
Abstract
Background:
There is increasing evidence that a significant proportion of randomized trials in medicine, and recently in orthopaedics, do not go on to publication.
Purpose:
The objectives of this study were (1) to determine publication rates of randomized controlled trials in sports medicine that have been registered with ClinicalTrials.gov (CTG) and (2) to compare the registration summaries of randomized trials on CTG with final published manuscripts on pertinent methodological variables.
Study Design:
Systematic review.
Methods:
Two independent investigators searched ClinicalTrials.gov for all closed and completed trials related to sports medicine until June 2009 using a text search strategy. The authors then searched for publications resulting from these registered trials in peer-reviewed journals that are indexed with MEDLINE and/or EMBASE as of February 2012 based on study authors and key words provided in the study protocol. Details of primary outcomes and secondary outcomes, study sponsors, and sample size were extracted and compared between registrations and publications.
Results:
Of 34 closed and completed trials registered on CTG, there were 20 resultant publications in peer-reviewed journals (58.8%). There was no significant relationship between source of funding and rate of publication (P > .05). The authors found a discrepancy between the CTG registration summary and the manuscript in at least one methodological variable (primary/secondary outcomes, inclusion/exclusion criteria, sample size) in 16 of 20 (80.0%) articles and a discrepancy in the primary outcome in 8 of 20 (40.0%) published trials.
Conclusion:
Although registration of sports medicine trials in CTG does not consistently result in publication or disclosure of results at 32 months from the time of study completion, observed publication rates are higher than in other orthopaedic subspecialties. Changes are also frequently made to the final presentation of eligibility criteria and primary and secondary outcomes that are not reflected in the registered trial data.
In a landmark study in 2004, Chan et al 6 compared study protocols and published manuscripts of randomized controlled trials in the general medical literature and demonstrated that outcomes reporting is frequently incomplete, biased, and inconsistent. In particular, this study indicated that 62% of published trials had at least 1 primary outcome that was changed, introduced, or omitted compared with the original protocol. To facilitate transparency, the authors suggested that planned trials should be registered and protocols should be made publicly available before trial completion. 6 In part, as a response to these findings, the International Committee of Medical Journal Editors (ICMJE) implemented a policy in 2005 that required registration of clinical trials in a public registry as a prerequisite for publication. 8 Acceptable registries, as determined by the ICMJE, would be electronically searchable, freely accessible to the public, open to all registrants, and managed by a nonprofit organization. 8
At the time the ICMJE implemented the aforementioned policy regarding mandatory trial registration, ClinicalTrials.gov (CTG) was the only existing registry that fulfilled the requirements. ClinicalTrials.gov was originally established in 2000 by the National Institutes of Health (NIH) and Food and Drug Administration (FDA) 37 because of previously existing concerns regarding ethical and scientific issues affecting the design, conduct, and reporting of clinical trials, including the selective reporting of results and unacknowledged alteration of prespecified outcome measures. 40 Furthermore, the establishment of CTG theoretically served to mitigate publication bias, wherein experimental results, which are statistically significant or favorable, are handled differently than are trials that show no statistical difference or trials that demonstrate negative results.1,10,16
Currently, the CTG registers an average of 220 trials a week, with a total of 106,309 trials from 174 countries. 2 Trials are registered in a standard format, including the following details: participant flow, baseline characteristics, outcome measures, planned statistical analyses including sample size, adverse events information, and administrative information.
Despite the intended theoretical uses of CTG as a bias-free repository of information, there is growing concern that a significant proportion of randomized trials do not go on to publication in peer-reviewed journals. For example, Bourgeois et al 4 demonstrated that the rates of pharmaceutical trial publication within 24 months of study completion ranged from 32.4% among industry-funded trials to 56.2% among nonprofit or nonfederal organization–funded trials without industry contributions. Ross et al 34 demonstrated that even among randomized trials that are funded by the NIH and have been registered on CTG, fewer than half of the trials were published in a peer-reviewed journal indexed in MEDLINE within 30 months of trial completion. In the orthopaedic literature, Smith et al 35 demonstrated that the publication rate of arthroplasty trials registered with CTG is 22.8%. In the latter study, changes were frequently made to the final presentation of the data (eg, primary/secondary outcomes measures, sample size) that were not reflected in the trial registry. Furthermore, only 3 of 23 publications had primary and secondary outcome measures that correlated exactly with those listed in the clinical trials database. 35
Despite the increasing importance and enforcement of mandatory trial registration, there is no literature on the compliance of researchers in the field of orthopaedic sports medicine. The objectives of this study were (1) to determine publication rates of randomized controlled trials in sports medicine that have been registered with CTG and (2) to compare the registration summaries of randomized trials on CTG with final published manuscripts on pertinent methodological variables. We hypothesized that orthopaedic sports trials registered on CTG would have low publication rates (ie, <60%) and that there would be significant discrepancies in reporting outcomes when comparing CTG registries with published manuscripts.
