
Abstract
Platelet-rich plasma (PRP) has been shown experimentally to improve tendon and ligament healing because of the presence of an increased concentration of growth factors. 38 In rats, PRP injection improved Achilles tendon healing. 4 In rabbits, PRP injection increased ultimate strength and stiffness when applied to the patellar tendon. 27
In sports medicine, some studies have shown that PRP can enhance the recovery of athletes with ligament and tendon injuries. 15 After anterior cruciate ligament (ACL) reconstruction, PRP achieved a complete homogeneous graft in half of the time compared with a control group. 31 A level III study has shown that PRP hastened the recovery of athletes with an Achilles tendon injury. 32 Moreover, studies have shown better outcomes in chronic patellar tendinopathy with PRP.17,24 The use of PRP in the patellar tendon harvest site reduced donor site morbidity after ACL reconstruction. 9
However, other high-level evidence studies have not shown benefits in the use of PRP. A level I study found PRP to be as efficient as saline in Achilles tendinopathy treatment. 16 In ACL reconstructions with allografts, Achilles tendon ruptures, and rotator cuff lesions, PRP did not improve surgical treatment results.8,30,33
Concerning traumatic sports injuries, one might consider the heterogeneity of these lesions, making them difficult to compare in prospective randomized trials. 14 The patellar tendon is often used as a graft donor site for ACL reconstruction. This procedure creates a standard and well-defined defect, or gap, in the patellar tendon central third. Several studies assessed harvest site defect healing with magnetic resonance imaging (MRI), showing that this healing is usually partial, even after many years.7,21-23,29
In animal studies, patellar tendon defects have been used as an experimental model to assess the effect of growth factors and PRP. Basic fibroblast growth factor used in a patellar tendon defect increased fibroblast proliferation and collagen type III synthesis in rats.10,11 Application of transforming growth factor-β1 increased the mechanical properties of the regenerated tissue in the rabbit’s patellar tendon after resection of the central portion. 3 Also, PRP improved the mechanical properties of the rabbit’s patellar tendon after resection of its central portion. 27
In this study, we used the patellar tendon harvest site as an experimental model to assess the effect of PRP on patellar tendon healing in humans in a prospective, randomized, evaluator-blinded study. The hypothesis was that adding PRP to the patellar tendon harvest site would improve tendon healing and improve clinical outcome at 6 months after ACL reconstruction with a patellar tendon graft.
Materials and Methods
Approval by the local ethics committee and written informed consent were obtained. Recruitment started in November 2008 and was completed in February 2010. Inclusion criteria were ACL injury, bone maturity, and age less than 45 years. Exclusion criteria were complex ligament lesions, osteoarthritis, previous surgeries in the same joint, postoperative infection, arthrofibrosis, reoperation, inadequate follow-up, and thrombocytopenia.
Twenty-eight patients met the inclusion criteria; one refused to participate. Twenty-seven patients were randomized using a computer-generated sequence into 2 groups: PRP (n = 12) and control (n = 15). The resulting demographics are summarized in Table 1. In the PRP group of patients, PRP was added to the patellar tendon defect after harvesting its central third for an ACL reconstruction graft; in the control group of patients, nothing was added. All patients received the allocated treatment (Figure 1).
