
Abstract
Background:
Orthopaedic registries have shown value in tracking and surveillance of patients, implants, and outcomes associated with procedures. No current anterior cruciate ligament reconstruction registry (ACLRR) exists in the United States.
Purpose:
To describe the current cohort captured by an institutional ACLRR and describe the outcomes observed in the registered patients and how findings from the ACLRR are disseminated.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
The anterior cruciate ligament reconstructions (ACLRs) registered between February 2005 and September 2011 by 244 surgeons in 48 medical centers were evaluated. The ACLRR collected data intra- and postoperatively using paper forms and electronic medical records. The ACLRR cohort was longitudinally followed and outcomes were prospectively ascertained. Outcomes (ie, revisions, subsequent operations, venous thromboembolism, and surgical site infections) were adjudicated via chart review. Descriptive statistics are used to describe the cohort and Kaplan-Meier curves to evaluate survival.
Results:
During the study period, 16,192 ACLRs (15,101 primary and 1091 revisions) with a median follow-up of 1.6 years (interquartile range, 0.7-2.8 years) were registered. Male patients received 64% of both primary and revision ACLRs. The mean age at surgery was 29.5 years (SD, 11.4 years) for primary and revision reconstructions. Cartilage injuries were noted in 25.2% of primary and 37.5% of revision ACLRs, and meniscal injuries were identified in 60.8% and 53.2%, respectively. Autografts were used in 57.6% of primary ACLRs and 20.9% of revisions. Allografts were used in 42.4% of primaries and 78.8% of revisions. In primary ACLR, the most common femoral and tibial fixation types were interference screws (42.2% and 79.7%, respectively). Fixation type distribution was nearly identical in primaries and revisions. Of the primary ACLRs, 3.7% had subsequent operations on the same knee and 1.7% on the contralateral knee. Deep surgical site infection developed in 0.3% of primaries and 0.8% of revisions. Symptomatic deep vein thromboses were seen in 0.2% of both primaries and revisions. The overall revision rate was 1.7%. Lower rates of graft survival were identified in younger patients and those with allografts.
Conclusion:
Large, community-based ACLRRs are useful in informing participating surgeons of current treatment practices, prevalence of concurrent injuries, and outcomes associated with the procedures. Information from the ACLRR can be used to develop interactive patient and surgeon tools that can be used to optimize patient care.
Patient, device, and disease registries are valuable tools in many different medical disciplines, 4 including orthopaedics. Arthroplasty registries have demonstrated the value and importance of these tools. For example, the outcomes of arthroplasty surgery have improved in Scandinavia because of the early detection of poorly performing implants identified by the Scandinavian arthroplasty registries. 17 It is likely that similar benefits may be realized in other orthopaedic subspecialties. This was the impetus for the Kaiser Permanente Anterior Cruciate Ligament Reconstruction Registry (KPACLRR).
National knee ligament registries have been in existence in Norway, Sweden, and Denmark for a number of years.1,5,15 The goals of ligament registries, as delineated by Engebretsen and Forssblad, 3 are (1) to improve outcomes through improved feedback to surgeons and hospitals, (2) to identify factors related to good and poor outcomes, and (3) to identify procedure and devices that result in premature failure.
The purpose of this study is to describe the current cohort of registered patients captured by the KPACLRR. This study also highlights how this anterior cruciate ligament reconstruction (ACLR) registry monitors the safety of ACLR grafts and implants, identifies risk factors associated with complications and failures, and provides feedback to surgeons and hospitals on clinical outcomes associated with ACLR surgery.
