
Abstract
Background:
There have been no previous studies showing clinical outcomes according to treatment options of posterior cruciate ligament (PCL) injury with mild grade 2 or less posterior translation (<7 mm) combined with posterolateral rotatory instability.
Purpose:
To compare the clinical outcomes of posterolateral corner (PLC) reconstruction with or without simultaneous PCL reconstruction in PCL injuries with mild posterior translation.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 46 patients with a PCL injury with mild posterior translation combined with posterolateral rotatory instability were retrospectively reviewed. Twenty-two patients had undergone isolated PLC reconstruction (group A), and 24 patients had undergone simultaneous reconstruction of the PCL and PLC (group B). Each patient was assessed for knee instability with the dial test at 30° and 90° as well as with varus and posterior stress radiography and were evaluated with the Lysholm knee score and International Knee Documentation Committee (IKDC) subjective and objective grading.
Results:
In all cases, the minimum follow-up period was 24 months. At the final follow-up evaluation, no significant side-to-side difference was found on varus stress radiography (group A, 1.55 ± 0.78 mm vs group B, 1.35 ± 1.00 mm; P = .458) or the dial test (at 30°: group A, 4.00° ± 1.83° vs group B, 4.04° ± 1.30°; P = .929; at 90°: group A, 3.64° ± 1.18° vs group B, 3.67° ± 1.37°; P = .937). However, group B showed a significant improvement compared with group A on posterior stress radiography (group A, 0.16 ± 0.44 mm vs group B, –1.44 ± 0.74 mm; P < .001), Lysholm knee score (group A, 18.36 ± 8.73 vs group B, 23.42 ± 7.44; P = .040), IKDC subjective score (group A, 25.51 ± 7.11 vs group B, 33.08 ± 5.89; P < .001), and IKDC objective score (group A preoperatively: grade C = 19 patients, grade D = 3; group B preoperatively: grade C = 20, grade D = 4; group A postoperatively: grade B = 11, grade C = 11; group B postoperatively: grade A = 12, grade B = 9, grade C = 3) (P < .001).
Conclusion:
Simultaneous reconstruction of the PCL and PLC is recommended when addressing PCL injuries with mild grade 2 or less posterior translation combined with posterolateral rotary instability.
Keywords
Combined injury of the posterior cruciate ligament (PCL) and the posterolateral corner (PLC) is a challenging problem. Isolated reconstruction of the PCL without reconstruction of PLC insufficiency has shown poor clinical outcomes.4,14,19 Cases of PCL injury with grade 2 posterior translation accompanied by PLC insufficiency are treated by reconstruction of both structures, whereas knees with isolated grade 2 or less posterior translation tend not to be reconstructed surgically and have good clinical outcomes without reconstruction.2,23,25,26 However, no study on clinical outcome according to the treatment option of PCL injuries with grade 1 (<5 mm) posterior translation combined with posterolateral rotatory instability has been reported previously. The purpose of this study was to compare the clinical outcomes of reconstruction of the PLC with or without simultaneous reconstruction of the PCL in injured knees with mild grade 2 or less posterior translation. We hypothesized that the results of isolated reconstruction of the PLC without reconstruction of the PCL would be similar to those of simultaneous reconstruction of the PCL and PLC in terms of clinical outcomes.
Materials and Methods
Patients
We retrospectively reviewed the medical records of 201 patients who underwent PLC reconstruction between November 2002 and August 2008. All surgeries were performed by the senior author (S.-J.K.). This study included patients who had combined PLC and PCL insufficiency with mild grade 2 or less posterior translation. The PLC insufficiency was treated by anatomic reconstruction of the lateral collateral ligament (LCL), popliteus tendon, and popliteofibular ligament (PFL) using a tibialis posterior tendon allograft. Surgical indications for posterolateral instability included a positive reverse pivot-shift test result and a difference of greater than 10° in external rotation compared with the normal contralateral knee as assessed by the dial test at 30° and 90° of knee flexion. Increased varus gap of the affected knee of more than 3 mm compared with the normal contralateral knee on varus stress radiography and subjective functional deficit associated with pain and instability were also indications for surgery. All patients underwent magnetic resonance imaging (MRI) before surgery. The injury status of the PCL and component of the PLC was confirmed radiologically. The range of mild grade 2 or less posterior translation was arbitrarily defined as a side-to-side difference (SSD) of 3 to 7 mm to include grade 1 together with borderline grades 1 and 2.
Patients were excluded according to the following exclusion criteria: (1) previous surgery on the affected knee, (2) instability of the contralateral knee, (3) PCL avulsion fracture, (4) malalignment of the lower extremity (>5 mm of mechanical axis deviation as measured by standing hip-knee-ankle radiographs), (5) grade 3 or higher chondral lesion according to the Outerbridge grading system at arthroscopic examination, 21 (6) a severe meniscal injury requiring subtotal or total meniscectomy, (7) concomitant ligament injuries other than the PCL or PLC, or (8) inadequate duration of follow-up of less than 24 months. Nine patients who had an insufficient duration of follow-up were excluded from the current study: 4 patients in group A and 5 patients in group B.
Forty-six patients were included in this study. Group A consisted of 22 patients who had undergone isolated reconstruction of the PLC without reconstruction of the PCL between November 2002 and October 2005. Group B consisted of 24 patients who were treated with simultaneous reconstruction of the PCL and PLC between June 2005 and August 2008. Anterolateral transtibial single-bundle PCL reconstruction with an allogenic Achilles tendon–bone graft with a 1-incision technique 11 was used in group B. Institutional review board approval was obtained.
