
Abstract
Background:
Efforts still need to be made to improve the technique for surgical anterior cruciate ligament reconstruction (ACLR). Several reports have claimed that ACLR with the remnant preservation technique can obtain satisfactory clinical results.
Purpose:
To compare the short-term clinical outcome of remnant-preserving ACLR with standard ACLR.
Study Design:
Randomized controlled trial; Level of evidence, 2.
Methods:
A prospective, randomized controlled study was performed in 90 consecutive patients who underwent ACLR with the remnant preservation technique (study group, n = 45) or the standard technique (control group, n = 45) with the use of a 4-strand allograft. The Lysholm score, International Knee Documentation Committee (IKDC) grade, stability assessments (Lachman test, pivot-shift test, and KT-1000 arthrometer side-to-side differences), synovial coverage of the graft, and proprioception measurements were evaluated preoperatively and at the last follow-up.
Results:
All consecutive patients who were screened for eligibility between August 2008 and April 2010 were enrolled and followed clinically. There were 39 patients in the study group and 41 in the control group who were followed for at least 2 years (mean follow-up, 25.7 months). At the last follow-up, the median Lysholm score was 99 in the study group and 95 in the control group (P = .07). The IKDC grade was A or B in 38 patients in the study group and 40 patients in the control group (P = .548). Lachman test results were negative in 38 patients in the study group and 40 patients in the control group (P = .862), and the pivot-shift test result was negative in 37 patients in the study group and 36 patients in the control group (P = .523). The mean KT-1000 arthrometer side-to-side difference averaged 1.6 ± 1.7 mm in the study group and 1.8 ± 1.8 mm in the control group (P = .694). Second-look arthroscopy was performed to evaluate synovial coverage of the graft. Normal or nearly normal synovial coverage, graded as A or B, was 71.4% (20/28) in the study group and 70.4% (19/27) in the control group (P = .966). The passive angle reproduction test result at 15° was 3.6° ± 1.8° in the study group and 3.9° ± 2.2° in the control group (P = .739).
Conclusion:
This short-term study showed that, in terms of stability, synovial coverage, and proprioception recovery, remnant preservation ACLR using an allograft had no evident advantages in clinical outcome over the standard technique.
Keywords
Anterior cruciate ligament reconstruction (ACLR) has become a common orthopaedic surgical procedure in the past several decades, and good to excellent results have been reported. However, in reviewing the literature and the senior author’s own results, a significant number of patients appear to develop late symptoms, and the failure rates vary between 8% and 25%.19,21 Therefore, as with any surgery, efforts still need to be made to improve the technique for surgical ACLR.
Recently, several reports claimed that ACLR with the remnant preservation technique can obtain satisfactory clinical results.1-5,11,14-16,18 The authors believed that the preserved remnant was likely to promote revascularization and synovial coverage of the grafts, thus improving both postoperative stability and proprioception recovery. However, the current research is limited to retrospective or noncontrolled studies,1,3,4,14,15,18 and ACLR with the remnant preservation technique has not been verified by definite clinical evidence.
The purpose of this prospective, randomized controlled study was to compare the clinical outcome of remnant-preserving ACLR with standard ACLR. The hypothesis of this study was that the remnant preservation technique could improve knee stability and promote synovial coverage of the graft and knee proprioception recovery.
Materials and Methods
This clinical trial was prospectively designed, and the patients were recruited consecutively. From August 2008 to April 2010, a total of 525 consecutive patients underwent ACLR in our hospital, from which 90 patients were enrolled and available for this study according to the inclusion and exclusion criteria. All the operations were performed by a single senior surgeon. The flowchart is presented in Figure 1.
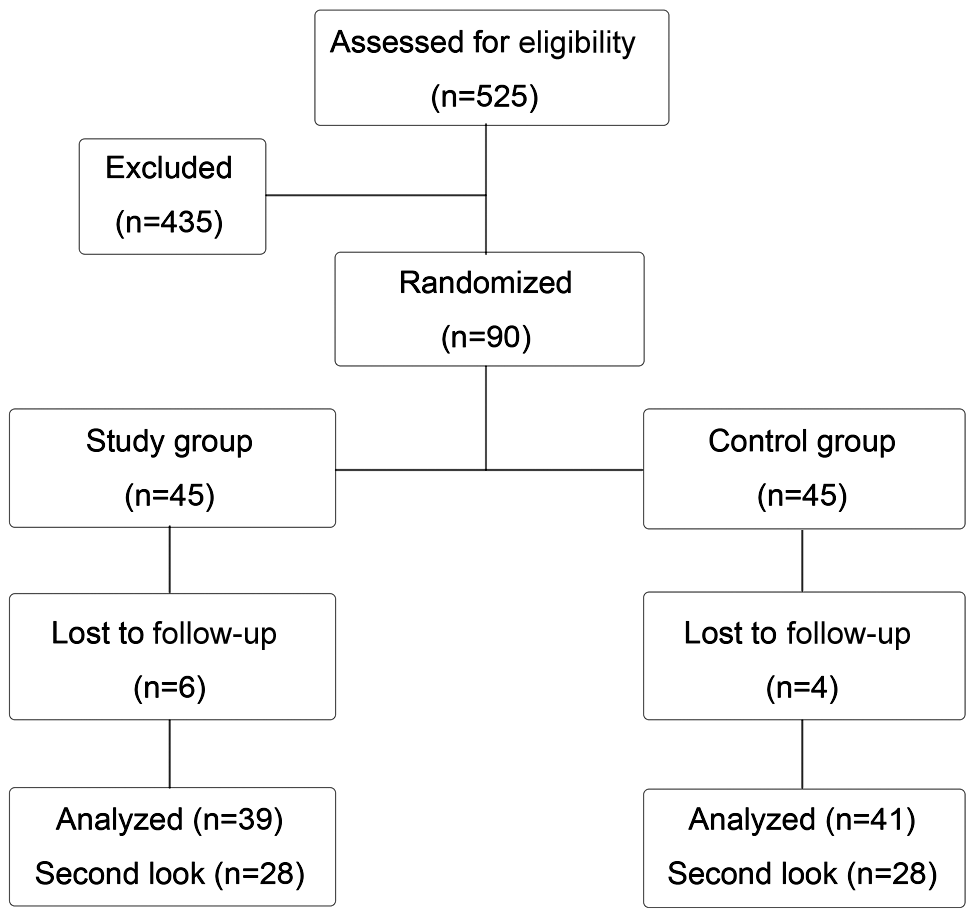
CONSORT flowchart of this trial.
