
Abstract
Background:
An olecranon stress fracture is a rare injury associated with valgus extension overload in baseball players. No long-term outcomes studies have been published documenting the results of surgical fixation of olecranon stress fractures with or without concomitant injuries in baseball players.
Hypothesis:
Open reduction and internal fixation (ORIF) of an olecranon stress fracture will reliably produce bony union and allow a successful return to the previous level of activity in competitive baseball players.
Study Design:
Case series; Level of evidence, 4.
Methods:
Twenty-five patients treated with ORIF for an olecranon stress fracture at least 2 years earlier (range, 2-10.14 years) were retrospectively contacted to complete a telephone survey; 18 of 25 (72%) patients responded. Data were collected to determine the return to play rate, level of arm pain, and overall arm function.
Results:
All 18 stress fractures went on to successful union; 17 of 18 (94%) athletes returned to baseball at or above their previous level. Average return to play time was 29 weeks. The numeric analog pain score was 0.2 at rest and 0.3 when throwing at the time of follow-up, at an average 6.2 years (range, 2.0-10.14 years) after surgery. The average score at follow-up on the Disabilities of the Arm, Shoulder and Hand Outcome Measure–shortened version (QuickDASH) was 4.1 (range, 0-27.3). Ten (56%) patients required 13 additional future surgeries on their throwing arm; 7 surgeries in 6 (33%) patients were not related to the index surgery. Six of 18 (33%) patients underwent hardware removal, with 2 (11%) for infection.
Conclusion:
Open reduction and internal fixation of olecranon stress fractures in competitive baseball players has a high rate of success in returning players to or above their former level of play and allows for good elbow function at an average of 6.2 years postoperatively. However, these patients are at high risk for additional future surgeries on their throwing arm.
An olecranon stress fracture is a rare injury sustained by overhead-throwing athletes (Figure 1). It was originally described in javelin throwers by Waris in 1946. 31 It has subsequently been described in multiple case reports in baseball players, gymnasts, weight lifters, and divers. ¶ However, there are no prospective or retrospective case series reporting the outcome of surgical fixation of olecranon stress fractures in baseball players in the current literature.
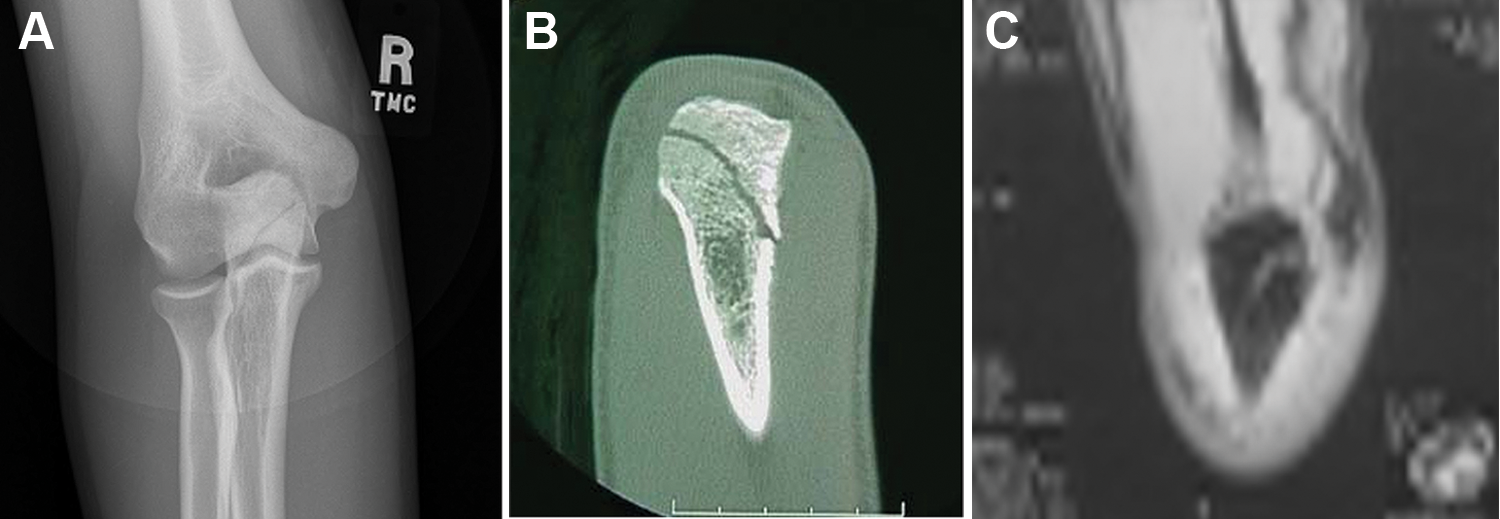
Preoperative imaging of an olecranon stress fracture. (A) Anteroposterior view of the elbow with an oblique fracture line noted, (B) computed tomography scan with the fracture line noted, and (C) magnetic resonance imaging scan with the fracture line noted.