Operative Procedures
Anterolateral Transtibial Single-Bundle PCL Reconstruction With Use of an Achilles Tendon–Bone Allograft With a 1-Incision Technique 11
To reconstruct the PCL more conveniently, 3 unique portals were used: a high medial parapatellar portal, a far anterolateral portal, and a high posteromedial portal. 10 For the tibial tunnel, a PCL guide inserted through the high medial parapatellar portal passed through the intercondylar notch and was positioned about 1.5 cm below the articular surface and just lateral to the midline on the PCL fossa. The tunnel was made on the anterolateral tibial cortex to reduce graft angulation. The femoral socket was made through the far anterolateral portal. The center of the femoral socket was placed 8 mm posterior from the articular junction at the 10:30 clock position for the left knee and the 1:30 clock position for the right knee. An Achilles tendon–bone allograft was used. For tibial fixation, the bone plug was trimmed to 11 mm in width and 25 mm in length. The tendon was prepared to 11 mm in width and 60 mm in length. For femoral fixation, the tendon was threaded 30 mm in length with a whipstitch technique, and a 9-mm EndoPearl (Linvatec, Largo, Florida) was attached to the end of the tendon. The fixation of grafts in the femoral socket and tibial tunnel was achieved with bioabsorbable interference screws.
Anatomic Reconstruction of the LCL and Popliteus Tendon With Use of a Tibialis Posterior Allograft for PLC Insufficiency 13
A skin incision was made from just anterior to the fibular head to the lateral femoral epicondyle. The interval between the iliotibial tract and the biceps tendon was developed. For popliteus tendon reconstruction, the tibial tunnel was made from the Gerdy tubercle to a point 10 mm inferior from the posterior joint line and 5 mm medial to the posterior aspect of the tibiofibular joint. The proximal insertion site was located at the superior margin of the anterior one fifth of the popliteal sulcus, about 10 mm anterior and 15 mm distal to the lateral femoral epicondyle at the isometric point where migration of the tendon was less than 2 mm during knee flexion and extension. For LCL reconstruction, the fibular tunnel was made from the anteroinferior aspect of the fibular head 10 mm above the peroneal nerve to the point just posteromedial to the LCL of the fibular head. The proximal insertion site was placed at the lateral epicondyle after an isometric test was performed. A tibialis posterior tendon allograft was used. Each tendon end was threaded 25 mm in length with a whipstitch technique, and a 7-mm EndoPearl was attached to the end of the tendon. The tendon was fixed using a bioabsorbable interference screw. The distal portion of the reconstructed popliteus tendon was sutured to the posterosuperior ligamentous tissue of the fibular head to restore the function of the PFL (Figure 1).
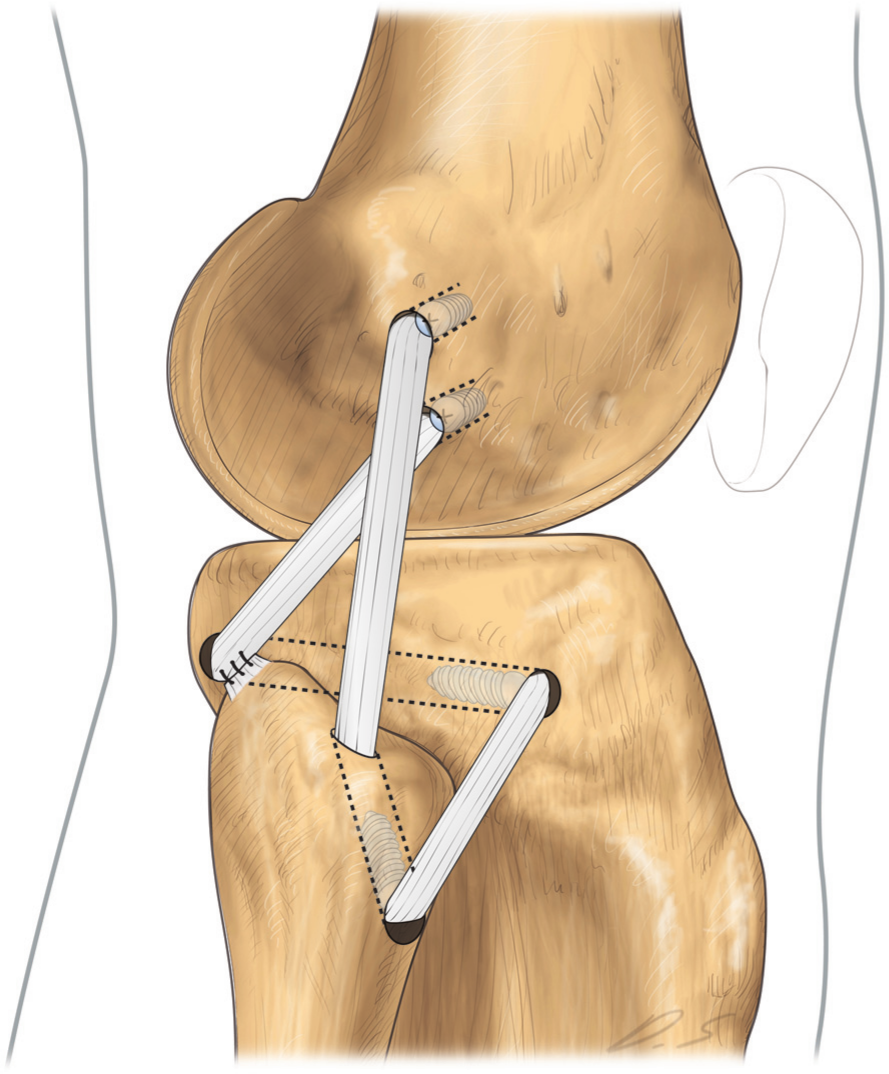
Anatomic reconstruction of the lateral collateral ligament, popliteus tendon, and popliteofibular ligament with use of a tibialis posterior allograft was performed for posterolateral corner insufficiency.
Postoperative Rehabilitation
All patients in both groups followed an identical postoperative rehabilitation protocol. The involved knee was immobilized in extension with a hinged knee brace for the first 4 to 6 weeks. Quadriceps strengthening and mobilization with patellar exercises were initiated immediately after surgery. Toe-touch weightbearing was allowed. Passive range of motion exercise was allowed 3 times a day from 2 weeks as tolerated. After the first 4 to 6 weeks, weightbearing with crutches as tolerated and limited flexion of the knee with a gradual increase up to 90° were encouraged. At 8 to 10 weeks after surgery, the brace was removed and closed kinetic chain exercises initiated. At 12 to 14 weeks after surgery, stationary bicycle, stair climbing, full flexion, and squatting were allowed. At 4 to 5 months, swimming and cycling were permitted. Return to sports activity involving jumping and pivoting was permitted at 6 to 9 months after surgery.
