
Abstract
Background:
Although arthroscopic techniques are the most common procedures today when reconstructing the anterior cruciate ligament (ACL), many surgeons still prefer the open and/or 2-incision techniques.
Hypothesis:
There are no differences in knee function or prevalence of knee osteoarthritis (OA) in patients who have undergone the open versus endoscopic technique for ACL reconstruction using the patellar tendon autograft.
Study Design:
Randomized controlled trial; Level of evidence, 2.
Methods:
Sixty-seven patients with subacute or chronic rupture of the ACL were randomly assigned to open (OPEN) (n = 33) or endoscopic (ENDO) (n = 34) reconstruction. Function was evaluated by the Cincinnati knee score, single-legged hop tests, and isokinetic muscle strength tests. The radiographs were classified according to the Kellgren and Lawrence (KL) classification system, defining grade 2 or more as the cutoff point for knee OA. The Insall-Salvati ratio and the Blackburne-Peel ratio were used to calculate the patellar position and height.
Results:
Mean age at inclusion and at the 12-year follow-up evaluation was 27.9 ± 8.6 and 39.8 ± 8.6 years, respectively. At 12-year follow-up, 53 patients (79%) were eligible for evaluation. There were no significant differences between the 2 surgical procedures with respect to the pain, function, muscle strength, hop tests, patellar height, or the prevalence of OA. The prevalence of OA was high in the tibiofemoral joint on the operated side, 79% and 80% in the OPEN and ENDO groups, respectively. For the uninvolved knee, the corresponding numbers were 36% and 21%.
Conclusion:
This study suggests that the open procedure does not produce more functional problems or osteoarthritis compared with the endoscopic technique up to 12 years postoperatively.
In the past few decades, operative techniques for reconstruction of the ruptured anterior cruciate ligament (ACL) have gone through an enormous development, from open and mini-open techniques with 1 or 2 incisions to arthroscopic techniques, different graft choices, multiple-bundle techniques, and change of graft placement. But there is still lack of science behind the technical changes. Several advantages of endoscopic techniques compared with open approaches have been described: smaller incisions 4 ; avoiding lateral femoral incision, giving easier rehabilitation and better quadriceps function 5 ; more accurate visualization and precise placement of the tunnels for better biomechanics; better stability and less osteoarthritis; and more rapid rehabilitation. 25 It may be hypothesized that open and mini-open procedures cause increased donor site morbidity (tenderness, anterior knee pain, disturbance in sensitivity, and inability to kneel) compared with the endoscopic techniques. The open procedure is done through the patellar tendon defect using forceful retractors and arthrotomy, which may cause increased soft tissue trauma and scar tissue, leading to anterior knee problems such as patella baja, quadriceps deficit, and joint degeneration. However, whether the surgical endoscopic procedure advances have improved the patients’ function and activity level or decreased the prevalence of osteoarthritis (OA) in the long term is still to be proved. One may claim that this question is no longer relevant according to current clinical practice. Although arthroscopic techniques are most common today, there are still huge patient cohorts earlier treated with open surgery. In addition, a large number of surgeons still prefer the open and/or 2-incision techniques. Therefore, long-term follow-up data on functional outcome and prevalence of OA are still of significant importance.
No previously published randomized controlled trials have compared the long-term effects after open versus endoscopic ACL reconstructions. The aim of the present study was to compare the functional results, prevalence of OA, and donor site morbidity 12 years after the 2 procedures. We hypothesized that there were no differences in knee function or prevalence of knee OA in patients who have undergone the open versus endoscopic technique for ACL reconstruction using a patellar tendon autograft.
Materials and Methods
Patients
Between 1994 and 1995, a total of 67 patients with chronic rupture of the ACL (>6 months since injury) were asked to participate in a randomized controlled study comparing open (OPEN; n = 33) versus endoscopic (ENDO; n = 34) ACL reconstruction. The inclusion criteria were persons aged between 15 and 50 years who had an isolated ACL rupture or an ACL rupture combined with medial collateral ligament rupture and/or meniscal tear. Exclusion criteria were other major knee injuries and/or degenerative joint disease. The participants were assigned to the OPEN or ENDO group by a simple randomization procedure using sealed opaque envelopes. It was conducted by a person working in the orthopaedic department who was not involved in the study.
Twenty-six women and 41 men with a mean (SD) age of 27.9 (8.6) years were included in the study. No performance-based tests were carried out preoperatively. The patients were tested 6, 12, and 24 months after surgery and were called up for a long-term follow-up evaluation 12 years postoperatively (Figure 1). The study was approved by the Norwegian Ethics Committee of Medical Research, and the patients gave their written, informed consent to participate.
