
Abstract
Background:
The early stages of spondylolysis are extremely difficult to diagnose on plain radiography. Although several studies have examined changes in active spondylolysis on magnetic resonance imaging (MRI), no studies to date have determined the onset frequency of active spondylolysis detectable on MRI but occult on plain radiography. Moreover, the clinical features of active spondylolysis described in the literature do not facilitate the differentiation of this condition from other causes of low back pain.
Purpose:
This study aimed to evaluate the usefulness of MRI in diagnosing active spondylolysis early and in determining the prevalence of active spondylolysis in cases where findings were not detected on plain radiography. In addition, specific clinical features to aid in the early detection of active spondylolysis were evaluated.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients were 200 consecutive young athletes (144 boys and 56 girls; mean age, 14.1 ± 1.5 y) with low back pain. All patients were examined by plain radiography (188 with negative findings and 12 with unclear findings of spondylolysis) and MRI. Computed tomography (CT) was performed only for patients with high intensity changes of the pedicle observed on MRI. The presence or absence of low back pain was examined during lumbar spine extension and flexion. The Kemp test on the right and left sides and percussion of the vertebral spinous process were also performed.
Results:
Ninety-seven (48.5%) patients showed evidence of active spondylolysis on MRI, findings that had been missed by plain radiography. These pars defects were organized into the following categories based on CT findings: nonlysis stage, 52; very early stage, 37; late early stage, 22; progressive stage, 10; and terminal stage, 0. No significant physical examination factors were identified that could assist in the early detection of active spondylolysis.
Conclusion:
The MRI results suggest a high rate of active spondylolysis in young athletes with low back pain who test negative for spondylolysis on plain radiography. Magnetic resonance imaging appears to be useful in the early diagnosis of active spondylolysis, especially as we found no significant physical examination factors that could assist in early detection.
Lumbar spondylolysis is a defect of the pars interarticularis that commonly occurs in young athletes. Although multiple factors may be involved in its occurrence, spondylolysis is generally believed to be caused by a stress fracture of the pars interarticularis as a result of repetitive extension activities.8,31,36,45 The progression of active spondylolysis to nonunion has been associated with an increased incidence of spondylolisthesis,20,36 which can be avoided by repairing the pars defect with bony union. Spondylolysis and spondylolisthesis are not necessarily related to lumbago in adult patients,3,27,44 but in young athletes, spondylolysis is a common cause of low back pain. There are several reports that young athletes with spondylolysis or spondylolisthesis had a higher incidence of low back pain than those with no abnormal radiographic results.23,24,35
As previous studies have reported a significant correlation between the stage of the defect and the success of bony union,14,36,39,41,42 the early detection and treatment of spondylolysis are clearly important to achieve bony union. Although some patients do not experience pain even with bony nonunion, it would be more beneficial to aim for bony union, which can be better expected with early detection and treatment. However, diagnosing the early stages of spondylolysis on plain radiography is difficult,17,37 even when the oblique view is used, 9 because the angle or site of the defect in the pars interarticularis is inconsistent and the fracture lines are sometimes faint.
Recent studies have found bone scintigraphy, single-photon emission computed tomography (SPECT), and magnetic resonance imaging (MRI) to be useful in the early diagnosis of spondylolysis.4,6,12,14,22,32,39 Among these imaging techniques, MRI offers many advantages, such as its noninvasive nature and the absence of radiation exposure, the latter of which is of particular importance in spondylolysis because spondylolysis occurs mainly during growth periods.5,13 Although several studies have examined MRI-documented changes in active spondylolysis, no studies to date have determined the onset frequency of active spondylolysis detected on MRI in cases that were occult on plain radiography.
In addition, the clinical features of active spondylolysis previously described in the literature, such as pain on the 1-legged hyperextension test or pain throughout the lumbar spine range of motion, do not facilitate the differentiation of this condition from other causes of low back pain.7,32,35 Having a validated physical examination for active spondylolysis would help to diagnose active spondylolysis before imaging.
The aims of this study were therefore to evaluate the usefulness of MRI in diagnosing early-stage active spondylolysis and in determining its prevalence in cases where findings were not detected initially on plain radiography. In addition, specific clinical features of active spondylolysis at the first medical examination were evaluated to determine whether they could aid in early detection.
Materials and Methods
A prospective cohort design was used in this study, which involved 200 consecutive patients who presented to our clinic from May 2009 to May 2011 with low back pain. Patients were 144 boys and 56 girls (age, mean ± standard deviation [SD], 14.1 ± 1.5 y; range, 10-18 y) who met the following inclusion criteria: low back pain without neurological abnormalities in the lower limbs, age ≤18 years, actively participating in sports, and no (or unclear) findings of spondylolysis on plain radiography. “Unclear” cases were defined as suspected spondylolysis but with no clear fracture line evident. Patients with early-stage lumbar spondylolysis diagnosed by MRI at another institution or patients who had clear spondylolysis or spondylolisthesis detected by radiography were excluded. This study was approved by the institutional review board at Asakura Sports & Rehabilitation Clinic, and all patients provided informed consent.