Both nonsurgical20,26,28 and surgical treatments # of olecranon stress fractures have been described. In our practice, open reduction and internal fixation (ORIF) is performed after the failure of nonoperative treatment and is based on each individual athlete’s goals for their return to play. Based on the assumption that fracture fixation and bony union would allow for a return to function, we hypothesized that ORIF of an olecranon stress fracture would reliably produce bony union and allow the successful return to the previous level of activity in competitive baseball players.
Materials and Methods
After receiving approval from our local institutional review board, a search of our prospectively collected database (American Sports Medicine Institute) was performed for patients undergoing ORIF of the olecranon. Forty potential patients were identified for inclusion. Patients were included if they were athletes involved in overhead sports treated for an olecranon stress fracture with ORIF at least 2 years earlier and if they were available for follow-up. All injuries were diagnosed by a thorough clinical examination and radiographic work-up, including plain radiographs with stress views and magnetic resonance imaging (MRI) arthrograms and/or computed tomography (CT) scans. All patients had failed results with a period of nonoperative treatment including active rest with or without bracing and a formal throwing program where indicated, as described by Schickendantz et al. 26 Patients were excluded if they were treated for an acute olecranon fracture or an unfused olecranon physis or if they had surgery less than 2 years previously. A chart review yielded 25 potential participants who met inclusion and exclusion criteria. Preoperative, operative, and postoperative information was collected from the patients’ charts to document preoperative diagnoses, procedures performed, and implants used and to verify the postoperative course.
A custom questionnaire was designed for a retrospective telephone follow-up to increase the participation rate over a traditional mailed questionnaire. The questionnaire included an 11-point numeric analog pain scale (NAPS; low to high pain level from 0 to 10) and a shortened version of the Disabilities of the Arm, Shoulder and Hand Outcome Measure (QuickDASH).
Patients were contacted using telephone numbers from their clinical charts or that were found through the use of an Internet telephone number database. The survey was administered by one of the authors or a member of the research staff at our institution. During the follow-up interview, each patient answered questions about 3 time periods: postinjury/presurgery, return to play, and currently at the time of follow-up. Preoperative and postoperative radiographs of all included patients, when available, were reviewed independently to verify the stress fracture pattern and the time to radiographic evidence of bony union.
Surgical Technique
Open reduction and internal fixation was performed under C-arm fluoroscopic control. The patient was positioned supine with the arm placed on a hand table. A tourniquet was placed high on the arm and out of the sterile field and was inflated after induction of anesthesia, preparation, and drape. A small percutaneous approach was used for screw placement with a stab incision located over the screw insertion point. In cases with an additional injury, a medial incision was made in addition to the small posterior incision to address the medial injury. A guide pin was placed under fluoroscopic control, perpendicular to proximal transverse–oriented stress fractures and down the ulnar canal for midproximal oblique stress fractures. The guide pin was then overreamed for the appropriately sized cannulated screw based on the patient’s anatomy, as determined by preoperative radiographs. A single titanium cannulated screw was then placed. C-arm radiographs were taken to verify hardware position. Any additional surgical intervention was then performed. The tourniquet was deflated before irrigation and wound closure to avoid hematoma formation. A sterile dressing was then placed and a posterior splint applied.