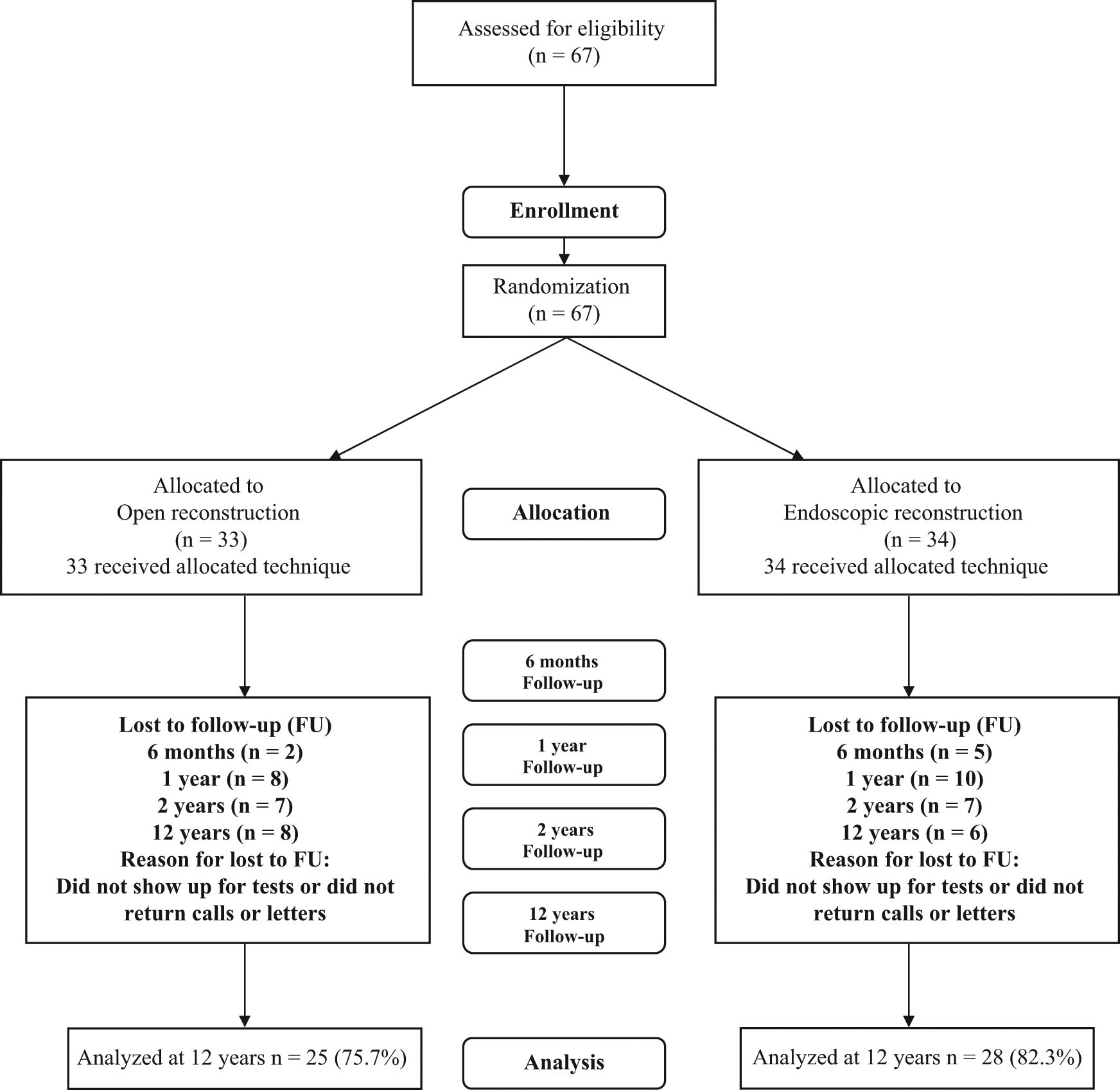
Study flowchart.