Materials and Methods
Study Design, Data Collection Procedures, and Participants
A retrospective analysis of a prospectively followed cohort of ACLRs entered in the KPACLRR between February 1, 2005, and September 30, 2011, was conducted. The data collection process, coverage, and participation have been previously described. 20 In brief, surgeons collect intraoperative information during the registration procedure and send it to the registry data repository center using paper forms. In addition, the registry collects information from the electronic medical records using electronic algorithms and queries. This additional information includes demographic information, comorbidities, and events associated with the procedures (failures and complications). The registry covers a large integrated health care system with an estimated 9.2 million members in 8 geographical regions within the United States. The 2010 voluntary participation in the registry was 93%; this is the proportion of procedures performed at the covered institution that were registered during the year. 20 The KPACLRR has external and internal institutional websites used to disseminate registry findings. For an external audience, all publications, abstracts, and highlights from the registry are at http://kpimplantregistries.org/Registries/ACL.htm. Internally, all participating surgeons have access to regional and facility-specific participation reports, can access the revision risk calculator described in this study, can download annual reports from the registry, and can request a personalized annual report (surgeon-specific information) or make a quality or research data request.
During the study period, 7 regions participated in the registry (Northern California, Southern California, Hawaii, Pacific Northwest, Colorado, Mid-Atlantic, and Ohio). The current sample presented includes data from these 7 regions, with 48 medical centers and 244 participating surgeons. This study included all registered cases in the ACLR registry during the study period. This study is inclusive of primary and revision ACLRs, reconstructions with multiligament injuries, and ACLRs with other concurrent injuries such as cartilage and meniscal damage. Institutional review board approval was obtained prior to the beginning of the study.
Risk Factors, Confounders, and Covariates
The KPACLRR collects information on patient factors, concurrent injuries/procedures, graft/fixation, surgical technique, and surgeon and hospital factors that serve as the basis for identification of risk factors, confounders, and covariates in our analyses. Patient factors captured by the registry include age, sex, race, body mass index (BMI), physis status, sports played at the time of injury, time from injury to surgery, history of previous surgery on index knee, and whether the contralateral knee is normal. Concurrent injuries/procedures captured by the registry include type of menisci and cartilage injury and procedure performed (if any) and whether other knee ligaments were injured or repaired at the time of ACLR. “Other” diagnoses written by the surgeon are also recorded, and these can include patellar instability and/or dislocation, osteoarthritis, loose body, and other less common conditions that are present at the time of surgery. The type of graft used, either allograft, autograft, or hybrid, and the type of tissue are recorded. For allografts, the tissue type, company, and reference/lot number are also captured. Primary tibial and femoral fixation devices are captured as well as any supplemental fixation devices used. Surgical technique factors include whether this is a revision or primary procedure, femoral tunnel drilling method (ie, transtibial, medial portal, or lateral approach), whether single or double bundle procedures were performed, and whether this is a staged procedure. Surgeon factors captured by the registry include sports medicine fellowship training status and ACLR annual volume. Hospital annual volume is also captured.
Outcomes
The ACLR registry captures 6 major end points associated with ACLR. These outcomes are identified by surgeon and patient report as well as electronic screening algorithms, which are used to review the patients’ electronic medical records. After initial identification of the end points through surgeon report and electronic screening algorithms, patient charts are reviewed and outcomes are adjudicated by trained clinical content experts according to predetermined criteria. In addition, patients who leave the integrated health care system (19% lost to follow-up) and have not had an end point are contacted annually (both via mail and e-mail) for information on revisions and subsequent operations. (1) Short-term revision is the main end point of interest and is defined as a postoperative procedure to replace the graft after the index primary ACLR. (2) Reoperation is the second end point of interest and is defined as a subsequent operation for any reason in the same knee after the index primary ACLR. (3) Operation in the contralateral knee for any reasons, at any time after the index procedure (inclusive of ACLR), is the third outcome. (4) Surgical site infection (SSI), the fourth outcome of interest, as defined by the Centers for Disease Control and Prevention (CDC)/National Healthcare Safety Network criteria, 7 is identified by use of a validated SSI screening algorithm. 8 Deep SSI can be attributed to the procedure up to 1 year postoperatively (if device is present) and appears related to the procedure and involved deep soft tissues and at least one of the following: (a) There is purulent drainage from the incision; (b) the incision dehisces or is opened and is culture-positive or not cultured and the patient has fever, pain, or tenderness; (c) an abscess or other evidence of infection is found during examination, reoperation, or histopathologic or radiologic examination; (d) deep incisional SSI is diagnosed by a surgeon or attending physician. Superficial SSIs are only attributed to the procedure within the first 30 days postoperatively and involve only skin or subcutaneous skin and one of the following: (a) There is purulent drainage from the incision; (b) an organism is cultured from the incision site; (c) pain, tenderness, swelling, redness, and heat are present, and the surgeon opens a culture-negative incision; (d) superficial incisional SSI is diagnosed by a surgeon or an attending physician. Finally, (5) deep venous thrombosis (DVT) and (6) pulmonary embolism (PE) occurring within 90 days of the index procedure as identified by use of the Agency for Healthcare Research and Quality Patient Safety Indicator algorithm are the fifth and sixth outcomes of interest and are adjudicated by chart review. Clinical failures that have not been revised are not captured by the registry and not included in the analysis.
