
Abstract
Background:
A few national cruciate ligament (CL) registers have been initiated with operative surveillance and outcome monitoring. No nationwide study describing CL injury has ever been done.
Purpose:
To study the incidence and characteristics of patients diagnosed with cruciate ligament injury in Sweden.
Study Design:
Descriptive epidemiology study.
Methods:
Data for all patients with a diagnosed CL injury between 2001 and 2009 were identified from the National Swedish Patient Register. Risk analysis and specific incidences were calculated according to age, sex, geographic region, and surgery.
Results:
A total number of 56,659 patients with CL injury were included in the study, and the overall incidence of CL injury in Sweden was 78 per 100,000 persons. Sixty percent of the patients were male. The mean age was 32 years (range, 1-98 years), and 50% of the cohort was younger than 30 years. There was an increased rate of injury among female patients younger than 20 years as compared with male patients in that age group. Among patients with CL injury, 36% underwent reconstructive surgery, with one-third of these performed within 1 year after injury. Among patients who underwent surgery, 59% were male; the mean age was 27 years (range, 5-89 years).
Conclusion:
This study defines the incidence of CL injury and also demonstrates sex differences in which men were more likely to sustain a CL injury, although female patients were injured at an earlier age. The findings in this study corroborate the results from recent surgical registers.
Clinical Relevance:
No data have hitherto been published including all patients with CL injury, treated both surgically and nonsurgically. Such baseline epidemiologic data are crucial to be able to validate and judge the generalizability of results from procedure registers and clinical studies.
Keywords
Cruciate ligament (CL) injury occurs primarily in activities with knee-pivoting movements such as soccer, floorball, team handball, basketball, and alpine skiing. Affected persons are in general young. A knee with a CL injury is often functionally unstable and predisposes the person to subsequent injuries and early onset of osteoarthritis.4,5,14,26
Very few previous studies have investigated the incidence of CL injury. A Danish study published in 1991 reported a yearly incidence of 30 per 100,000 people. 23 In the United States, it has been estimated that about 80,000 CL injuries occur every year and that almost half of them undergo reconstructive surgery. 12 Another study from New Zealand reported an incidence rate of 1147.1 per 100,000 person-years for (nonsurgical) knee ligament injuries, 10 and a Swedish hospital-based study of 159 patients reported a yearly incidence of 81 per 100,000 inhabitants aged 10 to 64 years. 8 The true incidence of CL injury in Sweden and internationally is unknown due to lack of population-based studies.
Optimal treatment of a CL injury is under continuous debate despite a plethora of inventions ranging from new surgical methods to rehabilitation protocols.19,31 Different techniques and grafts have been suggested.3,29,36 Reconstructive surgery of the CL has become a common procedure, especially in patients engaged in high-level sports, whereas nonoperative treatment is considered to have a satisfactory outcome in the general population.6,35
To the best of our knowledge, this is the first nationwide, population-based study investigating the incidence of CL injury as well as the operative and nonoperative treatment of this injury. In this open cohort study, we used data from the Swedish National Patient Register to estimate the sex- and age-specific incidence of CL injury and define demography and characteristics of patients diagnosed and/or treated surgically for CL injury.
Methods
The study was a nationwide, open cohort study using data from the population-based National Patient Register (NPR), including both inpatient and outpatient care, from 2001 to 2009. The NPR was established in 1964 by the Swedish National Board of Health and Welfare. For inpatient visits, the register has been 100% complete since 1987 and is of high validity. A review of 132 studies resulted in an overall positive predictive value of 85% to 95%. 18 The outpatient register, including information on specialist care at the hospital, started in 2001. The NPR contains documentation of all individual hospital discharges, with each record corresponding to 1 hospital-episode. Every record contains a national registration number, a unique identifier assigned to all Swedish citizens, the date of hospital admission and discharge, age, sex, geographical location of the hospital, clinical ward, and up to 8 discharge diagnoses and surgical procedures. The discharge diagnoses are coded according to the World Health Organization’s International Classification of Diseases (ICD-7 until 1968, ICD-8 from 1969-1986, ICD-9 from 1987-1996, and ICD-10 thereafter). We included all patients diagnosed with CL injury (ICD-9: 844C, cruciate ligament in knee; ICD-10: S835, distortion engaging the cruciate ligament in the knee; M235, chronic instability in the knee joint) for the first time between 2001 and 2009 (Figure 1). The NPR also provided data on those who underwent CL reconstructive surgery (ICD-9: 8573, reconstruction of ligament in knee; ICD-10: NGE41, arthroscopic or endoscopic reconstruction of ligament in the knee without foreign material; ICD-10: NGE42, open reconstruction of ligament in the knee without foreign material). The earlier coding was used to exclude those with previous injuries. This resulted in 65,179 unique patients with a diagnosed primary CL injury between 2001 and 2009. This methodology did not allow for distinction between anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) injuries or information on diagnostic method.