Methods
Selection Criteria
Registered studies were eligible for review if they met the following criteria: (1) randomized controlled trials registered on CTG; (2) trials that were reported as closed and completed as of June 2009; (3) trials investigating operative or nonoperative (rehabilitation, immobilization, injections) treatment for disorders of the shoulder, hip, knee, or ankle joints; and (4) trials investigating operative or nonoperative (rehabilitation, immobilization, injections) treatment for common soft tissue injuries in the field of orthopaedic sports medicine, including muscle contusions or tears, tendinitis, tendinopathy, and bursitis. Exclusion criteria included (1) ongoing randomized trials, (2) trials evaluating anesthetic interventions (ie, anesthetic type, preoperative or postoperative nerve blocks) for patients undergoing arthroscopy, and (3) trials investigating the role of nonoperative modalities only (injections, pharmaceutical agents, physical therapy) for the treatment of osteoarthritis in the appendicular or axial skeleton. We limited our sample to trials whose overall recruitment status had been updated to notify CTG that the trial was completed by June 30, 2009. A trial with a status of “completed” is defined by the National Library of Medicine as a trial that has ended and participants are no longer being examined or treated (ie, the last participant’s last visit has occurred). 2 This deadline was chosen to provide authors a minimum of 32 months from study completion to manuscript publication.
Search Strategy
Two investigators independently performed a search of orthopaedic sports medicine trials in CTG. Because of the large scope of topics pertinent to the field of sports medicine, 3 distinct search strategies were employed (with search terms defined a priori) to ensure that pertinent studies relating to the most common sports medicine diagnoses would not be missed. All discrepancies in the search results were resolved by discussion among investigators by reviewing the inclusion and exclusion criteria of study selection.
In search strategy 1, the terms (knee OR shoulder) AND (cartilage OR ligament OR tendon OR meniscus OR labrum) were used. By limiting our search to interventional studies closed to enrollment with complete follow-up by June 2009, we identified 34 studies for analysis. After reviewing trial registrations on CTG, it was determined that 12 studies were related to the medical management of osteoarthritis, and 2 were related to anesthetic interventions for arthroscopy. These papers were excluded, resulting in 20 eligible studies.
In search strategy 2, the terms (sports medicine OR arthroscopy) were used with the same aforementioned search limits. This yielded an additional 42 papers. Of these, 12 were related to postoperative analgesia, 8 were related to the medical management of arthritis, and 10 were duplicates from our previous search. This resulted in 12 new pertinent studies from our second search and a running total of 32 eligible studies.
Finally, in search strategy 3, common orthopaedic sports medicine diagnoses were used as the basis for a text-searching strategy (with the same limits): shoulder instability (1 additional study found), rotator cuff (4 additional studies), SLAP (no additional studies), knee meniscus (no additional studies), cruciate ligament (no additional matches), collateral ligament (no additional matches), patellofemoral (2 additional studies), quadriceps OR patellar OR Achilles OR tendon (1 additional study), and ankle sprains OR ankle instability (1 additional study found). This yielded a running total of 41 studies. Review of the abstracts of these studies by 2 reviewers indicated that 3 of these studies were observational studies, 2 were double cohort studies, 1 was for physical therapy protocols following total hip arthroplasty, and 1 was to evaluate dietary therapy for obesity.
Publication Rate
Each identified clinical trial registration was reviewed to determine whether a publication resulting from the study was listed. If no publication was listed on CTG, 2 investigators independently searched MEDLINE and EMBASE (February 2012) using the key words provided in the trial registry and by the names of the principal investigator. Published manuscripts were identified by the title and content of the abstract. This study used 32 months between completion and literature search for a publication in MEDLINE.
