
Abstract
Background:
Anterior cruciate ligament (ACL) and meniscus injuries are common in female athletes participating in cutting and pivoting sports such as basketball. The epidemiological characteristics of injury in athletes seen at the Women’s National Basketball Association (WNBA) combine and the effect of ACL reconstruction and meniscus surgery on longevity in the WNBA are unknown.
Purpose:
To evaluate the details and spectrum of injuries in athletes entering the WNBA combine and to assess the potential effect of specific injuries on the round drafted into the WNBA and career length.
Study Design:
Descriptive epidemiology study.
Methods:
Demographic data and the documented collegiate injury profile were reviewed from the WNBA database for all players entering the WNBA combine in 2000-2008. The study included injury data on 506 athletes. Complete demographic data were available for 496 players.
Results:
Of the athletes taking part in the combine, 45.2% were guards, 33.7% were forwards, and 21.1% were centers. Ankle sprain (47.8% of players), hand injury (20.8%), patellar tendinitis (17.0%), ACL injury (15.0%), meniscus injury (10.5%), stress fracture (7.3%), and concussion (7.1%) were the most common injuries reported. Seventy-three athletes (14.4%) reported ACL reconstruction before entering the WNBA combine, and meniscus surgery was the next most common surgery (n = 50 players; 9.9%). There were no differences in ACL or meniscus surgery when analyzed by player position or round drafted. History of ACL or meniscus surgery did not affect career length in the WNBA. Excluding ACL and meniscus surgery, other reported surgical procedures were knee arthroscopic surgery (11.7%), ankle reconstruction (2.6%), and shoulder stabilization (2.0%).
Conclusion:
The ankle is the most common site of injury and ACL reconstruction is the most common surgery in elite female athletes participating in the WNBA combine. A history of injury or surgery did not affect the round drafted or career length.
Keywords
The Women’s National Basketball Association (WNBA) in the United States has gained national interest since its inception in 1997; however, little data exist regarding injuries in the athletes who participate in the professional league. Anterior cruciate ligament (ACL) injuries and meniscus tears are common and serious problems in women’s basketball and women’s athletics in general. Previous studies have shown that women have a rate of ACL injury that is 2 to 8 times higher than men.1,3,4 The proposed causes for the increased incidence of ACL injury in women include notch width,5,11,20,29 Q angle, 46 joint laxity and flexibility,37,44,45,50 hormonal variations,22,38,52 hamstring and quadriceps muscle strength and activation,9,25,30,36 jumping and landing characteristics10,12 including landing with the knee in abduction (valgus torque), 21 knee recurvatum or hyperextension,6,42 increased posterior tibial slope, 16 core proprioception deficits, 54 and race. 49
Zelisko et al 55 compared the injury rates between men and women in professional basketball and found that women sustained 60% more injuries than men. At the scholastic and collegiate level of play, women have been found to have a higher risk of injury to the knee and ankle than men. ‡ Additionally, significant differences in injury incidence, rate, and risk between sexes in sports have been found. ‡ Several studies have examined the risk of injury to athletes participating in the National Basketball Association (NBA).18,28,48,53 Players in the NBA have twice the risk of game-related injury when compared with college players because of the longer seasons and longer games in the NBA. 48 Deitch et al 8 compared injury rates between WNBA and NBA athletes and found that the lower extremity was the most frequently injured body part in both groups and that ankle sprain was the most common diagnosis.
These studies provide evidence that female athletes have higher rates of injury in college and likely during their professional basketball career; however, there are no published data that examine the injury profile of an athlete entering the WNBA combine. The purpose of this study was to (1) determine the demographics of the players entering the combine, (2) evaluate the history of injury in players entering the WNBA combine, (3) determine whether specific injuries have an effect on the round in which the athlete is drafted, and (4) determine whether a history of ACL or meniscus surgery has an effect on career length in the WNBA.
Materials and Methods
This study was approved by the institutional review board at our institution. We reviewed the WNBA medical records for all athletes entering the WNBA combine in 2000-2008, excluding 2003 when the combine was not held. Players are invited to the combine by invitation only. Athletes who were among the final 4 teams (the “Final Four”) in the National Collegiate Athletic Association (NCAA) tournament do not take part in the combine, as both take place on the same weekend. Additionally, not all players who are drafted participate in the combine. Those in the Final Four of the tournament, international athletes, and other postcollegiate athletes do not participate in the combine. This study included information on 506 total players participating in the combine. The information collected included player age, height, weight, body mass index (BMI), playing position, history of injury, and history of surgery. Inclusion criteria included all players who were evaluated by the medical staff before the combine and who entered the combine. Exclusion criteria included any player who was drafted into the WNBA but did not participate in the combine. Injury data were grouped into ACL injury and/or surgery, meniscus injury and/or surgery, other nonsurgical injury, and other surgical injury. The percentages in the “other” category were broken down to determine the most common injury and surgery reported. Data regarding the round drafted were acquired from the WNBA league office. Data on length of career in the WNBA were generated from the number of years of insurance coverage for each athlete, as athletes were provided insurance coverage through the WNBA for the years they were active in the league.
