
Abstract
Background:
Symptom reports play a critical role in the assessment and management of concussions. Symptoms are often conceptualized as factors comprising several related symptoms (eg, somatic factor = headache, nausea, vomiting). Previous research examining the factor structure of the 22-item Post-Concussion Symptom Scale (PCSS) has been limited to small samples and has not adequately evaluated factor loadings at both baseline and postconcussion for male and female athletes at the high school and collegiate levels.
Purpose:
To examine the factor structure of the 22-item PCSS in independent samples of high school and collegiate athletes reported at baseline and postconcussion, and to evaluate sex and age differences in the resulting baseline and postconcussion symptom factor scores.
Study Design:
Case series; Level of evidence, 4.
Methods:
Exploratory factor analytic (EFA) methods were applied to 2 separate samples of athletes who completed the PCSS at baseline (n = 30,455) and 1 to 7 days after a sport-related concussion (n = 1438). The baseline sample (mean ± standard deviation) was 15.74 ± 1.78 years, with a range of 13 to 22 years, and the postconcussion sample was 17.14 ± 2.25 years, with a range of 13 to 24 years.
Results:
A 4-factor solution accounting for 49.1% of the variance at baseline included a cognitive-sensory, sleep-arousal, vestibular-somatic, and affective factor structure. A 4-factor solution that included cognitive-fatigue-migraine, affective, somatic, and sleep was revealed for the postconcussion EFA. High school athletes reported higher baseline levels of the cognitive-sensory and vestibular-somatic symptom factors and lower levels of the sleep-arousal factor than college athletes. Female participants reported higher symptoms on all postconcussion factors than male participants.
Conclusion:
The current findings reveal different symptom factors at baseline and postinjury and several age and sex differences on the symptom factors. At postconcussion, symptoms aggregated into a global concussion factor including cognitive, fatigue, and migraine symptoms. Symptoms reported at baseline are not the same as those reported after injury. The presence of a global postconcussion symptom comprising the fatigue factor highlights the importance of physical and cognitive rest during the first week after a concussion. Although headache was the most commonly reported symptom, it was not the greatest contributor to the global postconcussion symptom factor.
The assessment and management of sport-related concussions are challenging for clinicians because the presentation of concussion symptoms varies considerably from athlete to athlete. 15 In this context, it has been recommended that a multidisciplinary approach to the injury include a clinical examination, neurocognitive testing, balance and vestibular assessments, and symptom reports. 15 Symptom self-reports obtained from concussed athletes are incorporated into most on-field concussion assessment tools (eg, Sport Concussion Assessment Tool 2 [SCAT2]) and post acute computerized neurocognitive tests (eg, Immediate Post-concussion Assessment and Cognitive Test [ImPACT], CogSport). These reports require athletes to rate (on Likert-type scales) the severity of each of approximately 20+ symptoms that they may experience after a concussion including, but not limited to, headaches, dizziness, nausea, fogginess, and sleep problems. Factor analytic statistical methods have been used by researchers to aggregate concussion symptoms into factors to better inform the clinical assessment and management of sport-related concussions.11,18,19
The use of concussion symptom factors, which comprise similar individual symptoms, is intuitive to clinicians and patients and may better inform and provide a more targeted approach to the assessment, management, and treatment of concussions, particularly for concussion symptoms that linger beyond 21 days. For example, a concussed athlete presenting predominately with cognitive symptoms (eg, difficulty concentrating, memory problems) may benefit from different management and treatment programs relative to a patient with a postinjury migraine presentation or affective presentation. Different clinical management approaches (eg, specific academic accommodations), treatment strategies (eg, neurostimulant vs preventative migraine medication), and rehabilitation plans (eg, exertional activity vs rest) may be predicated on these symptom factors. Moreover, proper establishment of concussion symptom factors may provide an appropriate foundation to research different subtypes of concussive injury and more targeted outcome studies aimed at treatment and rehabilitation. The concussion symptom factors currently in use by many clinicians are generally based upon research that has been characterized by several methodological limitations, including only healthy baseline or concussed participants, nonindependent sampling methods, and lack of consideration for potential age and sex differences.
Factor analytic methods have been applied previously to commonly used concussion symptom checklists including the Post-Concussion Symptom Scale (PCSS), 17 Head Injury Scale (HIS), 18 Graded Symptom Checklist (GSC), 19 and Rivermead Post-Concussion Symptoms Questionnaire (RPQ). 11 Principal component analysis of the 22-item PCSS in a sample of 327 concussed athletes aged 12 to 25 years within the first week of recovery revealed a 4-factor solution that included a 7-item cognitive, 3-item sleep problem (ie, more or less sleep), 4-item emotionality, and 8-item somatic factor. 17 These researchers concluded that the emergent 4 factors may reflect different subtypes of concussion.
An examination of HIS symptom reports from 279 collegiate athletes at baseline reported that theoretically derived 6-item somatic, 4-item cognitive, and 6-item neuropsychological factors provided a good fit for the 16-item HIS and an excellent fit for a modified 9-item HIS. 18 However, the researchers acknowledged that the small sample size, predominately male participants, and lack of cross-validation for the 9-item HIS in an independent sample limited their conclusions. 18 Moreover, this study examined only the presence of concussion-related symptoms (ie, yes/no) rather than the presence and severity of difficulties assessed within a Likert scale format (ie, 0-6 rating scale). A subsequent follow-up study involving a sample of 1089 high school football players at baseline addressed some of the preceding limitations; results supported a 3-factor structure for the 9-item version of the GSC that included somatic, neurobehavioral, and cognitive symptom factors. 19 Similar symptom factors have been reported for the RPQ in a sample of mild-to-moderate traumatic brain injury (TBI) patients. 20 However, the findings using the GSC 19 were limited by age, sport, and sex, as the study included only collegiate male football players. Additionally, these results do not apply to postconcussion symptoms, as all symptom reports used in the factor analysis came from a baseline sample. Surprisingly, none of the previous factor analytic studies has examined sex and age in regard to symptom factors. Also, the PCSS study 17 only examined the symptom factor structure within a concussed sample.
The research examining sex and age differences for both baseline and postconcussion symptom reports has focused primarily on total symptom scores and group differences for individual symptoms. Some researchers have reported a greater number of symptoms at baseline for female patients compared with male patients, 7 whereas others have reported that baseline symptom reports did not differ between male and female patients. 6 Sex differences seem to be more consistent and pronounced after concussions, as female athletes consistently report greater increases in symptoms after concussions compared with male athletes.3,46 With regard to age, researchers have reported no significant differences on baseline symptom reports between high school or collegiate athletes. 13 Considering the prolonged neurocognitive recovery times reported in high school athletes compared with collegiate athletes, 8 an examination of potential age differences in postconcussion symptom reporting is warranted.