All patients were examined with plain radiography and MRI. Radiography was performed with the patients in the recumbent position, and 4 views of the lumbar spine were obtained at the initial consultation: posterior-anterior, lateral, and right and left oblique. Magnetic resonance imaging was performed with a 0.3-T open field imager (AIRIS Elite, Hitachi Medical Corp, Tokyo, Japan). Five images were recorded for each patient, with the following MRI sequences: sagittal view of the lumbar spine with (1) sagittal T2-weighted images (echo time [TE], 110 milliseconds; repetition time [TR], 3200 milliseconds; slice thickness, 5 mm; interslice gap, 1 mm) and (2) sagittal short tau inversion recovery (STIR) images (TE, 17 milliseconds; TR, 2800 milliseconds; slice thickness, 5 mm; interslice gap, 1 mm); axial view of the pedicle of each vertebral body (L3-L5) using 2 slices and pedicle of the L2 vertebral body and each intervertebral disc using 1 slice (Figure 1), with (3) axial T1-weighted images (TE, 21 milliseconds; TR, 450 milliseconds; slice thickness, 4 mm; interslice gap, 1 mm), (4) axial T2-weighted images (TE, 110 milliseconds; TR, 3500 milliseconds; slice thickness, 4 mm; interslice gap, 1 mm), and (5) axial STIR images (TE, 30 milliseconds; TR, 4000 milliseconds; slice thickness, 4 mm; interslice gap, 1 mm). This protocol enabled us to investigate not only active spondylolysis but also other pediatric spinal disorders such as disc herniation, disc degeneration, and apophyseal ring tear. Active spondylolysis was defined as high signal intensity in the pedicle region on the STIR axial and sagittal images, as reported previously (Figure 2). 39
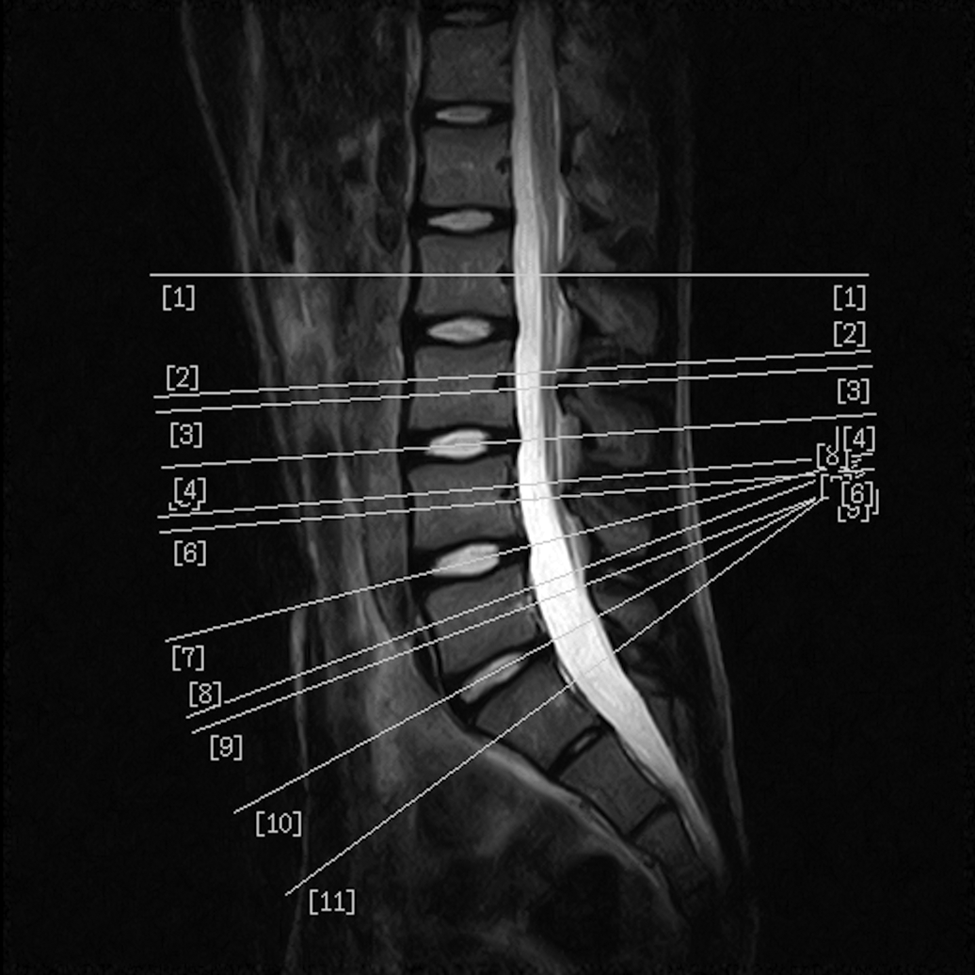
Magnetic resonance imaging sequence in the axial view: white lines indicate the plane of axial slices for screening lumbar disorders in young athletes.

Magnetic resonance imaging scan of the lumbar spine in a 15-year-old male athlete. (A) Sagittal short tau inversion recovery image showing high signal intensity in the L4 pedicle (arrow). (B) Axial slice showing high signal intensity in the right pedicle. White arrow indicates an active spondylolysis lesion.
In total, 97 patients exhibited active spondylolysis on MRI. Of these, 92 patients from this group consented to examination by CT (Auklet, Toshiba Medical Systems, Tokyo, Japan). The CT scans were obtained with a reverse gantry angle in the plane parallel to the pars interarticularis only for the vertebral body corresponding to the area of the high intensity change seen on MRI (Figure 3). The images were acquired in 2-mm-thick slices and at 2-mm intervals. The defects were classified into the following 5 stages according to the classification systems of Yamane et al 46 and Sairyo et al 39 : nonlysis, very early, late early, progressive, and terminal (Figure 4). Lysis was not visible in the nonlysis stage, a hairline was visible in the partial CT slice in the very early stage, a clear hairline was visible in all of the CT slices in the late early stage, and a gap was visible in the progressive stage. Terminal-stage defects were characterized by pseudarthrosis.