Postoperative Rehabilitation
Rehabilitation after ORIF of an olecranon stress fracture was and continues to be a multiphased approach. 33 Immediately after surgery, the patient’s arm was placed into a posterior splint at 90° of flexion for 7 to 10 days to allow the soft tissues to heal. The length of immobilization depended on the patient’s variables (age, osseous status, health, desired goals, healing response). During this time, the patient was allowed to perform wrist, hand, and shoulder range of motion exercises. Unlimited passive motion was allowed once the splint was removed. Active pronation, supination, and flexion were allowed; however, active flexion beyond 90° was avoided for 6 weeks. Full motion in all directions was expected to be achieved by 6 weeks. During this period, the patient was allowed to perform rotator cuff, scapular, and shoulder exercises. At 6 weeks, gentle active flexion was initiated, and strengthening was started at 8 weeks. At 8 weeks after surgery, the patient started our “thrower’s ten program” 32 designed to restore strength in the entire upper extremity, trunk, and core. At 12 weeks after surgery, the patient started the advanced “thrower’s ten program” and plyometrics, and shortly thereafter, the interval throwing program 23 was initiated at 14 to 16 weeks after surgery. Throwing from the mound was initiated once the patient had completed a long toss program to 120 to 145 ft without any elbow symptoms or complaints.
Results
Eighteen of 25 patients (72%) were available for follow-up (Table 1). All 18 were male baseball players with an average age of 20 years (range, 16.1-23.8 years) at the time of surgery. Average time to follow-up was 6.2 years (range, 2.0-10.14 years). Sixteen were pitchers, including 1 who also played third base, as well as 1 who was a catcher and 1 who played shortstop. Two were professionals (1 played for Major League Baseball, and 1 was on a Minor League Baseball Class A team), 11 were collegiate players, and 5 were high school athletes. All had a diagnosed symptomatic olecranon stress fracture clinically and radiographically (Figure 1) and underwent ORIF of an olecranon stress fracture using a single cannulated titanium screw, with the