Statistical Analysis
Means, medians, standard deviations (SDs), interquartile ranges (IQRs), frequencies, and proportions are provided to describe the study cohort. Crude revision rates were calculated as the proportion of ACLRs (during the entire study period) that were revised divided by all procedures performed. The annualized rate of revision, or (incidence) revision density, is the percentage of patients who failed per year of follow-up. Crude subsequent operations and subsequent operation density were calculated in a manner similar to the revision estimates, with the number of operations used as the numerator. Kaplan Meier survival curves are used to describe the crude survival rates (with revision as the end point), and log-rank tests were used to compare survival distributions. Patients were censored before the end of the study period if they died or left the integrated health plan membership. The revision risk calculator was developed by use of binary logistic regression models. The ACLR registry is an SQL database that can be accessed via secured (password protected) connections with several programming tools. Most reports provided by the registry were created with Microsoft Access (Microsoft, Redmond, Washington). Analysis provided by the ACLR Registry was done with SAS 9.2 (SAS Institute, Cary, North Carolina).
Results
Current Cohort of Registered Patients
During the study period, 15,101 (93.3%) primary ACLRs were recorded in the registry. The average age of the cohort is 29.5 years (SD, 11.4 years), with the largest age category being 14 to 17 years (19.8%, n = 2998). A different distribution of males and females in different age groups is observed. See Table 1 for cohort characteristics. Most patients with primary ACLR present with some type of meniscal injury (60.8%, n = 9185), and 25.2% (n = 3802) have cartilage damage. Of the patients with primary reconstruction, few have multiligament injuries (2% with medial collateral ligament, 1% with posterior collateral ligament, and 0.4% with posterolateral rotatory instability), and 1% of patients have other diagnoses. Of primary revisions, 71% are performed by sports medicine fellowship–trained surgeons. Of the patients available for 1-year follow-up (surgeries performed between February 1, 2005, and September 30, 2010, n = 12,008) 90% follow-up was available; of the patients available for 2-year follow-up (February 1, 2005, to September 30, 2009, n = 8322) 81% follow-up was available; and of the patients available for 5-year follow-up (February 1, 2005, to September 30, 2006, n = 813), 63% had complete follow-up.