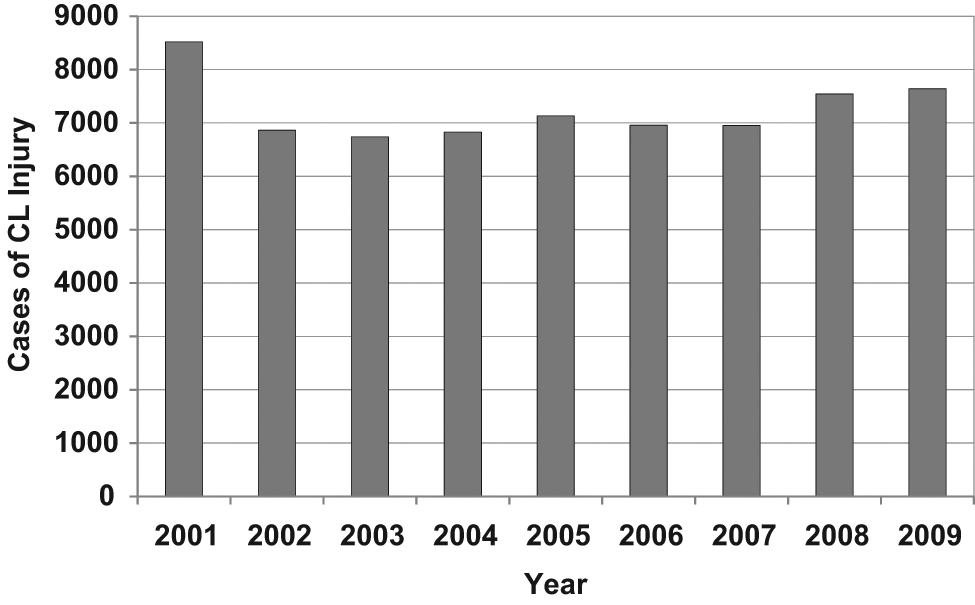
Incident and prevalent cases of cruciate ligament (CL) injury reported in the Swedish National Patient Register between 2001 and 2009.
The data collection started in 2001, initially with a pool of registered prevalent cases with CL injury in 2001 and successively stabilizing on a lower number, assumed to represent the annual incidence (Figure 1). Thus, we defined patients diagnosed for the first time in 2002 and onward as incident cases, resulting in 56,659 unique patients with CL injury (33,778 male and 22,881 female patients). Of these patients, 20,622 underwent reconstructive surgery.
The Swedish population statistics and date of death were acquired using registers held by Statistics Sweden. 32 This study was approved by the regional ethics committee, Karolinska Institutet (Dnr: 2010/1713-32).
Statistical Analysis
Poisson regression model was used to estimate the risks associated with sex, categories of age (≤10, 11-20, 21-30, 31-40, 41-50, >50), residential place (20 Swedish counties), and year of diagnosis (2002-2009).
The Kaplan-Meier estimate was computed to describe the probability of being operated with CL reconstruction, and a statistical hypothesis test (the log rank test) was performed to compare survival curves.
The age- and sex-specific incidence rates were computed by using the number of midyear population as the denominator. The incidence rates were calculated by dividing the numbers of new cases in each age and sex group by the age-, sex-, and calendar year–specific population figures obtained from Statistics Sweden. 32 Confidence intervals for estimated incidences were calculated assuming a Poisson distribution for the number of newly diagnosed patients. Student t test was used for the comparison of continuous variables, and the χ2 test was used for categorical variables when comparing means of the groups. The significance level was set at P < .05.