Descriptions of the 2 Groups
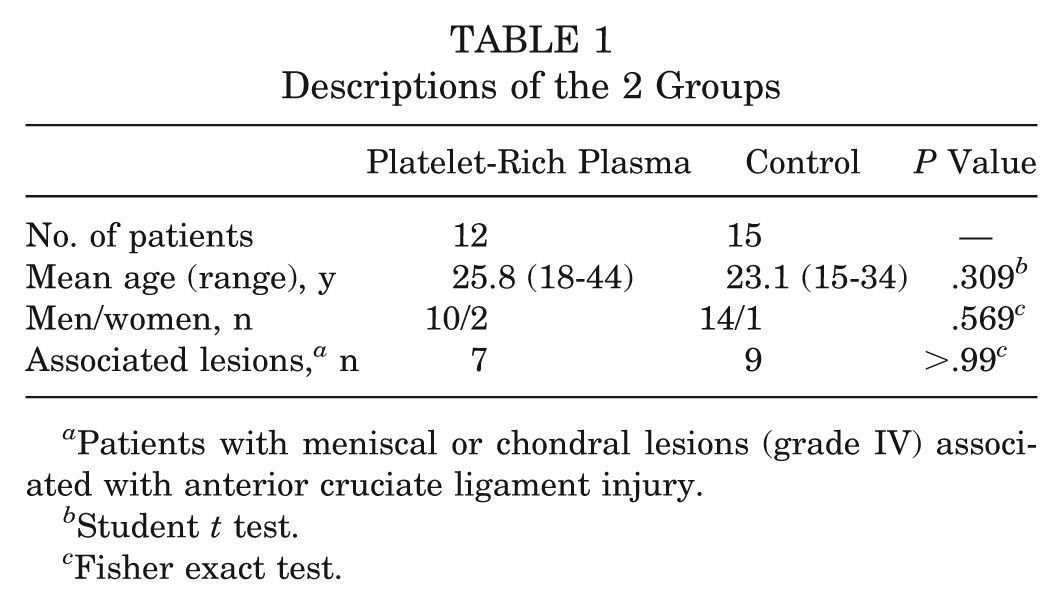
Patients with meniscal or chondral lesions (grade IV) associated with anterior cruciate ligament injury.
Student t test.
Fisher exact test.
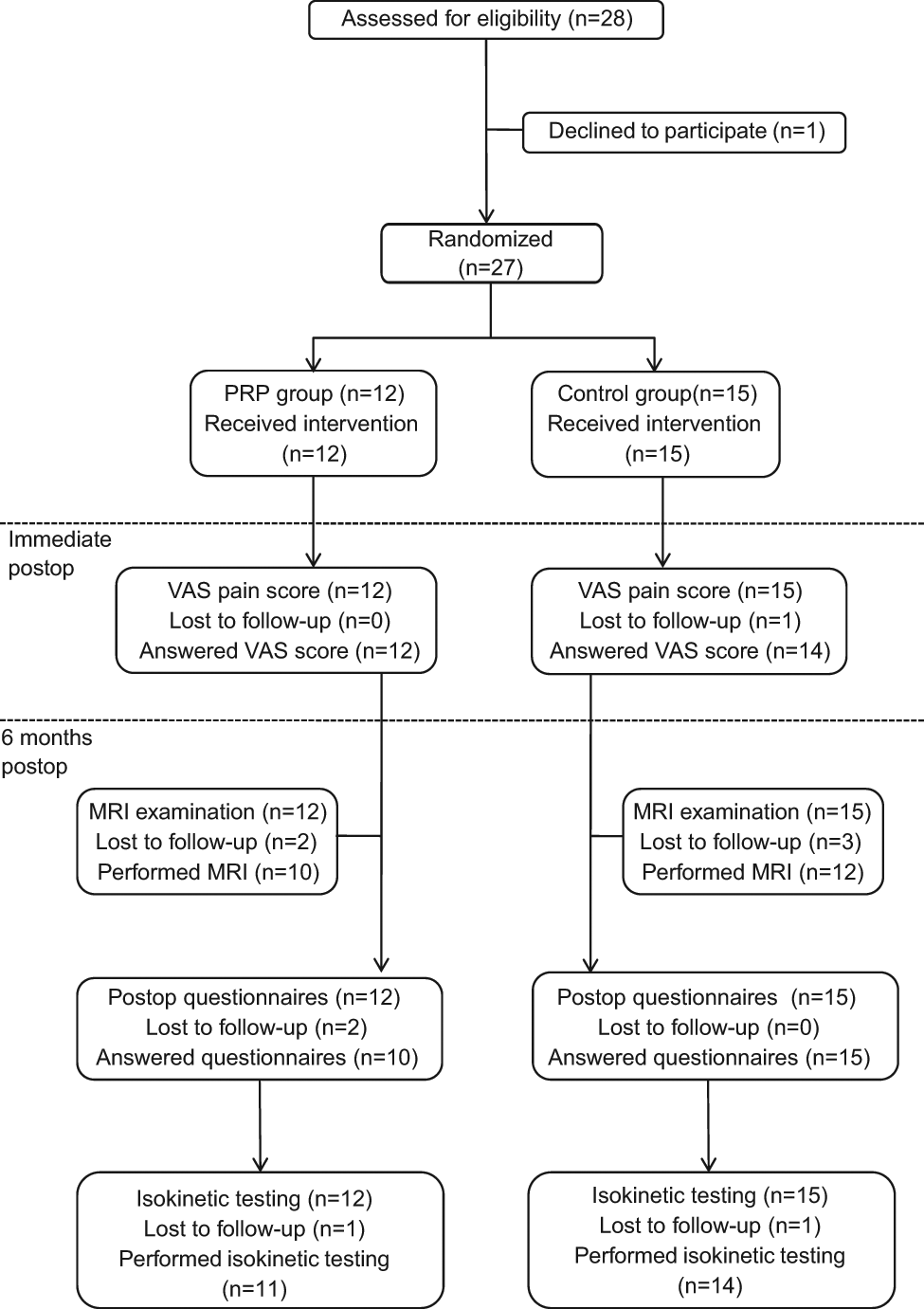
CONSORT flow diagram.
Outcomes
The primary outcome was magnetic resonance imaging (MRI) assessment of patellar tendon harvest site healing. On MRI, we also evaluated tendon thickness and length. Secondary outcomes were functional and clinical evaluations of ACL reconstruction with a patellar tendon graft to examine whether adding PRP to the harvest site affects the clinical and functional outcomes of the procedure. We determined postoperative pain, specific questionnaires of knee function, and isokinetic testing. Any complication was reported whether related to the procedures or not. Our hypotheses were that PRP would increase patellar tendon defect healing and improve clinical outcome at 6 months after the surgery.
PRP Gel Preparation
Platelet-rich plasma was obtained from each patient from the PRP group during anesthesia. A Haemonetics MCS+ 9000 cell separator with a specific kit for platelet apheresis 995-E (Haemonetics Corp, Braintree, Massachusetts) was used in the operating room simultaneously with ACL reconstruction. This cell separator withdraws 450 mL of autologous whole blood through a peripheral venous catheter. Citrate (10%) was used as anticoagulant. Platelet-rich plasma was separated from platelet-poor plasma (PPP) and