
Abstract
Background:
Debate exists on whether hip labral tears should be surgically repaired, partially resected, or reconstructed. Furthermore, limited data exist regarding the fluid seal properties of hip labrum repair and/or reconstruction with iliotibial band autograft when compared with the labrum-intact condition.
Hypothesis/Purpose:
The purpose of this study was to investigate the fluid seal properties of hip labral repair and reconstruction techniques. We hypothesized that hip labral repair preserves the acetabular labral fluid seal greater than labral tear, partial-resection, and reconstruction conditions.
Study Design:
Controlled laboratory study.
Methods:
Six human cadaveric hemipelvises were dissected of all soft tissue, leaving the hip capsule intact. Fluid efflux was measured under 5 conditions using a custom fluid infusion device: (1) hip labrum intact, (2) labral tear, (3) labral repair with suture anchors, (4) partial labral resection, and (5) labral reconstruction using ipsilateral iliotibial band autograft. Joint fluid expression was measured as flow rate under 3 different pressure settings (2, 3, and 4 psi). Statistical differences between conditions were assessed using 2-way, repeated-measures analysis of variance. The Student-Newman-Keuls (SNK) multiple comparison test was used to determine differences between levels.
Results:
There was a significant increase in fluid efflux with a simulated labral tear (0.54 ± 0.3 mL/sec) when compared with the intact hip labrum condition (0.006 ± 0.008 mL/sec, P < .05). The labrum-repaired condition (0.21 ± 0.2 mL/sec) demonstrated significantly less fluid efflux when compared with the labral-tear condition. Hip labral repair significantly prevented greater fluid efflux when compared with partial labral resection (0.60 ± 0.4 mL/sec) and reconstruction with iliotibial band autograft (0.54 ± 0.3 mL/sec; P < .05). Labral repair did not preserve fluid efflux as effectively as in the labrum-intact condition (0.21 ± 0.2 > 0.006 ± 0.008 mL/sec; P < .05). There was no difference observed in fluid efflux between the labral reconstruction, tear, or resection conditions (P > .05).
Conclusion:
In this human cadaveric model, hip labral repair outperforms partial labral resection and reconstruction in preserving the joint fluid seal; however labral repair does not restore fluid seal characteristics as effectively as in the labrum-intact condition.
Clinical Relevance:
Further prospective studies are needed to determine whether hip labral repair outperforms partial labral resection and/or reconstruction in clinical practice.
The hip labrum is an important contributor to hip joint stability and articular cartilage health. 8 It has been hypothesized that hip labral tears place the hip at risk for the development of osteoarthritis, presumably via disruption of the labrum joint “fluid seal effect.” The “fluid seal” provided by the labrum prevents efflux of synovial fluid from the central compartment, thus protecting the femoral and acetabular articular cartilage surfaces from degeneration as a result of first, preservation of nutrition to chondrocytes via diffusion and second, by affecting contact stresses via hydrostatic fluid distribution.8-10 Labral preservation and reconstruction has been favored by some surgeons over partial labral resection for the treatment of labral tears with or without femoroacetabular impingement.14,18,19 Despite this increasing trend and reported favorable clinical results, the “fluid seal” characteristics of hip labral repair and reconstruction techniques have not been well studied. Thus, the goal of this study was to investigate the fluid efflux characteristics of current hip labral repair and reconstruction techniques when compared with the labrum-intact, -tear, and partially resected conditions. We hypothesized that labral repair preserves the acetabular labrum fluid seal more effectively than the labral tear, partially resected, and reconstructed conditions.
Methods
Six fresh-frozen, unpaired human hemipelvises were stored in an airtight bag at −20°C and thawed overnight at room temperature for testing the following day. The mean age of the specimens was 78.3 ± 6.7 years. There were 3 male and 3 female specimens. Five specimens were left hemipelvises, and 1 was a right hemipelvis. Fluoroscopic images were obtained before dissection to exclude the presence of significant degenerative joint disease.