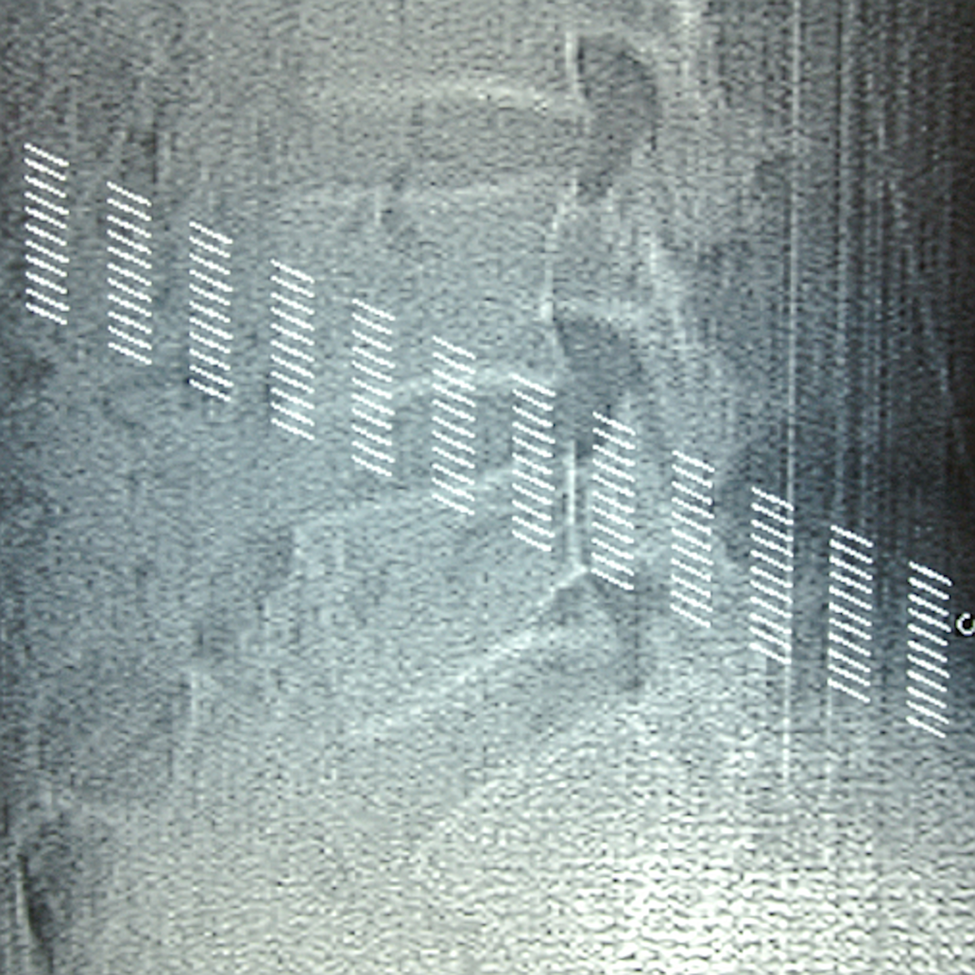
Computed tomography scans with reverse gantry angles on the plane parallel to the pars interarticularis were performed only for the affected vertebral body. White lines indicate the plane of the scans.

Stages of pars defects: (A) nonlysis stage, (B) very early stage, (C) late early stage, (D) progressive stage, and (E) terminal stage. White arrows indicate spondylolysis lesions.
During physical examination, the following 5 factors were assessed: (1) presence or absence of low back pain during lumbar spine extension, (2) presence or absence of low back pain during lumbar spine flexion, (3) right-sided Kemp test, (4) left-sided Kemp test, and (5) percussion of the vertebral spinous process. The Kemp test involves lateral flexion and extension of the trunk while standing upright on both legs (Figure 5) to confirm the presence or absence of low back pain in this maneuver. Pain on each of these physical examinations was categorized into 1 of 3 levels: no pain, slight pain, or strong pain. For statistical analysis, physical examination data were entered in an Excel spreadsheet (Microsoft, Redmond, Washington) and were later exported to SAS-JMP (SAS Institute Inc, Cary, North Carolina). Logistic regression analysis was then performed. An analysis of the physical examination data revealed missing values in some patient cases; therefore, only the data from patients for whom all data were available were included in the statistical analysis.
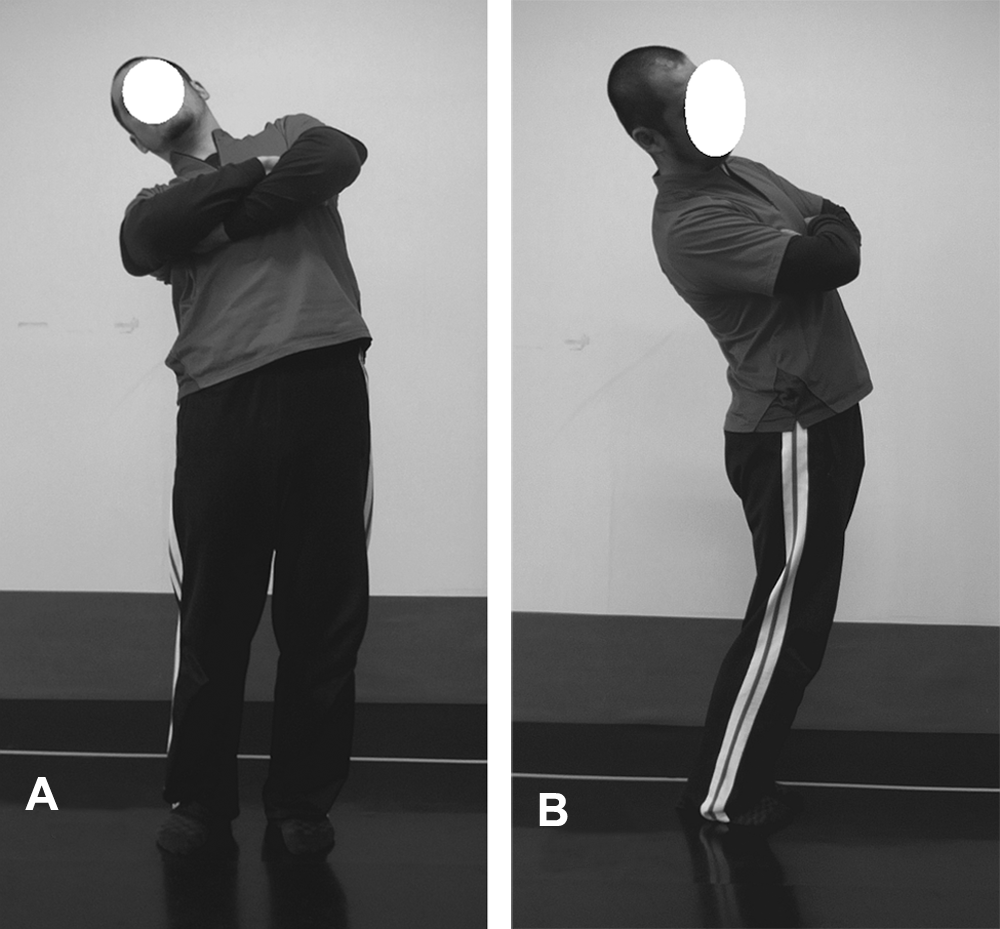
Kemp test on the right side to confirm the presence or absence of low back pain. (A) Front view and (B) lateral view.