red blood cells in different sterile collection bags. The red blood cells and PPP (up to 400 mL) were returned to the patient from their collection bags through the peripheral venous access. With this system, we could obtain 30 to 50 mL of PRP. So, in fact, the total amount of blood collected from the patient is up to 50 mL.
The PRP obtained was divided into 10-mL tubes. To the first tube, 0.8 mL of calcium chloride (CaCl2) was added to allow clot formation and separate it from the plasma, which contains autologous thrombin. We added 1 mL of the resulting plasma with thrombin plus 0.8 mL of CaCl2 to another tube to generate the PRP gel. The average concentration of platelets in PRP was 1,185,166/mm3 ± 404,472/mm3 and represented an average increase of 7.65 times (range, 3.82-26.03) related to basal levels. Average white blood cell concentration was 0.91/mm3 ± 0.81/mm3.
Surgical Technique
A single surgeon performed all surgical procedures. Under tourniquet control, a longitudinal incision was made in the anterior aspect of the knee. The peritendon was open longitudinally and separated from the underlying patellar tendon. We obtained a bone–patellar tendon–bone graft with 1-cm width, measured with a ruler. The ACL reconstruction was performed arthroscopically using the trans-tibial drilling technique, and the graft was fixed with a transverse double pin absorbable system (Rigidfix, Depuy Orthopaedics, Warsaw, Indiana) in the femur and an absorbable interference screw in the tibia.