Overall, summary statistics were calculated in terms of means ± standard deviations for continuous variables and frequencies and percentages for categorical variables. After the initial analysis, univariate analysis of group differences between continuous variables was evaluated using independent-samples t tests. Group differences for discrete variables were evaluated using the χ2 or Fisher exact test. Odds ratios (ORs) and their respective 95% confidence intervals (CIs) were calculated to assess the magnitude of the association. Survival analysis was conducted to assess the effect of previous ACL and meniscus surgery on career length in the league. Cox proportional hazard ratio models were created with hazard ratios (HRs) and their corresponding 95% CIs to evaluate the time to occurrence.
Statistical significance was set at α equal to .05; however, to adjust for multiple comparisons, critical P values were adjusted using Bonferroni correction to compare the incidence of non-ACL or meniscus injuries by draft years. Critical P values of ≤.006 were considered statistically significant for those comparisons. All analyses were performed using SPSS version 20.0 (SPSS Inc, Chicago, Illinois).
Results
Demographics
The study included 506 athletes. Table 1 lists the description of the player population for which complete demographic information was available in 496 players. The mean age was 22.2 years (range, 19-37 years), mean height was 70.6 inches (range, 62-80.5 inches), mean weight was 166.7 lb (range, 117-278 lb), and mean BMI was 23.4 (range, 17.6-35.5). Guards comprised the highest percentage of players (45.2%) and were significantly shorter (mean, 67.9 inches; range, 62.0-76.3 inches) than forwards (mean, 71.6 inches; range, 66.0-75.3 inches) and centers (mean, 74.8 inches; range, 69.3-80.5 inches) (P < .001). Forwards were also significantly shorter than centers (P < .001). Guards were significantly lighter (mean, 150.8 lb; range, 117.0-207.0 lb) than forwards (mean, 171.2 lb; range, 125.0-218.0 lb) and centers (mean, 194.4 lb; range, 135.0-278.0 lb) (P < .001). Forwards were also significantly lighter than centers (P < .001). Guards had a significantly lower BMI than centers (mean, 23.0 vs 24.5; P < .001). Forwards also had a significantly lower BMI than centers (mean, 23.5 vs 24.5; P = .002). A total of 292 athletes were drafted over 4 rounds (72 in round 1; 93 in round 2; 86 in round 3; and 41 in round 4).
Player Demographics by Position (N = 496 Players) a
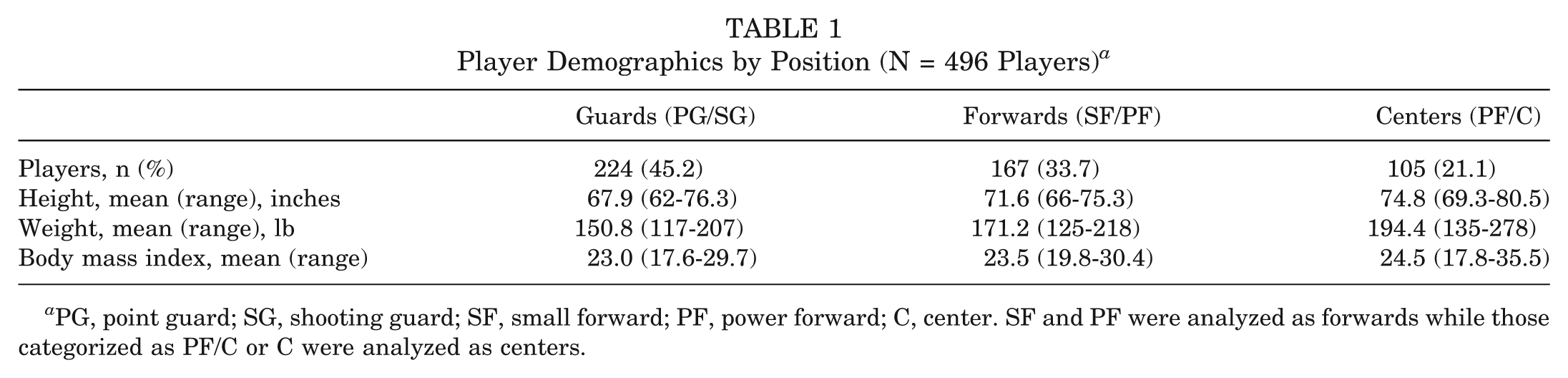
PG, point guard; SG, shooting guard; SF, small forward; PF, power forward; C, center. SF and PF were analyzed as forwards while those categorized as PF/C or C were analyzed as centers.