Results
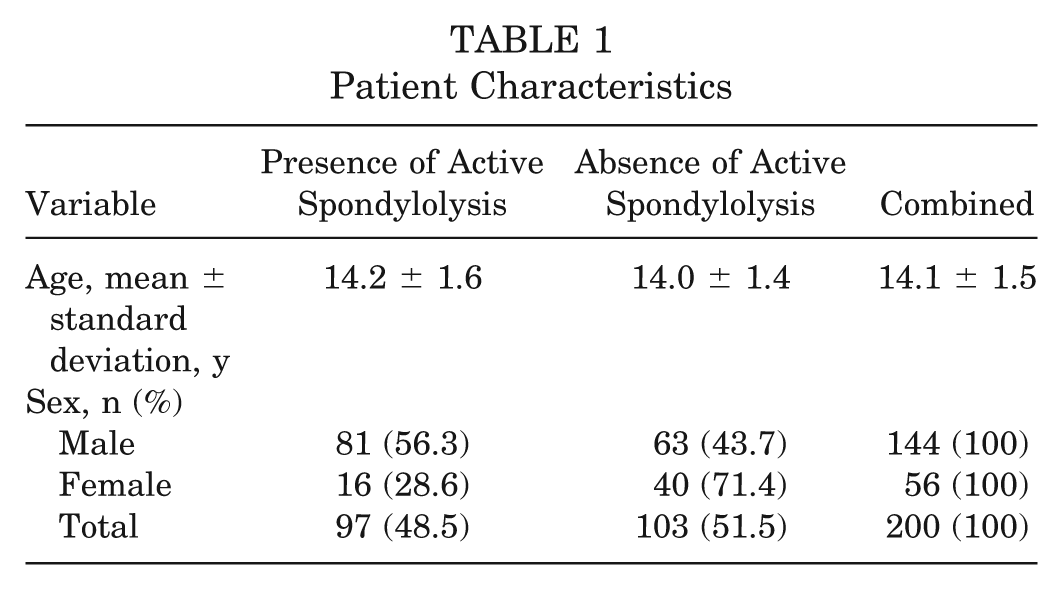
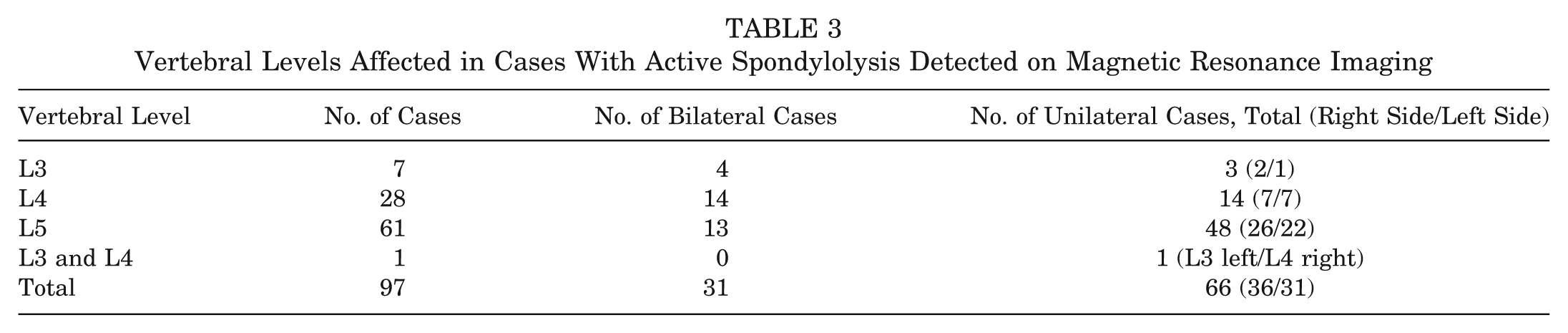
The right and left pars interarticularis were studied separately between L2 and L5 (1600 pars interarticularis examined in total). Abnormal evidence of active spondylolysis on MRI was found in 129 (8.1%) pars interarticularis, that is, in 97 (48.5%) of the 200 patients (Table 1). On plain radiography, 188 of the 200 patients had no findings of spondylolysis, and the remaining 12 had unclear findings of spondylolysis. Evidence of active spondylolysis on MRI was found in 86 (45.7%) of the 188 patients with negative findings on plain radiography and in 11 (91.7%) of the 12 patients with unclear findings on plain radiography. The sports-related activities of the patients are shown in Table 2. Active spondylolysis was most apparent in those playing baseball, 37 (61.7%) of 60 cases, followed by soccer in 25 (53.2%) of 47 cases and then basketball in 15 (50%) of 30 cases. There were a small number of cases also seen for other sports activities. The affected vertebral levels were at L3, L4, and L5 in 7, 28, and 61 patients, respectively. We detected bilateral active spondylolysis on MRI in 31 patients and unilateral active spondylolysis in 66 patients. Among the unilateral lesions, 31 and 36 were on the left and right sides, respectively (1 patient had multiple-level unilateral spondylolysis at L3 and L4) (Table 3).