The harvest site was prepared in both groups with absorbable 3-0 sutures at the patellar tendon margins to the underlying fat pad to avoid the gel entering the knee joint through the fat pad (Figure 2). In the PRP group, the patellar tendon defect was completely filled with 20 to 40 mL of PRP gel (Figure 3), and in the control group, nothing was added. The peritendon was closed with absorbable 3-0 sutures without closing the tendon itself.

Patellar tendon harvest site prepared to receive (or not) platelet-rich plasma.
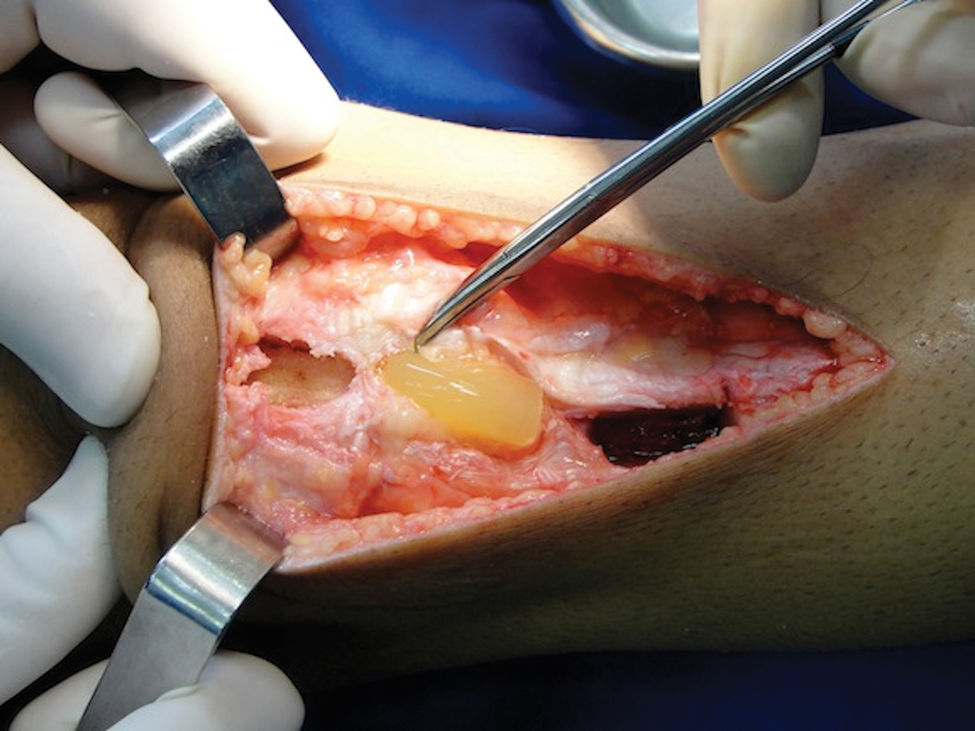
Platelet-rich plasma gel being added to the patellar tendon harvest site.
Postoperative Period and Visual Analog Scale
Suction drains were used inside the knee joint and removed before the patient was discharged, 24 hours after the operation. No drains were used in the subcutaneous tissue. During this period, postoperative analgesia was carefully monitored, and all patients received the same medications (ketoprofen, tramadol, sodium dipyrone) with the same dosage at the same intervals. A visual analog scale (VAS) was used to evaluate pain level at the first postoperative day. We allowed early range of motion and progressive weightbearing with crutches for 3 weeks. All patients followed the same rehabilitation protocol.