Clinical Assessment
Postoperative follow-up examinations were conducted at 3 and 6 months after surgery and then annually. The preoperative and latest follow-up values measured between 2 and 4 years after surgery were assessed. All manual examinations were performed by the senior author (S.-J.K.) and trained orthopaedic fellows. Radiological evaluation by stress radiography was performed by 2 different clinical fellows, who were blinded to the study to increase the reliability of measurements. The mean of these 2 numerical values was used. The PCL laxity was evaluated with posterior translation on lateral stress radiography, and varus laxity was evaluated with varus gap on anteroposterior stress radiography using a Telos stress device (Telos, Marburg, Germany) with a load of 15 kPa at 90° and 30° of flexion, respectively. To measure posterior instability, the bony landmarks and method to measure the magnitude of translation described by previous reports were used.16,22,27 One horizontal line tangential to the tibial plateau was drawn. Two additional vertical lines perpendicular to this horizontal line were drawn. Each line passed the midpoint between the vertical lines tangential to the most posterior outlines of both femoral condyles and both tibial plateaus, respectively. The distance between these 2 vertical lines was considered the degree of posterior translation (Figure 2). To measure varus instability, the method described by Jakobsen 8 was employed. One line tangential to the most distal portion of the medial and femoral condyles and another line tangential to the most proximal subchondral bone of the medial and lateral tibial plateaus were drawn. One line tangential to the lateral border of the proximal tibia was drawn perpendicular to the tibial line. The distance of this vertical line between the femoral and tibial horizontal lines was considered the degree of varus gap (Figure 3). The stress radiographs were evaluated via a picture archiving and communication system (Centricity PACS, GE Medical System Information Technologies, Milwaukee, Wisconsin).
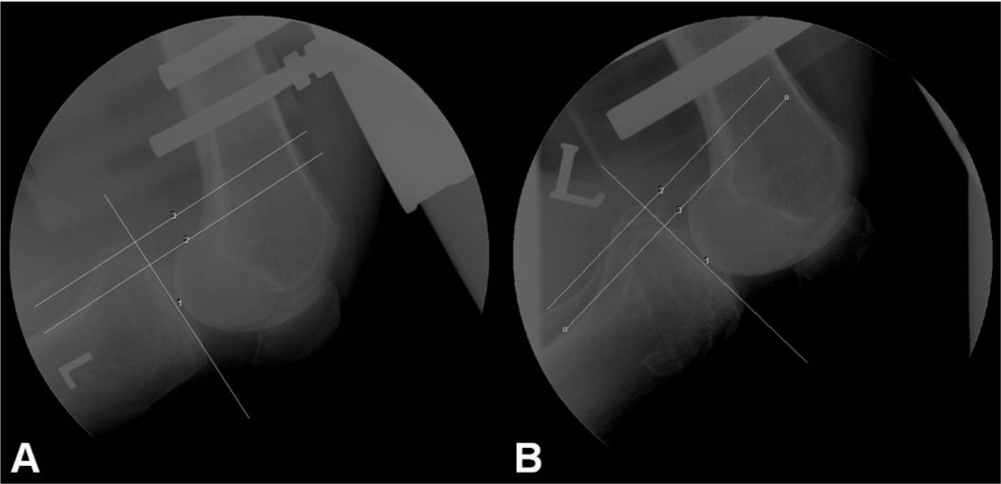
(A) The preoperative measurement of posterior translation on posterior stress radiography of a 32-year-old man in group A. One horizontal line tangential to the tibial plateau was drawn. Two additional vertical lines perpendicular to this horizontal line were drawn. Each line passed the midpoint between the vertical lines tangential to the most posterior outlines of both femoral condyles and both tibial plateaus, respectively. The distance between these 2 vertical lines was considered the degree of posterior translation. (B) The postoperative posterior stress radiograph of the same patient at 27 months after surgery.
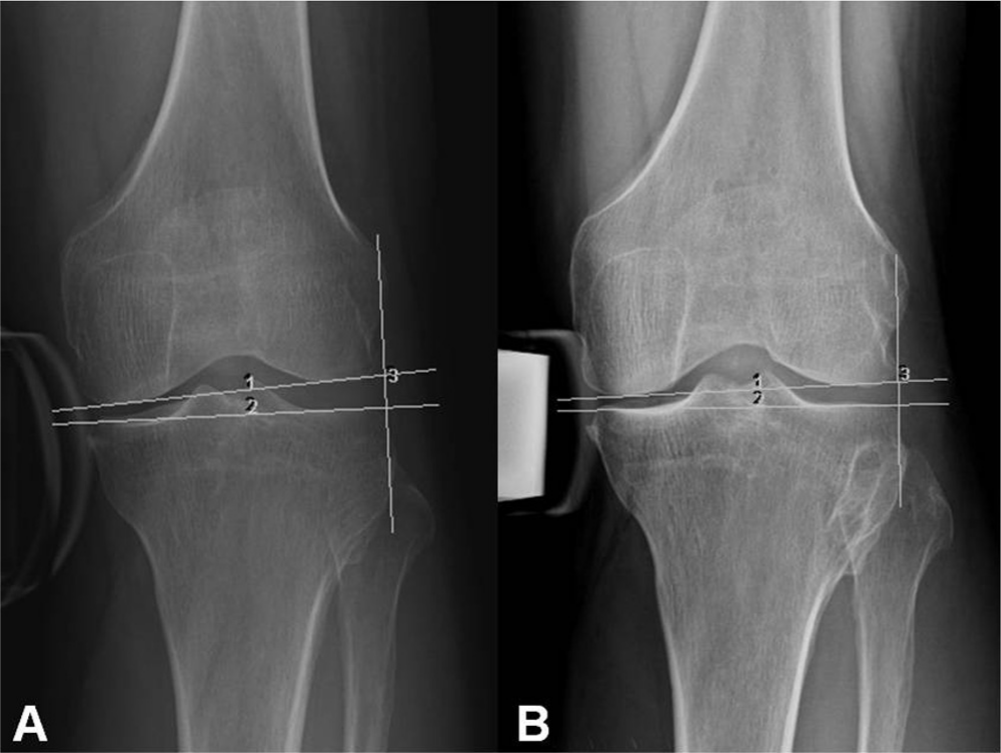
(A) The preoperative measurement of varus instability on varus stress radiography of a 32-year-old man in group A. One line tangential to the most distal portion of the medial and femoral condyles and another line tangential to the most proximal subchondral bone of the medial and lateral tibial plateaus were drawn. One line tangential to the lateral border of the proximal tibia was drawn perpendicular to the tibial line. The distance of this vertical line between the femoral and tibial horizontal lines was considered the degree of varus gap. (B) The postoperative varus stress radiograph of the same patient at 27 months after surgery.