Specimen Preparation
A 10-cm, longitudinal incision was centered on the lateral greater trochanter. Soft tissue dissection was carried down to the iliotibial band. A large rectangular section of the iliotibial band (approximately 5 × 7 cm) was excised and stored in moist, saline-soaked gauze and in an airtight bag for use as autograft for later labral reconstruction. All soft tissue superficial to the hip joint capsule was then sharply excised, leaving only the capsule and all intra-articular structures intact. The iliac wing of the pelvis and the midshaft of the femur were rigidly fixed to a stand using soft tissue clamps. The hip joint capsule was thoroughly inspected for any defects or evidence of iatrogenic injury sustained during dissection.
The 12-o’clock, or most superior, position on the articular surface of the acetabulum was identified. Under fluoroscopic guidance, an 18-gauge angiocatheter was inserted into the hip joint between the articular surface of the femoral head and labrum (Figure 1). Normal saline was infused at a constant pressure into the hip joint central compartment using a custom fluid infusion device. This fluid infusion device has been previously described. 1 Briefly, a precision regulator (type 700; ControlAir, Amherst, New Hampshire) and digital pressure gauge (MG1-9V; SSI Technologies, Janesville, Wisconsin) were used to regulate a standard laboratory air supply to deliver a constant pressure to a 1500-mL chamber filled with normal saline solution. Intravenous tubing was connected to the output of the chamber to the catheter inserted into the hip joint (Figure 2). Preliminary pilot studies were performed to determine the minimum pressure measurements required to create enough fluid distention of the hip joint capsule when all soft tissues remained intact. The fluid pressures determined to meet this criteria—2, 3, and 4 psi—were used in each labrum-tested condition.
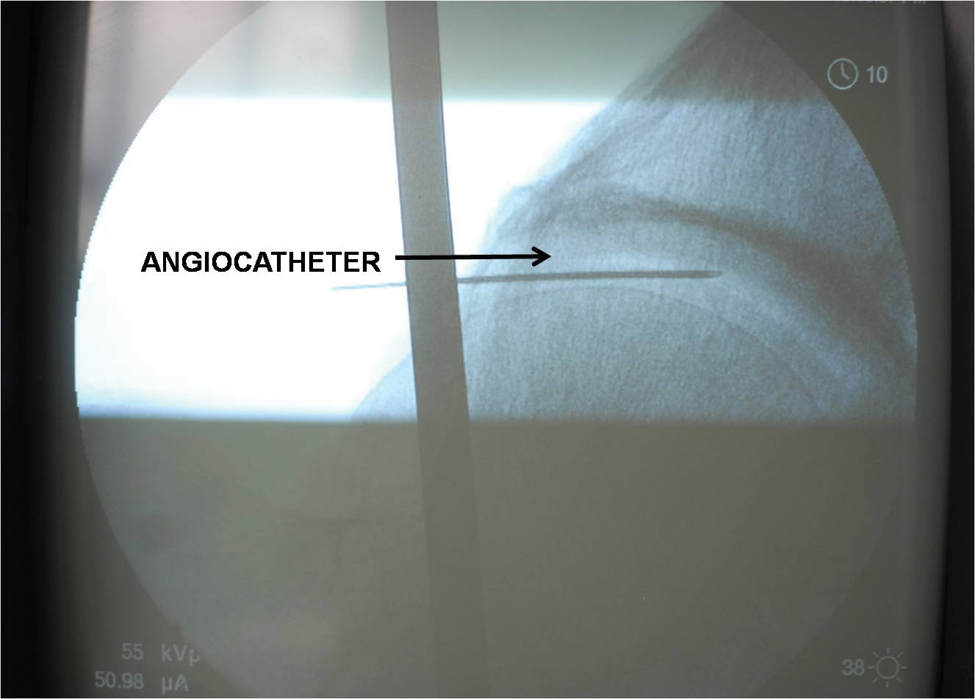
Fluoroscopic image of angiocatheter position within the hip central compartment.