screw size based on patient anatomy and orientation of the stress fracture (range, 4.5-8.0 mm). Preoperative radiographic work-up included plain radiographs, CT scans, and/or MRI arthrograms (Figure 1). Five (28%) were proximal transverse–oriented stress fractures, while 13 (72%) were midproximal oblique (proximal medial to distal lateral)–oriented stress fractures (Figure 2). 19
Patient Demographics a
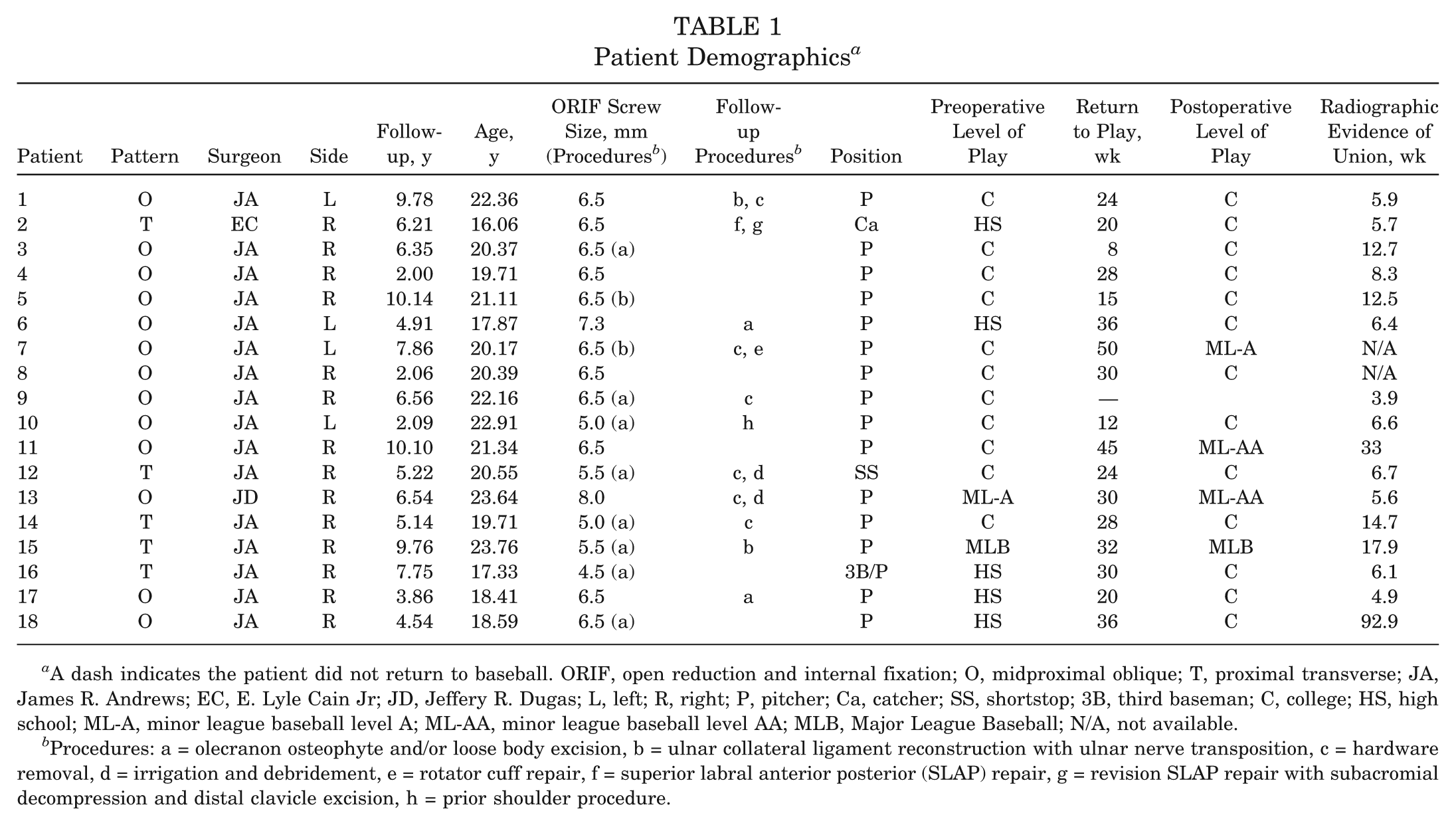
A dash indicates the patient did not return to baseball. ORIF, open reduction and internal fixation; O, midproximal oblique; T, proximal transverse; JA, James R. Andrews; EC, E. Lyle Cain Jr; JD, Jeffery R. Dugas; L, left; R, right; P, pitcher; Ca, catcher; SS, shortstop; 3B, third baseman; C, college; HS, high school; ML-A, minor league baseball level A; ML-AA, minor league baseball level AA; MLB, Major League Baseball; N/A, not available.
Procedures: a = olecranon osteophyte and/or loose body excision, b = ulnar collateral ligament reconstruction with ulnar nerve transposition, c = hardware removal, d = irrigation and debridement, e = rotator cuff repair, f = superior labral anterior posterior (SLAP) repair, g = revision SLAP repair with subacromial decompression and distal clavicle excision, h = prior shoulder procedure.

(A) Proximal transverse olecranon stress fracture before and after open reduction and internal fixation (ORIF). (B) Midproximal oblique olecranon stress fracture before and after ORIF.
There were 10 concurrent procedures performed at the time of the index procedure in 10 patients, including 8 (44%) olecranon osteophyte and/or loose body excisions and 2 (11%) ulnar collateral ligament (UCL) reconstructions with ulnar nerve transposition (UNT).
Based on chart review, all 18 stress fractures went on to successful bony union. Furthermore, 16 of 18 (89%) postoperative radiographs available for independent review verified successful union. The range of time to initial independent evidence of bony healing was 3.9 to 17.9 weeks (mean ± standard deviation, 10.9 ± 4.3), excluding 2 patients with no follow-up radiographs available for review and 2 patients with only postoperatively available radiographs from >6 months after surgery (Table 1).