The degree of external rotation was evaluated with the dial test. The patient was in a prone position with the knees at 30° and 90° of flexion. External rotation of the leg was performed with the patient’s foot. When the maximal degree of rotation with no more external rotation was reached with manual force, the angles between the axis of the medial border of the foot and long axis of the femur with the knees at 30° and 90° of flexion were measured with a goniometer. The values of the affected knee were compared with those of the normal contralateral knee for SSDs. The preoperative and postoperative functional outcomes were assessed with the Lysholm knee scoring scale and the International Knee Documentation Committee (IKDC) subjective score and examination form.5,15
Statistical Analysis
Both groups were compared with an independent 2-sample t test for continuous numerical data, satisfying the normality assumption, and the Fisher exact test for categorical data. Comparison between preoperative and postoperative data in the same group was performed with a paired t test for continuous numerical data and the McNemar test for categorical data. A simple linear regression analysis was used to identify preoperative variables (posterior translation, varus gap, degree of external rotation with the knees at 30° and 90° of flexion, Lysholm score, IKDC subjective score and objective grade, age, duration from injury to surgery, and additional diagnosis) that significantly influence the changes in postoperative Lysholm score and IKDC subjective score. The interobserver reliability in measuring the radiological variables was evaluated with intraclass correlation coefficients (ICCs) with 95% confidence intervals. Statistical analysis was performed using SPSS software (version 19, SPSS Inc, Chicago, Illinois). The level of significance was set at P < .05.
Results
Patient Demographics
Group A consisted of 22 patients including 20 male and 2 female patients, and group B consisted of 24 patients including 17 male and 7 female patients (P = .139). The mean age at the time of surgery was 39.0 years in group A and 40.3 years in group B (P = .715). The mean duration of time from injury to surgery was 45.0 months in group A and 27.3 months in group B (P = .301). The mean duration of postoperative follow-up was 33.5 months for group A and 35.4 months for group B (P = .322) (Table 1). The mechanism of trauma in groups A and B is listed in Table 1.
Patient Demographic Data a
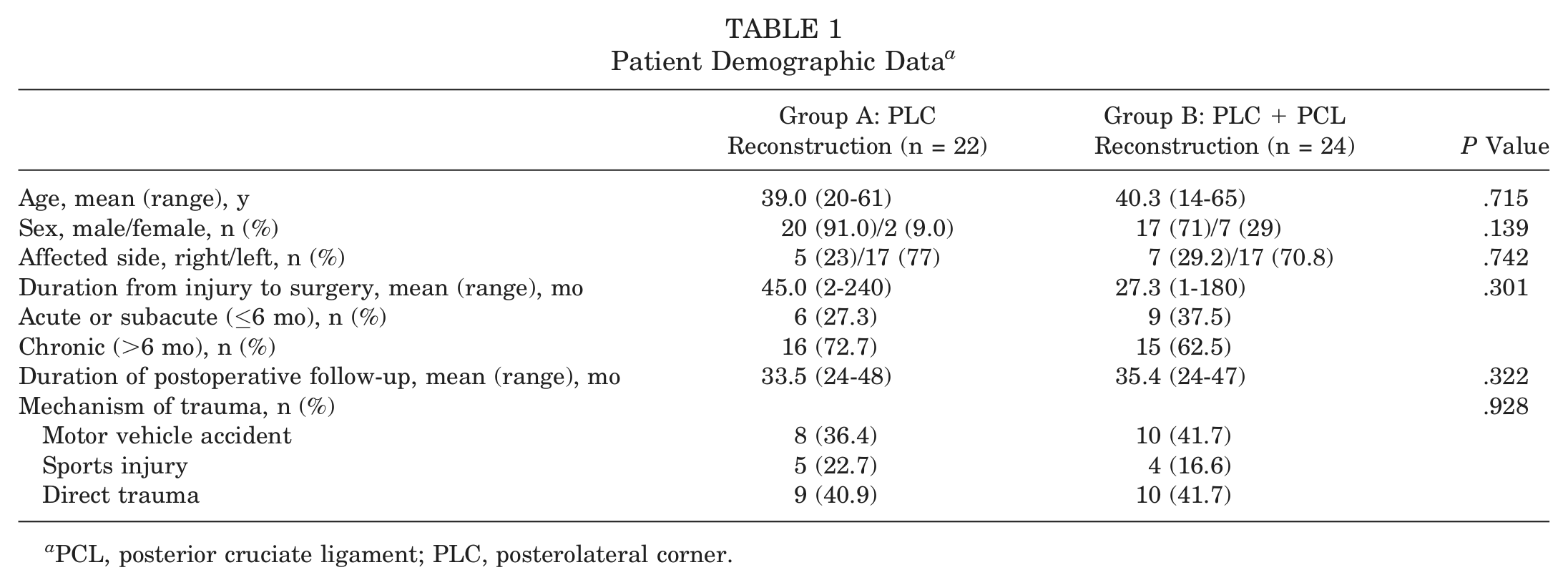
PCL, posterior cruciate ligament; PLC, posterolateral corner.
Magnetic resonance imaging showed an injury to the LCL in 20, the popliteus tendon in 6, and the biceps femoris tendon in 12 of 22 cases in group A. Also, MRI showed an injury to the LCL in 22, the popliteus tendon in 8, and the biceps femoris tendon in 16 of 24 cases in group B (Figure 4). Additional arthroscopic findings showed 2 cases of meniscal tears treated with partial meniscectomy, 5 cases of Outerbridge grade 1 or 2 chondromalacia, 1 case of medial patellar plica, and 1 case of a loose body in group A. In group B, 2 cases of meniscal tears treated with partial meniscectomy and 2 cases of Outerbridge grade 1 or 2 chondromalacia were noted.