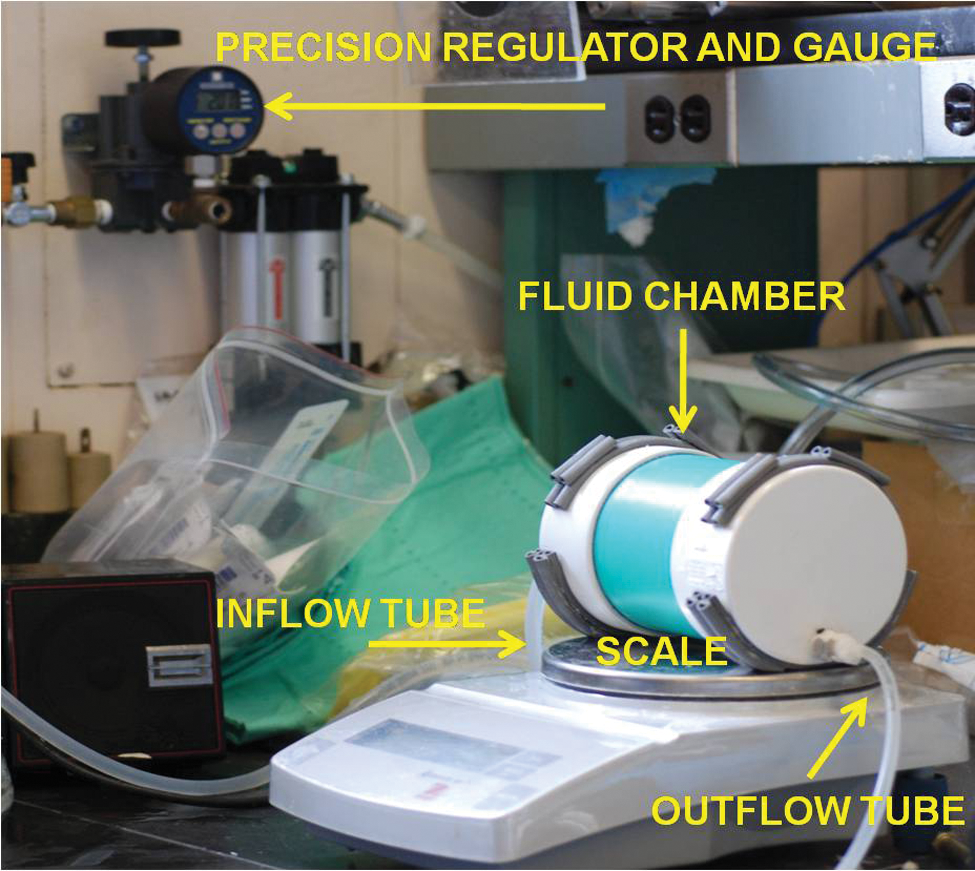
Fluid infusion testing apparatus. Here, 0.9% normal saline flows from the fluid-filled canister and outflow tubing into the hip central compartment at different labral-tested conditions under regulated infusion pressures generated from the air pressure gauge. Flow rate was determined by the calculated weight reduction of the fluid canister measured by a scale.
Labrum Testing Conditions
Five hip labrum conditions were tested at fluid pressures of 2, 3, and 4 psi at 30-second intervals for a total of 2 minutes. The sequence of fluid pressure settings was randomized for each testing condition. The 5 testing conditions were as follows: (1) labrum intact, (2) simulated 2-cm tear at labrum-chondral junction, (3) labral repair, (4) partial labral resection, and (5) labral reconstruction with ipsilateral iliotibial band autograft (Figure 3). For the labral tear condition, the superficial layer of the capsule was carefully lifted from the medial labrum and acetabulum to identify the labral-chondral junction. Once identified, a 2-cm labral tear was created to separate the labrum from the footprint using a sharp No. 11 blade at the labral-chondral junction. The location of the labral tear spanned the 12-o’clock to 2-o’clock position on the acetabular face of the right hip (10- to 12-o’clock position in the left hip), a common site where hip labral tears occur and a typical tear pattern seen specifically with cam impingement. Labral repairs were performed using three 2.3-mm PEEK suture anchors with No. 2 nonabsorbable sutures (Bioraptor, Smith & Nephew, Andover, Massachusetts) positioned slightly medial to the articular surface at the labral footprint to avoid joint penetration. Sutures were passed using a simple suture technique. Partial labrum resection was at the zone of the created labral tear. For labrum reconstruction, the piece of autogenous iliotibial band tissue that was previously harvested was sized to match the labral defect. The iliotibial band tissue was then tubularized using a 2-0 absorbable suture and attached to the labral footprint using suture anchors previously placed for the labral repair. Sutures were then passed and tied using a simple suture technique. The surrounding capsule was then sutured to the iliotibial band tissue using 2-0 absorbable suture, using a combination of simple and figure-of-8 sutures.