All statistical analysis was made with SAS (Statistical Analysis Software, version 9.2; SAS Institute, Cary, North Carolina). Proc Genmod was used for Poisson regression, and the logarithm of population size was used as the offset variable.
Results
We identified 56,659 patients with CL injury during 2002-2009 (Table 1). The average annual incidence of CL injury from 2002 to 2009 was 78 per 100,000 inhabitants (95% confidence interval [CI], 77.1-78.4). The mean (SD) age at diagnosis was 32 (13) years, and the median was 31 years (range, 1-98 years). Male patients had higher risks for injury than female patients (relative risk [RR] =1.44; 95% CI, 1.41-1.46). Table 2 shows the RR and 95% CI for CL injury in different age groups. We found a statistically significant difference between different age groups, with a peak during the third decade of life for men and a high-risk period from ages 11 to 20 years for female patients. The results revealed that men aged 21 to 30 years had the highest incidence: 225 per 100,000 inhabitants (95% CI, 220-229). Female patients were injured at an earlier age than male patients with the highest incidence: 144 per 100,000 inhabitants (95% CI, 140.1-147) in patients aged 11 to 20 years (Figure 2A).
Characteristics of 56,659 Patients With Cruciate Ligament Injury in Sweden, 2002-2009 a
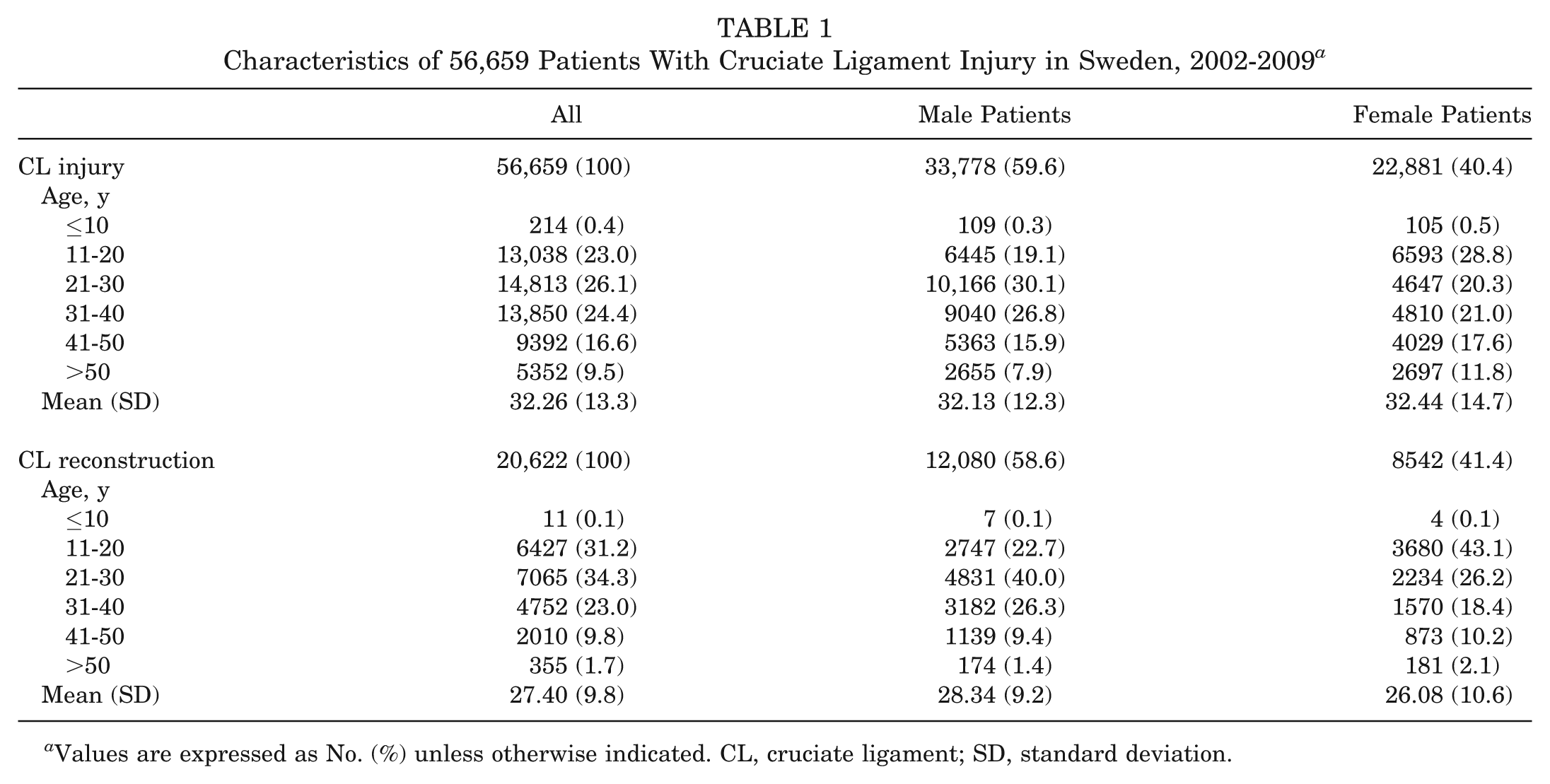
Values are expressed as No. (%) unless otherwise indicated. CL, cruciate ligament; SD, standard deviation.