In summary, previous factor analytic studies of sport-related concussion symptoms are characterized by several limiting factors including baseline-only or postconcussion-only samples, using baseline symptom reports to derive factor structures for postconcussion samples and nonindependent sampling methods. Additionally, previous factor analytic research has included aggregated age groups and has not compared symptom factors for high school and collegiate athletes separately. Also, there are no published comparisons of baseline and postconcussion symptom factor scores for male patients and female patients. Therefore, the primary purpose of the current study was to examine, using exploratory factor analyses (EFA), the factor structure of the 22-item PCSS in very large independent samples of baseline and postconcussion high school and collegiate athletes separately. A secondary purpose of the study was to examine sex and age differences in the resulting baseline and postconcussion symptom factor scores.
Materials and Methods
Participants
Participants comprised 2 independent samples of athletes: (1) baseline: those who completed the symptom report during preseason and (2) postconcussion: those who completed a symptom report during postconcussive assessments within 1 to 7 days after injury.
Baseline Participants
Baseline participants were from a prospective cohort sample of 30,455 healthy athletes (27,008 high school, 3447 collegiate; 14,295 female, 16,160 male) from across the United States over a 2-year period (2009-2011). Sports with greater than 1% representation in the baseline sample are presented in Table 1. The mean (± standard deviation) age for participants in the baseline sample was 15.74 ± 1.78 years, with a range of 13 to 22 years.
Sport Representation in the Baseline and Postconcussion Samples a
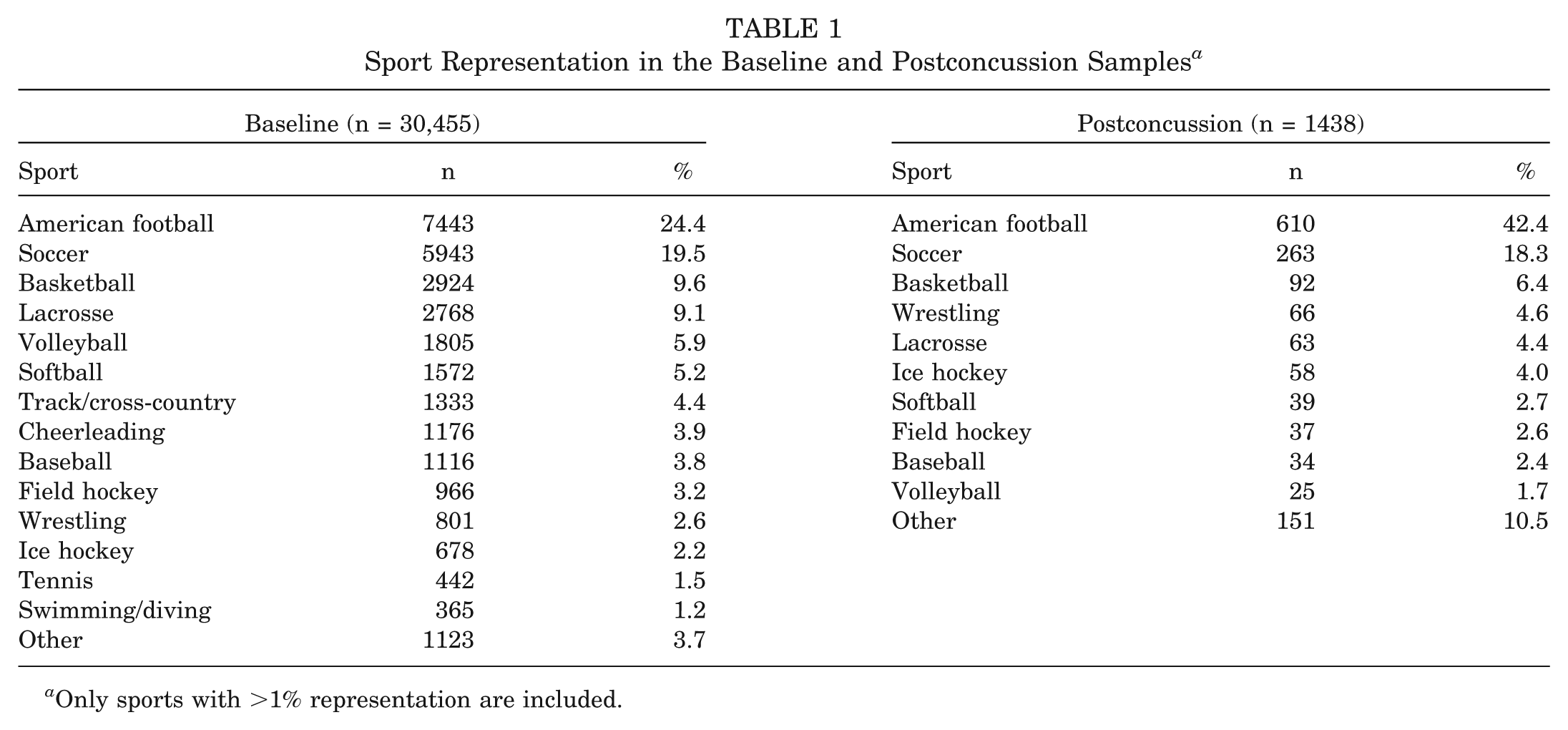
Only sports with >1% representation are included.
Postconcussion Participants
Postconcussion participants were from a prospective cohort sample of 1438 athletes (944 high school, 494 collegiate; 477 female, 961 male) from across the United States over a 5-year period (2006-2011). Refer to Table 1 for information regarding the sport representation for the postconcussion sample. All concussed participants were identified based upon the presence of on-field signs (eg, loss of consciousness, posttraumatic amnesia) and symptoms (eg, dizziness, headache) as determined by certified athletic trainers or other sports medicine staff (eg, physician). Athletes’ concussions were confirmed by positive symptom reports and/or neurocognitive test findings. The average age in the postconcussion sample was 17.14 ± 2.25 years, with a range of 13 to 24 years. All athletes completed symptom reports within 1 to 7 days after their concussion, with an average of 2.62 ± 1.71 days after injury.
Concussion Symptoms
Concussion-related symptoms were self-reported by athletes using the computerized version of the 22-item PCSS. 17 The PCSS is part of the ImPACT 13 computerized test program used to assess neurocognitive performance and concussion symptoms. Athletes are instructed to complete this symptom scale before administration of the neurocognitive testing battery. The 22-item scale includes headache, nausea, vomiting, balance problems, dizziness, fatigue, trouble falling asleep, sleeping more than usual, sleeping less than usual, drowsiness, sensitivity to light, sensitivity to noise, irritability, sadness, nervousness, feeling more emotional, numbness or tingling, feeling slowed down, feeling mentally “foggy,” difficulty concentrating, difficulty remembering, and visual problems. The PCSS uses a Likert-type scale, ranging from 0 to 6, with 0 indicating no difficulty with the outlined symptom and ratings of 1 to 6 representing mild-to-severe difficulty with the symptom. The reliability and validity of the PCSS are well documented. 14
Procedures
The current study was approved by the university institutional review board using an exempt, deidentified, existing medical records protocol. Ideally, and as recommended for best practice, athletes reported in groups of 10 to 15 at a time to their own institution’s computer laboratory, where they were informed about the standardized test procedures and completed the baseline PCSS as part of the computerized neurocognitive test battery (ie, ImPACT). In practice, the researchers acknowledge that variations in this recommended best practice for completing the PCSS at baseline testing may have occurred (eg, more than 15 students at a session, testing individually). The symptom reports required approximately 5 minutes to complete. As recommended for best practice, postconcussion PCSS reports were completed individually by participants in a quiet, private setting (eg, examination room, athletic training room office) within 1 to 7 days after injury. Again, although qualitative data were not available, some postconcussion tests may have been completed in small groups of injured athletes or in locations where distractions may have been present. All postconcussion PCSS reports were completed within 1 to 7 days after injury.