Surgical Procedures
For the patients randomized to the group undergoing endoscopic patellar tendon–bone (PTB) reconstruction (ENDO), graft from the central third of the patellar tendon was harvested via a longitudinal incision. The graft included a 25-mm trapezoidal bone block and a 25-mm rectangular tibial bone block. The bone blocks were trimmed to pass through a 9-mm diameter gauge. The intra-articular procedure was done using an arthroscope through a lateral portal. A medial portal was used for instrumentation. A guide wire was drilled from the medial side of the tibial tubercle at a 45° angle from the medial side of the tibial shaft and advanced to the preserved ligament stump of the ACL footprint with use of a drill guide (Linvatec Corp, Largo, Florida). A 9-mm cannulated drill bit was used to drill the tibial tunnel. With the knee flexed, a femoral aimer with 7-mm offset (Linvatec) was introduced through the tibial tunnel and positioned at the proximal part of the femoral insertion site. A guide wire was drilled through the aimer and advanced into the femur. A 9-mm cannulated drill bit was introduced over the guide wire and drilled to a depth of 25 mm. The graft was passed into the knee using the Paramax system (Linvatec) and fixed with a 7 × 25-mm titanium femoral interference screw (Linvatec). The knee was cycled under graft tensioning to allow stress relaxation of the graft. The graft was then tensioned to 20 pounds and, with the knee at 0° of flexion, fixed in the tibial tunnel with a 7 × 25-mm tibial interference screw. 1
The open PTB reconstruction (OPEN) used the same surgical procedure for harvesting, drilling, and fixation, but it was done through an arthrotomy in the patellar tendon defect. Visualization was enhanced using a self-holding retractor with light a source. Before the ACL reconstruction, a diagnostic or therapeutic arthroscopy was performed in both groups, and any meniscal injury was addressed. The same surgeon performed all the surgical procedures.
Rehabilitation
Both groups went through the same rehabilitation program. Weightbearing was permitted as tolerated from day 1 postoperatively. After 2 weeks, stationary bicycling was allowed, and after 6 to 8 weeks, light jogging was permitted. Return to full sports activities was allowed after 6 months if the criteria of full range of motion, no effusion, a limb symmetry index for hamstrings and quadriceps muscle strength of at least 85%, and knee stability were met.
Follow-up Evaluation
Follow-up evaluations were performed at 6, 12, and 24 months as well as 12 years after surgery, and the physical therapists who collected the evaluation data were unaware of which intervention had been administered to which participant. The results from the 2 first years have previously been published only as an abstract in Norwegian. Except for a significantly better functional outcome in the first postoperative weeks in the patients who had undergone endoscopic reconstruction, there were no differences between the 2 groups for knee joint laxity or function at the 2-year follow-up evaluation.
Twelve years after surgery, the patients received an invitation to participate in a further follow-up evaluation. The procedure at the 12-year follow-up evaluation has been published previously. 7 Activity level was estimated by the Tegner activity score, 26 and knee function was evaluated with the Cincinnati knee score. 14 Knee joint laxity was recorded using a KT-1000 knee arthrometer (MEDmetric Corp, San Diego, California) at the manual maximum force. 28 Visual analog scales (VAS) (0 = no pain and 100 = extreme pain) were used to evaluate pain at rest, pain in activity, and kneeling pain. 18 The VAS was also used to evaluate subjective function (0 = unacceptable function and 100 = excellent function).
Isokinetic muscle strength was measured with the Cybex 6000 dynamometer (Cybex International, Inc, Medway, Massachusetts). Before testing, the participants performed ergometer cycling for 8 to 10 minutes. The test protocol consisted of 5 repetitions at an angular velocity of 60 deg/sec, followed by a 1-minute rest period and then 30 repetitions at 240 deg/sec. Isokinetic parameter used for evaluation of muscle strength was total work (measured in Joules). Three functional knee tests (the stair hop, single-legged hop, and triple-hop tests) were used to evaluate lower limb function. 19
We used radiographs to evaluate the prevalence of knee OA. For the tibiofemoral joints, weightbearing frontal views were taken as posteroanterior fixed flexion radiographs. 11 A SynaFlexer frame (Synarc, Inc, Copenhagen, Denmark) was used to standardize the degree of knee flexion in approximately 20° and the feet in 5° of external rotation. 17 For the patellofemoral joints, we used both lateral and skyline views. The lateral views were taken standing with the knee flexed approximately 20°, and for the skyline view, the knee was flexed about 40°. The radiographs were classified according to the Kellgren and Lawrence (KL) classification system,10,17 including grade 0, no changes; grade 1, doubtful narrowing of the joint space and possible osteophytic lipping; grade 2, definite osteophytes and possible narrowing of the joint space; grade 3, moderate multiple osteophytes, definite narrowing of the joint space, and some sclerosis, as well as possible deformity of the bone ends; and grade 4, large osteophytes, marked narrowing of the joint space, severe sclerosis, and definite deformity of the bone ends. Grade 2 or higher was used as a cutoff for knee OA. 22 Both the Insall-Salvati ratio 8 and the Blackburne-Peel ratio 2 were used to calculate the patellar position/height bilaterally. Blinding of the radiologist evaluating the radiographs was not possible because of the visible screws in the surgically treated knee.