Magnetic Resonance Imaging
Patients were requested to have an MRI examination after 6 months to assess patellar tendon harvest site healing. All MRI studies were performed with a 1.5-T magnetic resonance system (Signa Excite HDXT, GE Healthcare, Waukesha, Wisconsin) by using a dedicated 8-channel knee coil. In all patients, axial T2-weighted fat-saturated fast spin-echo sequences (repetition time [TR]/echo time [TE], 3500-4467/65-70 milliseconds; echo train length, 8; 32 sections; number of signals acquired, 3; acquisition time, 4:35 minutes; bandwidth, 31.25 kHz) and sagittal T2-weighted fat-saturated (TR/TE, 3600-4100/84-88; echo train length, 10; 23 sections; number of signals acquired, 2; acquisition time, 3:50 minutes; bandwidth, 31.25 kHz) and intermediate-weighted (TR/TE, 2000-2300/14-18; echo train length, 6; 23 sections; number of signals acquired, 2; acquisition time, 3:10 minutes; bandwidth, 41.67 kHz) fast spin-echo sequences were performed. Sequence parameters included 3.5-mm section thickness, 256 to 512 × 192 to 256 matrix size, and 140 × 140-mm field of view. An independent, experienced musculoskeletal radiologist performed all blinded evaluations.
Using the MRI reconstruction program and computerized distance measurements, the following parameters were considered based on previously published data (Figure 4).7,21-23,29
Gap area of the patellar tendon harvest site (mm2): in the axial direction, the gap size was evaluated in the donor site corresponding to non–tendinous-like tissue signal. Measurement was performed at the midpoint through the length of the tendon from the apex of the patella to the insertion at the tibial tubercle.
Cross-sectional area of the patellar tendon (mm2): in the axial direction, at the same point, the cross-sectional area of the entire ligament, including the defect, was determined to assess ligament thickness.
Patellar height was assessed in the sagittal view with the Insall-Salvati index, determined by the patella length and patellar tendon length ratio.

Using magnetic resonance imaging (MRI), (A) the gap area of the patellar tendon harvest site and the cross-sectional area of the patellar tendon (B) were calculated through the midpoint along the length of the tendon from the apex of the patella to the insertion at the tibial tubercle, as shown in this control group patient. (C) An MRI scan of a platelet-rich plasma group patient, showing a smaller gap (arrow).
Isokinetic Testing and Questionnaires
Before the surgical procedure, patients answered knee function questionnaires (Lysholm, subjective International Knee Documentation Committee, Kujala, and Tegner) and submitted to isokinetic testing. These procedures were repeated 6 months after surgery. Isokinetic strength measurements of the quadriceps and hamstring muscles were performed on a Biodex System 3 Pro (Biodex Medical Systems Inc, Shirley, New York) at 60 and 240 deg/s. We compared the quadriceps peak torques of the injured and noninjured leg to calculate the quadriceps peak torque deficit.
Statistical Analysis
Magnetic resonance imaging data, patient age, and VAS score were analyzed with the Student t test. For VAS score, patient age was controlled with analysis of variance (ANOVA). Statistical analysis of associated chondral or meniscal lesions and patient gender were performed using the Fisher exact test. Questionnaire and isokinetic testing data were compared with the Student t test or the Mann-Whitney U test, depending on distribution. All P values were 2-sided. A P value of .05 indicated a statistically significant difference.
Results
No adverse effects occurred in these patients. Detailed descriptions of the demographics of the 2 groups are shown in Table 1. No differences were found between groups related to age, gender, or meniscal and chondral lesions related to ACL injury.
Magnetic Resonance Imaging
Magnetic resonance imaging was performed after surgery at an average of 208 days in PRP group patients and 212 days in control group patients, with no statistical difference. Patellar tendon harvest site nonregenerated area (gap area) in the PRP group patients was 4.9 ± 5.4 mm2 (95% confidence interval [CI], 1.1-8.8) and in the control group patients was 9.4 ± 4.4 mm2 (95% CI, 6.6-12.2). Statistical analysis showed a significant difference between groups (P = .046). There were no differences between the groups in the cross-sectional area of the patellar tendon or patella height, as reported in Table 2.