Seventeen of 18 (94%) patients returned to baseball, all at or above their prior level of play. One did not return to baseball because of continued elbow pain. The average time to return to throwing was 29 weeks (range, 8-45). On average, excluding the athlete who did not return to play, athletes played 3.1 years (range, 1-7) after surgery.
Ten (56%) patients required 13 additional surgeries on their throwing arm. Six patients (33%) had procedures for complications related to the index procedure, all requiring hardware removal, including 2 (11%) for infection. Diagnosis of infection was made clinically and based on laboratory data (complete blood count, erythrocyte sedimentation rate, and C-reactive protein) and culture results. One infection was acute and was treated with irrigation and debridement, 6 weeks of intravenous vancomycin therapy, and delayed hardware removal after fracture union. The other was subacute and was treated with irrigation and debridement, hardware removal, and 6 weeks of intravenous vancomycin therapy. The acute infection was identified as Staphylococcus aureus (resistant to penicillin G, ampicillin, and erythromycin), while no organism was identified for the subacute infection. The infections resolved uneventfully, and both athletes returned to play at or above their prior level at an average of 27 weeks after surgery. Of the 6 patients requiring hardware removal, 3 each were in the proximal transverse (3/5) and the midproximal oblique (3/13) groups. Six patients (33%) had additional surgeries on their throwing arm not directly related to their index procedure, including 2 UCL reconstructions with UNT (mean, 1.6 years after the index procedure; range, 1.6-1.7 years), 2 olecranon osteophyte and/or loose body excisions, 1 rotator cuff repair, and 1 labrum repair and revision labrum repair with subacromial decompression in the same patient. Of note, 1 patient had shoulder surgery on his throwing shoulder before his olecranon stress fracture. None had known prior elbow procedures. Including those performed at the time of and those performed subsequent to olecranon ORIF, 4 of 18 (22%) patients required UCL reconstruction with UNT, while 3 of 18 (17%) patients, including the patient with surgery before olecranon ORIF, required throwing shoulder surgery of some type.
Of those patients requiring UCL reconstruction with UNT at the time of the index procedure, both returned to play at or above their prior level. One played for 2 additional seasons, and the other played 5 additional seasons. Their average time to return to throwing was 33 weeks versus 28 weeks for those patients not requiring UCL reconstruction at the time of the index procedure. Of the 2 players requiring UCL reconstruction with UNT as an additional future procedure, 1 of 2 returned to play after the second surgery and continued to play 5 additional seasons.
All 8 of the 18 patients who underwent ORIF without additional procedures at the index surgery returned to throwing at an average of 29 weeks after surgery and were able to play at or above their prior levels of play. However, 3 required additional surgeries: 1 patient underwent hardware removal and UCL reconstruction with UNT, 1 required superior labral anterior posterior (SLAP) and revision SLAP repair with subacromial decompression, and 1 required irrigation and debridement and removal of hardware for infection.
The average QuickDASH score at the time of follow-up was 4.1 of 100 (range, 0-27.3), with 0 being a perfect score and 100 indicating the most disability. The mean elbow pain score at the time of follow-up was 0.2 ± 0.9 at rest and 0.3 ± 1.0 when throwing, where 0 indicates no pain and 10 indicates the maximum pain imaginable.
Discussion
A stress fracture of the olecranon is a rare consequence of overhead throwing, as in baseball and javelin throwing, and has also been reported in gymnasts, divers, and weight lifters. ** We have retrospectively analyzed a series of 18 baseball players requiring ORIF of an olecranon stress fracture. On the basis of our findings, we accept our hypothesis that ORIF of an olecranon stress fracture allows for a timely return at or above the prior level of play in competitive baseball players with a high rate of successful stress fracture union.
The limitations of this study include a small sample size, an incomplete follow-up (72%), the inclusion of patients with concomitant procedures to the elbow including UCL reconstruction, the retrospective collection of data that may introduce recall bias, the use of a telephone survey and the broad range of time to the final follow-up (range, 2-10.14 years), and the limited availability of postoperative radiographs to determine the definitive time to successful union. However, because of the rarity of this injury and the size of this cohort compared with any previously published literature about this condition, we accept these limitations.