Data Analysis
Descriptive statistics including mean, standard deviation, skewness, and kurtosis for the PCSS items in baseline and postconcussion samples by age and sex were conducted. Two separate EFAs using principal component analyses for baseline and postconcussion samples were conducted. Varimax rotation with Kaiser normalization, Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy, eigenvalues, and scree plot data were employed to assist with interpretation of the factors and structure. Specifically, the sampling adequacy should have KMOs above .850, while factors should have eigenvalues greater than 1.0, and factors that occurred before the curve in the scree plot levels off should be included in the factor model. As per previous research,5,23 items were retained in the factor models on the basis of having a primary factor loading of .5 or above on 1 factor, which is considered to be a strong loading item. In addition, any item that cross-loaded (>.4) on another item was retained for further analysis only if the main loading was above .6 and the difference between the main and highest cross-loading was +.2 or greater. Items not meeting these criteria were excluded from the factors used in the subsequent analyses. Single-item factors were also excluded. Given that this analysis was exploratory, factors with only 2 items were retained if the items met the strong loading criteria above. A series of 2 (age) × 2 (sex) multivariate analyses of variance (MANOVAs) with Bonferroni correction for multiple comparisons were conducted for the baseline and postconcussion factor structures. All analyses were conducted using the Statistical Package for the Social Sciences, version 19.0 (IBM Inc, Armonk, New York). Statistical significance for all tests was set at P < .05.
Results
Descriptive Data
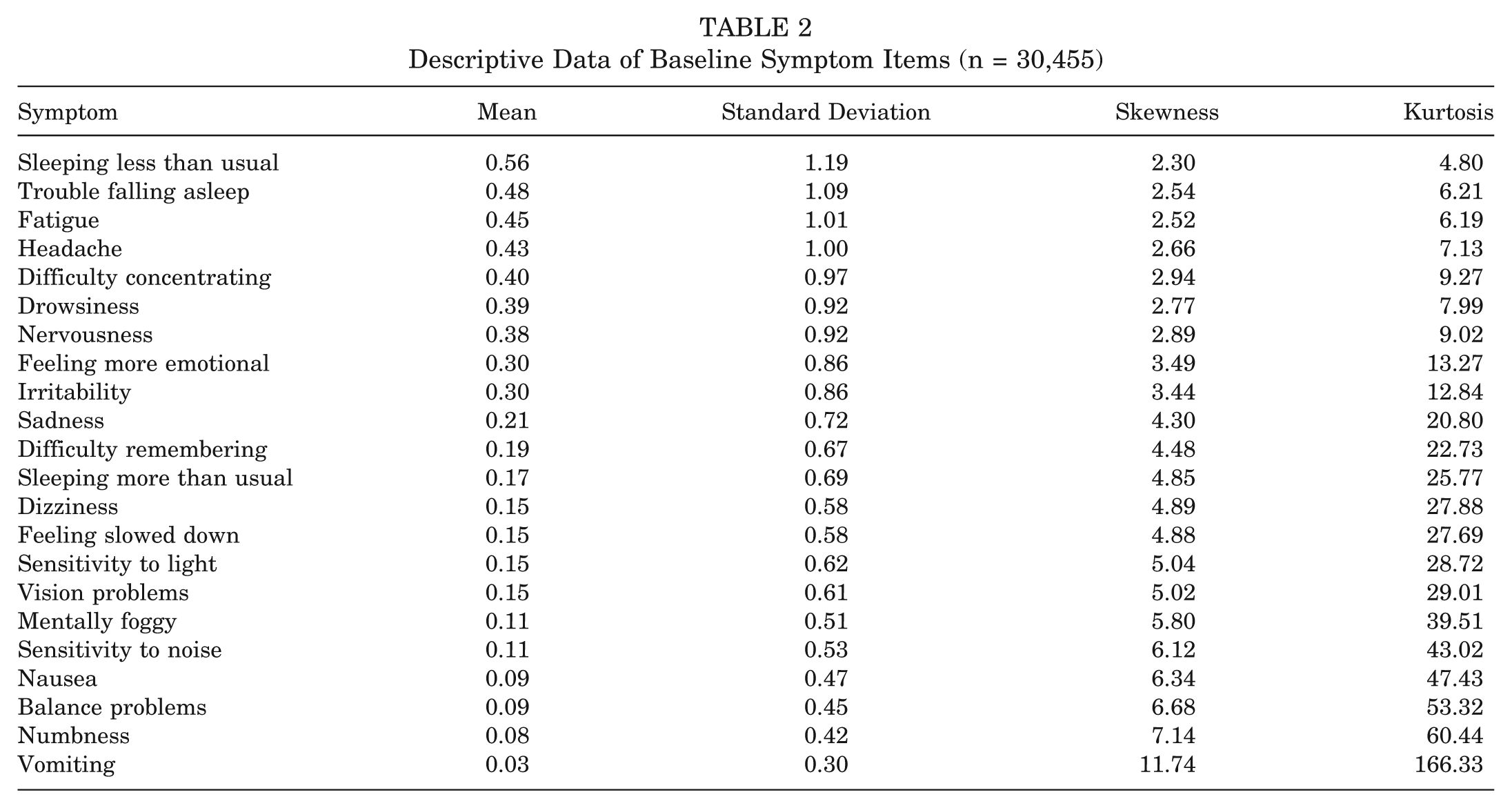
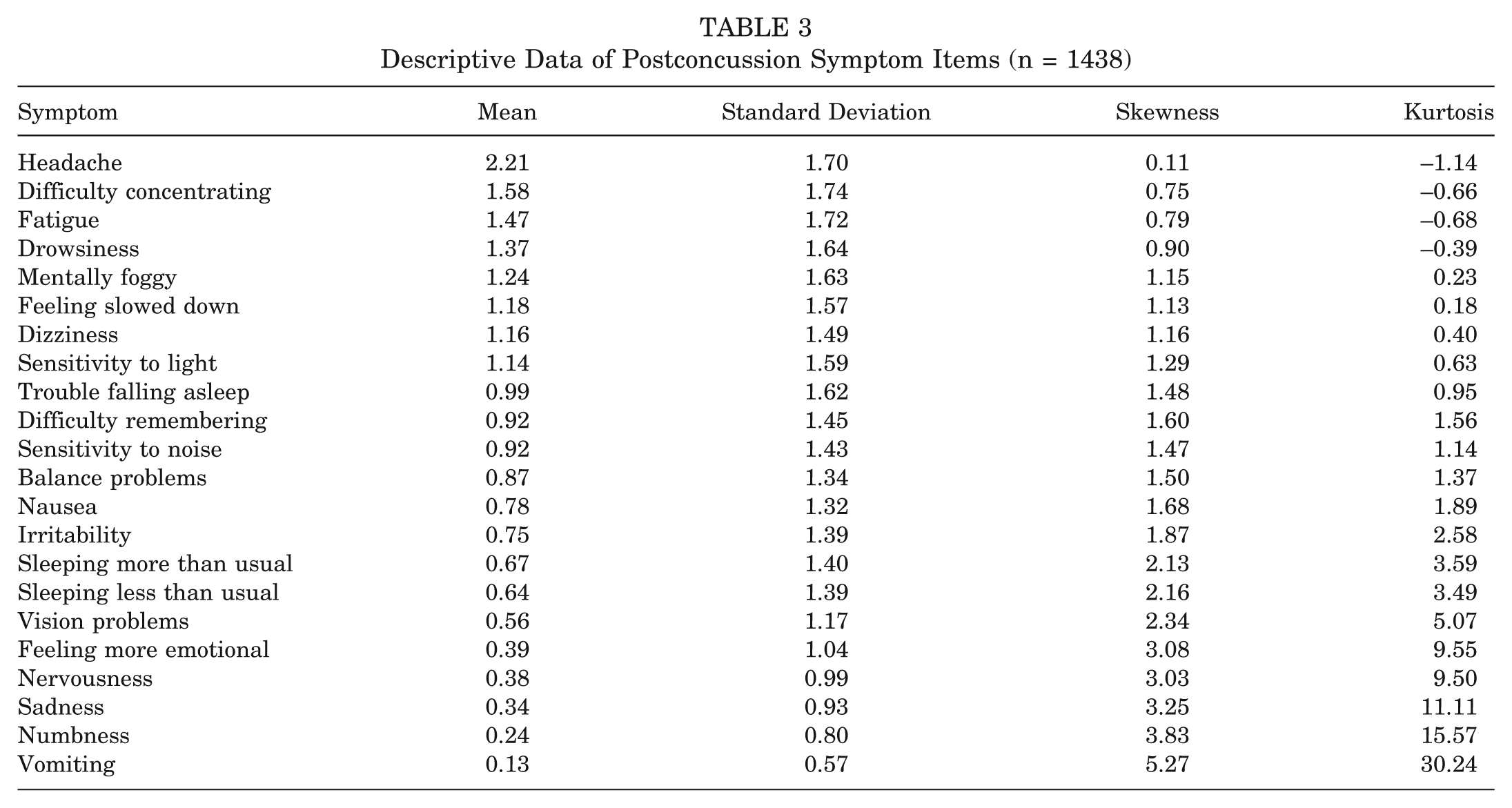