Patient Characteristics
Cases of Active Spondylolysis According to Patients’ Sports-Related Activities a
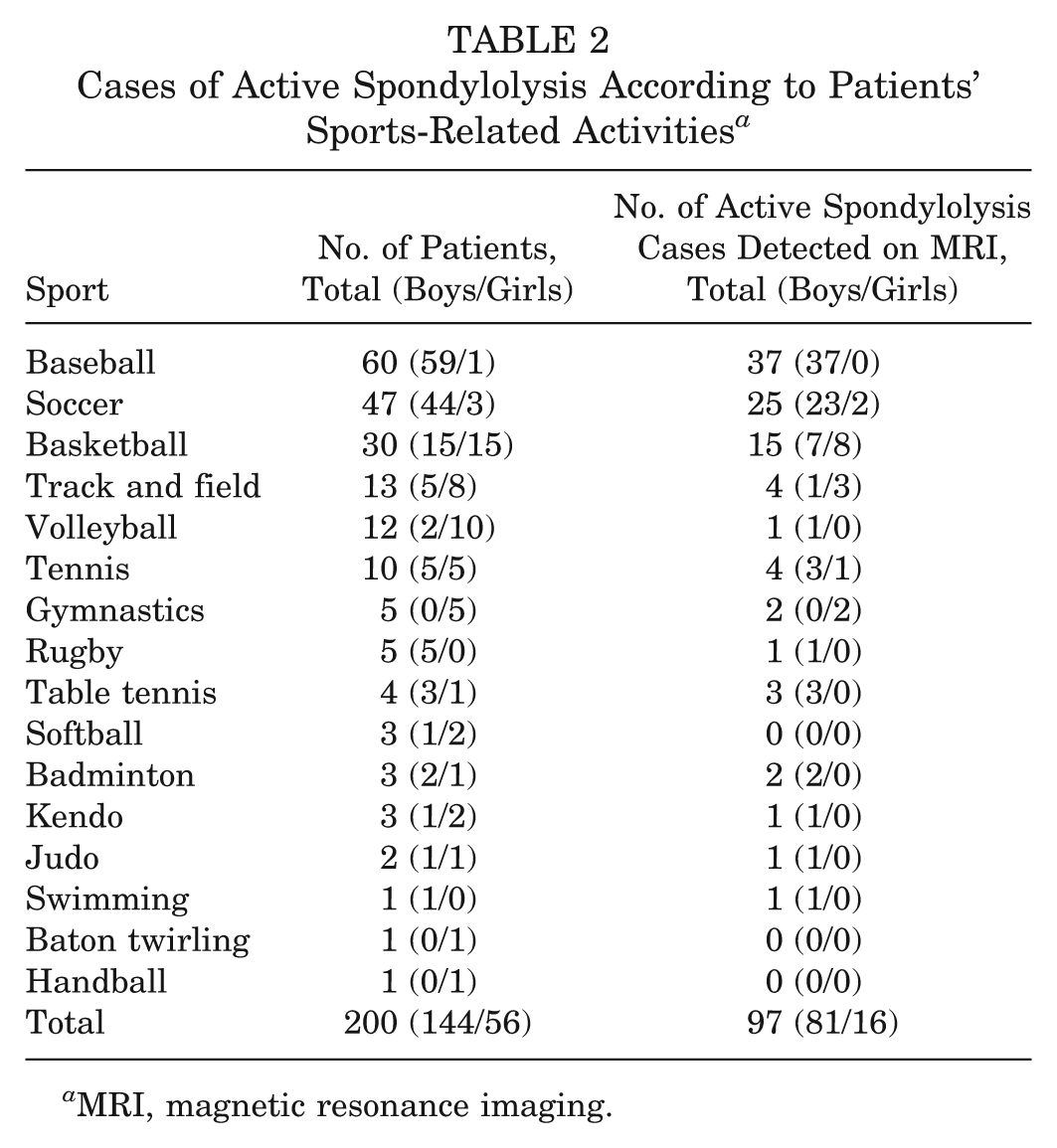
MRI, magnetic resonance imaging.
Vertebral Levels Affected in Cases With Active Spondylolysis Detected on Magnetic Resonance Imaging
Computed tomography scans were taken of 121 pars interarticularis in 92 patients who showed high intensity changes of the pedicle on MRI. These pars defects were organized into various categories based on CT findings as follows: nonlysis stage, 52; very early stage, 37; late early stage, 22; progressive stage, 10; and terminal stage, 0. Thus, 52 (43.0%) were in the nonlysis stage, and 37 (30.6%) were in the very early stage (partial lysis stage). Six patients with unilateral active spondylolysis on MRI showed contralateral inactive (chronic) spondylolysis on CT.
The findings of the physical examinations are shown in Table 4. Overall, 90% of the patients belonging to the group without spondylolysis on MRI and 88.1% belonging to the group with spondylolysis on MRI experienced pain during lumbar spine extension, which has been described as being diagnostic for lumbar spondylolysis. The results of the statistical analysis are shown in Table 5. We investigated whether the physical examination findings were normally distributed in the group in which MRI showed the presence of active spondylolysis and the group in which it showed an absence of active spondylolysis. The dependent variable was the finding of active spondylolysis on MRI, and the independent variables were sex, age, and each of the physical examination findings. Table 5 shows the final results for the eligible predictors and their significant interactions after multivariate logistic regression analysis using the forward stepwise method. The results indicate that sex could remain a significant factor in the model (P < .01). From these results, none of the physical examination factors was significant and therefore could not assist in the early detection of active spondylolysis.