Olecranon stress fracture, like a UCL tear, was first described in a javelin thrower. 31 It has subsequently been reported in baseball players, gymnasts, weight lifters, and divers. †† The mechanism responsible for olecranon stress fracture formation has been postulated to be related to valgus extension overload syndrome with posteromedial olecranon impingement and/or caused by repetitive triceps activity during deceleration.1,8,29 Three types of adult olecranon stress fractures have been reported based on the fracture orientation: olecranon tip, transverse, and oblique.1,19,29 In general, valgus stress causes oblique fractures, while a combination of valgus, extension, and triceps stress causes transverse fractures.1,19,29 Overall, throwers are more likely to have an oblique stress fracture line, as seen in the Suzuki et al 29 and Nuber and Diment 20 studies of 2 baseball pitchers each, while transverse fractures are seen in other activities like weight lifting because of excessive repetitive triceps strain. 22 Thirteen of our 18 patients had midproximal oblique stress fractures likely caused by the valgus extension overload mechanism commonly experienced by baseball throwers in the acceleration phase of throwing.10,14,29 Five had proximal transverse–oriented stress fractures, which have been proposed to be caused by a combination of valgus stress, extension/triceps stress, and posterior impingement. 19 These are not to be confused with olecranon tip stress fractures, which are caused by posterior impingement. 19 While it has been proposed that there may be slightly differing mechanisms for proximal transverse and midproximal oblique stress fracture patterns, they have been previously grouped together in the literature.12,19,20 This fine distinction deserves further investigation but is beyond the scope of this study.
As 4 of our patients required UCL reconstruction at the time of or after the index procedure, the role of added bony stress due to UCL insufficiency cannot be ruled out. In addition, 10 patients required surgical intervention for olecranon osteophytes and/or loose bodies at the time of the index procedure or during a later procedure. These osteophytes and loose bodies are often associated with valgus extension overload syndrome1,7,8,18,27,35 and were the most common diagnosis requiring surgical intervention in baseball players in the study by Andrews and Timmerman. 3 As noted by Morrey and An, 17 the bony articulation resists nearly one third of valgus stress in the elbow. With UCL insufficiency, posteromedial olecranon contact pressures have been shown to increase significantly. 2 Thus, it is highly likely that the mechanism of injury for our patients was repetitive stress across the olecranon caused by valgus extension overload, with or without UCL insufficiency. Because of the complex interaction of the pathological changes associated with valgus extension overload, we believe that it is prudent to treat all pathological conditions at the time of surgery, as they are interrelated. We think that this gives athletes the best chance of returning to their baseline physiology and eventual return to sport. As such, one must be prudent, when faced with a patient with an olecranon stress fracture, to rule out all possible associated injuries, especially when proceeding with surgical intervention. We excluded those patients with unfused olecranon physes due to delayed physeal closure because these are thought to be a different entity dependent on the physiological differences between skeletally immature and mature patients. 24
Treatment for olecranon stress fractures includes both nonsurgical and surgical options. ‡‡ Schickendantz et al, 26 in the largest documented series of its type, described 7 professional baseball players with MRI-documented olecranon osseous stress injuries who responded to nonsurgical treatment with relative rest, avoiding throwing or valgus stress for at least 6 weeks while wearing a protective brace for 4 weeks, followed by a progressive exercise regimen and throwing program. All 7 returned to throwing and play, starting their throwing programs at an average of 8 weeks after the initiation of care. Suzuki et al 29 reported on 2 cases of oblique olecranon stress fractures unresponsive to nonsurgical treatment requiring ORIF. Both returned to play after ORIF. One began a throwing program at 2 months and the other at 3 months after surgery, with a return to the prior level of pitching at 4 and 6 months after surgery, respectively. Because of the sclerotic nature of these stress fractures, Suzuki et al 29 recommended earlier surgical intervention for oblique-type stress fractures. Nakaji et al 19 reported the failure of olecranon stress fracture fixation with a tension band construct requiring revision with a lag screw construct and recommended treating baseball players with internal fixation with a lag screw construct to avoid nonunion.