Published studies were also reviewed for the National Clinical Trials Identification Number (NCT ID), study sponsor, and authors to confirm a match with the registry. Each listing on the registry is given a unique NCT ID with the prefix “NCT” and an 8-digit number that is used to locate and identify a specific trial. 13
Data Extraction
For each of the 34 studies determined to be eligible, 2 reviewers (JC, SST) independently extracted relevant data from the registry and published manuscript (if applicable), including authors, year of publication, NCT ID and its presence in the paper, trial status (complete, active, not recruiting, etc), study sponsor, study start date, registration date and completion date, primary and secondary outcome measures, inclusion and exclusion criteria, study phase and design, study location, and sample size. Industry trials were defined as those whose primary sponsor has a direct financial involvement with the manufacturing or retail of a particular intervention. Nonindustry trials are those in which the primary sponsor was a university or government funding agency. Discrepancies in data abstraction were resolved by discussion.
We then evaluated the agreement between the study methodology reported in the registry and that of the final manuscript. Discrepancies were defined as per the criteria of Chan et al 6 : (1) a prespecified primary outcome was now reported as secondary or was not labeled as either primary or secondary in the publication, (2) a prespecified primary outcome was omitted from the published article altogether, and (3) a new primary outcome, distinct from what was reported at registration, was introduced in the published article. In cases where there was discrepancy in any of the aforementioned categories among the 2 reviewers, the manuscript and corresponding registry entry were reviewed again, and agreement was reached by mutual consensus.