Relative Risk of Cruciate Ligament Injury and 95% Confidence Interval Among Different Age Groups, Stratified by Sex a
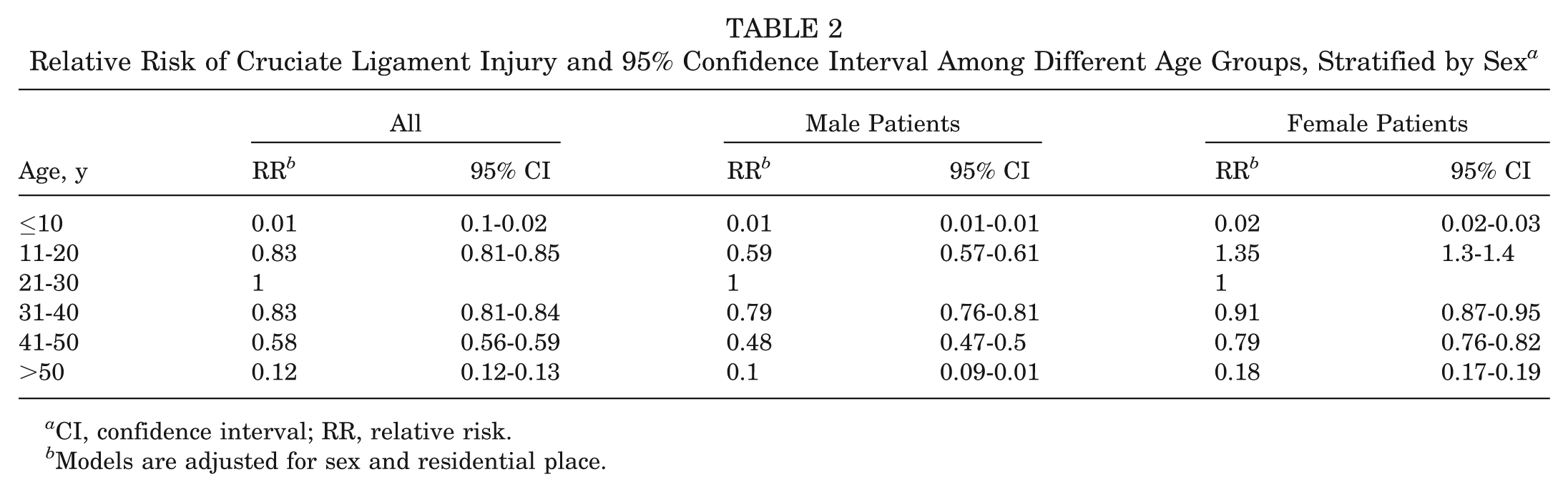
CI, confidence interval; RR, relative risk.
Models are adjusted for sex and residential place.