Kaiser Permanente Anterior Cruciate Ligament Reconstruction Registry Cohort, by Primary and Revision Procedure and Patient Sex, February 2005 to September 2011 a
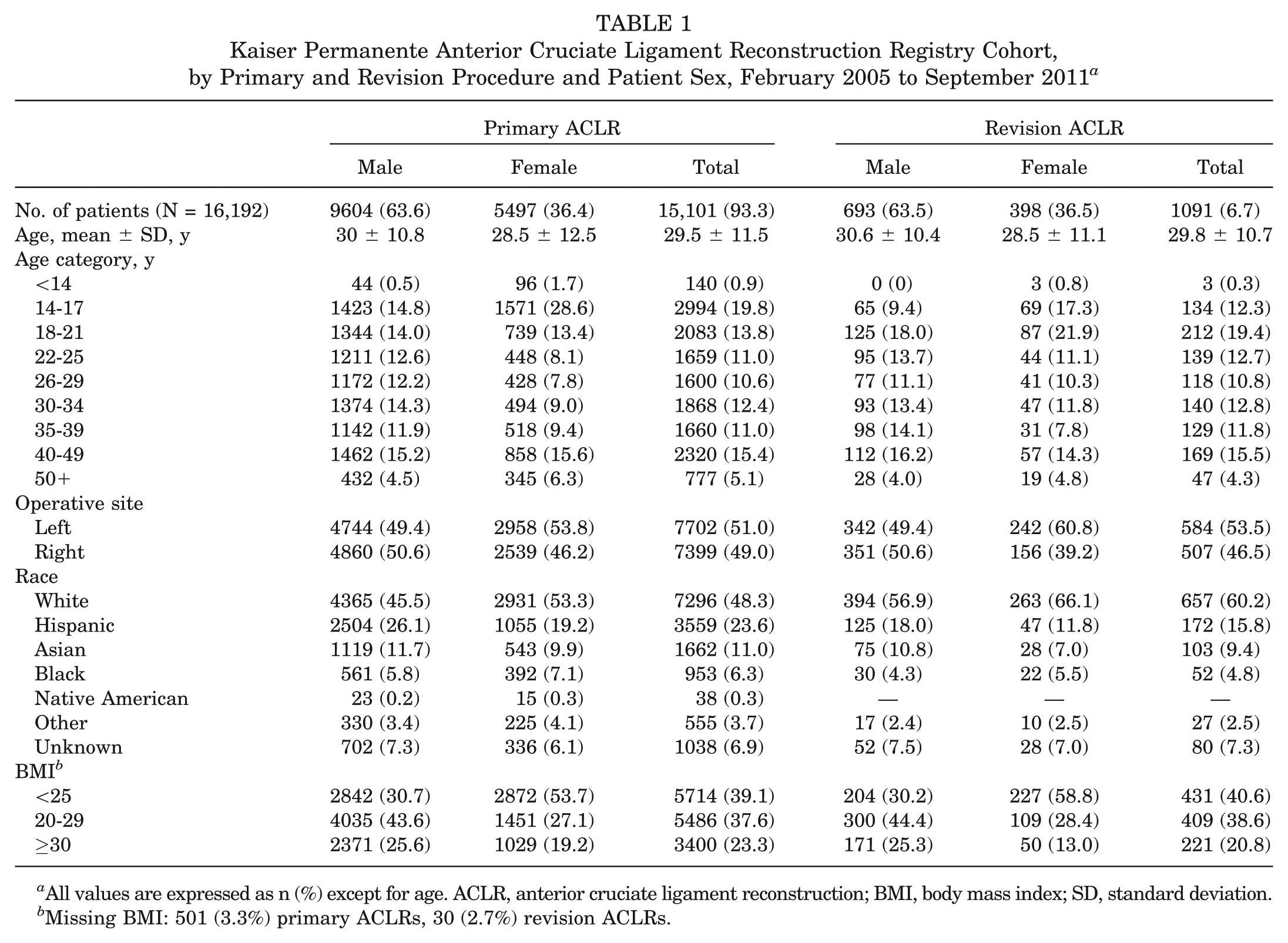
All values are expressed as n (%) except for age. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; SD, standard deviation.
Missing BMI: 501 (3.3%) primary ACLRs, 30 (2.7%) revision ACLRs.
An additional 1091 (6.7%) revision ACLRs (260 revisions of the primaries in the registry) were recorded. The average age of the cohort is 29.5 years (SD, 11.4 years), with the largest age category being 18 to 21 years old (19.4%, n = 212). In revision ACLRs, a lower prevalence of meniscal injuries (53.2%, n = 580) and a higher prevalence of cartilage injury (37.5%, n = 409) were observed compared with primary ACLRs. Sports medicine fellowship–trained physicians performed 73% of the revisions.