ACL and Meniscus Injury and Surgery
Complete injury data were available for 506 players. Seventy-six athletes (15.0%) reported an ACL injury, and 73 (14.4%) had an ACL reconstruction before entering the WNBA combine. Thirteen athletes (17.8%) had bilateral ACL reconstructions. Meniscus injury was reported in 53 athletes (10.5%) and meniscus surgery in 50 players (9.9%). Eight athletes (16.0%) had bilateral meniscus surgery.
Anterior cruciate ligament reconstruction and meniscus surgery were broken down and analyzed based on player position. There were no differences in ACL reconstructions based on player position (Table 2). Fewer ACL reconstructions were reported by centers than by other positions, but this was not statistically significant. Meniscus surgery was analyzed based on player position. There was no statistically significant correlation between player position and meniscus surgery (Table 2). There were no significant differences found for either bilateral ACL reconstruction or bilateral meniscus surgery.
ACL or Meniscus Surgery Versus Player Position (N = 496 Players) a
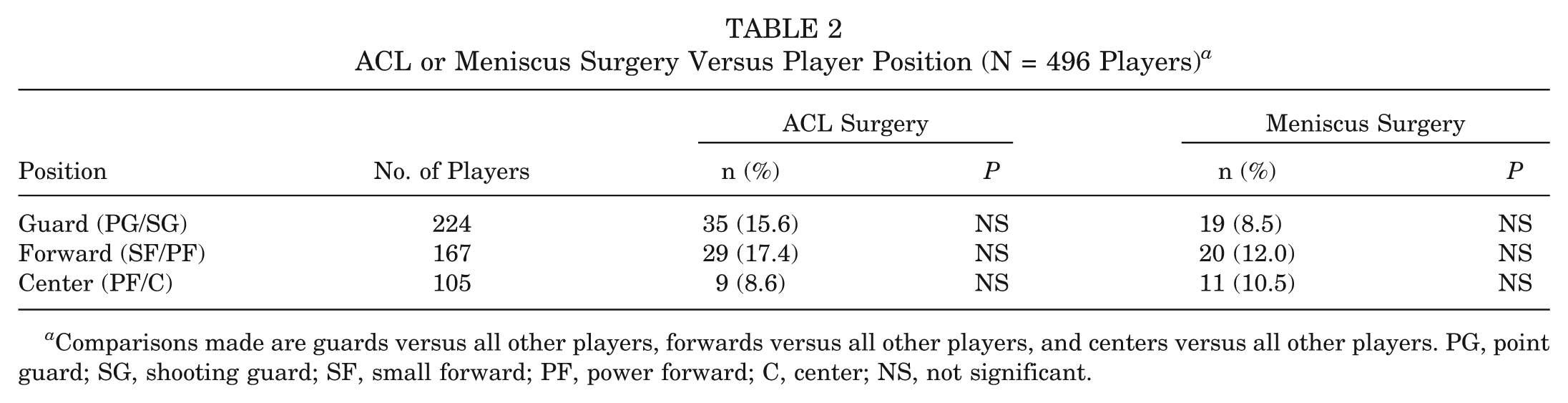
Comparisons made are guards versus all other players, forwards versus all other players, and centers versus all other players. PG, point guard; SG, shooting guard; SF, small forward; PF, power forward; C, center; NS, not significant.
The data for meniscus and ACL surgery (Table 3) were analyzed based on the round drafted of the 292 players who were drafted in the First Four rounds. Having an ACL reconstruction did not affect the round drafted nor did bilateral ACL reconstruction. There were no significant differences in meniscus surgery based on the round drafted or in those players with bilateral meniscus surgery.