Statistical Analysis
We used SPSS version 18.0 (SPSS Inc, Chicago, Illinois) for the statistical analyses. A priori statistical power analysis was performed with the Cincinnati knee score as the primary outcome variable. Sample size calculations estimated that 32 patients would be needed in each group to detect a 10-point difference in the Cincinnati knee score between the 2 groups, with a standard deviation (SD) of 12 points, an α level of 0.05, and a β level of 0.10. 20
Data are presented as arithmetic means and dispersion by 1 SD or as frequencies (categorical data). A mixed between-within subject analysis of variance (ANOVA) was used to assess the impact of the OPEN and ENDO procedures on the patients’ functional outcomes across the 4 periods. To compare the scores between the 2 surgical procedures for categorical data (OA classified by the KL system), we used a χ2 test. The significance level was set to .05.
Results
Patient Characteristics
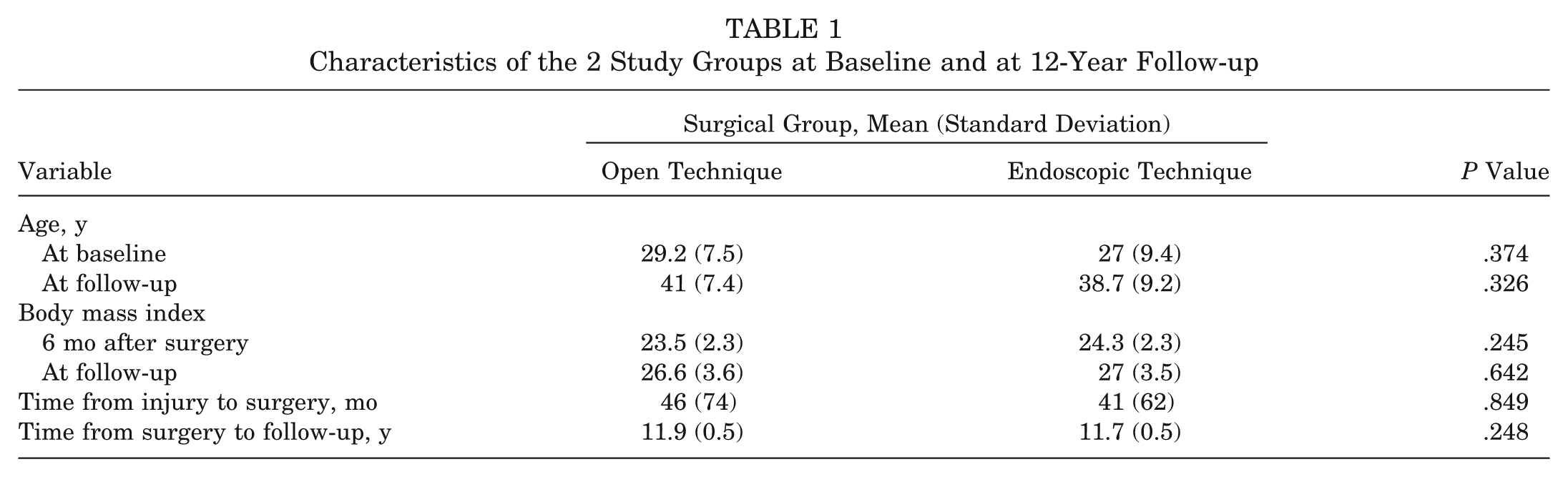
During the 12-year study period, 14 patients (21%) were lost to follow-up: 8 in the OPEN and 6 in the ENDO group, respectively (Figure 1). Patient demographics for the 2 groups at baseline and at 12-year follow-up are presented in Table 1. There were no differences between the groups either at baseline or at the 12-year follow-up evaluation. However, there was a significant increase in body mass index (BMI) for both groups during the study period.
Characteristics of the 2 Study Groups at Baseline and at 12-Year Follow-up
At baseline, 34 patients (50%) had an isolated ACL injury. Eighteen patients in the OPEN group and 16 patients in the ENDO group had additional meniscal tears. At 12-year follow-up, 14 patients (8 [32%] in the OPEN group and 6 [21%] in the ENDO group) had torn their contralateral ACL (P = .534). Four patients (16%) in the OPEN group and 7 patients (25%) in the ENDO group had reinjured their reconstructed ACL (P = .503). Knee joint laxity (KT-1000 arthrometer, manual maximum test) was 1.8 ± 2.9 mm and 1.4 ± 2.9 mm (P = .662) for the OPEN and ENDO groups, respectively. In the OPEN group, 68% (17 of 25 patients) scored 3 mm or less side-to-side difference, as did 82% (23 of 28 patients) in the ENDO group (P = .231).