Monitoring of ACLR Grafts and Implants Safety
In primary ACLR, autografts are the most commonly used grafts (57.6%, n = 8693), with hamstring (53.7%, n = 4667) being the most common autograft and bone–patellar tendon–bone (BPTB) the second most common (44.7%, n = 3884). Allografts were used in 42.4% of the primary ACLRs (n = 6396). The most common allografts used in primaries were tibialis posterior (24.8%, n = 1588), tibialis anterior (21.5%, n = 1373), Achilles tendon (19.7%, n = 1258), and BPTB (19.1%, n = 1221) (Table 2). The most common femoral fixation was interference (42.2%), followed by suspensory fixation (25.7%) and cross-pin fixation (17.3%); 14.8% were not reported. Tibial fixation was most commonly performed with interference screws (79.7%) followed by suspensory (4.2%) and cross-pin (0.2%) techniques, and 15.8% were missing implant information. Hamstring tendon autografts were most commonly fixed with a suspensory primary femoral fixation in combination with an interference tibial fixation (35.3%, n = 1621) or interference fixation on both the femur and tibia (25.0%, n = 1147). BPTB autografts were most commonly fixed with interference screws in both the femur and tibia (72.9%, n = 2825). Finally, allografts were fixed with various techniques depending on the graft used, but for the overall group, femoral fixation was performed with interference fixation (33.9%, n = 2169), suspensory fixation (28.1%, n = 1795), and cross-pin fixation (25.3%, n = 1619). Interference screw tibial fixation was used for 81.6% of the allografts.
Graft Use for Primary and Revision Anterior Cruciate Ligament Reconstruction Procedures a
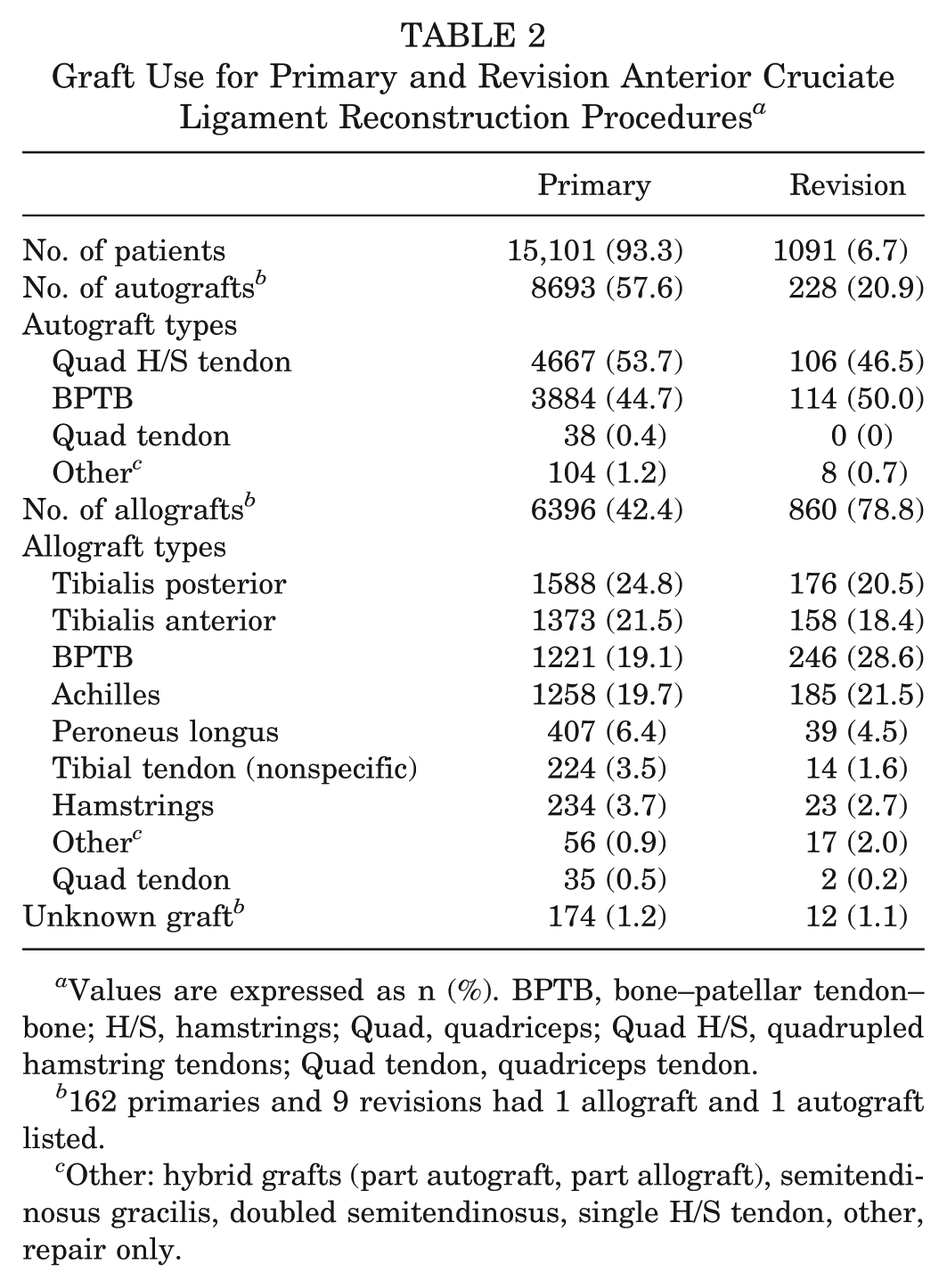
Values are expressed as n (%). BPTB, bone–patellar tendon–bone; H/S, hamstrings; Quad, quadriceps; Quad H/S, quadrupled hamstring tendons; Quad tendon, quadriceps tendon.