Magnetic Resonance Imaging (MRI) Measurements
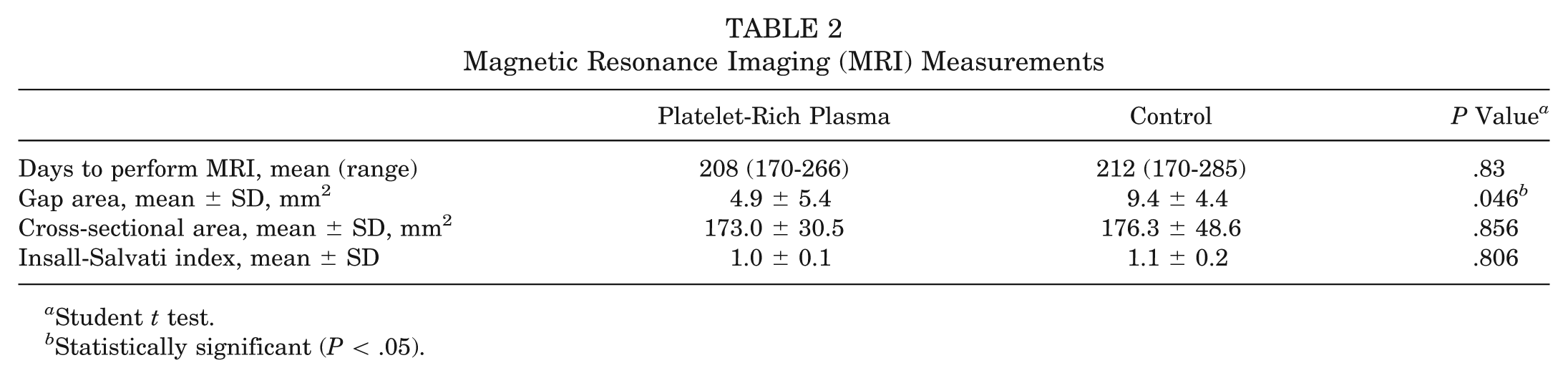
Student t test.
Statistically significant (P < .05).
VAS Score
Postoperative average VAS pain score in the PRP patients was 3.8 ± 1.0 (95% CI, 3.18-4.49) compared with 5.1 ± 1.4 (95% CI, 4.24-5.90) in the control group. The difference was statistically significant, indicating that PRP patients had less postoperative pain (P = .02).
Questionnaires and Isokinetic Testing
Comparing preoperative and postoperative results on subjective tests, we found that 6 months after arthroscopic ACL reconstruction surgery, both groups improved all scores except for the Tegner. On the Tegner questionnaire, both groups had worse results. When comparing the questionnaire scores of the 2 groups, there was no statistically significant difference. Comparing preoperative and postoperative quadriceps isokinetic testing results, both groups had an increased quadriceps peak torque deficit 6 months after ACL reconstruction. There was no statistically significant difference in quadriceps peak torque deficit between groups (Table 3).