ACL or Meniscus Surgery Versus Round Drafted (n = 292) a
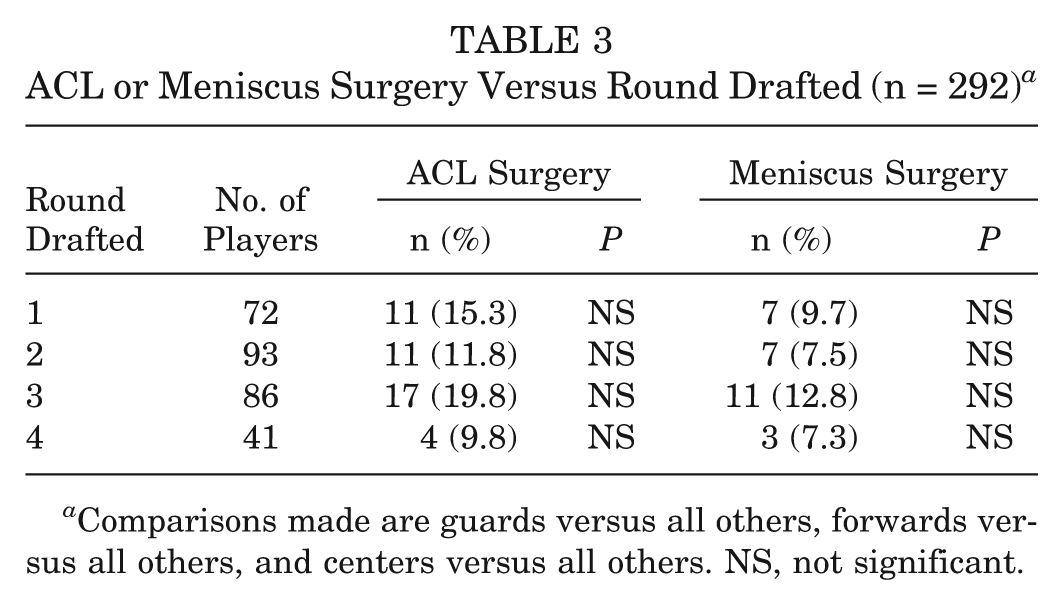
Comparisons made are guards versus all others, forwards versus all others, and centers versus all others. NS, not significant.
The data were also analyzed based on history of ACL and meniscus surgery and combine year for the 506 athletes in the combine. There was a decrease in the percentage of players with ACL reconstruction and with meniscus surgery entering the combine over time, but this was not statistically significant (Figure 1).
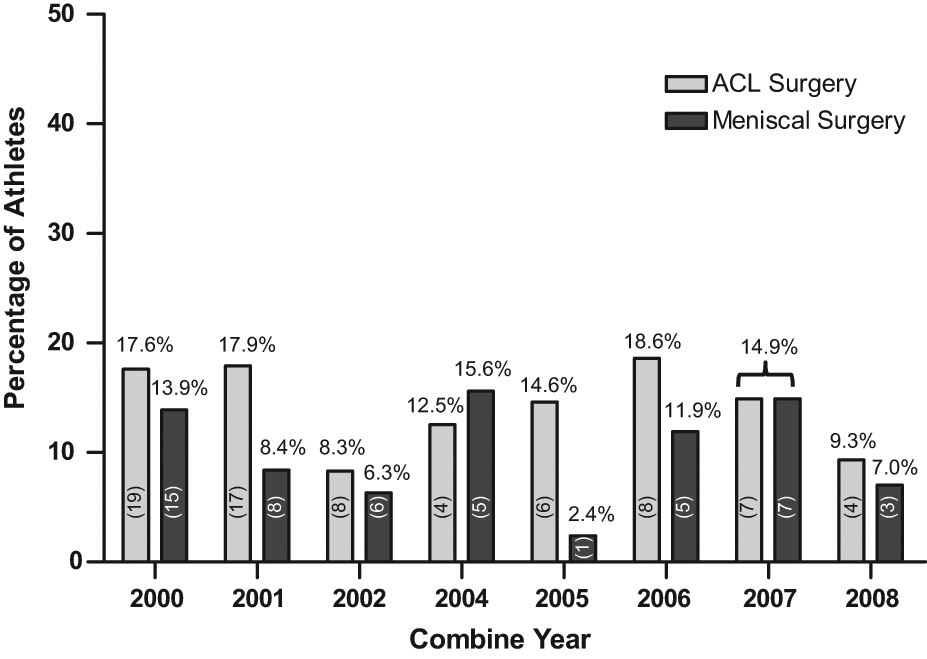
Percentage of athletes undergoing ACL and meniscus surgery in the Women’s National Basketball Association (WNBA) combine, 2000-2008.
Other Injuries
The other injuries that players reported included ankle sprain, patellar tendinitis, hand and wrist injury (including sprains and fractures), stress fracture, concussion, and shoulder injury. There were complete injury data in 506 players, with 364 players reporting other injuries (71.9%). Ankle sprain was the most common injury reported, with 242 athletes (47.8% of players) affected, followed by hand and wrist injury (105 athletes; 20.8%), patellar tendinitis (86 athletes; 17.0%), stress fracture (37 athletes; 7.3%), concussion (36 athletes; 7.1%), and shoulder injury (24 athletes; 4.7%). The injury data were analyzed based on year entering the combine. There were significantly more ankle sprains, hand/wrist injuries, and concussions reported in the more recent combine years than in the first years of the combine (Figure 2). The percentage of patellar tendinitis varied, and there were significantly more injuries reported in 2006 than in 2001 (P = .015), but no other significant differences were found. There were no significant differences based on combine year for stress fracture or shoulder injury.