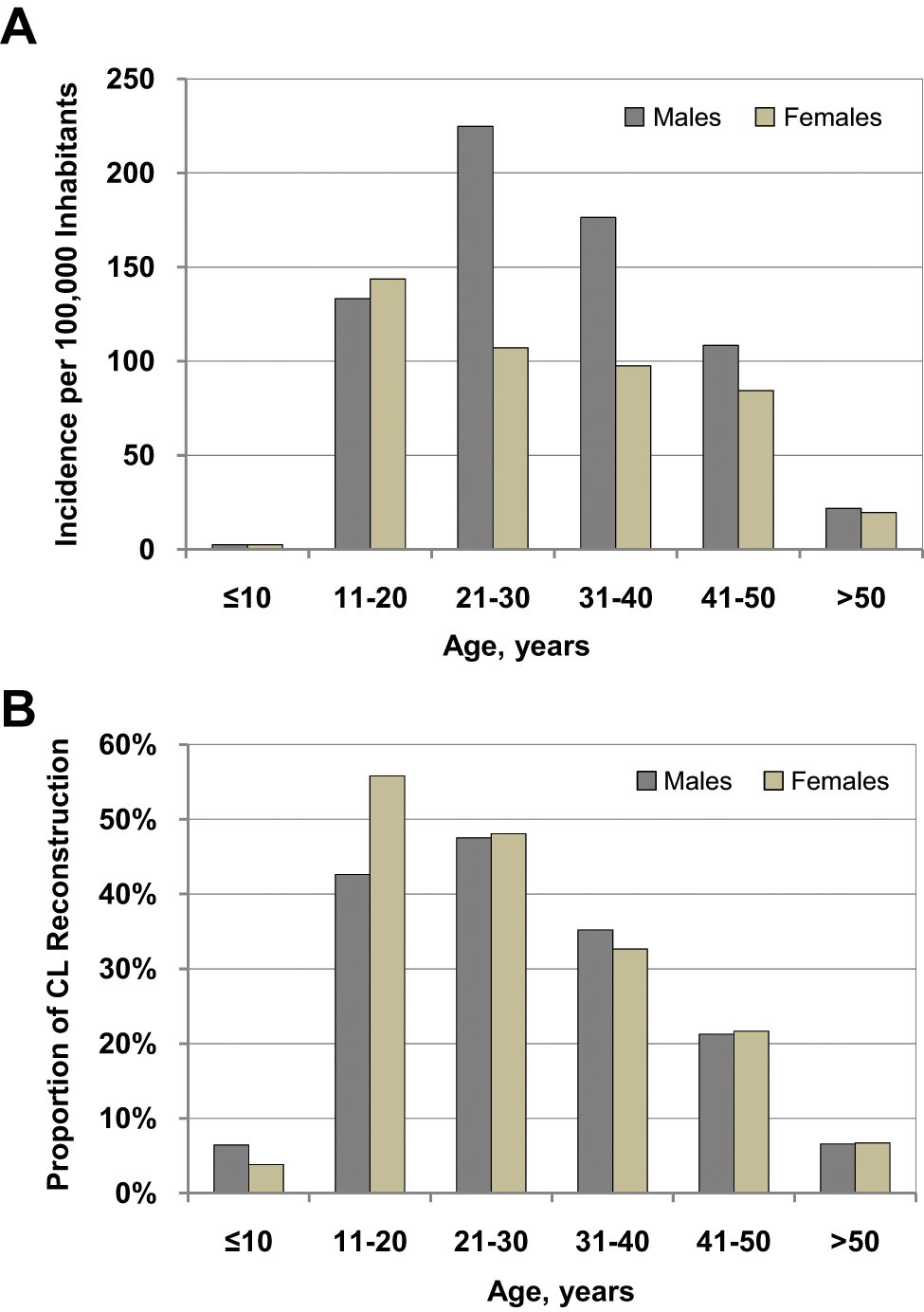
(A) Age- and sex-specific incidence of cruciate ligament (CL) injury in Sweden, 2002 to 2009. (B) Age- and sex-specific proportion of CL reconstruction in 56,659 patients with CL injury, 2002 to 2009.
There was no difference in treatment regarding surgery between sexes. Approximately 36% (95% CI, 35.3-36.2) of male patients and 37% (95% CI, 36.8-37.9) of female patients with CL injury underwent reconstructive surgery. Overall, the patients selected for surgery were younger at the first time of injury than the patients treated nonoperatively (P < .0001), with a mean (SD) age of 27 (10) years for the operated compared with 35 (14) years for the nonoperated (Figure 2B). The prevalence of CL reconstruction in patients younger than 30 years was 48% compared with 26% in patients 30 years or older at the time of injury. Mean (SD) age at time of operation was 29 (9) years for male patients and 27 (11) years for female patients.