Statistical Analysis
Study characteristics were presented with descriptive statistics. The kappa statistic was used to calculate the agreement between reviewers on study eligibility. We used the standard and well-established criteria of Landis and Koch 26 for the interpretation of agreement studies. Briefly, they define poor agreement as 0 to 0.2, fair agreement as 0.21 to 0.40, moderate agreement as 0.41 to 0.60, substantial agreement as 0.61 to 0.80, and nearly perfect agreement as more than 0.80.
A Fisher exact test was used to determine the association between trial sponsor and the rate of publication of registered trials. Statistical tests were 2-tailed, with a type I error of P = .05.
Results
Literature Search
Our search identified 34 eligible studies (Figure 1). The overall agreement for the search was substantial as indicated by a kappa value of 0.80. The percentage agreement between the 2 reviewers was 93%.
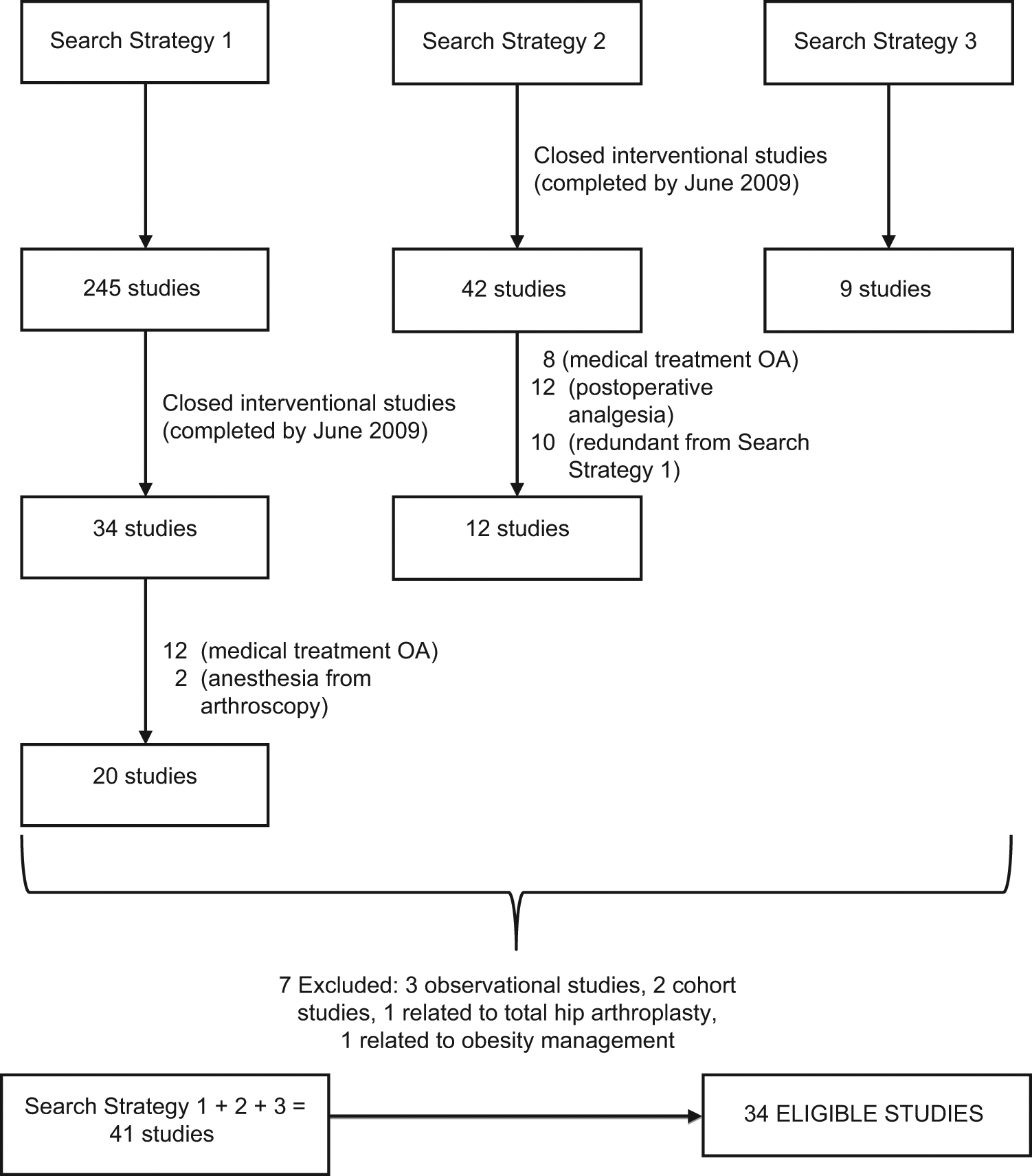
Search strategy for sports medicine trials registered on ClinicalTrials.gov (CTG). A detailed search history is illustrated for search strategy 1. OA, osteoarthritis.
Characteristics of Registered Trials
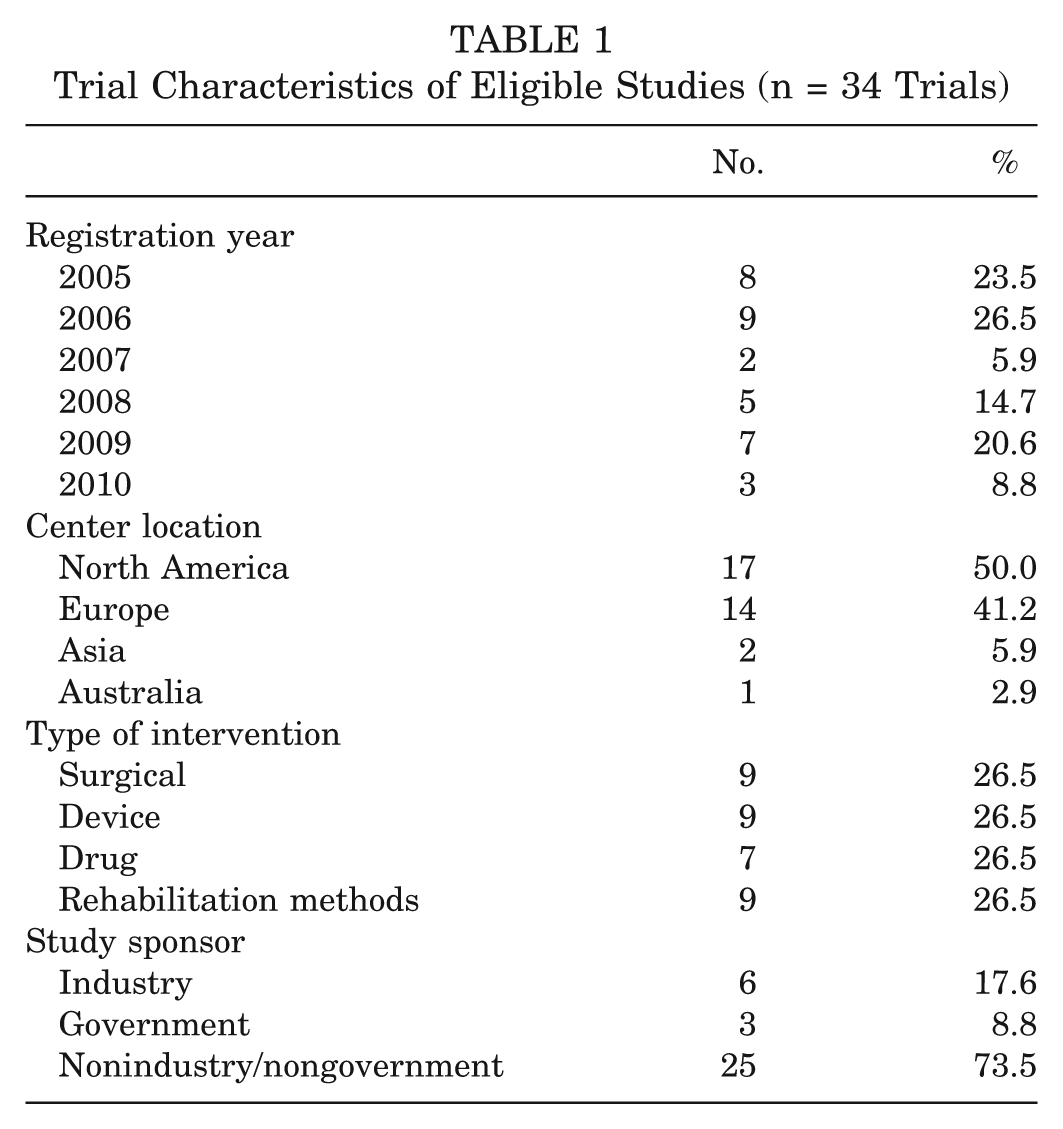
The baseline characteristics of registered trials are highlighted in Table 1. The 34 eligible trials evaluated interventions for surgical procedures, devices, rehabilitation protocols, or the use of corticosteroid injections. They were conducted at centers located in North America, Europe, Asia, and Australia.
Trial Characteristics of Eligible Studies (n = 34 Trials)
Publication Rate
Overall, 20 of 34 (58.8%) eligible trials were published. A list of unpublished trials can be found in the Appendix (available in the online version of this article at http://ajs.sagepub.com/supplemental/).