The mean, standard deviation, skewness, and kurtosis for the baseline and postconcussion samples are reported in Tables 2 and 3. In both the baseline and postconcussion samples, the full range of responses from 0 (not at all) to 6 (severe) was used for each symptom item. Overall, the reported symptoms at baseline were low, with means ranging from .03 ± .30 for vomiting to .56 ± 1.19 for sleeping less than usual. Postconcussion symptoms were higher, ranging from .13 ± .57 for vomiting to 2.21 ± 1.70 for headache. As reported previously, 18 the baseline samples were both skewed and kurtosed (Table 2). The postconcussion data were less skewed and kurtosed than the baseline data (Table 3).
Descriptive Data of Baseline Symptom Items (n = 30,455)
Descriptive Data of Postconcussion Symptom Items (n = 1438)
Baseline EFA
The results from the EFA for baseline data supported a 4-factor solution, named for the predominating symptoms within each factor, that accounted for 49.1% of the variance with a KMO measure of sampling adequacy of .927. The 4 factors included 20 of the original 22 items and consisted of (1) cognitive-sensory: 31.2% of the variance, eigenvalue = 6.86, 7 items related primarily to cognitive symptoms (eg, difficulty remembering) and sensory changes (eg, vision problems); (2) sleep-arousal: 7.3% of the variance, eigenvalue = 1.60, 4 items related to rest (eg, sleeping less than usual) and energy (eg, fatigue); (3) vestibular-somatic: 5.6% of the variance, eigenvalue = 1.23, 5 items related to corporeal symptoms (eg, nausea) and equilibrium (eg, dizziness); and (4) affective: 5.1% of the variance, eigenvalue = 1.12, 4 items related to emotions (eg, feeling more emotional). See Table 4 for the factor structure and loadings. The following symptoms, sleeping more and numbness, were excluded from the analysis because of cross-loadings (>.4) in 2 or more factors or low (<.5) loadings.
Baseline Symptom Factors and Item Loadings (λ) (n = 30,455)
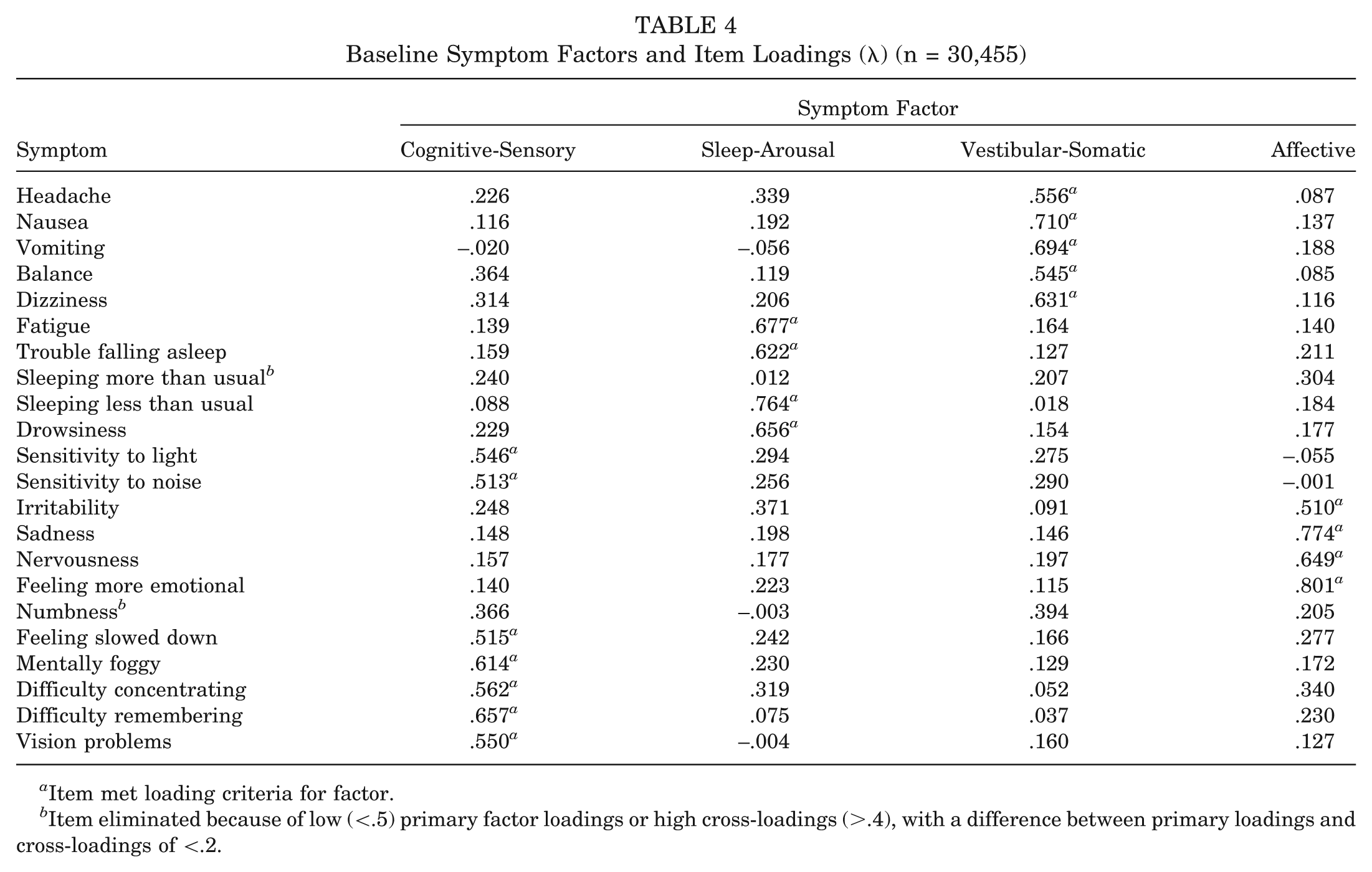
Item met loading criteria for factor.