Kaplan-Meier analysis indicated that the probability of being operated with CL reconstruction during the first 6 months after having been diagnosed with CL injury was 22% (95% CI, 21.9-22.7) for male patients and 24% (95% CI, 23.2-24.2) for female patients. The corresponding percentages were 29% (95% CI, 29.0-29.8) and 31% (95% CI, 30.6-31.6) during the first year (Figure 3). The higher probability of being operated for female patients compared with the probability for male patients was statistically significant (P < .001).
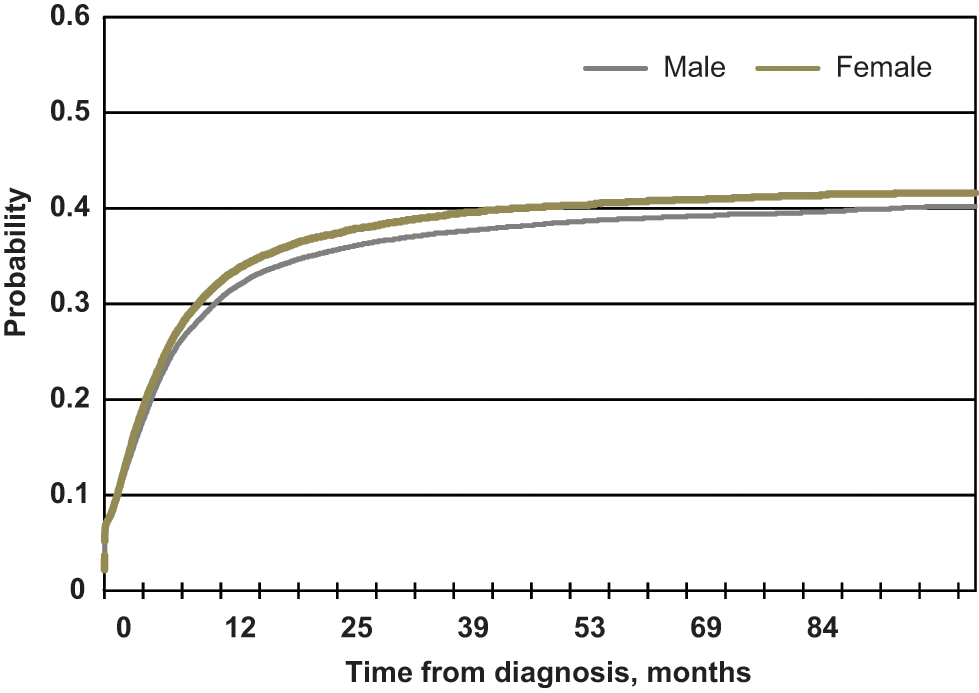
Cumulative incidence function for operation among 33,778 male and 22,881 female patients with cruciate ligament injury in Sweden, 2002 to 2009.
Discussion
This first population-based nationwide study reporting the incidence and characteristics of patients with a CL injury included 56,659 patients diagnosed with CL injury of the knee between 2002 and 2009 in Sweden. The main finding of this study was that the incidence of CL injury in the general population was 78 per 100,000 inhabitants and that 36% of the patients underwent reconstructive surgery. Male patients were more prone to injury, although female patients were injured at an earlier age. Men aged 21 to 30 years were at highest risk, with an incidence of CL injury of 200 per 100,000 inhabitants. Female patients as well as younger persons underwent surgery to a greater extent. The prevalence of surgery was not evenly distributed between different parts of Sweden.