According to the registration information on CTG, 2 trials (10.0%) were industry sponsored,12,17 2 (10.0%) were government sponsored,14,22 and 16 (80.0%) were sponsored by nongovernment and nonindustry sources. ‖ There was no statistically significant difference in publication rates between industry-sponsored and nongovernment/nonindustry trials (P = .21), between government-sponsored and nongovernment/nonindustry trials (P = 1.00), or in industry-sponsored trials (P = .52).
The sponsors of the 16 nongovernment/nonindustry trials were either hospitals or universities. However, when looking at the funding sources disclosed in the published manuscripts of these trials, 2 trials disclosed industry funding,36,39 5 trials acknowledged government grants,3,15,24,30,38 5 trials reported either no support or hospital/university funding,11,20,25,27,28 and 4 trials gave no details on funding.5,18,21,31
Consistency Between Trial Registration and Publication
The results of the comparisons for each published trial between the CTG registration and the published manuscript are presented in Table 2. We found a discrepancy between the CTG registry and the manuscript in at least 1 category (primary/secondary outcome, inclusion/exclusion criteria, sample size) in 16 of 20 (80.0%) articles. Seven of 20 trials (35.0%) had discrepancies in primary outcome. In 4 trials, the prespecified primary outcome was reported as secondary or not labeled at all,14,21,28,36 and in the other 3 trials, a new primary outcome was introduced.3,15,24 Ten of 17 trials (58.8%) had a discrepancy in secondary outcomes. Seven of 20 trials (35.0%) had a discrepancy in inclusion/exclusion criteria, and 8 of 20 trials (45.0%) had a discrepancy in sample size. Compared with the registration information, the sample size was lower in 5 published trials and higher in 3 trials. The discrepancies in sample size ranged from 13.3% higher 5 to 64.1% lower 14 than initially registered. Finally, 9 of 20 (45.0%) published manuscripts included the NCT ID number.