Preoperative and Postoperative Results of Isokinetic Testing and Questionnaires a
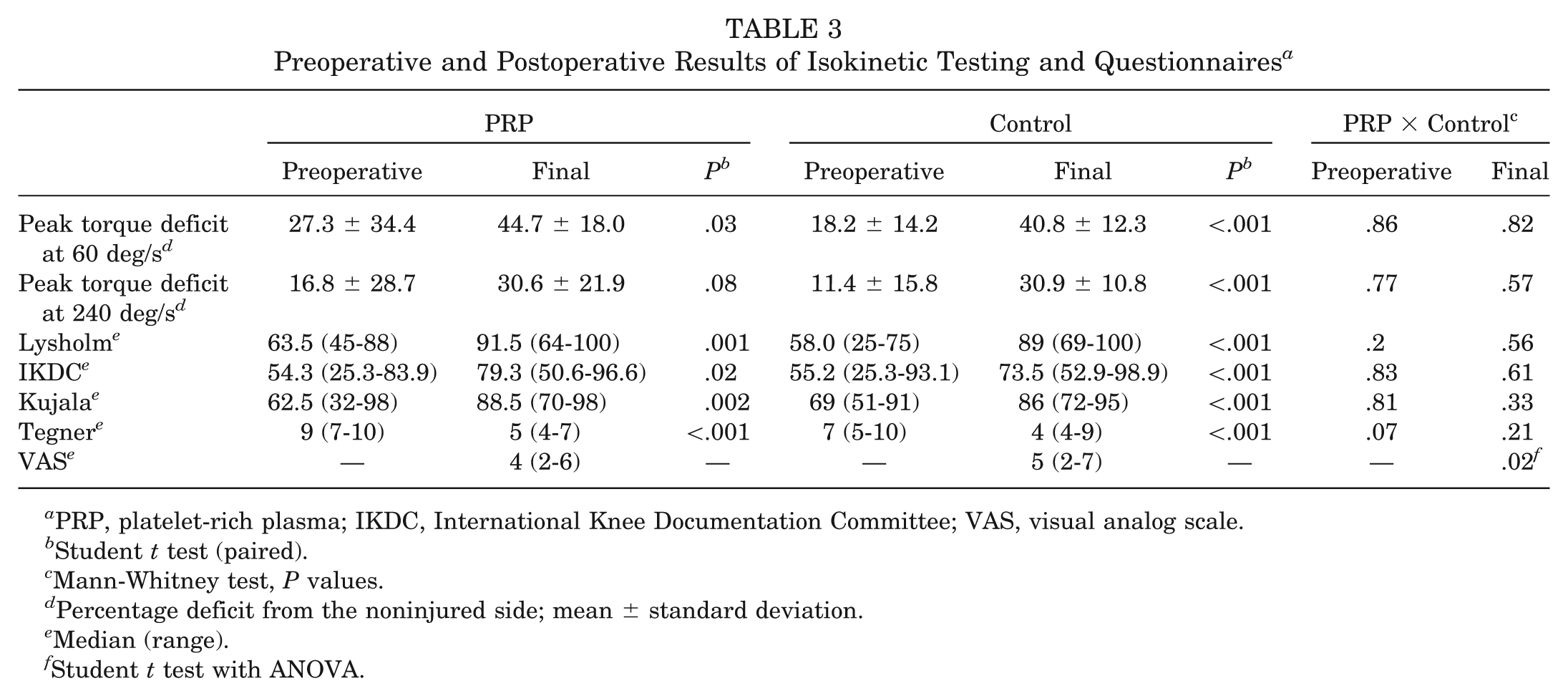
PRP, platelet-rich plasma; IKDC, International Knee Documentation Committee; VAS, visual analog scale.
Student t test (paired).
Mann-Whitney test, P values.
Percentage deficit from the noninjured side; mean ± standard deviation.
Median (range).
Student t test with ANOVA.
Discussion
Harvesting the patellar tendon surgically creates a standardized defect, or gap, in the tendon central third. We used it as an experimental model to assess the effect of PRP on patellar tendon healing.
Platelet-rich plasma has been used to improve the recovery of ligament and tendon injuries in athletes, in spite of a lack of definite clinical evidence.12,18,26 Previous experimental data have shown an improvement in patellar tendon healing in rabbits with PRP, with increased force at failure, ultimate stress and stiffness, and collagen synthesis. 27 Application of PRP gel at the patellar tendon donor site level significantly reduced knee pain after ACL reconstruction with patellar tendon grafts. 9 In that study, the authors showed no difference in the MRI signal of the tendon donor site compared with a control group, but their evaluation was only qualitative and not quantitative.
Previous studies have used MRI to evaluate quantitatively the natural outcome of the patellar tendon after harvesting its central third, showing a progressive gap reduction, with a plateau after 2 years,7,21-23 and a persistent defect even after many years.28,34,35 Previous histochemical and ultrastructural study of the patellar tendon donor site showed that it does not normalize over time.6,25,35
We showed that the patellar tendon had a significantly smaller gap size in the PRP group than in the control cases after 6 months. It indicates that PRP enhanced tendon healing. To verify the possibility of thickening or shortening of the patellar tendon, we also evaluated tendon thickness and length and showed no difference between the groups.