Item eliminated because of low (<.5) primary factor loadings or high cross-loadings (>.4), with a difference between primary loadings and cross-loadings of <.2.
Postconcussion EFA
The results from the EFA for the postconcussion sample also supported a 4-factor solution that accounted for 58.3% of the variance with a KMO measure of sampling adequacy of .939. The factor loading pattern differed in several notable ways. Specifically, cognition-based symptoms (eg, difficulty concentrating) were previously loaded with sensory-based symptoms; however, with the postconcussion data, cognitive symptoms loaded with fatigue and arousal symptoms, vestibular symptoms (eg, dizziness), as well as migraine-related symptoms (eg, headache). Affective symptoms continued to load together with the exception of irritability, which had a high cross-loading. The other 2 factors included only 2 symptoms each. The altered factor loadings in concussed athletes resulted in different nomenclature, again reflective of the predominant symptoms or symptom categories in a given factor. The 4 postconcussion factors included 17 of the original 22 items and consisted of (1) cognitive-fatigue-migraine: 40.0% of the variance, 10 items; (2) affective: 6.83% of the variance, 4 items; (3) somatic: 6.42% of the variance, 2 items; and (4) sleep-arousal: 5.04% of the variance, eigenvalue = 1.11, 2 items. See Table 5 for the factor structure and loadings. The following symptoms, nausea, balance problems, sleeping more than usual, irritability, and vision problems, were excluded from the analysis because of low (<.5) primary factor loadings or high cross-loadings (>.4), with a difference between primary loadings and cross-loadings of <.2.
Postconcussion Symptom Factors and Item Loadings (λ) (n = 1438)
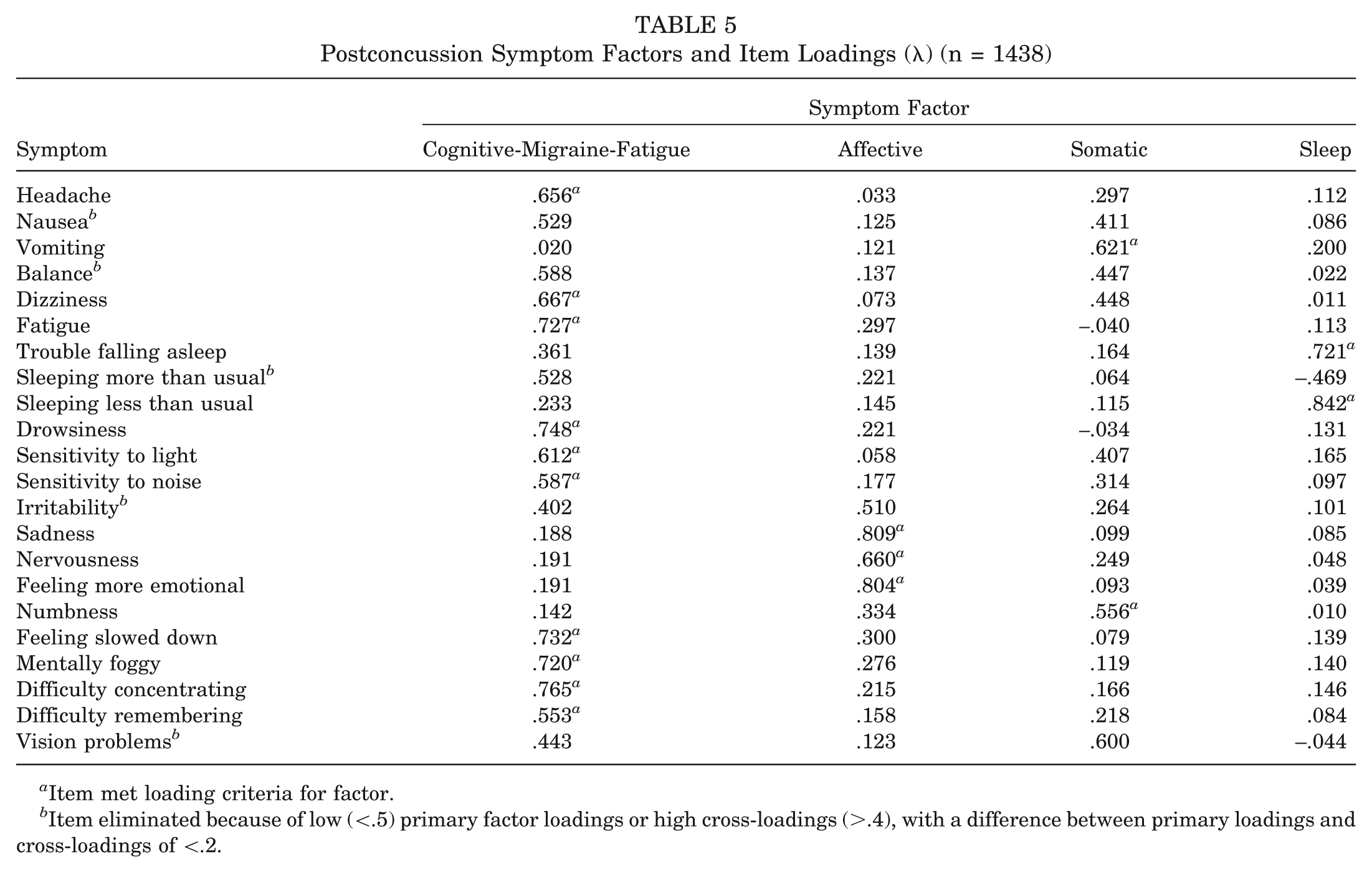
Item met loading criteria for factor.