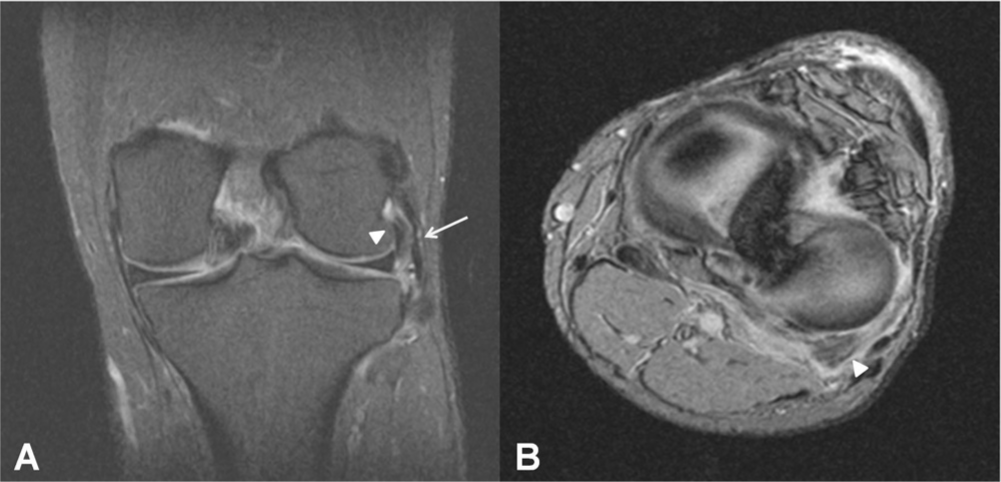
Preoperative magnetic resonance imaging scans of a 50-year-old man in group B. (A) Proton density–weighted coronal image with fat saturation showed a sprain of the proximal lateral collateral ligament (arrow) and a popliteus tendon injury (arrowhead). (B) Gradient echo T2*-weighted axial image showed hyperintensity of the popliteus musculotendinous junction (arrowhead).
Posterior Translation on Stress Radiography
In group A, the mean preoperative SSD on posterior stress radiography was 4.84 ± 1.05 mm (ICC = 0.931). Ten cases were grade 1 (<5 mm), and 12 cases were grade 2 (>5 mm). In group B, the mean preoperative SSD on posterior stress radiography was 5.02 ± 0.85 mm (ICC = 0.856). Thirteen cases were grade 1, and 11 cases were grade 2. There was no significant statistical difference between the 2 groups (P = .525) (Table 2). The mean postoperative SSD at the follow-up was 5.02 ± 0.99 mm (ICC = 0.908) in group A and 3.58 ± 0.50 mm (ICC = 0.845) in group B (Table 3). A significant difference was noted statistically (P < .001). A comparison of the amount of difference before and after surgery between group A and group B also showed a statistically significant difference (P < .001) (Table 4).
Comparison of Preoperative Variables Between Groups a
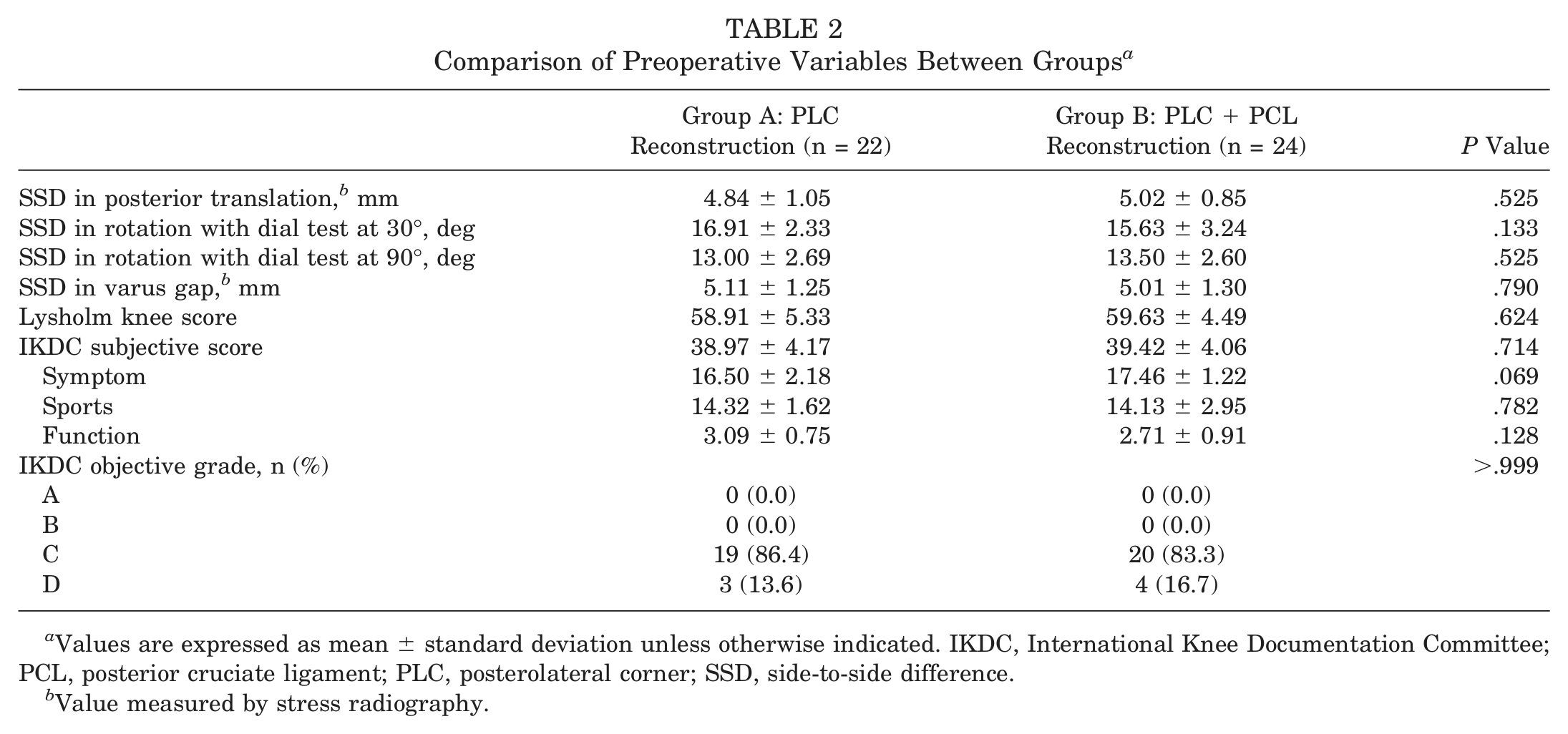
Values are expressed as mean ± standard deviation unless otherwise indicated. IKDC, International Knee Documentation Committee; PCL, posterior cruciate ligament; PLC, posterolateral corner; SSD, side-to-side difference.