Self-reported Function, Muscle Strength, and Hopping Performance
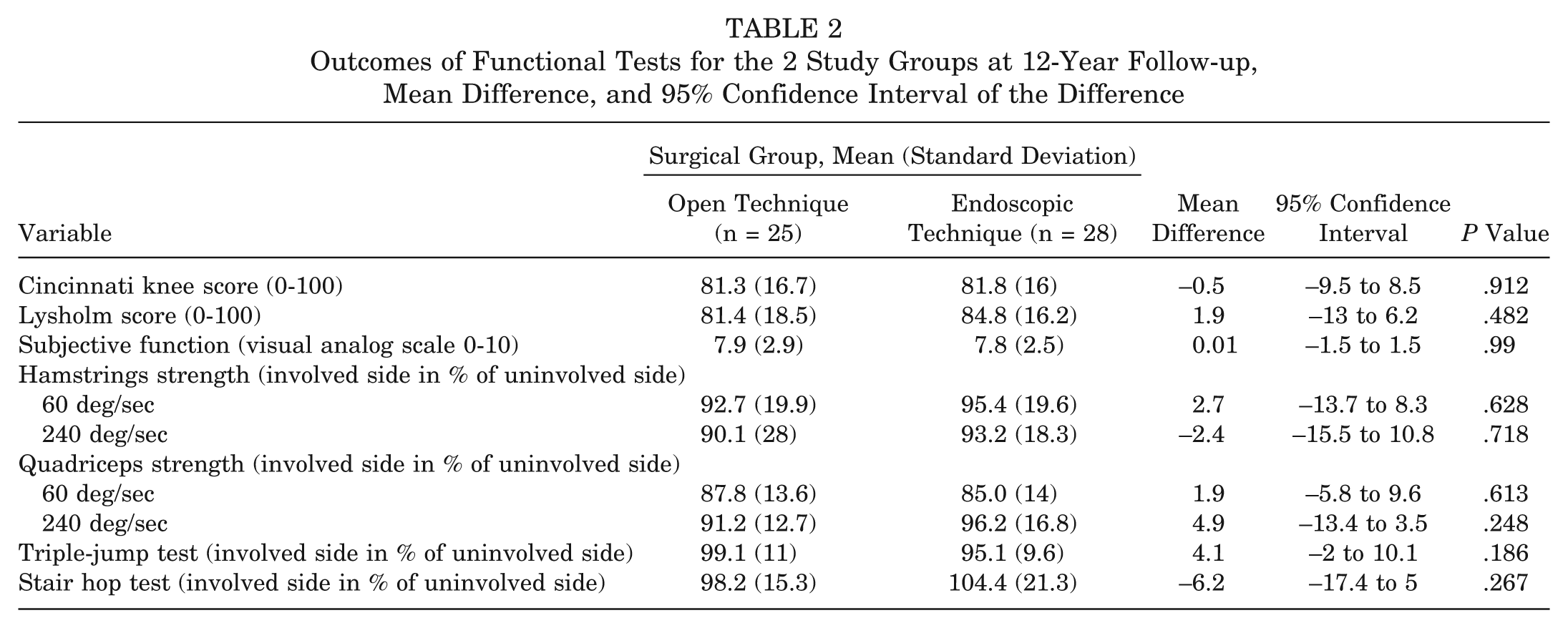
The results for the repeated measures showed no significant interaction between surgical procedure and time for any of the functional outcomes (self-reported function, muscle strength, and functional tests). There was a substantial main effect of time, with both groups showing change in function scores across the 4 periods. Both groups showed increased self-reported function, muscle strength, and hopping performance up to 2 years postoperatively (Figures 2 and 3). At 12-year follow-up, both groups showed reduced functional capacity, probably because of increased age and reduced activity level. The side-to-side differences, however, remained unchanged between the 2-year and 12-year follow-up, except for quadriceps strength, where the side-to-side differences were significantly reduced. Table 2 shows the self-reported function and the outcomes from the muscle strength and hop tests for both groups at 12-year follow-up, showing that quadriceps strength (60 deg/sec) was the only parameter that still showed a deficit of more than 10% compared with the nonoperated side. Kneeling pain (VAS) was 6.5 ± 3.7 and 6.2 ± 3.7 for the OPEN and ENDO groups, respectively.