Item eliminated because of low (<.5) primary factor loadings or high cross-loadings (>.4), with a difference between primary loadings and cross-loadings of <.2.
Age and Sex Differences in Baseline Symptom Factors
The results of 2 (age) × 2 (sex) MANOVAs with Bonferroni correction comparing scores on the 4 baseline factors (cognitive-sensory, sleep-arousal, vestibular-somatic, affective) supported main effects for age (Wilks λ = .99, F4, 30,448 = 22.36, P = .001, η2 = .01) and sex (Wilks λ = .99, F4, 30,448 = 93.373, P = .001, η2 = .01). Specifically, high school athletes reported higher baseline levels of cognitive-sensory and vestibular-somatic symptom factors but lower levels of the sleep-arousal symptom factor than college athletes (Table 6). There were no age differences for the affective symptom factor. With regard to sex, female athletes reported higher levels of the cognitive-sensory, sleep-arousal, vestibular-headache, and affective symptom factors than male athletes (Table 6). The interaction between age and sex was not significant (Wilks λ = 1.00, F4, 30,448 = 1.75, P = .14, η2 = .001).
Means and Standard Deviations of Baseline Symptom Factor Scores by Age and Sex
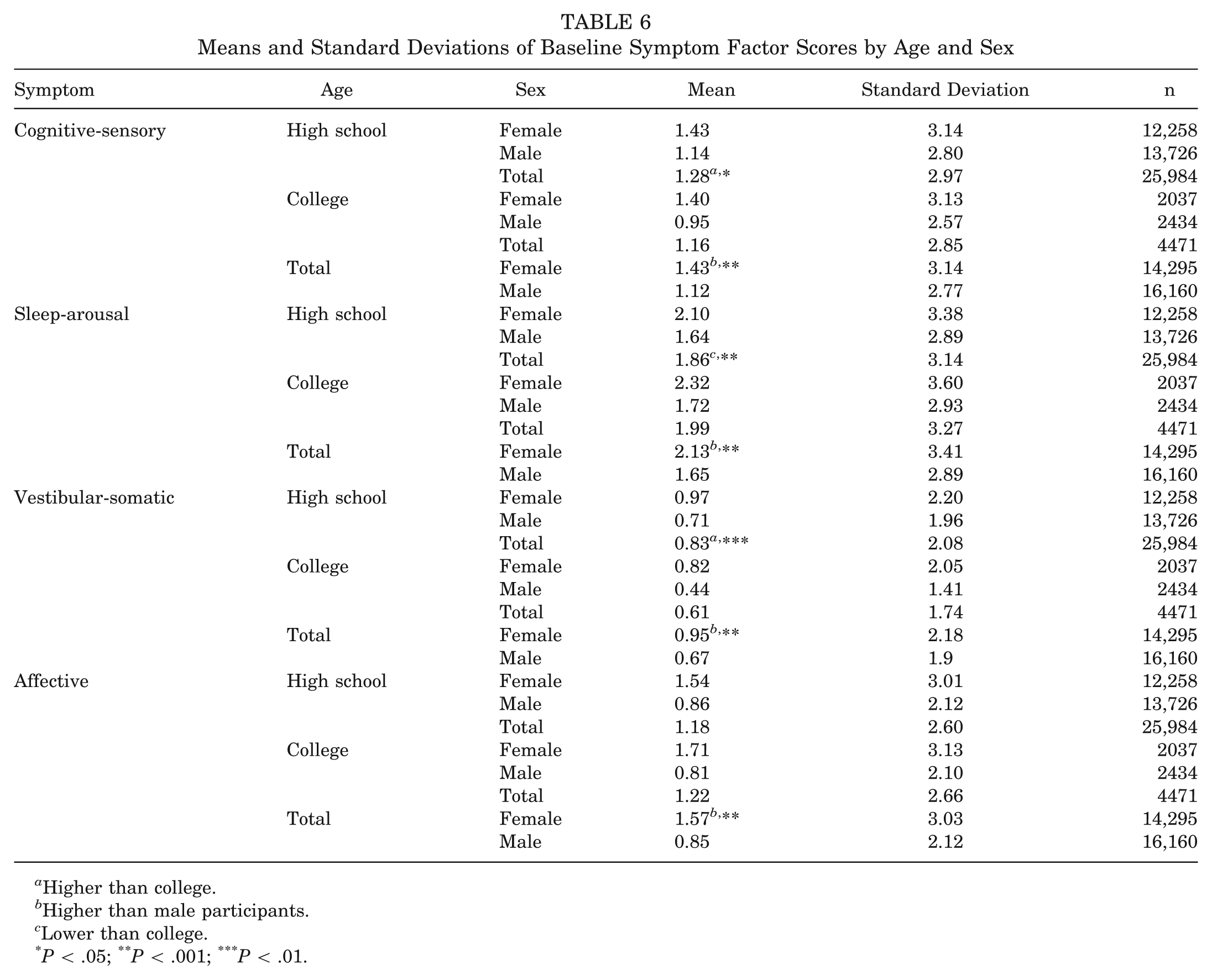
Higher than college.
Higher than male participants.
Lower than college.
P < .05; **P < .001; ***P < .01.
Age and Sex Differences in Postconcussion Symptom Factors
The results of 2 (age) × 2 (sex) MANOVAs with Bonferroni correction for multiple comparisons comparing scores on the 4 postconcussion factors (cognitive-migraine-fatigue, affective, somatic, sleep) supported main effects for age (Wilks λ = .99, F4,1429 = 3.53, P = .007, η2 = .01) and sex (Wilks λ = .99, F4,1429 = 7.09, P = .007, η2 = .02). Specifically, high school athletes reported lower postconcussion levels of the sleep symptom factor than college athletes (Table 7). There were no age differences for the cognitive-migraine-fatigue, affective, or somatic symptom factors. With regard to sex, female athletes reported higher levels of the affective symptom factor than male athletes (Table 7). There were no age differences for the cognitive-migraine-fatigue, somatic, or sleep symptom factors. The interaction between age and sex was not significant (Wilks λ = .99, F4,1429 = 2.14, P = .074, η2 = .001).