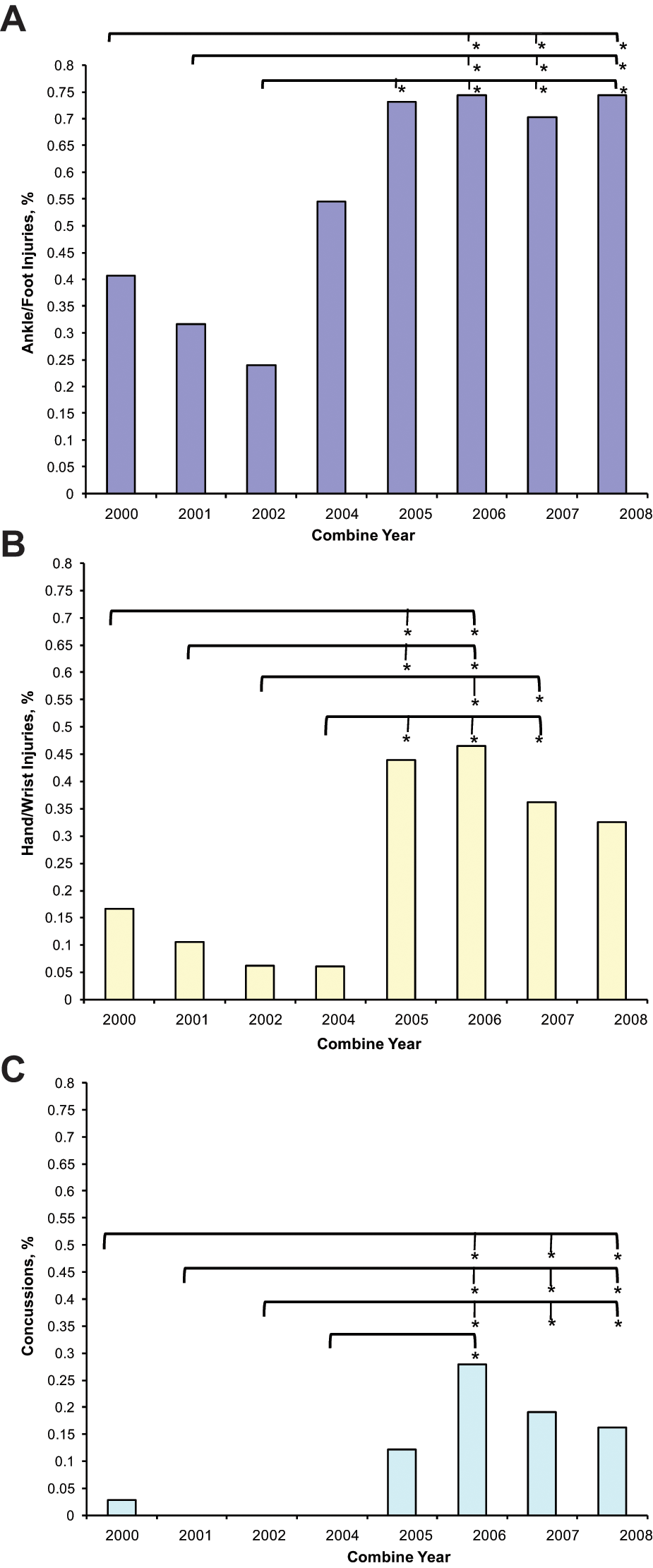
Percentage of (A) ankle/foot injuries, (B) hand/wrist injuries, and (C) concussions in the Women’s National Basketball Association (WNBA) combine, 2000-2008. *Significant difference (P ≤ .005).
Other Surgical Procedures
The other surgical procedures reported by combine athletes included knee arthroscopic surgery (excluding meniscus and ACL), foot and ankle surgery, and shoulder stabilization. Of the 506 athletes with complete injury data, 147 players reported other prior surgeries excluding ACL or meniscus surgery. Knee arthroscopic surgery was the most common surgical procedure followed by ankle reconstruction (13 athletes; 2.6%), shoulder stabilization (10 athletes; 2%), open knee surgery (9 athletes; 1.8%), tibial intramedullary nail for stress fracture (8 athletes; 1.6%), ankle arthroscopic surgery (8 athletes; 1.6%), nonmusculoskeletal surgery (7 athletes; 1.4%), exertional compartment syndrome release (6 athletes; 1.2%), lumbar laminectomy (4 athletes; 0.8%), elbow surgery (2 athletes; 0.4%), and hip surgery (2 athletes; 0.4%). Overall, 182 athletes (36.0%) reported a prior knee arthroscopic surgery including ACL and meniscus surgery. Excluding ACL and meniscus surgery, 59 athletes (11.7%) reported undergoing knee arthroscopic surgery. The knee arthroscopic surgery data are shown in Figure 3.