The inclusion criteria included the following: (1) there was a complete ACL knee injury, (2) tibial insertion of the ACL remnant was intact, and (3) arthroscopy confirmed that the length and diameter were adequate: the remnant could be pulled to reach the femoral ACL insertion, and the remnant diameter was more than half of the native ACL. The exclusion criteria included (1) a bilateral ACL knee injury; (2) concurrent posterior cruciate ligament (PCL) injury, posterolateral corner (PLC) injury, or grade III medial collateral ligament (MCL) injury; (3) total meniscectomy; and (4) history of knee surgery. Patients who had a grade I or II MCL injury or who underwent partial meniscectomy, meniscus repair, or cartilage microfracture were not excluded in this study.
The enrolled patients were randomly assigned to a study group (remnant preservation ACLR, n = 45 patients) and a control group (standard ACLR, n = 45 patients) according to the odd or even number of the medical record identification. Demographic data of patients are listed in Table 1. The local ethical committee approved the study, and the patients gave their informed consent to participate.
Demographic Data and Preoperative Evaluations of the Patients a
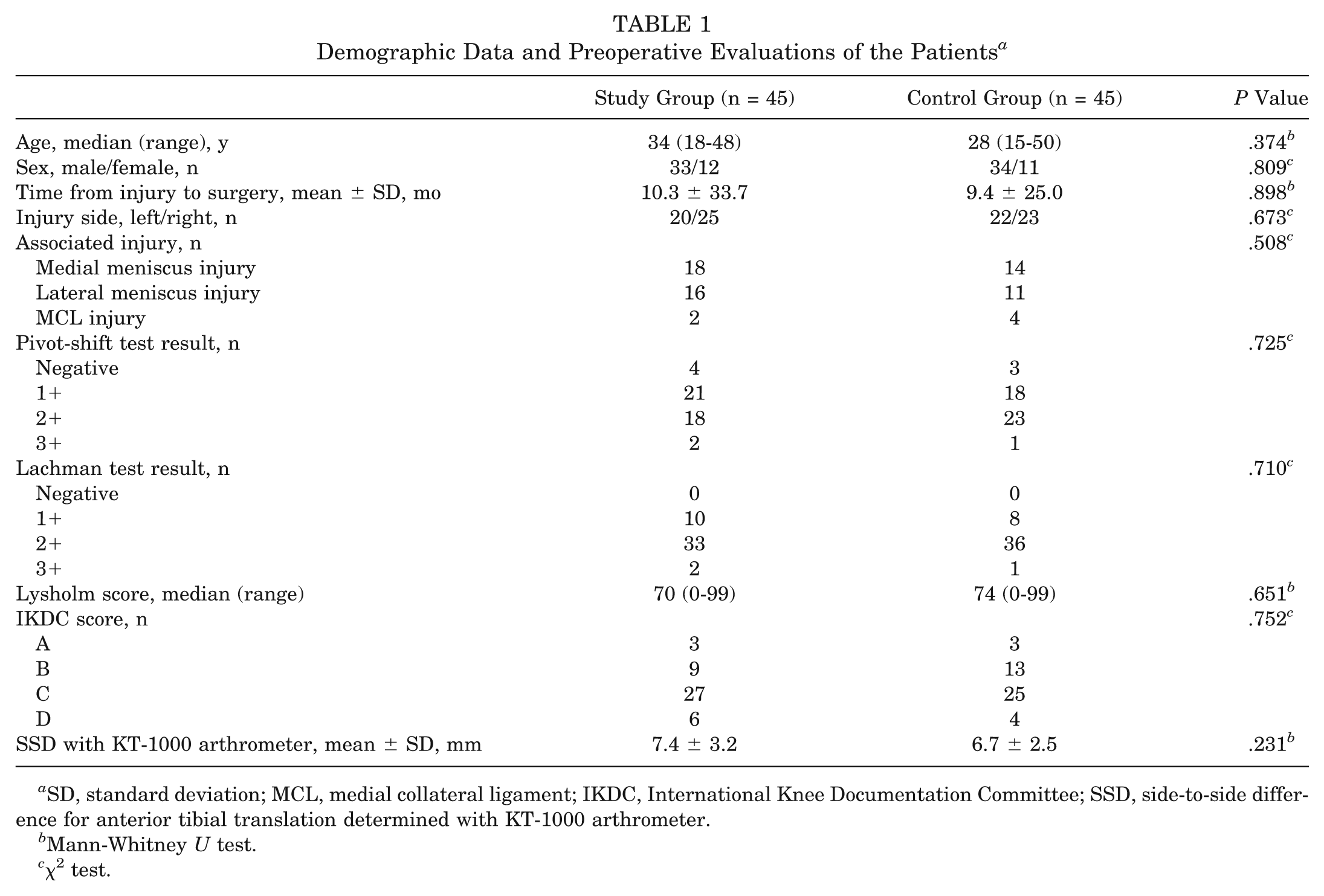
SD, standard deviation; MCL, medial collateral ligament; IKDC, International Knee Documentation Committee; SSD, side-to-side difference for anterior tibial translation determined with KT-1000 arthrometer.
Mann-Whitney U test.
χ2 test.
Surgical Techniques
First, examination under anesthesia was performed, including the Lachman test, pivot-shift test, and KT-1000 arthrometer (MEDmetric, San Diego, California) side-to-side difference measurement. During diagnostic arthroscopy, the native ACL was evaluated, and enrollment was determined according to the length and diameter of the ACL remnant.
The single-bundle ACLR technique with 4-strand allografts was used in both trial groups. The allografts were deep frozen (–80°C) and preserved with low-dose irradiation (1.5 Mrad) for secondary sterilization of the tibialis anterior or hamstring. The diameter of the graft was 8 to 9 mm. The RigidFix and IntraFix systems (DePuy Mitek, Raynham, Massachusetts) were used for the femoral and tibial side fixations, respectively.