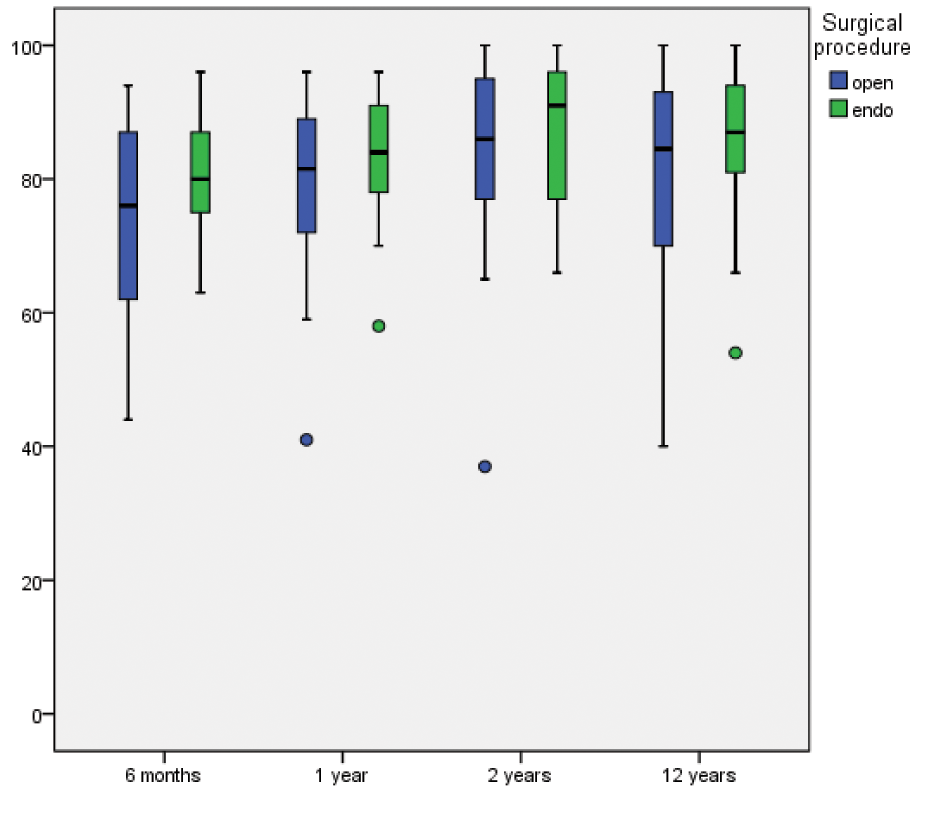
The Cincinnati knee score for the open and the endoscopic technique groups during the 12-year follow-up evaluation.
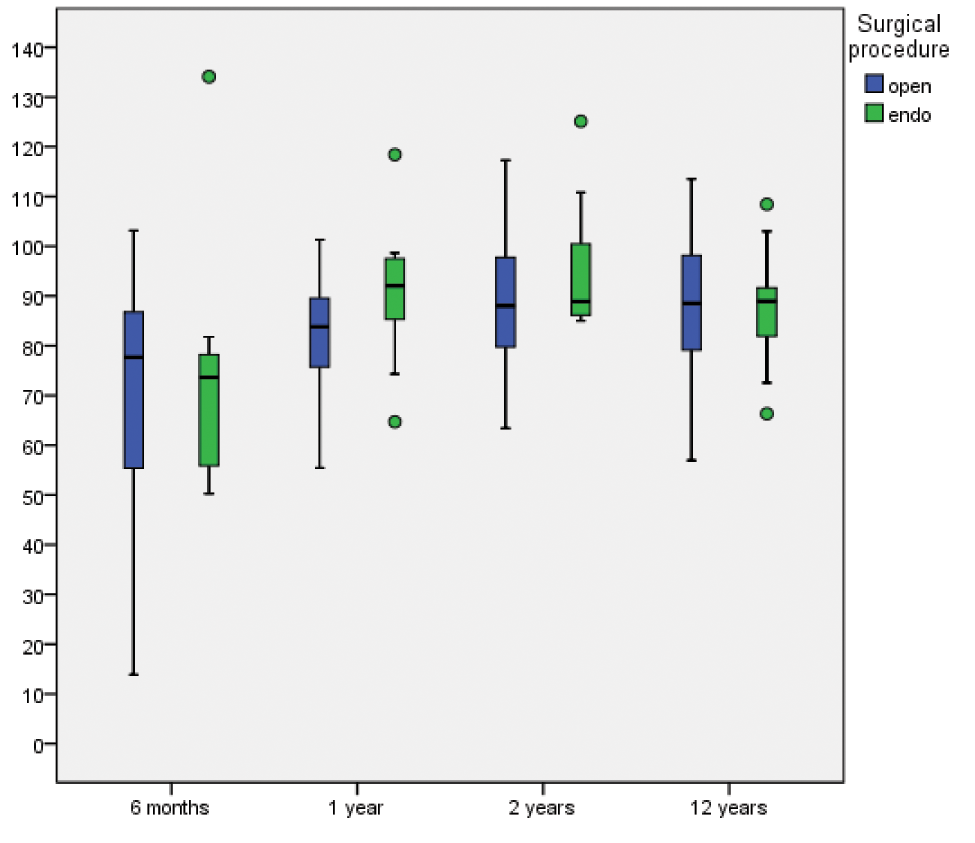
Limb symmetry index calculated from bilateral quadriceps strength for the open and the endoscopic technique groups during the 12-year follow-up evaluation. A value of 100 indicates total limb symmetry.