Means and Standard Deviations of Postconcussion Symptom Factor Scores by Age and Sex
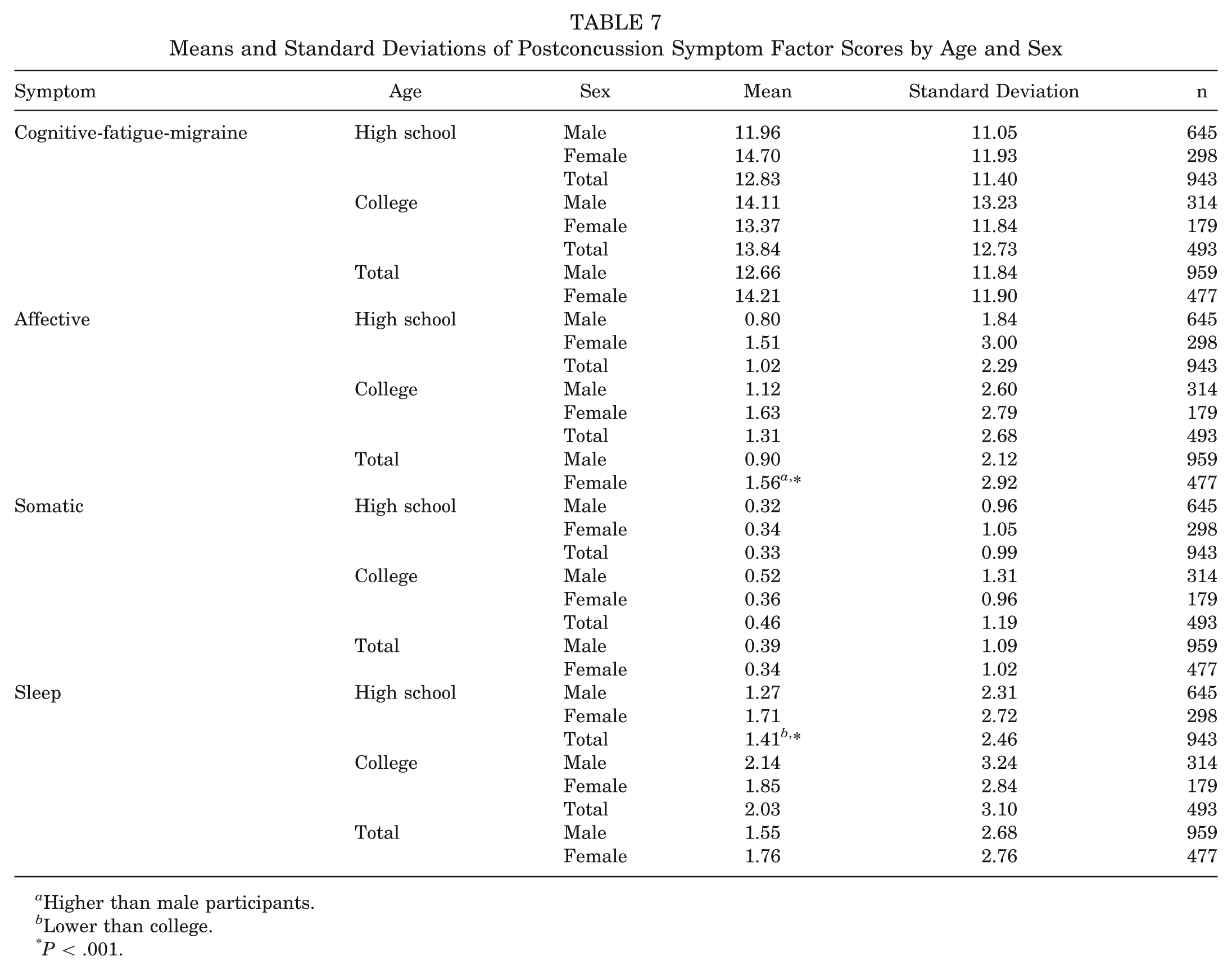
Higher than male participants.
Lower than college.
P < .001.
Discussion
The primary purpose of the study was to explore the symptom factor structures in independent baseline and postconcussion samples of athletes. The results supported a 4-factor structure for both the baseline and postconcussion samples, although several differences between baseline and postconcussion factor structures and items were revealed. The baseline factors (in order of contribution to the overall variance) included (1) cognitive-sensory (eg, sensitivity to light, difficulty concentrating), (2) sleep-arousal (eg, drowsiness, sleeping less than usual), (3) vestibular-somatic (eg, headache, dizziness), and (4) affective (sadness, nervousness), whereas the postconcussion factors included (1) cognitive-fatigue-migraine (eg, headache, difficulty concentrating, fatigue, dizziness), (2) affective (sadness, nervousness), (3) somatic (eg, nausea, numbness), and (4) sleep (eg, trouble sleeping, sleeping less than usual).
Several items from the PCSS did not meet the loading criteria for the study. Specifically, at baseline, only 2 items (sleeping more than usual, numbness) did not meet the loading criteria. In contrast, during the postconcussion state, 5 items (nausea, balance problems, sleeping more than usual, irritability, and vision problems) did not meet the loading criteria. Each of these postconcussion symptoms loaded on the cognitive-fatigue-migraine factor but had strong cross-loadings on other factors. This finding suggests that the cognitive-fatigue-migraine factor may reflect a global “concussion” factor, which includes an amalgamation of difficulties with fatigue, cognitive concerns, and posttraumatic migraine-type symptoms. However, it is important to note that there may be a temporal component to the presentation of symptoms after concussion. As the current EFA was conducted on a sample during the more acute/subacute phase of injury (within 7 days), the postconcussion factor structure presented here may only apply during this time period. This notion is supported, in part, by previous research that reported a different 4-factor model at 1+ week after injury. 17 Hence, future research should examine if the current symptom factor structure is supported during the more chronic phases of concussive injury.
Given that the pathophysiology of concussions involves a metabolic crisis in which there is a mismatch in energy demand and availability in the brain, 9 it is not surprising that our findings supported a fatigue component to the migraine-cognitive symptom cluster. During the less acute phase of injury, symptom clusters may become more defined, reflecting specific subtypes of the injury. Future research should examine this hypothesis.
Researchers have reported that balance problems and dizziness (ie, vestibular-related symptoms) typically recover within 1 to 3 days,2,10 whereas other researchers suggest that these symptoms may persist for several weeks after injury. 22 Neither balance problems nor dizziness loaded onto any factor in the postconcussion analyses. This finding does not suggest that these symptoms were absent at postconcussion. Rather, both dizziness and balance problems loaded across several factors at postconcussion and therefore could not be delineated into any single factor. Future research may delineate whether a factor analysis involving patients further removed from injury (ie, chronic postinjury phase) might establish vestibular-related symptoms as a stand-alone factor or as a part of another factor (eg, migraine).