Trial Characteristics of Published Studies (n = 20 Trials)
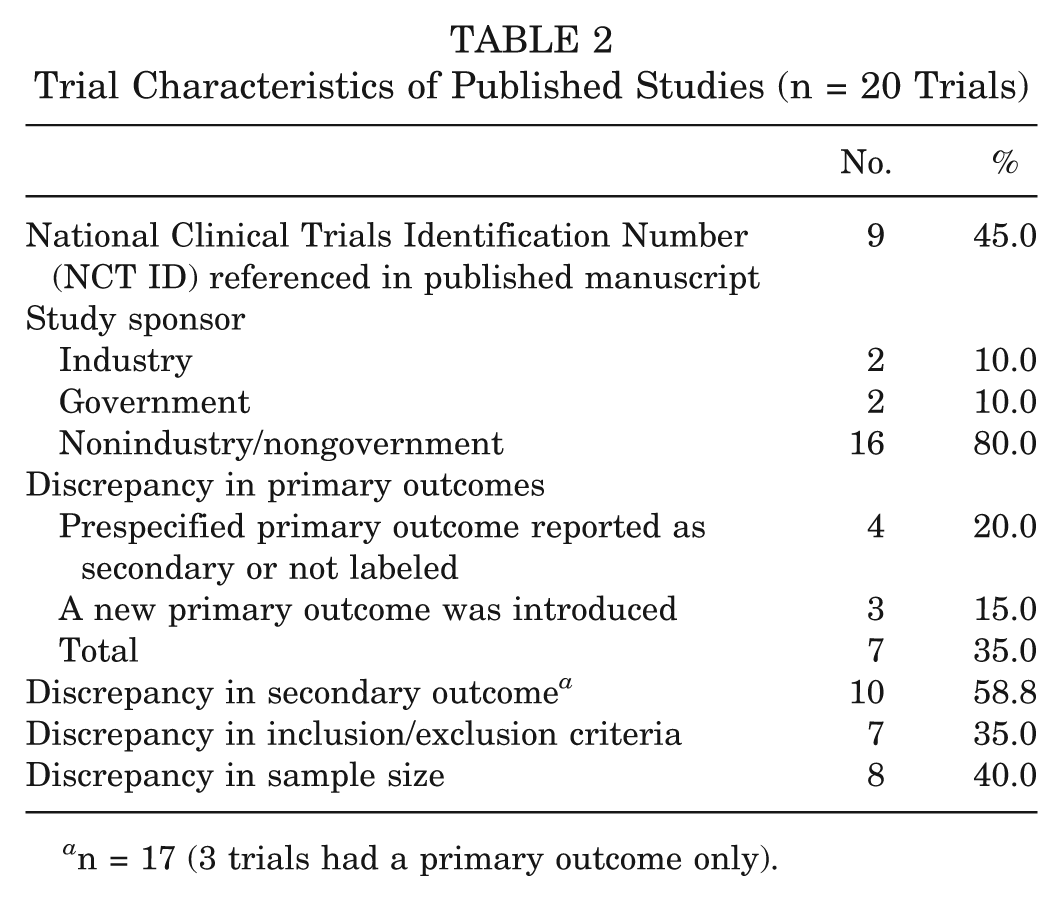
n = 17 (3 trials had a primary outcome only).
Discussion
In our study, we found that 58% of sports medicine randomized controlled trials registered on CTG were published in a peer-reviewed journal indexed by MEDLINE or EMBASE within at least 32 months from study completion. In addition, there was a discrepancy between registries and published manuscripts in important methodological variables, including primary and secondary outcomes, eligibility criteria, and sample size requirements in a majority of cases. Given that Level I evidence in the form of well-designed randomized controlled trials is considered the benchmark in clinical research, as well as the potential influence such research can have on a clinician’s daily practice, it is imperative that such studies be published in a timely manner and reported with complete transparency. The findings in this study challenge the notion that all Level I evidence is equal. Rather, there is a need for heightened awareness and recognition of the potential for publication bias and outcomes reporting bias within the field of sports medicine. The usefulness of CTG ultimately depends on whether responsible investigators and sponsors make diligent efforts to submit complete, timely, accurate, and informative data about their studies. 40
Our observed publication rate of sports trials registered on CTG is slightly higher than the rates observed in the orthopaedic literature. Smith et al 35 reported an overall publication rate of 22.8% for arthroplasty trials, whereas Gandhi et al 13 reported a publication rate of 43.2% for orthopaedic trauma trials registered with CTG. Reasons for failure to publish include lack of incentive to disseminate unsupportive findings, time constraints, limited resources, changing interests, or even failure to have an article accepted by a journal.13,34 Consistent with Gandhi et al, 13 we did not observe a difference in publication rates based on study sponsor; however, we did find discrepancies between sponsors as registered on CTG and funding sources disclosed in the published manuscripts. Two trials received industry funding, and 5 trials were supported by governmental grants, although they were all registered as sponsored by the universities and hospitals.
Forty-five percent of published trials in this study reported the NCT ID number in the final manuscript. A previous study looking at orthopaedic trauma trials demonstrated that the NCT ID was not included in approximately half of published papers. 13 It is important to include the NCT ID in a published manuscript to allow the reader to evaluate the strength of the trial by comparing it with the original plans as outlined in the registry. 13 Such transparency can allow the educated reader to make sound judgments regarding the presence of bias when interpreting the results of a manuscript.