Value measured by stress radiography.
Comparison of Postoperative Variables Between Groups a
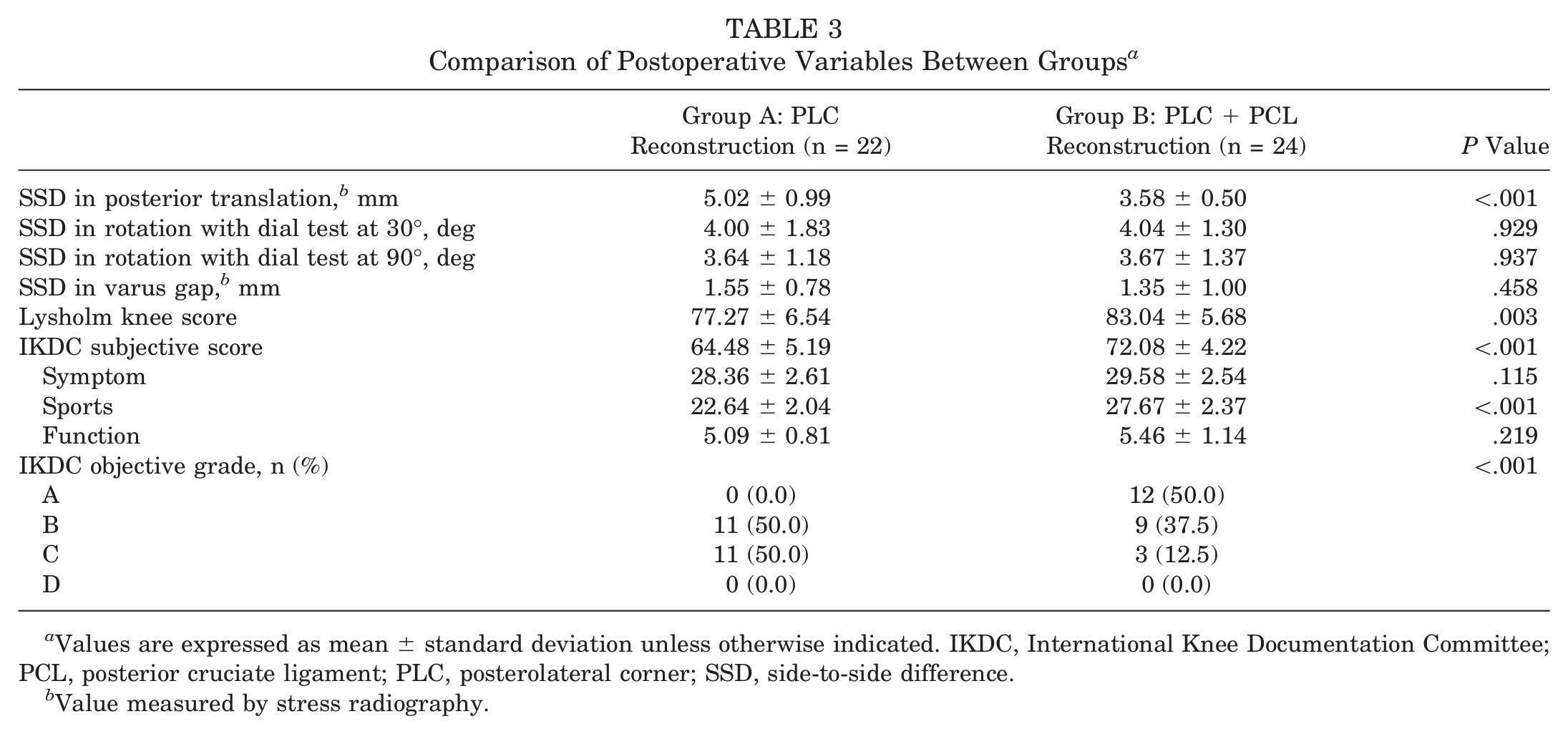
Values are expressed as mean ± standard deviation unless otherwise indicated. IKDC, International Knee Documentation Committee; PCL, posterior cruciate ligament; PLC, posterolateral corner; SSD, side-to-side difference.
Value measured by stress radiography.