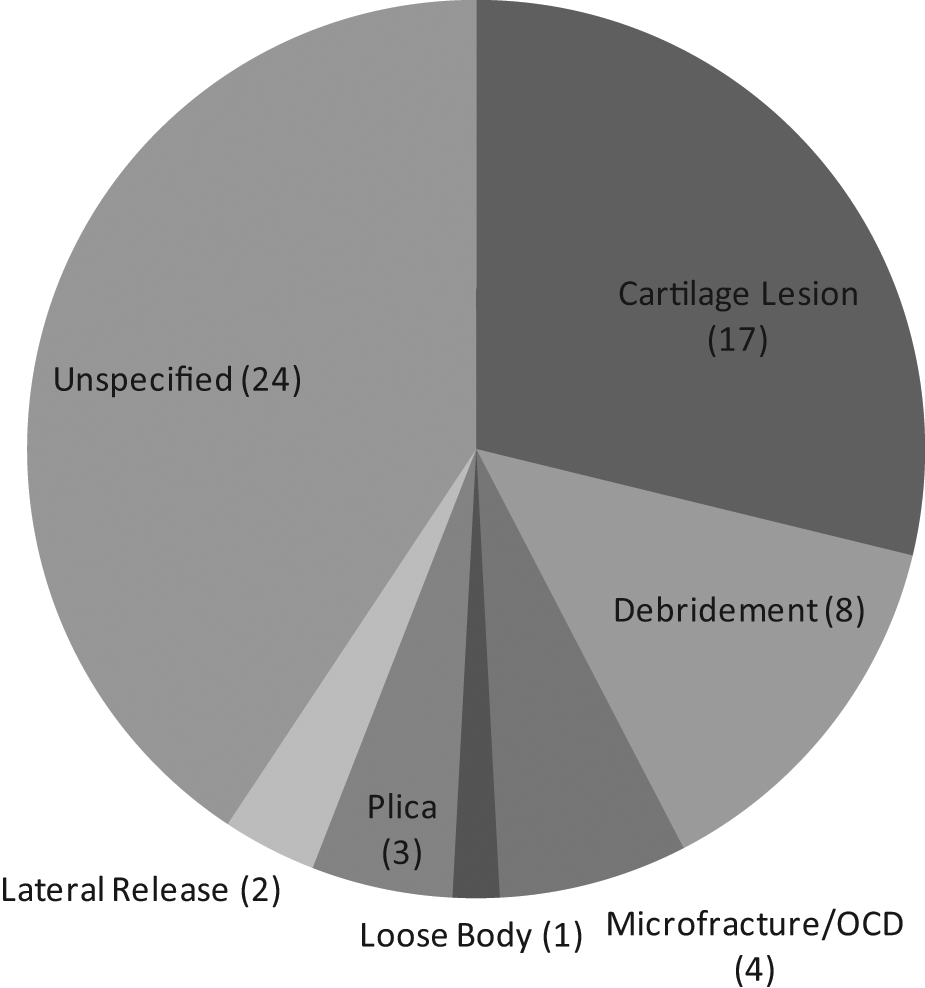
Number and indication for knee arthroscopic surgery (n = 59 athletes) in the Women’s National Basketball Association (WNBA) combine, 2000-2008. OCD, osteochondritis dissecans.
Career Length
Data on length of career in the WNBA were available for 220 athletes. Mean career length was 3.4 ± 2.8 years (range, 0-11 years). Thirty-six athletes with a history of ACL surgery had complete career length data. There were no differences in career length with a history of ACL surgery (mean, 3.8 ± 3.2 years) as compared with no ACL surgery (mean, 3.4 ± 2.9 years) (P = .526). Twenty-five athletes with a history of meniscus surgery had complete career length data. There were no differences in career length with a history of meniscus surgery (mean, 2.7 ± 2.5 years) as compared with no meniscus surgery (mean, 2.5 ± 2.2 years) (P = .696). Eight athletes had a history of an ACL surgery and a meniscus surgery. There were no differences in career length with a combined injury (mean, 3.3 ± 3.4 years) versus no injury (mean, 5.2 ± 3.6 years) (P = .220).
Survival analysis demonstrated no effect of previous ACL or meniscus surgery on length of career. Analysis of the data showed that players with a previous ACL surgery were approximately 20.6% more likely to have an extended playing career length versus those who had no history of ACL surgery (HR, 0.83; 95% CI, 0.51-1.36) (Figure 4A). Players who had a previous meniscus surgery had similar effects on career length. Players who had a previous meniscus surgery were 19.6% more likely to have a longer career length than those players who did not (HR, 0.84; 95% CI, 0.49-1.44) (Figure 4B). Having undergone both procedures had almost no effect on career length (HR, 0.93; 95% CI, 0.51-1.70) (Figure 4C).