We were able to identify and retrospectively contact 18 competitive baseball players requiring ORIF of an olecranon stress fracture at least 2 years after the index surgery. All had failed nonoperative management before surgical intervention. All stress fractures were fixed with a single lag screw construct, using cannulated titanium screws. Titanium screws were chosen to limit the possibility of MRI interference, should future MRI be warranted. As noted above, 2 athletes required later UCL reconstruction, and having titanium implants was helpful in diagnosing the UCL injury.
All patients went on to successful union, both radiographic and symptomatic, with 94% returning to competitive baseball, all at or above their prior level of play in an average of 29 weeks (28 weeks without UCL reconstruction and UNT and 33 weeks with). Patients who did return to play returned for an average of 3.2 additional years of baseball.
The QuickDASH was included as a measure of current arm function to help determine the effect of olecranon stress fractures on overall elbow and arm function. The average QuickDASH score was 4.1 of 100, with 100 being maximum disability. On the basis of these data, we believe that good long-term arm function is achieved after ORIF of olecranon stress fractures at an average of 6.2 years after surgery.
Despite good outcomes, a high return to play rate, low pain scores, and good function based on QuickDASH scores, there was a high rate of concomitant surgical procedures and additional procedures both related to and unrelated to the index procedure on the throwing arm of these athletes. Six patients had complications requiring later hardware removal, 2 because of infected hardware. This yielded an overall complication rate of 33% and an infection rate of 11%. Hardware removal after ORIF of traumatic olecranon fractures has been reported in up to 66% of patients, 25 while infection has been reported in 0% to 6% of cases.11,21 On the basis of these data, it is suggested that patients be informed that there is a significant risk of the need for hardware removal after this procedure and that there is a slightly greater risk for infection compared with the fixation of traumatic olecranon fractures. The high rate of infection may be related to the subcutaneous nature of the screw head after fixation. Use of a headless compression screw construct may decrease this risk and should be explored in a future study.
There were 2 postoperative infections in our group: 1 was an acute infection requiring irrigation and debridement and 6 weeks of intravenous antibiotics followed by delayed hardware removal, and 1 was a subacute infection requiring hardware removal and treatment with 6 weeks of intravenous antibiotics. Both went on to uneventful healing and resolution of symptoms and return to play at or above their prior level of play at an average of 27 weeks after surgery. Aggressive treatment is recommended for suspected infections, and limited change of outcome should be expected based on our 2 cases.
For 33% (6/18) of patients, additional throwing-related surgeries on their throwing arm, not related to the index procedure, were required. These surgeries included 3 shoulder surgeries in 2 patients (17%) (a rotator cuff repair on 1 patient and 2 labrum repairs on another patient) and 4 elbow procedures (22%) (2 UCL reconstructions with UNT and 2 olecranon osteophyte and/or loose body excisions). The total UCL reconstruction with UNT incidence in this patient population was therefore 22%, with 2 at the time of the index procedure and 2 after. The addition of UCL reconstruction with UNT at the time of the index procedure added 7 weeks more time to players’ return to throwing. One of the 2 patients requiring additional UCL reconstruction and UNT after the index procedure (an average of 1.6 years later) returned to play and continued to play 8 years after the index procedure. The other retired after his UCL reconstruction with UNT. Based on these data, we believe that an olecranon stress fracture is an injury caused by and indicative of an overall pathological condition in these athletes, related to throwing, that places them at high risk for injury to their throwing arm. Contributing factors to this state are beyond the scope of this study but should be looked into in future studies.
Conclusion
An olecranon stress fracture treated with single-screw fixation is successful in returning competitive baseball players to their prior level of play or higher with good elbow function at an average of 6.2 years’ follow-up. However, there is a relatively high rate of hardware removal and postoperative infection, and despite good outcomes, patients have a high risk for further throwing arm injuries requiring additional surgery.
Footnotes
Presented at the 37th annual meeting of the AOSSM, San Diego, California, July 2011.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.