The strength of this study on CL injuries is the large nationwide coverage allowing for analysis of the incidence of both injury and surgical reconstruction performed. Earlier studies are either not specific for CL injury 10 or based on few and local observations,8,23 making them less specific and less generalizable than this study. This study also has some limitations. The main limitation is potential misclassification because the registry information does not include information about criteria or diagnostic methods. However, any misclassification should most likely be random and therefore any relationship biased “toward the null.” Another limitation is that patients with CL injuries who never seek medical care for their injury are not included in this study. We believe, though, that most patients are likely to visit a health care provider, where it is hoped that the right diagnosis is given because CL injuries lead to a rapid hemarthrosis of the knee, precluding continuation of activity. 24 Diagnosis is made by clinical investigation, magnetic resonance imaging (MRI), or arthroscopy. 28 Sweden had a moderate accessibility of MRI machines, with 7.9 machines per 1,000,000 inhabitants in 1999. 25 Since then, there has been a dramatic increase in MRI accessibility. In 2009, around 50,000 MRI examinations of the knee were undertaken, giving an incidence of about 5.5 per 1000 inhabitants. 7 Another caveat is that bilateral injuries and the type of CL injury cannot be identified, making it impossible to differentiate between ACL injury and PCL injury. However, the ACL is injured in almost all patients with a CL injury, and PCL injuries and bilateral injuries represent a minority. Data from the Swedish Cruciate Ligament Register show that 2% of the patients underwent bilateral reconstruction. 34 Isolated PCL injuries are uncommon, accounting for an estimated 3% of all acute knee injuries. 15
Since 2001, specialist outpatient clinics have reported to the patient register. Since 2004, it has been mandatory for all health care providers to register the ICD codes for all diseases. The results of this study are coherent with the results published in the Swedish Cruciate Ligament Register. 34 This national quality register, established in 2005, is a surgical register that presently includes only patients undergoing CL reconstruction. 11 It has an estimated national coverage of 90% of all patients subjected to surgery of the CL, of which only a minority are PCLs. According to the Swedish Cruciate Ligament Register, 59% of the patients reconstructed in 2010 were male, and the group had an average age of 27 years. The incidence of CL reconstruction was 35 per 100,000 inhabitants. 34
This study reports the risks and incidence of CL injury in the general population. Many previous studies have studied smaller populations defined as being at risk (eg, sport leagues, including soccer, basketball, alpine skiing, basketball, rugby, handball, and military training).2,13,16,20,22,27,33 In these studies, female patients had an increased risk for ACL injury, ranging between 2.4 and 9.7 times greater than that for male patients. These studies are adjusted for exposure, which may explain the difference from the findings presented in this study.
Recent publications demonstrate sex differences regarding surgical outcome after CL reconstruction and also regarding concomitant joint injury such as cartilage lesions.1,30 Our results emphasize the sincere need to further investigate the effect of different treatment methods and their effect on health, recovery, economy, and society.
Regardless of treatment protocol, the end stage is often osteoarthritis.17,21 It is evident that management of CL injuries can be improved. Frobell et al 9 found that early ACL reconstruction plus structured rehabilitation was not superior to a strategy of rehabilitation with the option of delayed ACL reconstruction when needed in a normal population. There were no significant differences between the 2 treatment groups with respect to secondary outcomes. Adverse effects were common in both groups. Of the patients in this study, 39% went through surgery, which is concordant with the results presented in the current study. The nature of this study prevents comments on the comparative outcomes of surgical and nonsurgical treatment.
This is the first nationwide study describing the incidence and characteristics of ACL injury in the general population. The incidence reported in this study is significantly higher than both the results presented by Nielsen and Yde 23 (30/100,000 inhabitants) and the estimation of 80,000 yearly ACL injuries in the United States. 12 The results in this study are similar to the results presented by Frobell et al, 8 with an incidence of 81 per 100,000 inhabitants aged 10 to 64 years.
A torn CL represents one of the most common and complex injuries among young active people. Stakeholders with an interest in CL injury represent orthopaedic, sports medicine, general practitioner, and physical therapy communities; insurance companies; medical technology; and last but not least the sports industry—ranging from recreational to elite-level athletes—with optimal knee function underpinning huge financial aspects.
Even though the patients undergoing CL reconstruction in Scandinavia are nowadays thoroughly investigated, no data have hitherto been published including all patients with CL injury, treated both operatively and nonoperatively. Such baseline epidemiologic data are crucial to be able to validate and judge the generalizability of results from procedure registers.
In conclusion, this study defines the incidence of CL injury and also demonstrates sex differences, where male patients were more likely to sustain a CL injury, but female patients were injured at an earlier age. Our findings corroborate the results from registers with high quality and validity and provide information that will facilitate individualized treatment protocols. Future studies should focus on evaluation of individualized protocols, taking into consideration the factors coming from our study—in other words, that not all patients should be treated the same way.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was partly funded by the Foundation of Martin Lind and also by independent research grants at Karolinska Institutet.