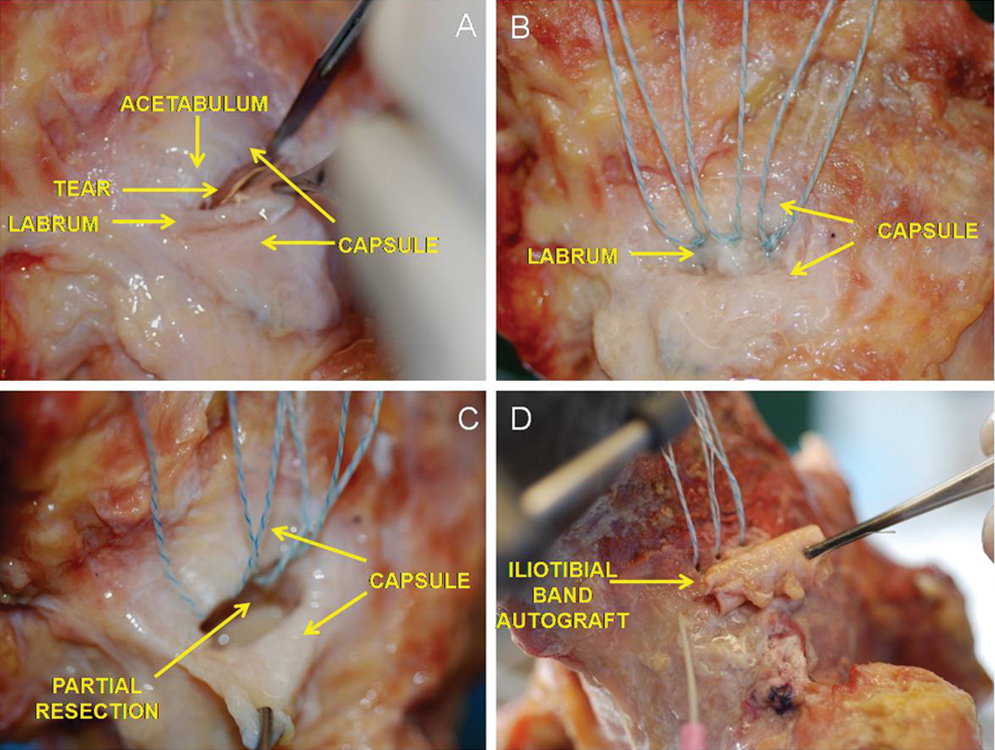
Labral tested conditions: (A) labral tear condition; (B) labral repair; (C) partial labral resection; (D) labral reconstruction with ipsilateral iliotibial band autograft.
Fluid expression for each condition was measured as fluid flow rate (mL/sec) and was determined by measuring weight reduction of the saline-filled chamber during pressurized fluid infusion during 30-second time intervals. For each condition and measurements, the fluid inflow was allowed to reach a steady state for approximately 60 seconds. The precision of the calculated density using this model has been previously determined by Ahmad et al to be 9.4 × 10−5 g/mL. 1
Statistical Analysis
Four measurements separated by 30-second intervals at each pressure setting (2, 3, and 4 psi) for each testing condition (labrum-intact, -tear, -repair, -resection, and -reconstruction) were obtained. The mean fluid efflux values for each pressure setting at each testing condition were calculated. Statistical differences between conditions were assessed using a 2-way, repeated-measures analysis of variance. The SNK multiple comparison test was used to determine differences between levels. Statistically significant difference was defined as α < .05.