The secondary purpose of the study was to examine age and sex differences in the resulting baseline and postconcussion factor scores. As expected, female athletes endorsed more concussion symptoms at baseline than male athletes. In fact, female athletes had significantly greater concussion symptoms than male athletes on all 4 symptom clusters, which is similar to findings in the literature in which 12 of the 22 postconcussion symptoms were higher in female athletes compared with male athletes at baseline. 7 With respect to postconcussion symptoms, the affective cluster, in isolation, was significantly higher for female concussed athletes than male concussed athletes. Specifically, the affective cluster included sadness, nervousness, and feeling more emotional. Although previous researchers reported higher concussion symptoms in female concussed athletes than male concussed athletes,3,6 none of these authors reported higher symptoms in nervousness, sadness, and feeling more emotional in female athletes. Moreover, researchers 5 have reported higher levels of sadness and vomiting in male concussed athletes than female concussed athletes. However, these differences may be because of the small sample size (n = 79) and inclusion of only collegiate athletes. An exploration of the possible reasons that female athletes tended to “load” higher on the affective symptom cluster was beyond the scope of this article. Possibilities to be explored in future work include personality differences, socialization differences, and other constitutional factors. As well, any contribution of personality and estrogen to the current findings would be speculative, given the lack of support on this relationship in the literature. With regard to age, high school athletes reported greater baseline symptoms for cognitive-sensory and vestibular-somatic symptom factors than collegiate athletes but lower baseline symptoms on the sleep-arousal symptom factor than collegiate athletes. Other researchers have also reported that headaches were the most highly endorsed symptom in healthy adolescents. 21 The increased presentation of headaches in adolescents at baseline may influence the increased presentation of headaches after brain injury as suggested in a recent study. 1 As such, clinicians should be aware of baseline levels of headaches. In regard to collegiate athletes reporting a higher level of sleep-arousal at baseline than high school athletes, this is consistent with published data 12 that suggested that healthy adults had the highest frequency of fatigue and difficulty sleeping on the PCSS. A possible explanation may be because of collegiate athletes having greater academic demands (eg, midterms, papers) combined with an intense athletic schedule (eg, 20 hours of practice/games, travel), resulting in less time for sleep. Despite the fact that this study did not find a difference in sleep symptoms at baseline between high school and collegiate athletes, age differences were supported for the sleep cluster at postconcussion. Specifically, high school concussed athletes reported less sleep symptoms than collegiate concussed athletes. The increased stressors experienced by collegiate athletes described previously likely contributed to this finding.
Limitations
The current study is not without its limitations. As with any factor analysis of symptom reports, the researchers assumed that participants responded honestly and accurately when completing the baseline and postconcussion symptom reports. From a methodological perspective, the current study did not confirm the proposed exploratory factor structure in an independent sample. The study sample was delimited to athletes aged 13 to 24 years, and therefore, the results cannot be generalized to athletes outside of this age range. Additionally, the current study examined samples at baseline and 1 to 7 days after concussion. As such, the proposed factor structures may not apply to patients still experiencing symptoms outside of the 1- to 7-day acute/subacute time period. Factor structures may differ at different recovery time points. The authors selected the acute/subacute time period to provide a “clinical snapshot” of symptom structures reported to a wide range of practitioners (eg, physicians, athletic trainers, neuropsychologists, school nurses) at a critical point in recovery.
Implications for the Practitioner
From a clinical perspective, the factor analysis in the current study demonstrates that symptoms that tend to be comorbid at baseline do not necessarily group themselves together in a similar manner after concussion. That is to say, symptoms endorsed at baseline are not necessarily the same symptoms that will be endorsed after injury. It is important for clinicians to understand which symptoms are being endorsed at baseline and how they might influence postinjury symptom scores and injury management. For example, if an athlete endorsed difficulty concentrating at baseline, it is important to understand if this was caused by a general (ie, trait) deficiency in concentration or if endorsement of this symptom was more temporally related to an event (ie, state) such as being distracted about an upcoming game. This does not negate the value of baseline symptom reporting, especially from a neurocognitive standpoint, but it does mean that clinicians must do their due diligence in understanding endorsed symptoms, be it at baseline or postinjury. What seems to be most apparent based on the current EFA is that the postconcussion symptoms, with the exception of the affective factor, seem to fall under a more general concussion factor that is composed of several different symptom types including fatigue, cognitive, migraine-related, and vestibular-based symptoms. As this analysis was conducted within 7 days of injury, it is not surprising to see a “global” presentation of symptoms, given the broader occurrence of symptoms during this more acute/subacute phase of injury. Within this context, it is interesting to note that in the current study during the acute/subacute phase of recovery from concussion, fatigue, migraine-type symptoms, vestibular concerns, and cognitive issues occurred in combination. The presence of the fatigue component in this symptom presentation highlights the need for physical and cognitive rest during this period of recovery as reported in a recent study. 16 Future research should explore the present factor structure during the more chronic phases of recovery from concussion. If symptom presentations become better defined and delineated (eg, vestibular, migraine, cognitive) over time (ie, 2 to 3 weeks after trauma), symptom factors might help inform more targeted and focused treatment plans. We believe that a critical next step for researchers is to build upon our current findings and delineate among acute, subacute, and chronic symptom factor structures.
Noteworthy for the clinician, the most consistently reported symptom (headache) is not among the largest contributors to the cognitive-fatigue-migraine factor within the current EFA. In fact, headache loads lower on the cognitive-fatigue-migraine factor than difficulty concentrating, drowsiness, feeling slowed down, fatigue, mental fogginess, and dizziness. This does not mean that headaches are less important in terms of symptom contribution. It simply means that headaches are not the greatest contributor to postconcussion symptoms. For the clinician, this means that assessing the presence or severity of headaches is not the only part of clinical management, nor is it even necessarily the most important. The current results would suggest that the loadings of other symptoms (ie, difficulty concentrating, drowsiness) are deserving of clinical attention and appropriate intervention. It is also important for the clinician to consider when concussions occur and how postconcussion headaches might differ from headaches prior to the concussion. Also, the fact that 2 cognitive symptoms (difficulty concentrating, feeling slowed down) are among the largest postconcussion contributors to the cognitive-fatigue-migraine factor underscores the importance of neurocognitive testing. Even though self-reported symptoms form a major part of how concussions are clinically managed, the objectivity provided by neuropsychological measures is essential to making good management decisions during recovery and appropriate return to play decisions in conjunction with self-report symptoms.
Conclusion
Several conclusions can be drawn from the current analyses. Symptoms that cluster together at baseline do not necessarily do so after a concussive injury. In other words, just because a patient tends to present with a certain symptom profile at baseline, his or her postinjury presentation is likely to vary considerably after a concussion. The types of symptoms reported by athletes at baseline vary by age and sex. Specifically, collegiate athletes were more likely to endorse fatigue and sleep-related symptoms at baseline, whereas female athletes were more likely to endorse more symptoms overall at baseline and more affective-related symptoms postinjury. The postconcussion global symptom cluster that emerged in the current study suggests a more general concussion factor rather than a specific “subtype” of concussion in the first week of injury, which is consistent with most clinicians’ experiences in the acute and subacute postinjury phases. This general factor, termed the cognitive-fatigue-migraine factor in the current study, comprises several different types (ie, cognitive: difficulty concentrating; migraine: headache; and fatigue). The presence of the cognitive-fatigue-migraine factor within the first week of injury supports the implementation of physical and cognitive rest during this more generalized period of injury. We speculate that the general postconcussion factor may comprise different symptom clusters that will vary greatly in their presentation after the first week of injury. Investigation of the current factor structure at more chronic (ie, 2-4 weeks, 1+ months) postinjury time points is warranted.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.