The remnant preservation technique was well described by Ahn et al.3,4 A traction suture with a No. 3-0 polydioxanone synthetic (PDS) suture (Ethicon, Somerville, New Jersey) was placed at the proximal end of the remnant with a suture hook (Linvatec, Largo, Florida), and both the free ends of the suture were temporarily retrieved through the anteromedial portal. The suture protected the remnant tissue and provided a wide view during ACLR. With medial traction of the suture, the remnant was retracted medially, and elevation was performed to explore the ACL tibial insertion posterior to the remnant. The tibial tunnel was made at the center of the footprint using a 6-mm-diameter reamer and dilated into the final diameter. The femoral tunnel was drilled at the anatomic anteromedial bundle position through the anteromedial portal with the knee in 120° of flexion.
After the femoral and tibial tunnel formation, the leading suture of the graft and traction suture of the remnant were pulled into the femoral tunnel; both ends of the remnant suture were individually threaded into the superior and inferior cross pin sleeves inserted with a crochet hook (Linvatec). After graft passage, the graft and remnant were respectively tensioned, making the proximal end of the remnant reach the entrance of the femoral tunnel. The graft was fixed with the RigidFix, and the remnant suture was compressed into the transverse sleeves by cross pins. Finally, the graft was tensioned in slight flexion before IntraFix system fixation.
After tibial fixation, the remnant and articular portion of the graft were sutured together with 2 No. 3-0 PDS stitches to make them a unit (Figure 2).
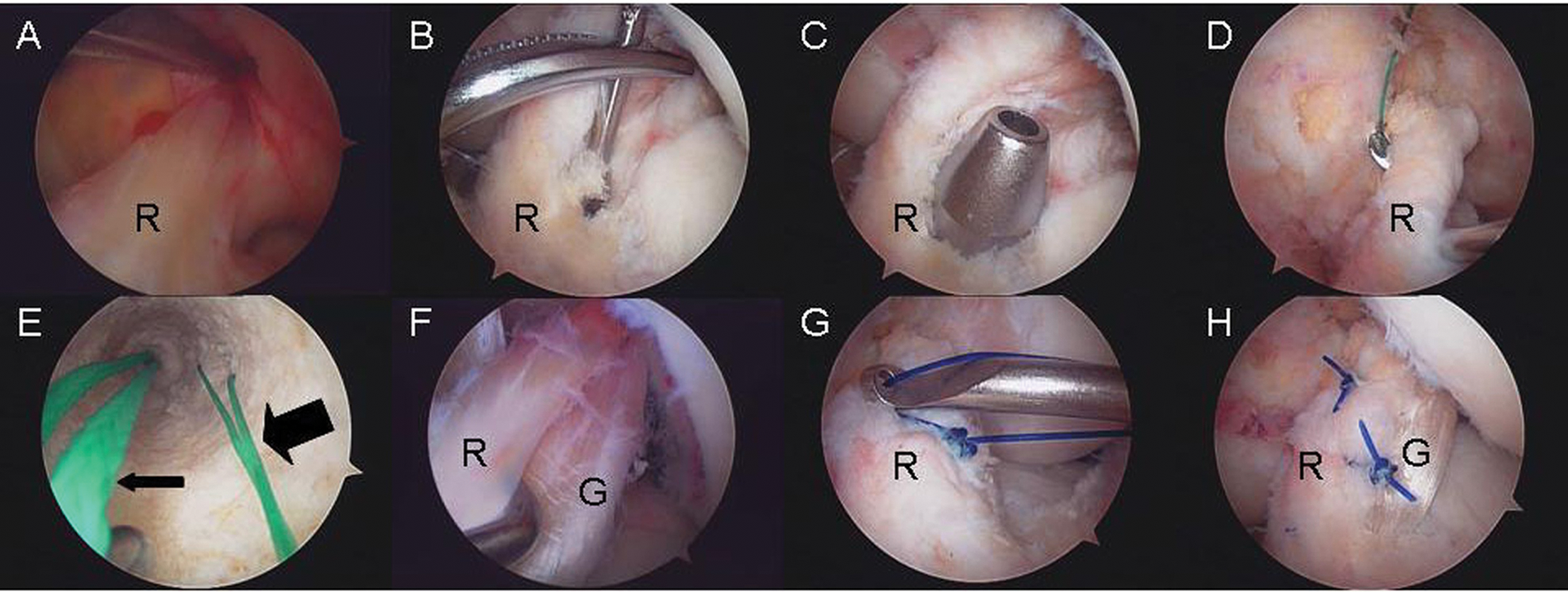
Arthroscopic lateral portal view of the left knee in 90° of flexion showing the remnant preservation technique for anterior cruciate ligament (ACL) reconstruction. (A) A complete ACL rupture with the remnant having an adequate length and diameter. (B) A traction suture was placed in the proximal end of the remnant. (C) Tibial tunnel position. (D) The tibial tunnel was dilated to protect the remnant. (E) Two leading sutures in the femoral tunnel. Thick arrow, leading suture of the graft; thin arrow, traction suture of the remnant. (F) Graft and remnant. (G) Remnant and graft were sutured together. (H) Final view after the remnant preservation technique. R, ACL remnant; G, graft.
In the standard technique, the tibial tunnel was made at the center of the ACL footprint and the femoral tunnel at the anatomic anteromedial bundle position. The femoral tunnel was prepared through the anteromedial portal.
Rehabilitation
All patients underwent the same rehabilitation protocol. A hinged knee brace locked in full extension was placed for 4 weeks. After 1 week, the brace was unlocked to allow passive range of motion from 0° to 90°, with emphasis on early passive extension stretching. Partial weightbearing was allowed at 4 weeks with the hinged brace remaining locked in full extension. Full weightbearing started at 6 weeks. Jogging was not permitted until 3 months postoperatively, and return to sports was not allowed until 9 to 12 months after surgery.
Clinical Scores
The standardized Lysholm and International Knee Documentation Committee (IKDC) grading systems were used at the 3-, 6-, 9-, 12-, 18-, and 24-month follow-ups.
Physical Examination
All the clinical evaluations of the patients were performed preoperatively and at least 2 years after surgery. The physical examination included assessment of range of motion, effusion, and ligament stability. The Lachman test was graded as negative (–), 1+, 2+, or 3+. The pivot-shift test was graded as negative (–), 1+ (glide), 2+ (clunk), or 3+ (locking). The KT-1000 arthrometer was used to measure the manual maximum side-to-side difference of anteroposterior translation in 30° of flexion.