Results
Effect of Simulated Labral Tear on Fluid Efflux When Compared With the Labrum-Intact Condition
Qualitatively, greater fluid efflux was seen in all specimens when a labral tear was created compared with the labrum-intact condition. Furthermore, fluid efflux occurred only at the region where the labral tear was created (eg, at the location of disruption of the chondral-labral junction). No fluid efflux was seen between the labrum and its lateral capsular attachments. Quantitatively, there was a significant increase in fluid flow rate in the simulated labral tear condition (0.54 ± 0.3 mL/sec) when compared with the intact labrum condition (0.006 ± 0.0 mL/sec, P < .05; Figure 4 and Table 1; mean flow rate of accumulated pressure settings for each labral-tested condition).
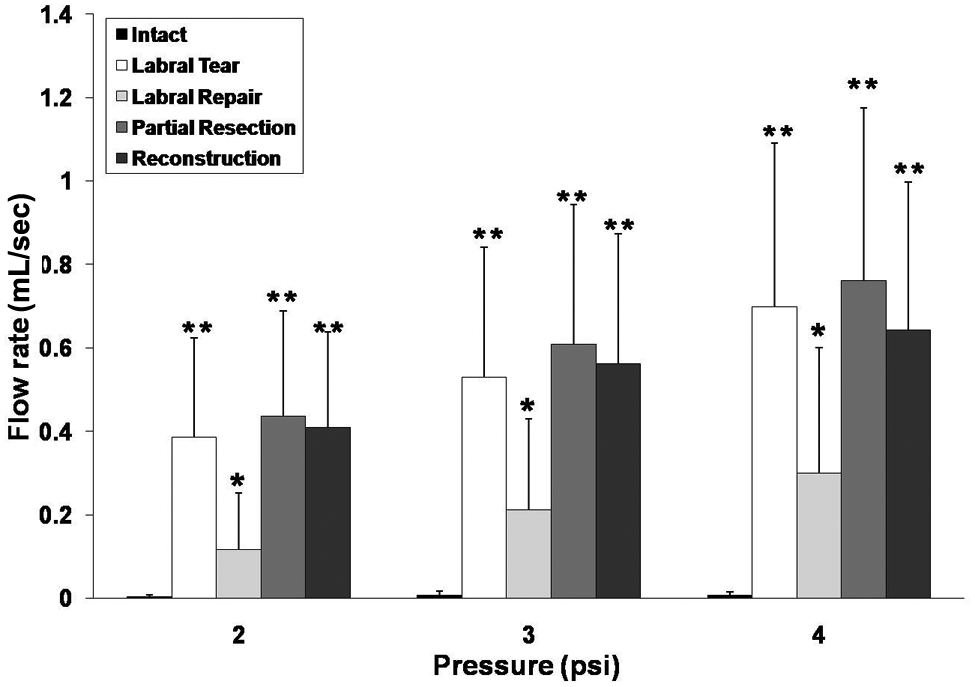
Central compartment fluid efflux (mL/sec) between the different labral-tested conditions at different infusion pressures (psi). * Denotes difference from intact, ** denotes difference between labral tear and intact conditions, P < .05.