Examination Findings: Incidence of Low Back Pain a
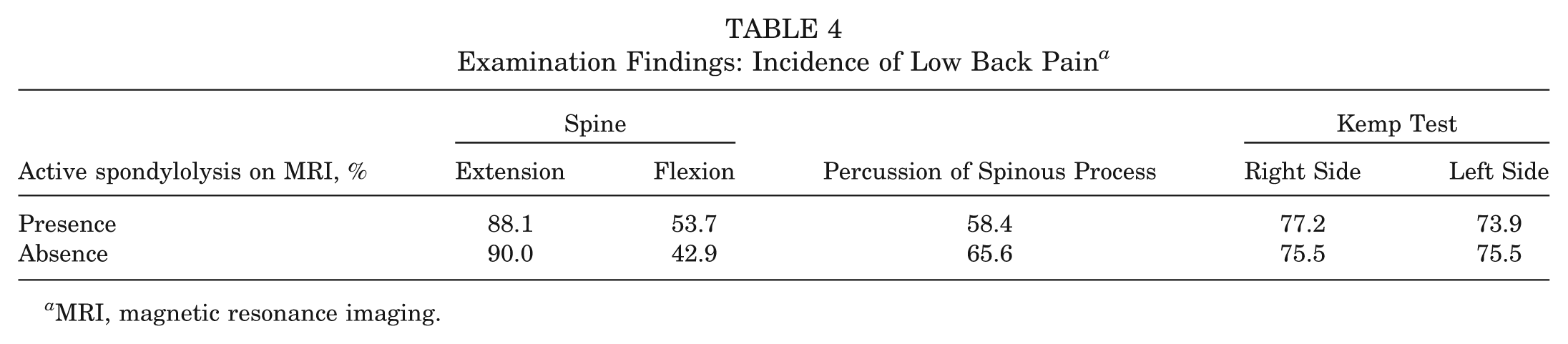
MRI, magnetic resonance imaging.
Statistical Analysis Results for Physical Examination and Active Spondylolysis a
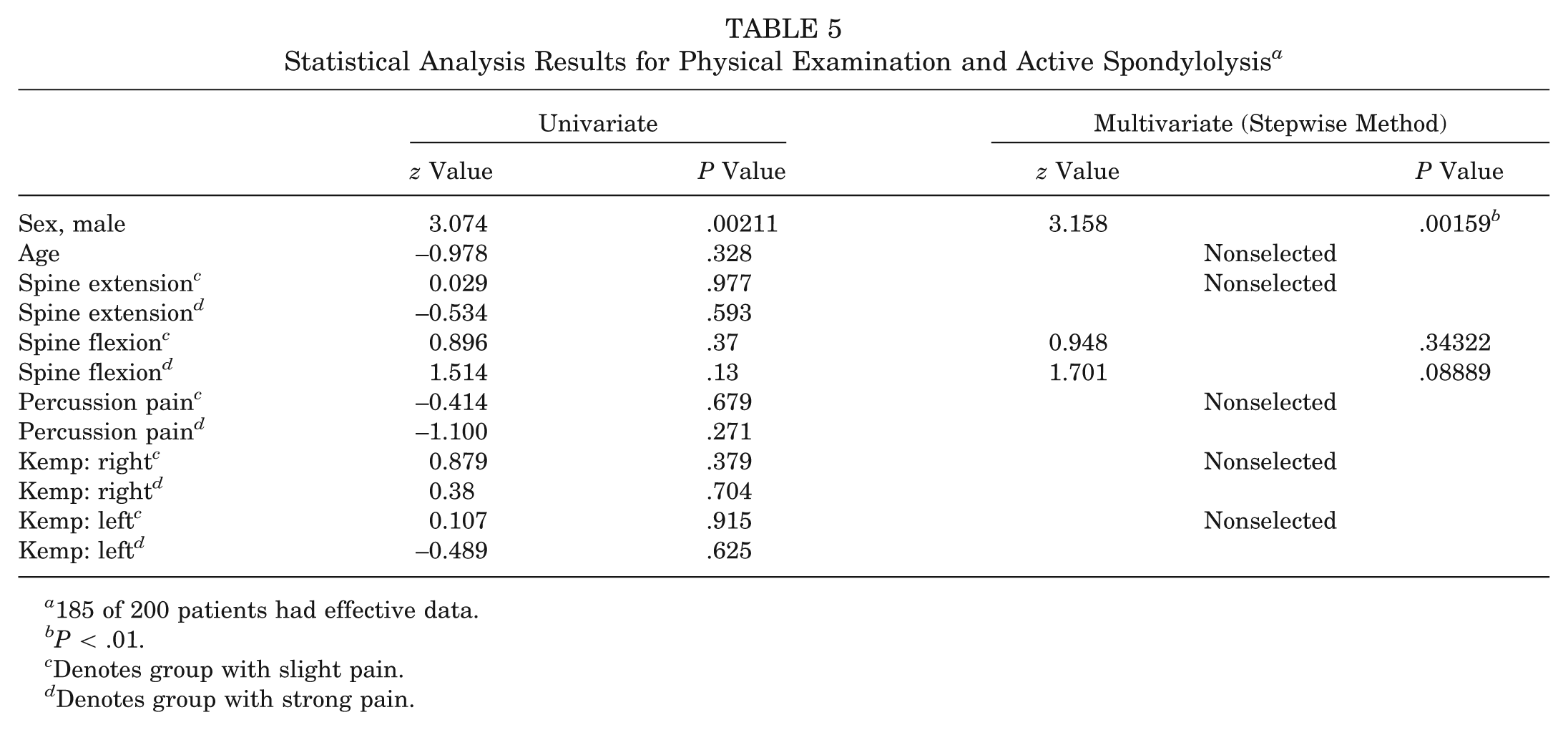
185 of 200 patients had effective data.
P < .01.
Denotes group with slight pain.
Denotes group with strong pain.
Discussion
Active spondylolysis is a common cause of low back pain in young athletes, 19 and the incidence appears to be higher in young athletes than in the general population.25,35 Sys et al 42 used the terms “active” and “inactive” related to the appearance on SPECT scintigraphy in their report of spondylolysis, and Sairyo et al 39 reported that a high signal change of the pedicle on MRI might overlap with the condition of active spondylolysis. Based on these reports, we used the term “active spondylolysis” in relation to the appearance on STIR MRI in this report.