Second-Look Arthroscopic Evaluation
Surgical indications of second-look arthroscopy were (1) patients who had no clinical symptoms but wanted to remove ACL graft tibial nonabsorbable IntraFix hardware (46 cases) and (2) patients who were symptomatic (9 patients, including 6 patients who had joint line tenderness at a meniscus tear and inadequate signaling at the meniscus repair site on follow-up magnetic resonance images, 2 patients with postoperative symptomatic clicking, and 1 patient with persistent postoperative joint effusion). We explained the purpose of the second-look arthroscopic procedure (evaluation of the ACL allograft and meniscus healing, debridement of scar tissues, etc) to all patients before surgery and received written consent. This study was approved by the institutional review board of our hospital.
During second-look arthroscopy, synovial coverage of the graft as well as cyclops lesions could be evaluated. The extent of synovial coverage was graded as 4 types 17 : A, normal (>75%); B, nearly normal (50%-75%); C, abnormal (25%-50%); and D, severely abnormal (<25%).
Proprioception Evaluation
The passive angle reproduction test, designed by Barrett, 7 is an examination to assess the proprioception recovery based on joint position sense. In the present study, the physical therapist was blinded. The same physical therapist who neither participated in surgery nor knew the grouping conditions completed measurement tests.
The examination steps were as follows. The patients sat on the Biodex detector (Shirley, New York), wore eyeshades and earplugs, and kept knees in a rotation-neutral position (Figure 3). The affected knee was flexed to 90° first, passively extended gradually with an angular velocity of 5 deg/s by the action of the Biodex detector, and then stopped at 15° of flexion. The movement was repeated several times until the patients were familiar with the setting angle. In the test, the affected knee was returned to 90° of flexion and then was extended by the action of the Biodex detector. When the patient felt the knee was at 15° of flexion, he or she would press the stop button. The true flexion angle of the knee was recorded as a test angle. The test angle minus the setting angle (15°) determined the difference value. The difference value was measured 3 times, and the mean value was used for analysis.
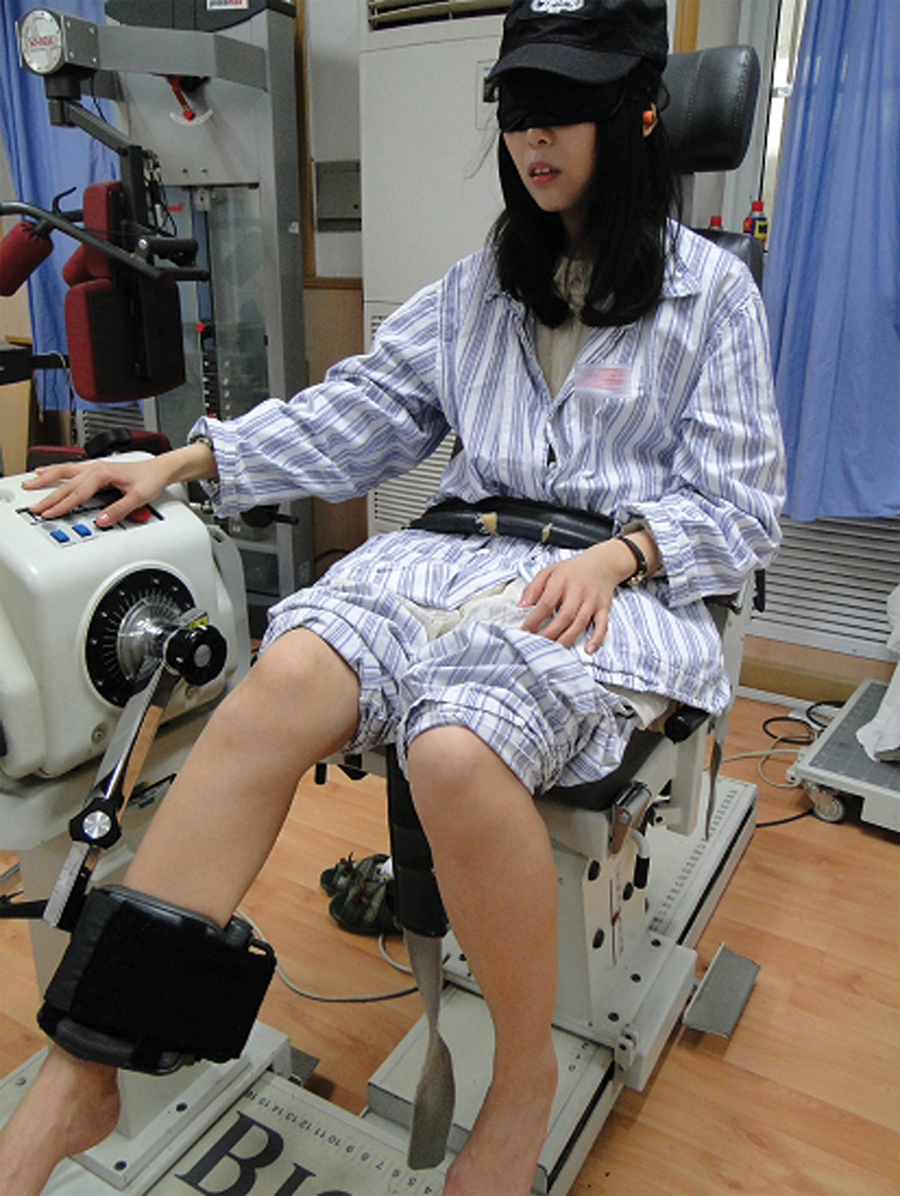
Illustrations of the passive angle reproduction test for proprioception measurements.
Statistical Analysis
All analyses were conducted on SPSS software for Windows, version 13.0 (Chicago, Illinois). For priori power analysis, the sample size was based on the Lysholm score, where 10 points between groups would be significant, and the expected standard deviation in the Lysholm score was 15 points; thus, for a power of .80, α = .05, a group size of 36 was required. To fulfill the demand of the statistical calculation, a group size of 45 was chosen for the study.