Next, we found a discrepancy between the CTG registration summary and the manuscript in at least one methodological variable in 80% of articles. Furthermore, 40% of the trials reviewed in this study had a discrepancy in the primary outcome. Such discrepancies in outcomes reporting are similar to that observed in published arthroplasty trials that have been registered on CTG. 35 As stated previously, such bias is certainly not unique to the orthopaedic literature and was also documented by Chan et al 6 in 2004.
Although the current study highlights the modest publication rates and discrepancies in reporting in registered randomized controlled trials in sports medicine, previous research has highlighted inconsistencies in this field. Kleweno et al 23 performed a systematic review of abstracts presented at the American Orthopaedic Society of Sports Medicine annual meetings from 1991 to 2001. Overall, 59.4% of abstracts were published in a peer-reviewed journal within 5 years. However, 63% of published manuscripts had at least one major inconsistency in one of the following areas: study objective/hypothesis, study design, primary and secondary outcome measures, sample size, statistical analysis, and reporting of results. 23
Based on the aforementioned shortcomings in the sports medicine literature, there is significant potential that both publication bias and outcomes reporting bias may be playing a role. Publication bias refers to the tendency of researchers and journal editors to more readily report and publish positive findings than to report negative or inconclusive findings, ultimately leading to bias in the overall published literature.1,10,19 Incomplete reporting would lead to wasted expenditure on trials and would bias the results of meta-analyses or systematic reviews. Although the current study did not ascertain whether the included trials had positive, negative, or inconclusive findings, the potential for publication bias certainly cannot be ruled out. It is one of the many possible explanations as to why more than 40% of the registered trials were not published at a minimum of 32 months from trial completion. In a study performed by Dickersin et al, 9 an analysis of completed unpublished trials revealed that the major reasons for nonpublication were “negative” results and lack of interest.
The results of this study indicate that outcome reporting bias is clearly present in the sports medicine literature. This type of bias occurs when several outcomes are measured over the course of a trial, but these are ultimately reported selectively based on the strength and direction of those results.7,29 Although the primary outcome is typically chosen to represent a measurement that is clinically meaningful, defining primary outcomes a priori (ie, prior to initiation of a trial) is also important as such a determination has direct implications in determining sample size and study power. Changing outcomes midway raises concerns that a given study is underpowered because the sample size determination depends on assumptions for the primary outcome only. Such a posteriori hypothesizing is also a major limitation in distinguishing association from causation and raises questions about the study design.
The role of administrative and technical barriers as an explanation for the observed discrepancies in outcomes reporting cannot be ruled out. ClinicalTrials.gov uses a Web-based system to facilitate clinical trial registration by any sponsor, principal investigator, or other person or organization with primary responsibility for the trial. 33 ClinicalTrials.gov includes mandatory and optional data elements. Trials cannot be registered without completion of all mandatory data elements, approval by a human subject review board (or equivalent), and conformity to the regulations of the appropriate national health authorities. The requirement for mandatory data points may preclude some investigators from pursuing timely registration. Data entry into CTG can be revised as the study develops and by any of the investigators. Such revisions may not be actively pursued by all investigators.
Another concern is the date of trial registration in relation to the time frame in which the study was conducted. Examining the dates of trial registration and data collection completion, we found that 13 of the 20 trials were registered retrospectively after the data were collected. This practice adds to the possibility of bias; it is impossible to determine if key methodological aspects changed after trial initiation as there is no record that predates the trial. As a response to such processes, some journals now mandate that clinical trials must be prospectively registered before enrollment of the first patient on any national or international registry.
In trials examining the results of oncology medications, Rasmussen et al 32 found that trial registration without full reporting of results did not reduce bias in the results favoring new drugs. On this basis, they recommended inclusion of full results reporting in trial registers and the creation of a system to assess if results have been completely reported. This was also supported by Ross et al, 33 who pointed out that without reporting of all data elements, CTG would be unable to eliminate selective publication bias.
