted into the model. ACL surgery analysis is limited by the sparse level 1 data that exist for it. The inherent differences in groups found in case control and cohort studies allow bias to be introduced into our model. For example, autograft patients were nearly 4 years younger than allograft patients in a study by Poehling et al 26 with 5-year follow-up. This inherent selection bias may be why 5-year follow-up showed little clinical difference between auto- and allografts. Poolman et al 27 recently examined the methodologies of different meta-analyses to determine why they reach different conclusions. Although none of the meta-analyses was perfect, they determined that Biau et al 2 had the highest level data. Therefore, when applicable, we used these rates in the model.
This cost-effectiveness model serves only as a guide and is certainly not a dictum determining the only graft for all patients. A multitude of factors determine an individual’s graft selection, including risks of postoperative knee pain and knee laxity. Although still controversial, given a recent publication showing no difference in long-term arthritis, the potential long-term ramifications of different graft choices on osteoarthritis were not evaluated. 13 In addition, reoperation between groups for factors such as cyclops lesions has been preliminarily shown to have no difference and therefore was not included in the model. 17 If future studies determine a discrepancy for revision surgeries for factors such as implant removal and cyclops debridement, these factors would need to be incorporated into the model.
Cost-effectiveness analysis is not intended to replace individual clinician judgment but rather is intended to examine both the effectiveness and costs associated with theoretical groups undergoing specific multifactorial decisions. This model suggests that hamstring autograft ACL construction is the most cost-effective method of surgery for the average ACL patient. However, specific clinical scenarios that change postoperative probabilities of the different complication states may sway surgeons to choose either allografts or BPTB autografts.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.