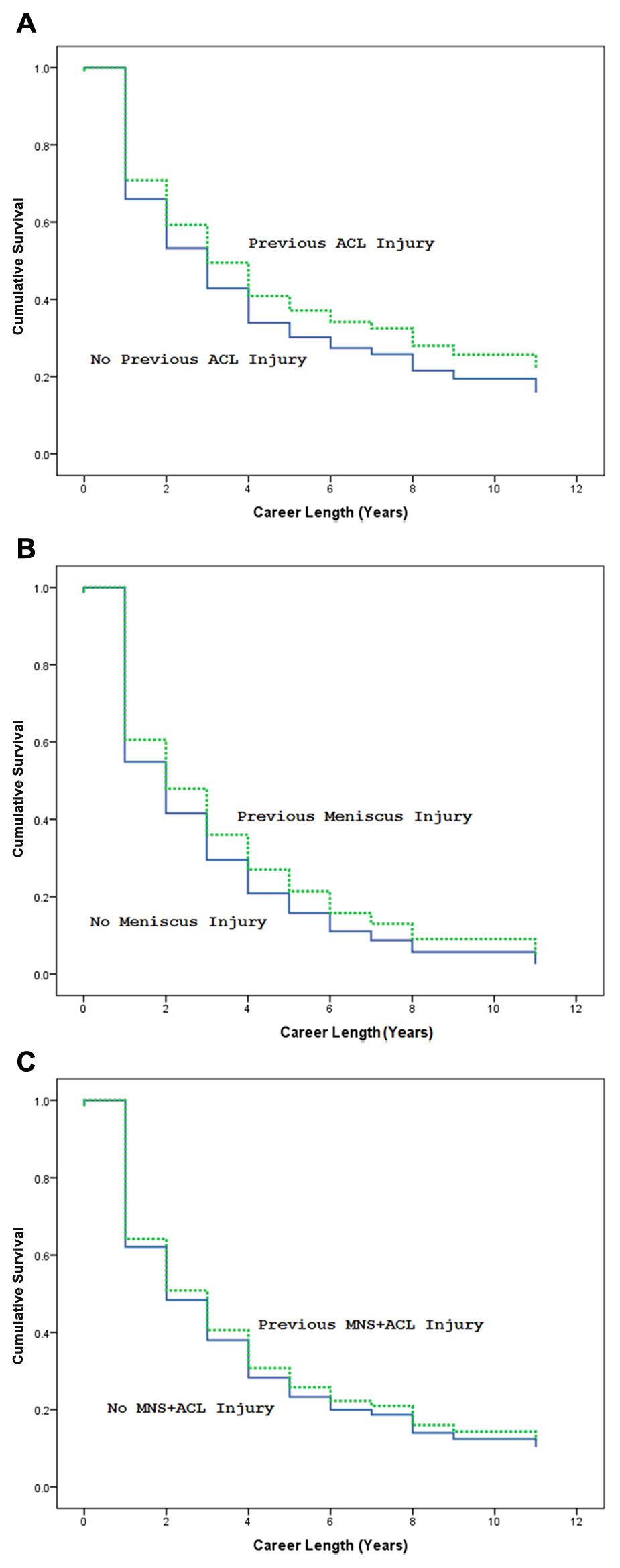
Survival analysis. Effect of (A) ACL surgery, (B) meniscus surgery, and (C) combined meniscus and ACL surgery (MNS+ACL) on career length.
Discussion
This is the first study to report the demographic and injury characteristics of athletes entering the WNBA combine. Both nonsurgical and surgical injuries were assessed to determine the incidence and potential effect on draft position and career length. Ankle sprains were the most common injury in players entering the WNBA combine, with 47.8% of players reporting a prior ankle sprain. This is consistent with other studies of basketball athletes from the collegiate to the professional level. § Messina et al 34 surveyed Texas high school basketball teams and found ankle sprains to be the most common injury in both male and female athletes. In an epidemiological prospective study of both interscholastic and collegiate basketball players, Hosea et al 24 found female athletes to be 25% more likely to suffer a grade I ankle injury than male athletes. The risk of ankle injury was doubled at the collegiate level compared with the high school level. Deitch et al, 8 in a retrospective review of 6 seasons of WNBA and NBA data, reported that the lower extremity (65%) was the most common site of injury, with lateral ankle sprains being the most common diagnosis.