Lesions of the pars interarticularis in spondylolysis are generally considered to arise from mechanical stress applied to that portion of the neural arch,7,10,31,43,45 and many authors believe that the increased rate of spondylolysis in athletes is related to the increased forces in the lumbar spine associated with various athletic activities.15,25,31 The pathogenesis of lumbar spondylolysis, however, remains controversial. Herman and Pizzutillo 18 proposed a new classification for pediatric spondylolysis and spondylolisthesis, classifying the former into 4 subgroups: dysplastic, developmental, traumatic (A, acute; B, chronic, further divided into stress reaction, stress fracture, or spondylolytic defect), and pathological. Although multiple factors may be involved in its genesis, it is currently considered to be a stress fracture when it occurs among athletes.7,10,31,43,45 The type of spondylolysis discussed here is a stress fracture, which represents the primary clinical lesions of the pars interarticularis in young athletes. In this sense, the patients serving as participants in this study differ from patients with developmental or other pathogenesis of spondylolysis.
The progression of active spondylolysis to pseudarthrosis has been associated with an increased incidence of spondylolisthesis. 36 Ikata et al 20 reported that spondylolysis-associated end-plate lesions in young athletes have a high risk of slippage, resulting in spondylolisthesis. Moreover, the early detection and treatment of acute spondylolysis are associated with improved fracture healing14,30,39 and are important for preventing the progression to established pseudarthrosis. Spondylolysis refers to a radiolucent defect in the pars interarticularis. However, early-stage spondylolysis is very difficult to diagnose on plain radiographs.17,37 Saifuddin et al 38 reported only 32% of defects identified by CT were actually identified even with lateral oblique views. In the present study, 6 patients with unilateral active spondylolysis on MRI showed contralateral inactive (chronic) spondylolysis on CT. As mentioned above, despite having negative findings on radiographs, unexpectedly, we saw that some lesions were quite advanced on CT. Adults with spondylolysis and low-grade spondylolisthesis have no more back pain than the general population and infrequently develop progressive spinal deformity or symptoms that require surgical intervention. Kalichman et al 27 reported no significant association between spondylolisthesis, isthmic spondylolisthesis, or degenerative spondylolisthesis and the occurrence of low back pain in their 3529 adult participants on CT. Beutler et al 3 reported that bilateral spondylolysis followed a clinical course similar to that of the general population in their 45-year follow-up studies. Moreover, Weil et al 44 reported that the incidence of sickness absenteeism due to low back pain was not influenced by spondylolysis in a population of 3988 police officers. Despite these findings in adults, spondylolysis is a common cause of low back pain in young athletes. Micheli and Wood 35 reported that 47% of young athletes (age ≤18 y) who were evaluated for low back pain had a diagnosis of lumbar spondylolysis compared with only a 5% prevalence in adult patients. Iwamoto et al 24 reported that spondylolysis was a significant radiological risk factor for low back pain in 327 high school rugby players. Iwamoto et al 23 reported that high school football players with spondylolysis had a higher incidence of low back pain (79.8%) than those with no abnormal radiographic results (37.1%), and college football players with spondylolysis had a similarly higher incidence of low back pain (80.5%) than those with no abnormal radiographic results (32.1%). They concluded that spondylolysis is the most significant risk factor for low back pain in high school and college football players. Given these findings, it would seem to be beneficial to achieve bony union if the detection and treatment of spondylolysis can occur in the early stages of the disease.
Computed tomography, SPECT, and MRI have all been used in the diagnosis of early spondylolysis, and there is considerable controversy regarding which diagnostic technique has the highest sensitivity and specificity.6,28,32 Each imaging modality has both advantages and limitations. Bone scintigraphy, SPECT, and MRI cannot determine the adequate bony defect for lumbar spondylolysis. Therefore, reverse gantry angle imaging on CT scans is likely the best method for detecting the anatomic details of the spondylolysis defect and monitoring recovery during the follow-up period. However, CT is less sensitive in distinguishing between active and inactive lesions than scintigraphy, SPECT, and MRI.2,6,32,37 The diagnostic utility of bone scintigraphy in combination with SPECT has also been studied for diagnosing active spondylolysis that was not observable on plain radiographs.2,16 Indeed, SPECT is the most sensitive tool for the early diagnosis of active spondylolysis in young athletes17,22,37 and has been considered the gold standard for diagnosing spondylolysis. Sys et al 42 reported that SPECT can help in the diagnosis of early active spondylolysis, which can heal with nonoperative treatment. Magnetic resonance imaging is also reported to be effective in diagnosing early spondylolysis,4,6,14,39,46 and one of its advantages is the lack of radiation exposure, which is particularly desirable in pediatric patients. It also provides a high diagnostic yield by detecting other pediatric spinal disorders (eg, degenerative disc disease, disc herniation, discitis, and apophyseal ring tear) that may be missed by scintigraphy. Additionally, MRI can detect spondylolysis activity. Sairyo et al 39 reported that high signal changes on T2-weighted MRI scans were useful as well as noninvasive in the early diagnosis of spondylolysis and could therefore serve as a good predictive indicator of bony healing after nonoperative therapy. Some studies have evaluated the effectiveness of MRI in comparison with SPECT for spondylolysis diagnosis. Masci et al 32 reported that MRI is inferior to SPECT because MRI results in a comparatively significant number of false-negative findings. Yet, Campbell et al 6 claim that MRI can effectively replace SPECT for the investigation of spondylolysis and that it is reasonable to utilize MRI as a first-line imaging modality for the investigation of juvenile spondylolysis. Therefore, opinions vary widely on the appropriate diagnostic imaging method for evaluating spondylolysis. The present study did not evaluate MRI versus SPECT, and we cannot therefore make any comment on the difference in sensitivity between MRI and SPECT. We can state through our primary finding that because MRI can detect abnormalities in radiographically occult patients, it is more sensitive than radiographs. Recently, some studies have recommended using MRI after initial negative radiography results rather than SPECT screening to investigate the presence of spondylolysis in young athletes because it minimizes radiation exposure for pediatric patients.28,34 Ishibasi et al 21 reported that even with negative radiographic findings, all scintigraphy and STIR MRI scans revealed stress injuries to bone (not spondylolysis) in their 31 patients, and all MRI findings corresponded with the scintigraphy findings. They concluded that MRI is less invasive and provides more information than scintigraphy and recommended it for the initial diagnosis of stress injury to bone. Taken together, we recommend using STIR MRI as a second screening when radiographs at first screening show no abnormality but the athlete has nonspecific low back pain, and spondylolysis that is potentially radiographically occult should be ruled out.