The χ2 test was used to compare the sex, injury side, associated injuries, data of the manual instability tests, IKDC objective examination rating, and data of the synovial coverage of the graft between the 2 groups. A paired t test was used for the comparison between preoperative and postoperative mean values of the KT-1000 arthrometer side-to-side difference. The Mann-Whitney U test was used to compare the age, the time from injury to surgery, the follow-up time, the data of the KT-1000 knee arthrometer, the Lysholm score, and the joint position sense between the 2 groups. The correlation analysis was conducted to determine the relationship between the length of time from injury to surgery and the outcome in the study group (Lysholm score, KT-1000 arthrometer, synovial coverage of the graft, and passive angle reproduction test). The level of significance was below .05.
Results
Overall, 80 of 90 patients (88.9%) were available for at least 2 years’ follow-up: 39 patients in the study group and 41 patients in the control group; 10 patients were lost to follow-up from this study. The mean ± standard deviation follow-up time was 25.7 ± 2.3 months. Outcomes of both groups of patients are shown in Table 2. Correlation analysis demonstrated no relationship between the length of time from injury to surgery and the outcome in the study group regarding median Lysholm score (P = .328), KT-1000 arthrometer score (P = .230), synovial coverage of the graft (P = .276), and passive angle reproduction test (P = .114).
Outcomes in Both Groups a
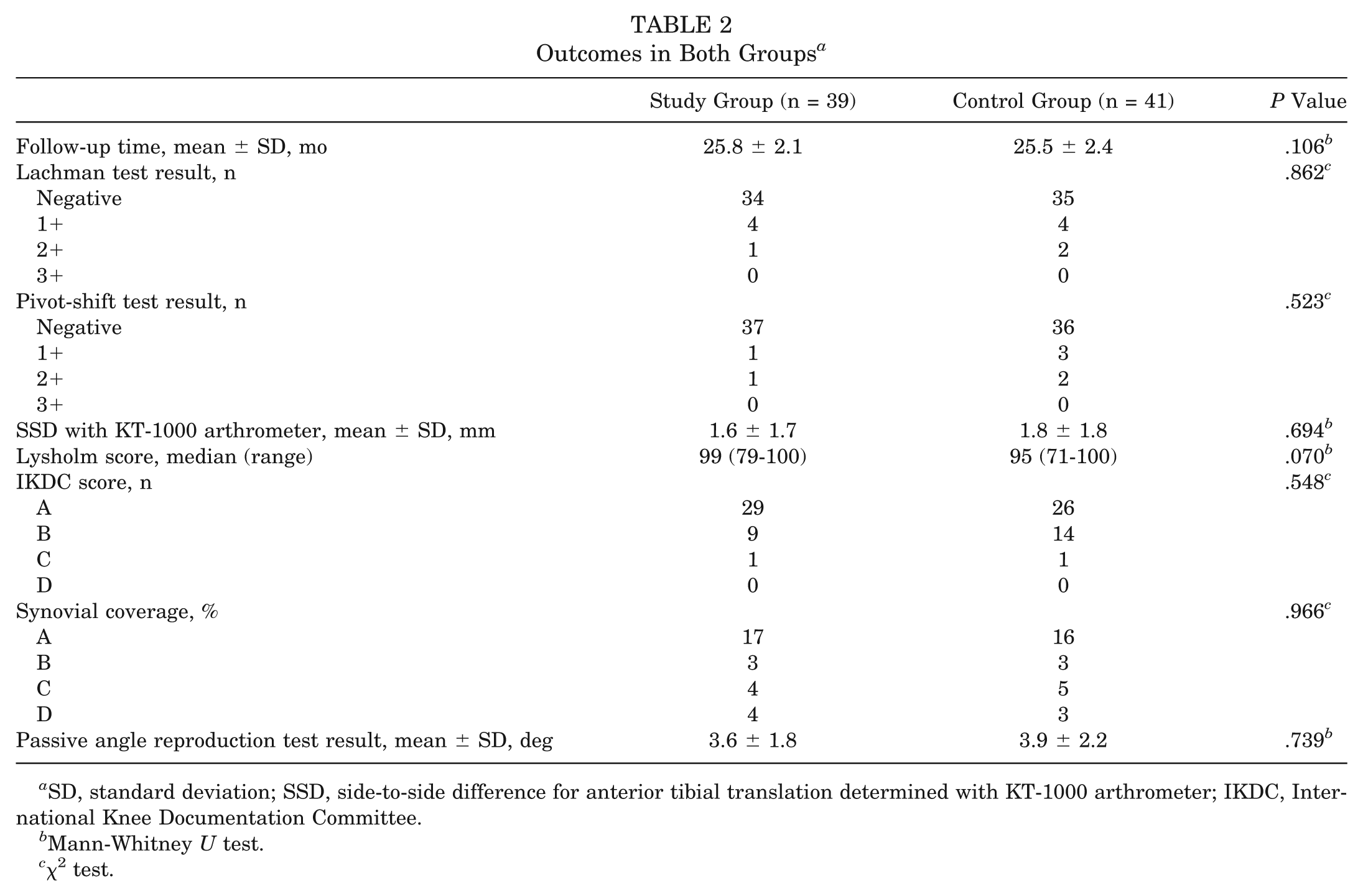
SD, standard deviation; SSD, side-to-side difference for anterior tibial translation determined with KT-1000 arthrometer; IKDC, International Knee Documentation Committee.
Mann-Whitney U test.
χ2 test.
Clinical Scores
The median Lysholm scores at different time points are shown in Figure 4. The latest median score was 99 (range, 79-100) in the study group and 95 (range, 71-100) in the control group at the last follow-up (P = .07). All patients had an IKDC grade of C or D preoperatively. Postoperatively, the IKDC grade was A or B in all but 2 patients at follow-up (1 in the study group and 1 in the control group). There were no significant differences in the median postoperative Lysholm score (P = .07) and IKDC grade between the 2 groups (P = .548). The median tourniquet time was 90 minutes in the study group and 75 minutes in the control group; the difference was statistically significant (P = .002).