Anterior cruciate ligament reconstruction was the most common surgical procedure performed on 14.4% of athletes entering the combine. Numerous studies have focused on the rate of ACL injury in female athletes at all levels. ‖ The majority of ACL tears occur between 15 and 25 years of age. 26 Agel et al 1 reviewed the NCAA injury surveillance system for both soccer and basketball athletes. The rate of ACL injury for female soccer players was 0.33 and for female basketball players was 0.29 per 1000 exposures. The rates for ACL injuries for women were statistically significantly higher (P < .01) than the rates for all ACL injuries for men, regardless of the sport. Deitch et al 8 reviewed WNBA injury data from 1997-2002 and found ACL injury comprised 0.9% of all injuries reported. The discrepancy between the number of collegiate and professional ACL injuries is likely caused by selection bias. The rate of ACL injury is greater in female collegiate and high school athletes when compared with professionals. Anterior cruciate ligament injury at a young age, and the subsequent sequelae, may result in the attrition of athletes who may have been capable of playing at a higher level. In addition, the low incidence of ACL injury occurring during professional play may reflect the strength, conditioning, and training programs used for injury prevention or a difference in intrinsic risk factors. 8 Our study also shows a trend toward a decrease in the percentage of players with ACL reconstructions entering the combine over time. This is in contrast to the statistically significant increase in ankle sprain, patella tendinitis, hand/wrist injury, and concussion in the later years of the combine, which may reflect an increasing intensity of play at the collegiate level. There are conflicting explanations for the decrease in ACL injuries reported. It is possible that the difference in ACL reconstruction reported by the WNBA combine athletes results from the strength, conditioning, and training programs designed to decrease injury risk at the high school and collegiate levels.2,47 Conversely, the apparent decline in ACL reconstruction may reflect a retirement from sport after ACL injury or a higher threshold for invitation to the WNBA combine. In addition, the number of athletes with bilateral ACL reconstructions, 17.8% or 13 athletes, suggests that there is a significant proportion of female athletes who may be more “at risk.” Determination of the risk factors for bilateral injury is an area that merits continued research.
No position player was more likely to have an ACL reconstruction than any other in our study. The published data on the role of position in ACL injury are conflicting. Gray et al 14 reported that ACL tears varied by playing position in high school female basketball players, with 78% of ACL tears occurring in guards while twisting or pivoting. However, Trojian and Collins 49 reported no variation in ACL incidence by position, and Meeuwisse et al 33 reported the highest number of injuries in centers followed by guards and then forwards. Guards and forwards are required to cover a larger surface area on both offense and defense, which may provide an explanation for the slightly but not significantly increased incidence of ACL injury compared with centers in our study.
Meniscus surgery was the second most common surgical procedure reported in this study. Prior studies of professional basketball players have reported that the majority of meniscus injuries are to the lateral (58%) versus medial (42%) side. 28 The WNBA data were collected as part of the combine and analyzed retrospectively and did not indicate whether the meniscus injury or surgery was medial or lateral. Meniscus surgery was not more prevalent in any particular position and did not affect draft position. There was insufficient power to determine the significance for the other knee injuries.
The most commonly reported prior injury and surgery occurred in the lower extremity (ankle sprain, patellar tendinitis, knee arthroscopic surgery, and ankle reconstruction), which is consistent with the literature. Deitch et al 8 reported that the lower extremity was the most commonly injured area in NBA and WNBA athletes (65% and 66%, respectively). Other common injuries reported were upper extremity injuries, followed by head trauma and cervical spine injuries, which is consistent with our data demonstrating hand/wrist trauma, shoulder injury, and concussion to be common injuries in athletes participating in the WNBA combine.
Brophy et al 7 reported on National Football League (NFL) players from the 1987-2000 seasons and concluded that meniscus injury alone, but not ACL reconstruction alone, reduced the probability of playing and the longevity of careers in players going through the NFL combine. The combination of ACL reconstruction and meniscectomy was most detrimental to player longevity. 7 Our survival analyses showed that a meniscus surgery, an ACL surgery, or a combined injury did not affect the length of career in the WNBA. This is encouraging information for future players who sustain meniscus or ACL injuries before professional competition. However, further study is needed to examine the reasons why these injuries are not detrimental to career length in the WNBA as compared with the NFL and other professional sports.
This study has some limitations. The accuracy of player data is based on reporting by athletes and collegiate training staff, which may introduce recall bias. Not all players in the WNBA go through the combine, with some signing as free agents; thus, this study does not capture all WNBA athletes. Although ACL or meniscus surgery did not affect draft position, players who were unable to return to high-level collegiate competition may not have been successful enough to gain an invitation to the combine. The current study provides a framework for future studies utilizing the WNBA injury database to determine the details of injuries sustained during a professional career and the effect that those injuries have on longevity in the WNBA.
Footnotes
Acknowledgements
Special thanks to the WNBA and to Lisa White for help with data collection.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.