Cumulative Flow Rate Among Different Labral-Tested Conditions a
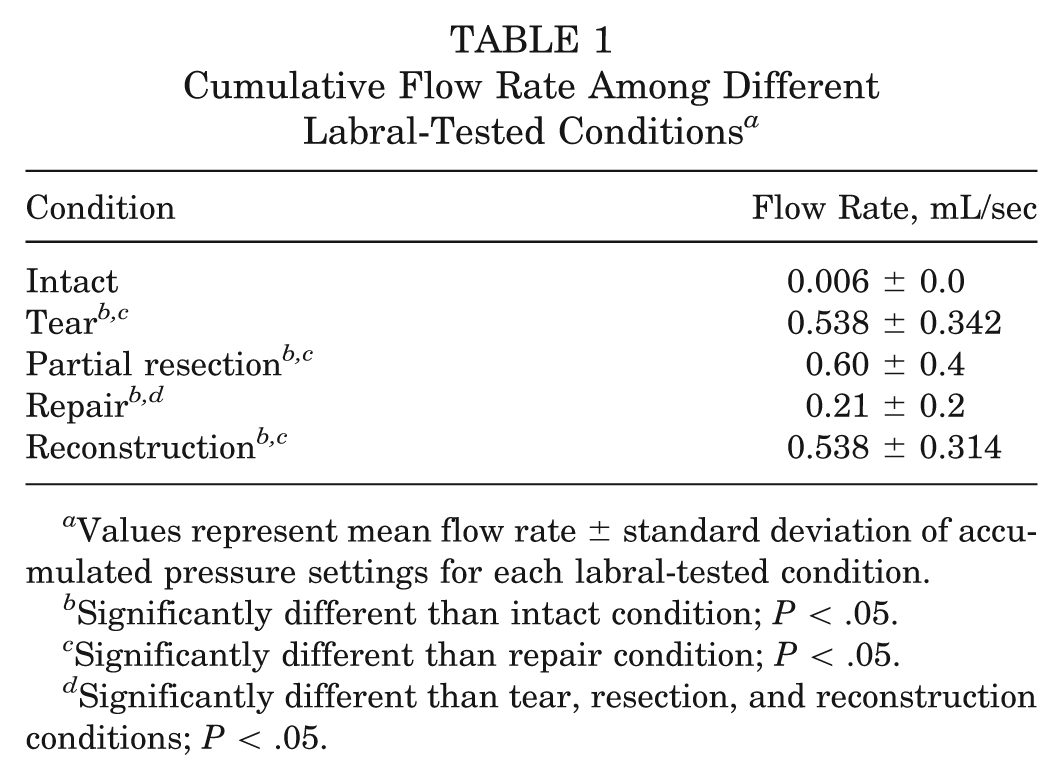
Values represent mean flow rate ± standard deviation of accumulated pressure settings for each labral-tested condition.
Significantly different than intact condition; P < .05.
Significantly different than repair condition; P < .05.
Significantly different than tear, resection, and reconstruction conditions; P < .05.
Effect of Labral Repair on Fluid Efflux When Compared With the Labral Tear and Intact Conditions
Qualitatively, less fluid efflux was seen at the repair site when compared with the labral tear condition; however, fluid impermeability did not approach levels seen in the labrum-intact condition. Quantitatively, significant decreases in fluid efflux were seen in the labral repair condition (0.21 ± 0.2 mL/sec) when compared with the labral tear condition (0.54 ± 0.3 mL/sec, P < .05). However, fluid flow rates in the labral repair condition were significantly greater when compared with the labrum-intact condition (0.006 ± 0.0 mL/sec, P < .05; Figure 4 and Table 1; mean flow rate of accumulated pressure settings for each labral-tested condition).
Effect of Partial Labral Resection and Reconstruction Using Autogenous Iliotibial Band on Fluid Efflux When Compared With the Labral-Repaired and Intact Conditions
Qualitatively, when compared with the labrum-intact, -tear, and -repaired conditions, fluid efflux occurred at a higher rate in the partial-resection condition. Fluid flow was visualized at the zone of labral resection. Quantitatively, significant increases were observed in fluid efflux with partial labral resection (0.60 ± 0.4 mL/sec) when compared with the labrum-intact and -repaired conditions, respectively (P < .05).
Qualitatively, fluid extravasated throughout the reconstructed construct, without a discrete focus of fluid efflux. Quantitatively, there was no significant difference observed in fluid flow rates with partial labral resection when compared with the reconstructed conditions (0.60 ± 0.4 mL/sec vs 0.538 ± 0.314 mL/sec). Furthermore, similar flow rates were seen with labral reconstruction when compared with the labral tear condition (0.538 ± 0.314 mL/sec and 0.538 ± 0.342 mL/sec, respectively; P > .05). Labral reconstruction was more permeable when compared with the labral repair and intact conditions (0.538 ± 0.314 mL/sec vs 0.21 + 0.2 and 0.006 ± 0.0 mL/sec, reconstructed vs repair and intact, P < .05; Figure 4 and Table 1; mean flow rate of accumulated pressure settings for each labral-tested condition).