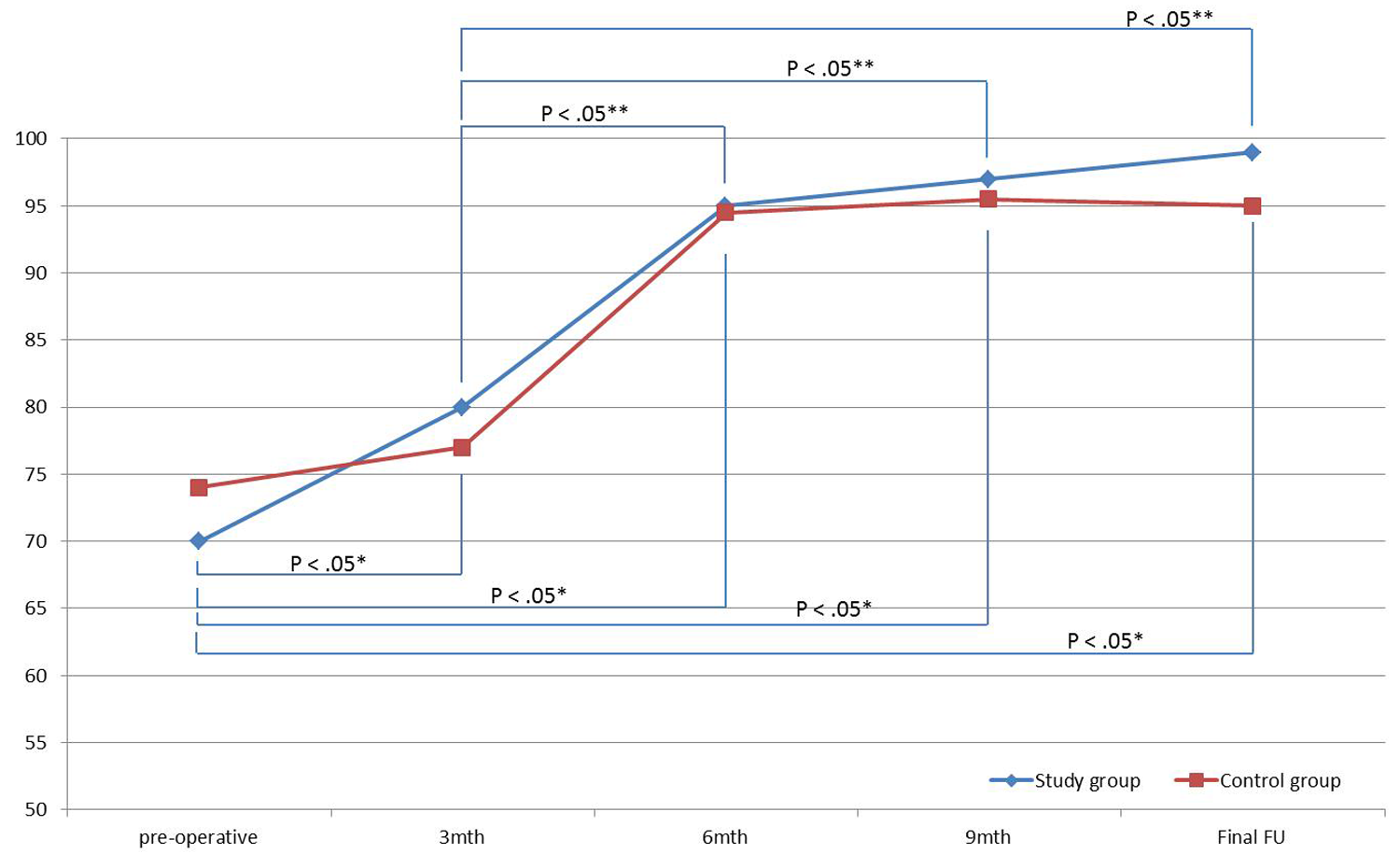
Illustration of the median Lysholm scores at different time points in the study group. There was a statistically significant difference preoperatively and 3-month, 6-month, 9-month, and final follow-ups postoperatively (*P < .05). A significant difference was also found between 3-month, 6-month, 9-month, and final follow-ups postoperatively (**P < .05).
Physical Examination
In both groups, the postoperative average KT-1000 arthrometer measurement was significantly reduced: from 7.4 ± 3.2 mm preoperatively to 1.6 ± 1.7 mm postoperatively (P < .05) in the study group and from 6.7 ± 2.5 mm preoperatively to 1.8 ± 1.8 mm postoperatively (P < .05) in the control group. The difference in postoperative stability (pivot-shift test, Lachman test, and KT-1000 arthrometer was not significant between the 2 groups (P = .523, P = .862, and P = .694, respectively). Postoperatively, all of the patients showed full extension and flexion of the knees.
Second-Look Arthroscopic Evaluation
Among the 80 patients who were available for final follow-up, 55 (69%) underwent second-look arthroscopic evaluation: 72% of patients (28/39) in the study group and 66% (27/41) in the control group. In terms of synovial coverage of the graft, 71.4% (20/28) of patients in the study group and 70.4% (19/27) in the control group had normal/nearly normal coverage (coverage of 50% of the graft) (Figure 5). There was no significant difference between the 2 groups (P = .966).
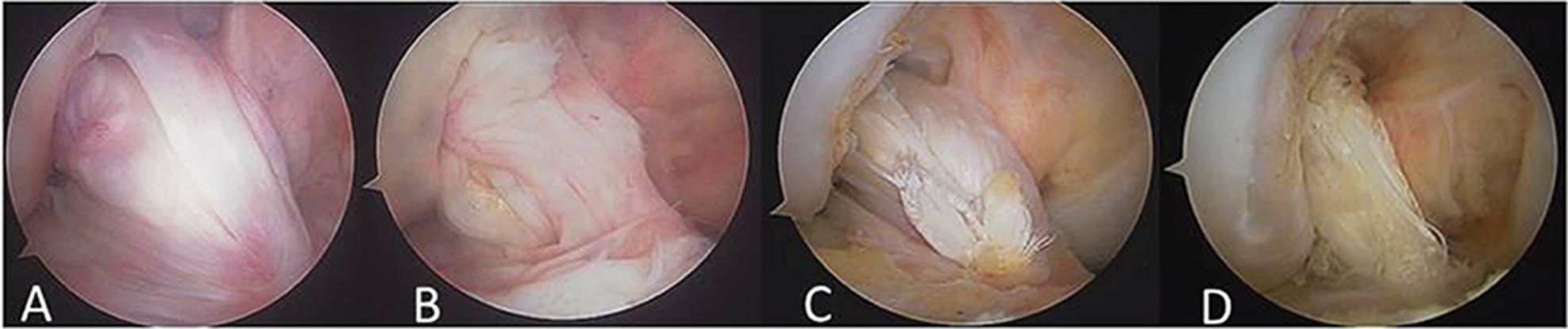
Arthroscopic lateral portal view of the right knee in 90° of flexion showing the synovial coverage grading: A, synovium covers >75% of the graft; B, 50% to 75%; C, 25% to 50%; and D, <25%.