Comparison of Amount of Difference Before and After Surgery Between Groups a
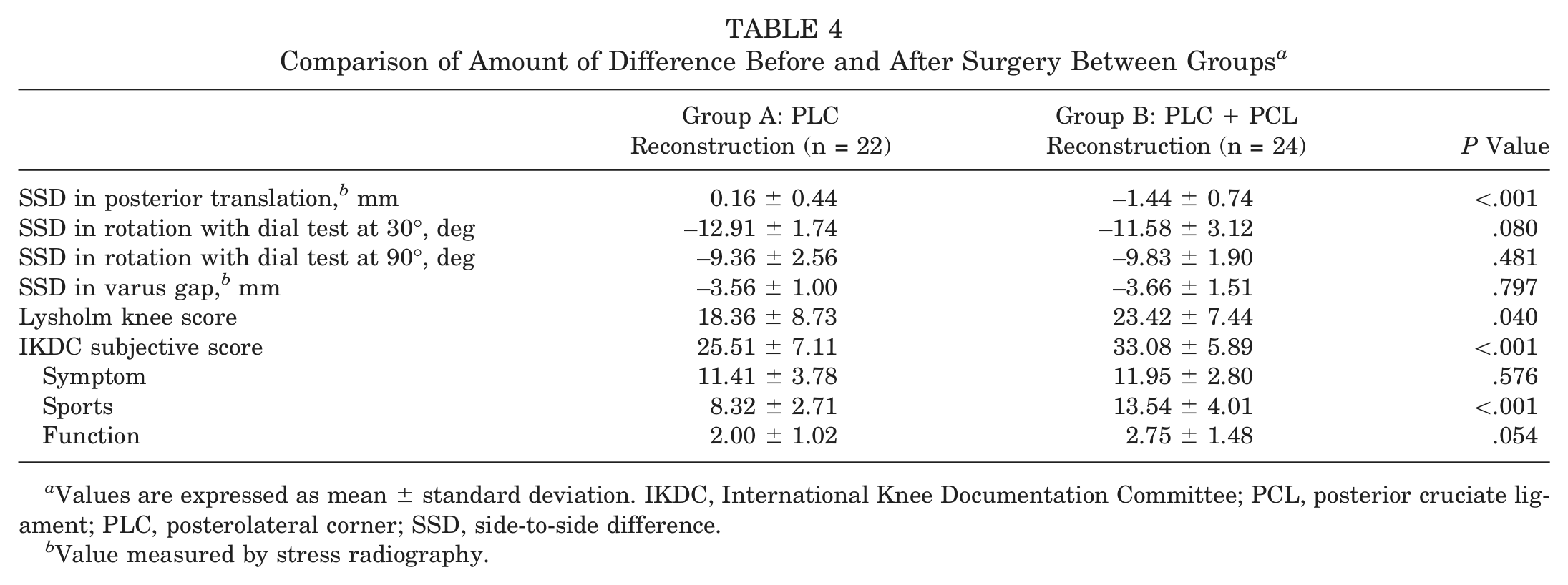
Values are expressed as mean ± standard deviation. IKDC, International Knee Documentation Committee; PCL, posterior cruciate ligament; PLC, posterolateral corner; SSD, side-to-side difference.
Value measured by stress radiography.
External Rotatory Instability by Dial Test
In group A, the mean preoperative SSD in external rotation was 16.91° ± 2.33° (ICC = 0.632) with the dial test at 30° and 13.00° ± 2.69° (ICC = 0.973) with the dial test at 90°; in group B, means of 15.63° ± 3.24° (ICC = 0.856) with the dial test at 30° and 13.50° ± 2.60° (ICC = 0.760) with the dial test at 90° were noted. There was no statistically significant difference between the 2 groups (P = .133 and P = .525, respectively) (Table 2). The mean postoperative SSD at the follow-up was 4.00° ± 1.83° (ICC = 0.759) with the dial test at 30° and 3.64° ± 1.18° (ICC = 0.715) with the dial test at 90° in group A and 4.04° ± 1.30° (ICC = 0.684) with the dial test at 30° and 3.67° ± 1.37° (ICC = 0.513) with the dial test at 90° in group B. No significant difference between the 2 groups was shown statistically (P = .929 and P = .937, respectively) (Table 3).
Varus Gap on Stress Radiography
The mean preoperative SSD in varus gap on stress radiography with the knee flexed at 30° was 5.11 ± 1.25 mm (ICC = 0.949) in group A and 5.01 ± 1.30 mm (ICC = 0.953) in group B (Table 2). The mean postoperative SSD at the follow-up was 1.55 ± 0.78 mm (ICC = 0.950) in group A and 1.35 ± 1.00 mm (ICC = 0.973) in group B (Table 3). No significant statistical difference between the 2 groups was noted (P = .790 preoperatively and P = .458 postoperatively).
Clinical Outcome Assessment by Knee Scores
There was no significant difference between the 2 groups with regard to any of the following preoperative variables: Lysholm knee score (P = .624), IKDC subjective score (P = .714), and IKDC objective grade (P > .999) (Table 2). The mean score of function before knee injury on the IKDC score was 9.72 in group A and 9.66 in group B (P = .664). The mean postoperative Lysholm knee score in group A was 77.27 ± 6.54, and the mean score in group B was 83.04 ± 5.68. Group B showed a statistically more significant improvement than group A (P = .003). In regard to the postoperative IKDC subjective score, group B (72.08 ± 4.22) had a better outcome than group A (64.48 ± 5.19) (P < .001). Group B (27.67 ± 2.37) had a statistically better result than group A (22.64 ± 2.04) concerning sports (P < .001). A comparison between postoperative objective grades of the 2 groups showed that group B had a better outcome than group A (P < .001): 11 cases of grade B and 11 cases of grade C in group A, and 12 cases of grade A, 9 cases of grade B, and 3 cases of grade C in group B (Table 3). A comparison of the amount of difference before and after surgery between the 2 groups also showed that group B displayed a significant improvement as compared with group A in regard to the Lysholm knee score (P = .040) and the total sum (P < .001) and sports component (P < .001) of the IKDC subjective score (Table 4). A simple linear regression analysis employed to identify preoperative variables that significantly influenced changes in the postoperative Lysholm score and IKDC subjective score showed that only duration from injury to surgery in group B had a significant effect on the IKDC subjective score statistically (β = –.06; P = .002).
Complications
There was 1 case of cortical breakage of the fibular head while making a fibular tunnel in group B. A firm fixation was not achieved with bioabsorbable interference screws; therefore, immobilization was maintained for 6 weeks.
Discussion
The PCL and PLC are complementary to each other in stabilizing the knee joint. The PCL is a primary restraint to posterior tibial translation through range of motion of the knee, and the PLC is an important secondary restraint to posterior tibial translation on the lateral tibiofemoral compartment. Regarding varus rotation, the PLC including the LCL is the most important restraint to varus stress. 6 With injuries to these structures, the PCL is placed under high loading conditions.3,17 The PCL and PLC are 2 main restraints to external tibial rotation. The PLC is the primary restraint at low flexion angles, and both the PCL and PLC are the main restraints at high flexion angles. 20 In assessing injuries to these 2 structures, the mutual relationship between the PCL and PLC has to be considered. A failure to recognize posterolateral instability is one of the causes of poor outcome after PCL reconstruction. Further, PCL insufficiency of grade 3 is usually accompanied by a PLC injury, in which case simultaneous reconstruction of these 2 structures is recommended.4,14,19 However, no study on how to treat a PCL injury with grade 1 posterior translation combined with posterolateral rotatory instability has been reported previously.