Effect of Fluid Infusion Pressure on Fluid Efflux Rates
Qualitatively, fluid was expressed at a higher rate with increasing fluid infusion pressure. Quantitatively, significantly higher fluid efflux was seen with increasing fluid infusion pressures for all labral conditions tested (0.27 ± 0.26 mL/sec < 0.38± 0.35 mL/sec < 0.48 ± 0.43 mL/sec; 2 psi < 3 psi < 4 psi; P < .05; Figure 5; mean flow rate of all labral-tested conditions relative to pressure setting).
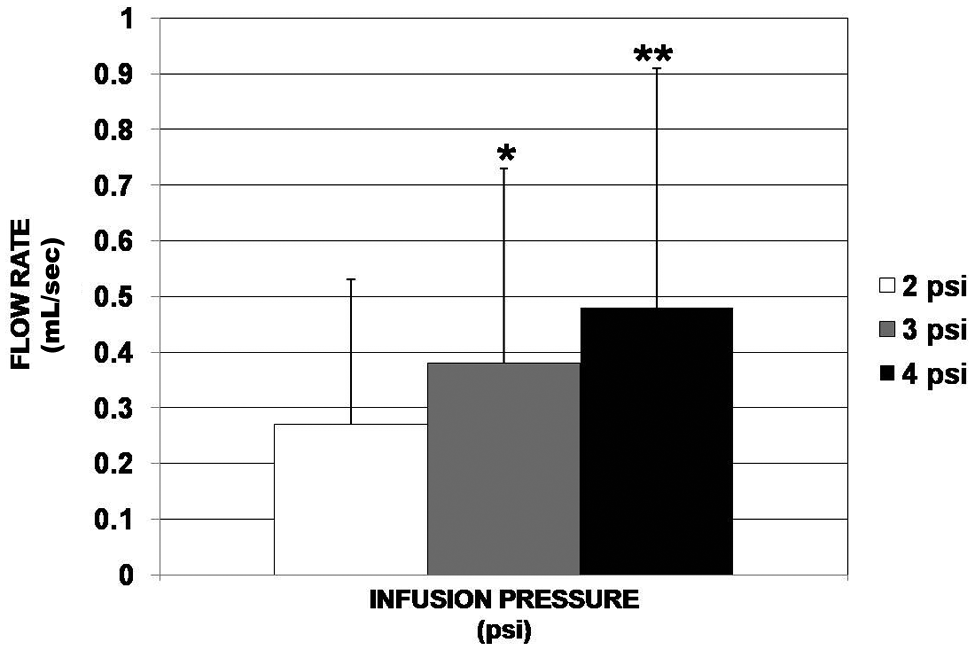
Central hip compartment fluid efflux (mL/sec) at different infusion pressures.
Discussion
The purpose of this study was to determine the fluid seal properties of the hip labrum in the intact and labral tear conditions, as well as in commonly encountered clinical scenarios, specifically, after repair, partial-resection, and reconstruction using ipsilateral iliotibial band autograft. To determine the fluid seal properties of these conditions, a custom-made, saline-fluid infusion pump was used to deliver saline into the hip central compartment at a constant rate and infusion pressure. Fluid efflux was measured as flow rates in a human cadaveric hip model. Our findings suggest that hip labral repair significantly decreased fluid efflux when compared with the labral tear and partially resected conditions; however, hip labral repair did not prevent fluid efflux as effectively as the labrum-intact state. Furthermore, in this model, labral reconstruction using ipsilateral iliotibial band autograft was not effective in preventing fluid efflux when compared with the labrum-repair or -intact conditions. Interestingly, labral reconstruction demonstrated high fluid permeation characteristics similar to those of the labrum-torn and partially resected conditions.