Outcomes of Functional Tests for the 2 Study Groups at 12-Year Follow-up, Mean Difference, and 95% Confidence Interval of the Difference
Distribution of Osteoarthritis
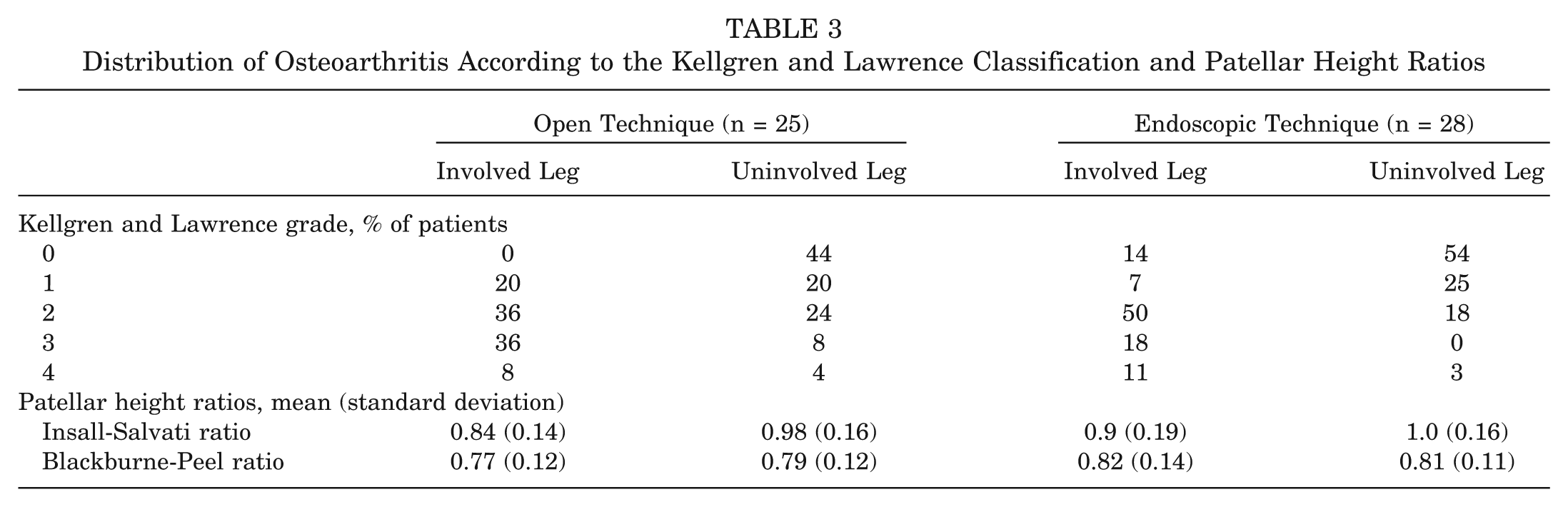
The distribution of radiologic tibiofemoral OA graded according to the KL classification system is shown in Table 3. Eighty percent and 79% of the patients had OA grade 2 or higher in the operated knee in the OPEN and ENDO groups, respectively (P = 1.000). The corresponding numbers for the uninvolved leg were 36% and 21% (P = .58). If the cutoff point for radiologic OA had been defined as grade 3 or higher, the prevalence of OA in the involved leg would have been 44% and 29% for the 2 groups, respectively (P = .247). The prevalence of OA in the patellofemoral joint was 20% and 36% for the OPEN and the ENDO groups, respectively (P = .09). The prevalence of symptomatic OA in the tibiofemoral joint (KL grade 2-4 and self-reported knee pain at 12-year follow-up) was 36% for the OPEN group and 43% for the ENDO group. The patellar heights measured at 12-year follow-up are shown in Table 3. There were no significant differences between the OPEN and ENDO groups; there was, however, a significant difference for the Insall-Salvati ratio between the involved and uninvolved leg in both groups, with P < .0001 in both groups.