Ninety-seven of our 200 patients (48.5%) showed evidence of active spondylolysis on MRI but not on plain radiography, and more than 70% who showed active spondylolysis on MRI were diagnosed as being in the nonlysis or very early stage. These findings suggest that MRI is indeed useful in the early diagnosis and also that there is a high rate (48.5%) of active spondylolysis in young athletes with low back pain. However, localized CT should also be performed for patients with active spondylolysis to serve as a baseline for follow-up and for supplementary evaluation in indeterminate cases, as recommended by Campbell et al. 6
We also acknowledge that MRI findings are not comparable with those of CT for the following reasons. First, bony healing cannot be detected on MRI, so we must confirm on follow-up CT whether bony union has been achieved and the condition at the fracture site. Second, differences between the stages cannot be seen on MRI, such as the difference between the nonlysis and very early stages or the very early and late early stages. As we decide the duration of the resting period depending on the patient’s stage of disease when he or she wants conservative therapy—6 weeks in the nonlysis stage, 8 weeks in the very early stage, and 12 weeks in the late early and progressive stages—it is important that we can determine the patient’s stage of spondylolysis accurately. After the resting period, we usually perform follow-up CT and confirm whether bony union has been achieved. Because CT exposes the pediatric patient to radiation, we perform CT only for the vertebral body corresponding to the vertebra with high intensity change seen on MRI to minimize the radiation exposure. However, CT cannot reliably distinguish between active and inactive lesions; therefore, we recommended MRI as the first diagnostic tool in cases where no findings are detected initially on plain radiography and then add CT to clarify any fracture shown on MRI and to follow up on osseous healing, as recent studies have also suggested.6,11
There were some limitations to this study regarding whether the high signal intensity in the pedicle region on STIR is active spondylolysis. Maurer et al 33 reported that of the 22 asymptomatic adolescent rowers included in their study, 5 showed high signal intensity of the pars interarticularis on T2-weighted MRI scans, and none showed symptoms associated with spinal problems up to 3 months after the end of the study. On the other hand, Masci et al 32 reported that of their 39 patients with positive SPECT results, 25 had normal CT scans; the authors defined this condition as a “stress reaction in active spondylolysis.” Herman and Pizzutillo 18 used the term “stress reaction” to describe positive MRI or SPECT findings where there was no evidence of cortical disruption on CT. In the present study, all patients had a history of low back pain, and in 2 of 5 patients who did not comply with nonoperative treatment and continued their sports activity, spondylolysis progressed from the nonlysis stage to the late early stage. We therefore suggest that the nonlysis stage is a positive indicator of spondylolysis and that the nonlysis stage is a prefracture.
The clinical features of active spondylolysis described in the literature cannot be used to differentiate this condition from other causes of low back pain.7,32,35 In addition, no validated examination factors have been established to date. The only putative pathognomonic finding noted in the literature is the repeated occurrence of pain when performing the 1-legged hyperextension maneuver, 29 and unilateral lesions often result in pain when standing on the ipsilateral leg. 26 However, these reports did not provide data indicating the 1-legged hyperextension test’s validity. Masci et al 32 reported, however, that this test is neither sensitive nor specific for diagnosing active spondylolysis. We consider the Kemp test to be more suitable for stimulating the pars interarticularis as well as more simple to perform than the 1-legged hyperextension test and thus used the maneuver instead in our physical examination. In the present study, despite completing 5 examinations—presence or absence of low back pain during lumbar spine extension, presence or absence of low back pain during lumbar spine flexion, right-sided Kemp test, left-sided Kemp test, and percussion of the vertebral spinous process—we could find no significant physical examination factors that could assist in the early detection of active spondylolysis.
As to the incidence of lumbar spondylolysis and sex, Sakai et al 40 reviewed the CT scans of 2000 patients without low back pain and found lumbar spondylolysis in 117 patients with a male:female ratio of 2:1.1,13 Other authors have similarly noted male patients being affected 2 to 3 times as often as female patients. In the present study, sex was a significant factor of spondylolysis. We considered that the reason for spondylolysis being more prevalent in boys than in girls was the difference in their sports activity. Spondylolysis is generally believed to be caused by a stress fracture of the pars interarticularis because of repetitive extension or rotational motion of the lumbar spine.7,8 In our study, many of the children showing spondylolysis participated in baseball (61.7%) and soccer (53.2%), which are sports that require repetitive extension or rotational motion of the lumbar spine, and boys took part in these sports more often than girls.
Because early spondylolysis cannot be detected with plain radiography, MRI should be considered for the diagnosis of young athletes with low back pain and negative radiographic results. However, we cannot conclude from the findings of the present study that MRI should be performed in all young patients with low back pain immediately on the first visit to the doctor. Further studies are required to investigate when it is appropriate to perform an MRI examination in cases where young athletes’ symptoms have persisted, for example, immediately or at >2, 4, or 6 weeks afterward. If physicians are considering using MRI to detect active spondylolysis, we recommend STIR MRI and to take slices of not only the disc but also the pedicle in the axial view. The MRI protocol to examine primarily for disc protrusion may not be as sensitive as the protocol used in the present study for detecting spondylolysis. Given that 48.5% of our young patients showed active disease, physicians should be cognizant that active spondylolysis can be a cause of low back pain in young athletes especially in the sports of baseball and soccer.
Conclusion
The MRI results suggest that there is a high rate of active spondylolysis in young athletes with low back pain who show negative findings for spondylolysis on plain radiography. Based on our results, MRI appears to be very useful for early diagnosis, especially as we found no significant physical examination factors that could assist in early detection.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.