In each group, cyclops lesion formation occurred in 3 patients, and the lesions were resected subsequently.
Proprioception Evaluation
Of the 80 patients, all underwent the proprioception evaluation. The passive angle reproduction test was performed at 3, 6, 9, 12, 18, and 24 months after surgery. There was no difference between both groups at final follow-up (P = .739).
Discussion
The primary purpose of this study was to compare the clinical outcome of remnant preservation reconstruction with standard reconstruction for ACL ruptures. Preoperatively, there were no significant differences in demographics between the 2 groups. The most important finding of the present study was that the results of remnant preservation reconstruction were not superior to standard reconstruction for all objective and subjective outcome measurements, including knee stability, graft revascularity, and knee joint proprioception. The original hypothesis proved to be incorrect.
According to the literature, most ACLs are ruptured in the proximal half; the thick and abundant tibial-based remnant bundle could be encountered during ACLR surgeries. Crain et al 9 reported that at least 50% of patients with an ACL injury had some remnant scar tissue that could be classified into 4 types. In addition, there were vascularity and mechanoreceptors reported to be located in the subsynovial layer near the tibial insertion site of ACL fibers.6,16 Therefore, some authors have attempted to preserve the remnant in addition to the reconstructed graft, assuming that the remnant may have the potential to enhance the revascularization, incorporation, and reinnervation and, more importantly, lead to better postoperative biomechanical stability of the knee joint.1,4,11,14,15,17 Lee et al 15 reported better proprioceptive and functional outcomes in patients with a preserved remnant more than 20% in length than those with less than 20% in a group of 16 patients. Ahn et al3,4 described a remnant preservation and tensioning technique and reported favorable clinical outcomes by evaluating knee stability, second-look arthroscopy, and postoperative magnetic resonance imaging (MRI). Even though, until now, the relevant publications were mainly case series studies with few control groups included,1,12,15,17 Gohil et al 12 showed level I evidence that minimal debridement of the residual stump of the ruptured ACL leads to earlier revascularization of ACLR in humans. However, the study was limited by a MRI study without quantification of the remnant as well as lacking proprioception assessments. Therefore, high quality–designed, prospective, randomized controlled scientific research with comprehensive assessment of postoperative knee stability, graft revascularization, and knee proprioception is still needed.
The major concerns regarding remnant preservation ACLR are surgical timing and remnant amount. Reider et al 20 believed that the time interval from injury to surgery could influence the postoperative recovery of proprioception. Denti et al 10 observed that after the ACL completely ruptured, mechanoreceptors could exist for 3 months and then gradually disappear over time. However, Georgoulis et al 11 reported that mechanoreceptors could still be found even 3 years after injury in patients with an ACL remnant adapted to the PCL. Ahn et al 4 believed that early reconstruction would facilitate preserving more remnant tissue and mechanoreceptors and thereafter assumed to yield good clinical results. In our study group, nevertheless, we failed to determine any trend/relationship between the length of time from injury to surgery and outcome in terms of Lysholm score, KT-1000 arthrometer score, synovial coverage, and proprioception evaluation. Regarding the issue of preserved remnant volume, Lee et al 15 concluded that patients with a preserved remnant more than 20% in length had better proprioceptive and functional outcomes than those with less than 20%. In both groups of the present study, we designed the inclusion criteria mainly based on sufficient remnant amount quantified by length and diameter. In our clinical practice, a number of proximal rupture cases with thick and abundant remnants could still be found even in the chronic phase. In contrast to Lee et al, 15 favorable clinical results with statistical significance could not be observed between the 2 groups. Therefore, although repair of the ACL remnant with adequate volume seems to be reasonable in an acute setting, which is usually considered within 3 weeks after injury, the potential contribution of the ACL remnant to the fate of the ACL graft is still debatable. To justify the true significance of the remnant, further study is required.
Improving graft revascularization is one of the primary goals of the remnant preservation technique. Some authors have reported that cases with more graft coverage showed better incorporation on follow-up MRI and furthermore correlated with favorable results. Adachi et al 1 confirmed favorable remodeling of the graft covered with synovium in 12 patients who underwent second-look arthroscopy (40 patients in the study group). They believed that as the remnant was preserved, a portion of blood vessels from the tibial attachment were also preserved, which had a good influence on revascularization of the graft. Ochi et al 18 performed selective single anteromedial bundle or posterolateral bundle ACLR; postoperative MRI showed good incorporation of the preserved remnant bundle with the graft. In addition, second-look arthroscopy at 1 year after surgery verified that 70.8% of patients showed the previously preserved remnants were well maintained with good tension. Lee et al 17 reported the arthroscopic finding that 62.5% and 72.3% of the patients with a bone-tendon-bone allograft and a tibialis anterior tendon allograft, respectively, had normal/nearly normal synovial coverage. Ahn et al 4 performed second-look arthroscopy in 62% of patients who underwent remnant preservation ACLR and reported 91% with fair synovialization of the ACL graft. Gohil et al 12 inferred that minimal debridement (remnant of the ACL, notch synovium, ligamentous mucosa, and fat pad were left untouched as much as possible) leads to earlier revascularization of the ACL graft at 2 months using MRI assessment. Comparable with these results, in the present study group, normal/nearly normal synovial coverage of the graft (type A or B) consisted of 71.4%. However, in the control group, the corresponding rate was also as high as 70.4%, which was not statistically different from the study group. This interesting result implies that synovial coverage appears to form automatically after ACLR, even without preservation of the remnant, which was inconsistent with other reports and questioned the contribution of the remnant to revascularization of the graft.
It is noteworthy that some authors1,4,17,18 prefer second-look arthroscopy as an evaluation tool for assessment of the amount of preserved remnant tissue or synovialization of the graft. However, second-look arthroscopy would have made studies more invasive and more costly and increased the reoperation rate. These drawbacks restrict its feasibility. Further study, which is more objective, noninvasive, and patient compliant, should be utilized to define the true synovial coverage status.