Distribution of Osteoarthritis According to the Kellgren and Lawrence Classification and Patellar Height Ratios
Discussion
The present study showed that there were no differences in knee function or prevalence of OA 12 years after open versus endoscopic reconstruction of the ACL. The results are in correspondence with the findings by Harner et al 6 and Fremerey et al 4 but add important information about the prevalence of OA. In the present study, the prevalence of OA, particularly mild OA, in the tibiofemoral joint on the operated side was high in both groups (80% and 79%, respectively) and significantly higher than on the contralateral side. The prevalence of radiographic tibiofemoral OA has been reported to be 13% for isolated ACL injuries and from 21% to 48% for patients with combined injuries more than 10 years after ACL injury or reconstruction. 16 Possible explanations for the extremely high prevalence of tibiofemoral OA in the present study could be the high incidence of combined injuries (50%) and the long time from injury to surgery, 43 ± 64 months. Another explanation for the high prevalence of radiographic tibiofemoral OA might be the choice of defining grade 2 or more (according to the KL classification system) as the cutoff for knee OA. The KL grade 3 is possibly more in correspondence with, for example, the International Knee Documentation Committee’s definition of OA, 9 and a cutoff of 3 would have reduced the prevalence of OA significantly. The prevalence of OA in the patellofemoral joint was 20% and 36% for the OPEN and the ENDO groups, respectively. Our findings correspond with the results from a study reporting on 249 individuals who had undergone primary single-bundle ACL reconstruction 7.8 years earlier, 13 where the prevalence of patellofemoral OA was 25.3%.
Forty-four percent and 29% of the OPEN and the ENDO groups, respectively, showed moderate to severe OA (KL grade 3 or 4) in the tibiofemoral joint compared with only 1 patient showing a grade 3 OA in the patellofemoral joint. Duncan et al 3 reported that radiographic severity is significantly associated with severity of pain and function in the knee and that moderate/severe OA in any single compartment of the knee is as strong a determinant of symptoms as multicompartment disease. In the present study, there were no significant correlations between mild/moderate/severe OA findings and self-reported pain or any of the functional outcomes. The explanation for this discrepancy between these 2 studies may be that the patients included in the study by Duncan et al were significantly older than our participants.
There were no differences between the OPEN and ENDO groups concerning the position of the patella (Table 3). However, the Insall-Salvati ratio showed a significant difference between the operated and the nonoperated leg in both surgical groups, indicating that independent of the surgical approach, the procedure per se results in a certain degree of patella baja.
The increasing focus on technical advantages in ACL surgery has so far not shown any improvement in the most important outcome parameters, function and OA. Improvement in function is related to improvement in rehabilitation rather than new techniques. Shelbourne and Nitz23,24 have used the same open technique over 3 decades, showing the significant improvement of function by improving the rehabilitation strategy. The change from a 2-incision to a 1-incision technique moved the femoral fixation out of place. In 1996, O’Neill 15 found better results using the 2-incision versus 1-incision method. A decade later, the focus in ACL surgery was to reintroduce the more “anatomic” femoral fixation. Whether this fixation reduces the prevalence of OA to a higher extent is still a question. One may claim that the open technique is still an approach to consider; it is easier to learn and is less resource demanding. In addition, the present results show that an arthrotomy through the patellar tendon does not increase donor site morbidity and the prevalence of OA or reduce physical function 12 years after surgery.
No significant differences in laxity or knee function were found between the 2 groups. The knee laxity (side-to-side difference >3 mm) measured at 12-year follow-up was 32% in the OPEN group and 18% in the ENDO group (P = .231). Other recently published long-term follow-up studies have found a corresponding prevalence of laxity.12,21 Except for the maximal quadriceps strength, all side-to-side differences in muscle strength were less than 10% (Table 2), which are in agreement with the results from Wipfler et al, 27 who followed for 9 years 2 groups of patients with ACL reconstruction who received either hamstring tendon or patellar tendon grafts. The results from the triple-jump test and the stair hop test found in the present study indicate that the deficit in maximal quadriceps strength does not influence the patients’ performance of simple functional tasks.
In the present study, some limitations need to be addressed. First, the primary aim of the study was to compare the functional results between the 2 randomized groups 2 years after surgery. The power calculation was therefore based on the Cincinnati knee score as the primary outcome, not the OA classification. Thus, we do not know if the statistical power was sufficient to detect significant differences between the OPEN and ENDO groups, indicating that a type II error may have occurred.
A challenge in long-term follow-up studies is loss to follow-up. In the present study, only 20% of the patients were lost after 12 years. Nevertheless, the loss to follow-up resulted in the number of patients in each group falling below the number dictated by the original sample size calculation. Another limitation is the evaluation and classification of the radiographs, which might partly be subject to individual interpretations. However, all the readings were performed by the same radiologist and should therefore be reliable.
Conclusion
There were no significant differences between the 2 surgical procedures with respect to the self-reported function, pain, muscle strength, hop tests, patellar height, or the prevalence of OA. The prevalence of OA was high in the tibiofemoral joint, 79% and 80% in the OPEN and ENDO groups, respectively. The findings from the study suggest that the open procedure does not produce more functional problems or radiological changes compared with the endoscopic technique up to 12 years after surgery.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.