This study consisted of patients with less than 7-mm posterior translation (grade 1 together with borderline grades 1 and 2 on stress radiography). The patients were assigned to either group A or group B according to the treatment method for a PCL injury. Nonoperative management was used to treat mild grade posterior translation until 2005, but there were some cases with poor outcomes. Therefore, the treatment method for posterior instability was changed to operative management to compare the 2 options in treating PCL injuries with mild grade 2 or less posterior translation combined with posterolateral rotatory instability.
The hypothesis we assumed was that the results of isolated reconstruction of the PLC without reconstruction of the PCL would be similar to those of simultaneous reconstruction of the PCL and PLC in terms of clinical outcomes. The hypothesis included 2 issues to verify posterolateral and posterior stability. The first issue was whether a surgically reconstructed PLC was affected by the remaining PCL insufficiency without reconstruction. In this study, there was no significant difference in posterolateral stability between the 2 groups. External rotation with the knees at 30° and 90° of flexion and varus gap on stress radiography did not show any significant difference. The method of PLC reconstruction employed in this study was to reconstruct the LCL, popliteus tendon, and PFL anatomically. These are principal components of the PLC and primary restraints to varus rotation and external rotation. Recent biomechanical and clinical studies have compared different techniques of PLC reconstruction.1,9,12,18 Kim et al 12 reported that anatomic reconstruction of the popliteus tendon and LCL resulted in better outcomes than a modified biceps rerouting tenodesis. In the current study, the postoperative posterolateral stability achieved with anatomic PLC reconstruction was considered to be unaffected by the remaining posterior insufficiency.
The second issue was whether unreconstructed mild grade 2 or less posterior insufficiency in combined cases of PCL and PLC injury showed similar clinical outcomes to nonoperative treatment of an isolated PCL injury. Some studies noted that nonoperative treatment of an isolated PCL injury with less than grade 3 achieved acceptable functional stability.2,23,25,26 According to Shelbourne et al, 23 isolated grade 2 or less PCL injury treated nonoperatively showed the same or less PCL laxity at the time of the initial injury examination. Shino et al 26 reported that 15 patients with isolated PCL laxity who underwent nonoperative treatment had good clinical outcomes at a mean of 51 months. This is because of the good healing potential of the PCL induced by abundant synovial coverage and blood circulation.23,24 In the current study, there was no statistically significant difference between preoperative and postoperative PCL laxity in group A. This result was similar to the outcomes of cases of isolated PCL injury reported in a previous study. 23 However, group B showed statistically more improvement than group A when comparing postoperative PCL laxity between the 2 groups. The clinical subjective score of the Lysholm knee scale and the IKDC subjective score also showed better outcomes in group B than in group A. The difference in the mean SSD in posterior translation between the 2 groups was relatively small, but the difference in the clinical scores showed a statistically significant distinction between the 2 groups.
According to previous studies, there was no correlation between the PCL laxity grade and subjective scores.23,25 The IKDC subjective knee evaluation form is composed of symptom, sports, and function components. The sports score of the IKDC subjective form showed a remarkable difference. The patients after isolated reconstruction of the PLC without reconstruction of the PCL were considered to have a similar symptom score to simultaneous reconstruction of the PCL and PLC but to have more limited activities of daily living, including sports activities. Group A, in which isolated reconstruction of the PLC without reconstruction of the PCL was performed, did not achieve a good outcome, unlike isolated PCL grade 2 injuries, which did not have adverse effects on knee function in other studies.2,23,25,26 The combined injury of the PCL and PLC is caused by more severe trauma than an isolated PCL injury. Considering the effect of the trauma, the condition of the remaining posterior instability even after anatomic PLC reconstruction, which had no difference in posterolateral stability between the 2 groups, is not thought to be the same as the condition of the isolated PCL grade 2 injury. As a result, the difference in condition is considered to be a cause of group A having worse outcomes in comparison with group B and of group A not achieving a good outcome, unlike isolated PCL grade 2 injuries. Therefore, preoperative low-grade PCL injuries in combined injury cases should not be treated like isolated PCL injury cases, and reconstruction of both the PCL and PLC is needed. Lastly, when treating low-grade PCL injuries in combined injury cases, there is one aspect that should be taken into account. The difference in knee functional scores between the 2 groups showed a statistically significant distinction, but it was less than the minimal clinically important difference (MCID). The MCID of the IKDC subjective score was 11.5 in a previous study including a wide variety of knee conditions. 7 Because the difference in the mean SSD in posterior translation between the 2 groups was small, and the difference in the clinical scores was statistically significant but below the MCID, extra surgical time, additional cost, and potential morbidity, which can be associated with PCL reconstruction, should be considered.
This study has several limitations. First, the study was based on a retrospective review. This can be associated with a bias in measurements. To draw a more reliable result, a prospective study to investigate long-term follow-up outcomes is needed. Second, the assignment of patients was not randomized. Third, radiological evaluation by stress radiography and the dial test employed in this study to examine the degree of external rotation of the tibia had inherent limitations as to objectivity and accuracy. Although measurements were performed 2 times by different orthopaedic surgeons to lower subjectivity, the ICC was relatively low, especially in the dial test compared with values measured on stress radiography.
Conclusion
Isolated reconstruction of the PLC without reconstruction of the PCL had a similar result to simultaneous reconstruction of the PCL and PLC with regard to posterolateral stability. Yet, the simultaneous reconstruction group showed better knee functional scores than the isolated PCL reconstruction group, despite a relatively small improvement in posterior translation after PCL reconstruction. Simultaneous reconstruction of the PCL and PLC is a reliable treatment method in addressing PCL injuries with mild grade 2 or less posterior translation combined with posterolateral rotatory instability.
Footnotes
Acknowledgements
The authors thank Dong-Su Jang (medical illustrator, Medical Research Support Section, Yonsei University College of Medicine, Seoul, Korea) for his support with the medical figures.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.