Many authors2-4,11,15,16,18 have considered that the regeneration of mechanoreceptors could be accelerated by revascularization of the graft and that the recovery of knee proprioception function could be promoted by the surviving mechanoreceptors within the ACL remnant and the regenerated mechanoreceptors. Nevertheless, few human studies that conducted clinical proprioception testing have been reported.1,15 Adachi et al 1 used a hamstring tendon autograft for augmentation ACLR with the remnant-preserving technique and showed that the postoperative inaccuracy joint position sense was 0.7° ± 0.7° in the remnant group versus 1.7° ± 1.2° in the standard ACLR group (P < .05). Lee et al 15 reported that patients with a remnant more than 20% of its length had better proprioceptive results than those with less than 20% regarding the threshold to detection of passive motion at 30° of knee flexion and reproduction of passive positioning at 15° and 30°. In the present study, for the passive angle reproduction test, we set up the joint position at 15° of flexion and had the knee joints moved from 90° in the direction of extension, which has been shown to be significantly more sensitive. 8 However, there was no significant difference between the 2 groups, which is inconsistent with the results of Adachi et al 1 and Lee et al. 15 One of the possible reasons for the discrepancy between the results may be the difference between allografts and autografts. Kim et al 13 conducted a histological study in 11 patients who underwent ACLR using Achilles tendon allografts and concluded that mechanoreceptors would not grow in Achilles allografts after ACLR. Furthermore, multiple factors, not only limited to the ACL itself but also to the joint capsule, meniscus, surrounding muscle, and even skin, can influence the final results and make it impossible to directly compare the studies in the literature. In addition, despite many reports on postreconstruction recovery of proprioception function being published in the literature,1,7,11,14,19 until now, there has been a lack of a consolidated guideline for evaluation. In the future, more accurate and reproducible equipment as well as histological assessment should be introduced to detect the true in vivo status of proprioception function.
Although there are still some controversies regarding the function of the remnant, one should always bear in mind that the biomechanical stability of the knee joint must be the primary purpose of performing a successful ACLR. Some authors believe that preservation of the remnant for ACLR has a certain influence on the stability of the knee joint. Kim et al 14 reported that the postoperative mean side-to-side difference was 1.67 mm on KT-2000 arthrometer measurement in the patients who underwent double-bundle ACLR with the remnant-preserving technique. Similarly, Adachi et al 1 showed that KT-1000 arthrometer results in patients who underwent remnant preservation ACLR were 0.7 ± 1.8 mm versus 1.8 ± 2.1 mm in the standard ACLR group (P < .05). Ahn et al 4 reported significantly improved postoperative stability with 1.8 ± 2.0 mm on the KT-2000 arthrometer measurement, 94% negative/1+ on the Lachman test, and 89% negative on the pivot-shift test. Our results in both groups were comparable with these studies: 1.6 ± 1.7 mm and 1.8 ± 1.8 mm with the KT-1000 arthrometer, 97% and 95% negative/1+ Lachman test results, and 95% and 88% negative pivot-shift test results, respectively. However, no statistically significant differences were found in stability between the 2 groups. Possible explanations were the following: (1) The dominant postoperative stability was provided by the ACL graft, and the strength of the remnant was not large enough to contribute a significant difference. (2) The postoperative tension of the remnant was not adequately maintained, as shown in cases of abnormal/severely abnormal synovial coverage. (3) Inferior incorporation between the remnant and graft was far beyond our anticipation. Further histological study should be conducted to verify the sequence of the preserved remnant and its relationship with the ACL graft.
In considering the clinical outcome of remnant preservation ACLR, whether the type of the graft might possibly affect the results still remains unknown. Lee et al 17 compared ACLR surgery by use of bone–patellar tendon–bone allografts, tibialis anterior tendon allografts, and hamstring tendon autografts with respect to objective knee testing measures and second-look arthroscopy. The authors concluded that the autograft group had better synovial coverage on second-look arthroscopy (90.7% normal/nearly normal), and the group with better synovial coverage on second-look arthroscopy presented better clinical results on the IKDC objective examination form. Kim et al 13 reported there were no newly ingrown mechanoreceptors in ACL Achilles allografts. However, in both of the above studies, the authors did not use the remnant preservation technique for ACLR. In our series, an allograft was used in both groups, and synovial coverage extent graded A and B were 71.4% and 70.4%, respectively, which are comparable with the tibialis anterior tendon allograft group in the study of Lee et al 17 (72.3%) but lower than that in the autograft group (90.7%). A few authors described the remnant preservation technique of ACLR using autografts and already reported positive proprioception results,1,14 whereas in our study, the proprioception result was negative. Therefore, before coming to a conclusion, there should be further study on the correlation between the graft and clinical outcome in terms of extent of revascularization, reinnervation, and mechanical stability, as well as functional activity.
Strengths and Limitations
This study had the following strengths: (1) prospective, randomized controlled study; (2) the quantified inclusion criteria for the remnant eliminated the bias induced by the remnant’s quality; (3) a comprehensive assessment, including subjective score, stability, and proprioception, was conducted; and (4) the sample size of this study fulfilled the demand for statistical calculation.
The limitations of the study included the following: (1) the reoperation rate was high because of second-look arthroscopic evaluation of graft synovial coverage; (2) the method for randomization was not perfect; (3) the synovial coverage assessment method is subjective, without accurate measurement. Furthermore, only a portion (69%, 55/80) of patients participated in synovial coverage follow-up, which may introduce substantial bias; (4) the method for proprioception measurement was simple; (5) the follow-up period was relatively short; and (6) other abnormalities affected the scores, such as allografts in the study, which might influence the incorporation between the remnant and graft.
Conclusion
The short-term study showed that, in terms of postoperative knee stability, synovial coverage of the graft, and knee proprioception recovery, remnant preservation ACLR using allografts had no evident advantages in clinical outcome over the standard technique. Based on the results of no obvious superiority, the clinical relevance should be the following: there is less need to perform a remnant-preserving and tensioning procedure, which is time consuming and technique demanding in ACLR. Instead, it may be more prudent to perform a standard technique, either anatomic single-bundle or double-bundle ACLR. However, in the future, studies with long-term follow-ups and a more sensitive examination method would be of great value to disclose the true function of the ACL remnant.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.