The hip labrum has been hypothesized to serve a vital role in providing hip stability by first, increasing the articular surface area and volume,21,22 and second, through its “fluid seal” effect.8-10 The “fluid seal” refers to the ability of the hip labrum to prevent synovial fluid efflux from the intra-articular central compartment to the peripheral compartment. Through the “fluid seal” effect, the hip labrum creates a layer of pressurized fluid that decreases contact stresses between the acetabular and femoral cartilaginous surfaces. 9
The long-term consequence of hip labral tears and labral deficiency remains controversial; however, basic science studies have suggested that labral tears and/or resection can (1) increase femoral head translation within the central compartment, potentially subjecting the adjacent articular cartilage to increased strain 3 ; (2) decrease distraction forces of the femoral head, thus potentially contributing to hip joint instability 3 ; and (3) increase strain to the adjacent intact labrum via disruption of hoop stresses. 4 Furthermore, labral tears and deficiency have been hypothesized to contribute to the development of early degenerative hip disease via the previously mentioned mechanisms.15,21
Despite historically good to excellent results achieved after surgical labral debridement and/or resection,2,7 emphasis is currently being placed on labral preservation, in the form of repair when possible, in addressing labral tears or re-fixation of the labrum in the setting of the surgical management of femoroacetabular impingement.6,11-14,16 Although relatively avascular, the hip labrum has been previously demonstrated to possess the potential to heal after repair; however, this healing process has been shown to be “incomplete,” which has been demonstrated by persistent defects at the labral-chondral junction seen on histologic analysis. 17 This issue raises the question of how effective current hip labral repair techniques are in preserving the “fluid seal” characteristics of the hip joint when compared with the intact, debrided, or partially resected states. To the authors’ knowledge, there are no current studies that have investigated the fluid efflux properties of hip labral repairs. Our study demonstrates that labral repairs in a cadaveric hip model inhibit fluid efflux from the central compartment when compared with the torn, partially resected, and reconstructed states, but these repairs are not as effective as in the labrum-intact state.
Furthermore, recent studies have shown promising clinical outcomes performing open and arthroscopic labral reconstruction using either ipsilateral iliotibial band autograft5,18 or ligamentum teres capitis 22 in patients with symptomatic labral deficiency after previous labral debridement. Presumably, the clinical benefits of labral reconstruction would be from restoration of the integrity of the hip joint “fluid seal”; however, such properties of labral reconstruction have yet to be studied. Our study is the first to investigate the fluid permeability characteristics of current hip labral reconstruction techniques. Our findings suggest that labral reconstruction may not significantly restore the fluid seal when compared with the labrum-intact and -repair states in vitro; however, our results cannot explain the benefit observed clinically in patients who have undergone labral reconstruction in the setting of labral deficiency. The clinical benefits seen after labral reconstruction in the labral-deficient hip may come from restoring hip stability by increasing surface area, a theory that was beyond the scope of this current study.
Several limitations exist in the study. First, our cadaveric hip model does not take into account the biologic responses after labral repair and reconstruction and underrepresents potential healing that can occur at the labral-chondral junction, which would therefore potentially affect synovial fluid efflux from the central compartment. Second, 1 labral repair and reconstruction technique was used during this investigation. We recognize that other labral repair and reconstruction techniques exist and may be more effective in fluid efflux prevention. Third, hip joint kinematics after labral repair, resection, and reconstruction were beyond the scope of this study and were not investigated. This limitation may under-represent the potential biomechanical benefits of such treatment interventions or determining a “critical” limit for labral debridement or resection. Fourth, axial or rotational loading of the hip joint was not included in our protocol. We recognize that all of these factors play an important role in accurately characterizing fluid flow dynamics within the hip joint in vivo. Furthermore, we recognize that the viscosity and flow characteristics of normal saline differ compared with synovial fluid and between younger and aged specimens, and as such, different flow rate results may be seen between the 2 media and in younger cadaveric specimens. In addition, the relationship of a controlled capsulotomy and hip joint fluid expression was not entirely studied in this work. The authors recognize that this specific maneuver performed in arthroscopic and open hip joint surgery may affect fluid seal characteristics. Finally, only 1 type of labral tear was investigated. We recognize that several different labral tear patterns exist in clinical practice, and these different tear patterns may have different fluid expression characteristics than those represented in this model.
In conclusion, our study demonstrates that hip labral repair significantly prevents fluid efflux from the central compartment when compared with the labral tear, partially resected, and reconstructed conditions in a hip cadaveric model. However, labral repair did not restore fluid seal characteristics to those seen in the labrum-intact condition.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: The authors acknowledge Smith & Nephew (Andover, Massachusetts) for contribution of the 2.3 mm PEEK suture anchors (Bioraptor) for completion of this project.