As secondary objectives, we evaluated the clinical and functional outcomes of ACL reconstruction comparing both groups. The VAS pain scores were lower in the PRP group than in the control group in the immediate postoperative period. This analgesic effect of PRP was also shown in other applications, such as knee arthroplasty 19 and periodontal surgery. 2 This may be because of the presence of substances in PRP other than the growth factors, such as serotonin, dopamine, and catecholamines. 12
The exact mechanisms of action of PRP are not fully understood. Mechanical load is essential to tendon healing. One experiment in rats 37 evaluated the effect of PRP and botulinum toxin in the Achilles tendon. They found that the paralyzation of the gastrocnemius muscle with this toxin reduced the positive effect of PRP in tendon healing. They concluded that there is an interplay between PRP action and mechanical load, with PRP-treated tendons responding earlier to this stimulus. However, many in vitro studies have shown a positive effect of growth factors and PRP without mechanical load.1,5,10 Therefore, we believe that both mechanisms, direct and indirect, are involved.
After 6 months, knee function scores were improved in both groups, except the Tegner results, where the findings worsened in both groups. This is expected because Tegner questionnaires address sports activities, 36 and at 6 months, most patients are beginning to return to strenuous sports after ACL reconstruction. 20 Regarding the quadriceps isokinetic testing, both groups had an increased quadriceps peak torque deficit at 6 months compared with preoperative levels. This was also expected according to the literature. 13 These instruments of evaluation are not specific for donor site morbidity and determine the results of ACL rupture treatment, in which harvest site morbidity is just a part of the outcome.
Strengths of this study are that it is a prospective, randomized, and evaluator-blinded study, in which all parameters were evaluated independently. Another strength is the injury pattern, which creates a standard defect in the central portion of the patellar tendon. Through this experimental model, we could assess and compare patellar tendon harvest site healing after a standardized and well-established procedure.
This study has provided some interesting insights but also has some limitations. A weakness in this study is the small number of patients. We had no previously published data to estimate the difference between the groups to calculate the sample size. Second, VAS pain was measured only within the first 24 hours after the surgery, so the duration of the difference in pain is unknown. However, pain is one query of the knee function scores used in this study, which showed no difference between the groups after 6 months.
This clinical follow-up period is considered short for ACL surgery outcomes, but our purpose was not to assess the final outcomes of ACL reconstruction surgery but to evaluate whether there was any clinical difference between the groups. Despite better healing of the patellar tendon harvest site in PRP group patients, we did not find any difference in the score results. We also made a power analysis for these variables and found that, to show a significant difference between the groups, the sample size would need to be huge. We believe that the need for a large sample size in an ACL surgical study may translate in a low clinical significance of the intervention. Finally, a biopsy of the tissue was not performed, and therefore, we cannot comment on whether the structure, composition, or mechanical properties of the patellar tendon were improved by PRP.
In conclusion, we confirmed the hypothesis that PRP could improve tissue healing at the patellar tendon harvest site. Platelet-rich plasma also reduced pain in the immediate postoperative period. With the clinical and functional evaluation instruments used in this study, we were not able to find any difference in the outcome of the procedure, and therefore, PRP did not seem to improve patients’ early recovery after ACL reconstruction with a patellar tendon graft.
Footnotes
Acknowledgements
The authors thank Luiz César Spirandelli, Nelson Tatsui, Marcia Maria de Camargo, and Criogenesis for providing the personnel support and platelet-rich plasma separation system equipment used in this study.
One or more of the authors has declared the following potential conflict of interest or source of funding: Criogenesis and Haemonetics Corp provided the personnel support and platelet-rich plasma separation system used in this study.