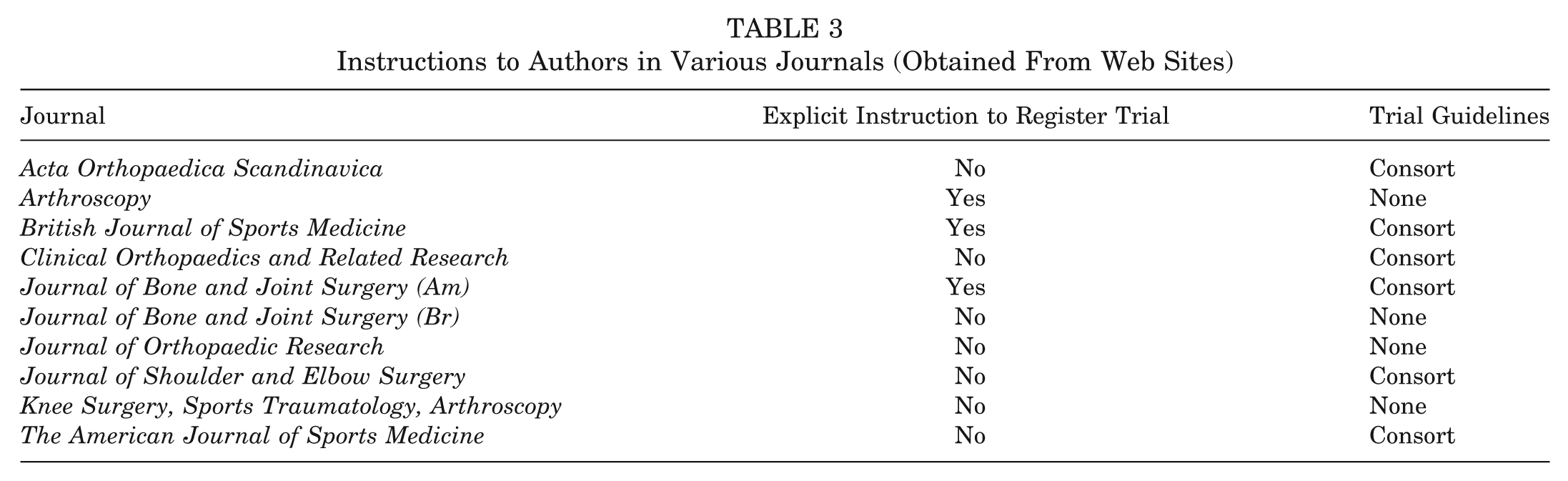
Interestingly, few orthopaedic journals that publish sports medicine trials explicitly state the need to register any trial on the instructions webpage for a given journal. However, several do state that the trial must conform to CONSORT guidelines. As of February 2012, several specialty journals do neither. Table 3 illustrates the preference for trial registration and reporting for the major orthopaedic sports medicine journals.
Instructions to Authors in Various Journals (Obtained From Web Sites)
This study does have some limitations. First, there may have been some selection bias in determining which papers we included in our analysis. Because of the large scope of anatomic and didactic topics that can be included within the realm of sports medicine, there is a possibility that our search strategy may have overlooked some areas. Nonetheless, we attempted to perform a rigorous search with 3 distinct yet integrated search strategies performed by 2 independent investigators. We also limited our inclusion of trials to those related to the shoulder, hip, knee, and ankle to focus on the most common diagnoses that are pertinent to practicing physicians. In doing so, some sports content related to other anatomic areas may have been overlooked. Finally, it is possible that the closed, completed trials registered on CTG that were included in this study may not have been published because the study authors may not have had time for data analysis, manuscript preparation, and submission for publication. As a result, our findings may underestimate to some degree the publication rates of registered trials on CTG. However, we did not review registered trials that were completed after June 2009—this allowed authors at least 32 months to publish their trials. This timeline is higher than similar studies that have been published on publication rates for registered trials on CTG.34,35
To the best of our knowledge, this is the first publication to review trial registration on CTG and evaluate resultant publication rates and outcomes reporting bias in the sports medicine literature. The results of our review indicate that a significant proportion of registered sports medicine trials are not published within 32 months of trial completion. Moreover, changes are frequently made to the final presentation of the data that are not reflected in the registry of the trial. When trials are registered, a great number of them do not cite the registration number in the publication, making it difficult for the reader to evaluate the study conclusions in relation to the original plans for the trial. It is clear that more rigorous adherence to protocols is required by trial investigators in addition to vigilance by journal editors with regard to discrepancies in outcomes reporting bias, possible publication bias, and eligibility criteria.
Conclusion
Although registration of sports medicine trials on CTG does not consistently result in publication or disclosure of results at 32 months from the time of study completion, observed publication rates are higher than in other orthopaedic subspecialties. Changes are also are frequently made to the final presentation of eligibility criteria and primary and secondary outcomes that are not reflected in the registered trial data.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.