162 primaries and 9 revisions had 1 allograft and 1 autograft listed.
Other: hybrid grafts (part autograft, part allograft), semitendinosus gracilis, doubled semitendinosus, single H/S tendon, other, repair only.
Allografts were used in 78.8% (n = 860) of the revisions. The most common allografts used in revisions were BPTB (28.6%, n = 246), Achilles tendon (21.5%, n = 185), tibialis posterior (20.5%, n = 176), and tibialis anterior (18.4%, n = 158) (Table 2). The most common femoral fixation in revisions was interference (44.3%) screws, followed by suspensory (25.5%), cross-pin fixation (14.6%), and 15.7% were not reported. Tibial fixation was most commonly performed with interference (78.9%) followed by suspensory (4.2%), and cross-pin (<0.1%), and 16.8% of revisions were missing implant information.
Risk Factors Associated With Complications and Failures
In the described cohort, the crude revision rate in the primary ACL cohort, at median follow-up time of 1.6 years (IQR 0.7-2.8 years), is 1.7% (n = 260) (Table 3). The annualized rate of revision after primary ACLR for this cohort was 0.9% per knee per year. Subsequent operations other than for revision occurred in 5.5% (n = 824) of the primary ACLRs (3.7%, n = 560 on the same knee and 1.7%, n = 264 on the other knee). The annualized rate of subsequent operation after primary ACLR for the entire cohort was 2.9% per knee per year. See Table 4 for reasons for subsequent reoperations in primary ACLR. There were 64 SSIs (0.4%, 44 deep SSI and 20 superficial SSI) on the primary procedures and 11 (1.0%, 9 deep SSI and 2 superficial SSI) on the revision procedures. There were 26 (0.2%) symptomatic DVTs and 15 PEs (<0.1%) in the primary procedures. In revision ACLR, 0.2% (n = 2) had a DVT and no PEs were observed.
Postoperative Outcomes of Anterior Cruciate Ligament Reconstructions by Primary and Revision Procedures and Patient Sex a
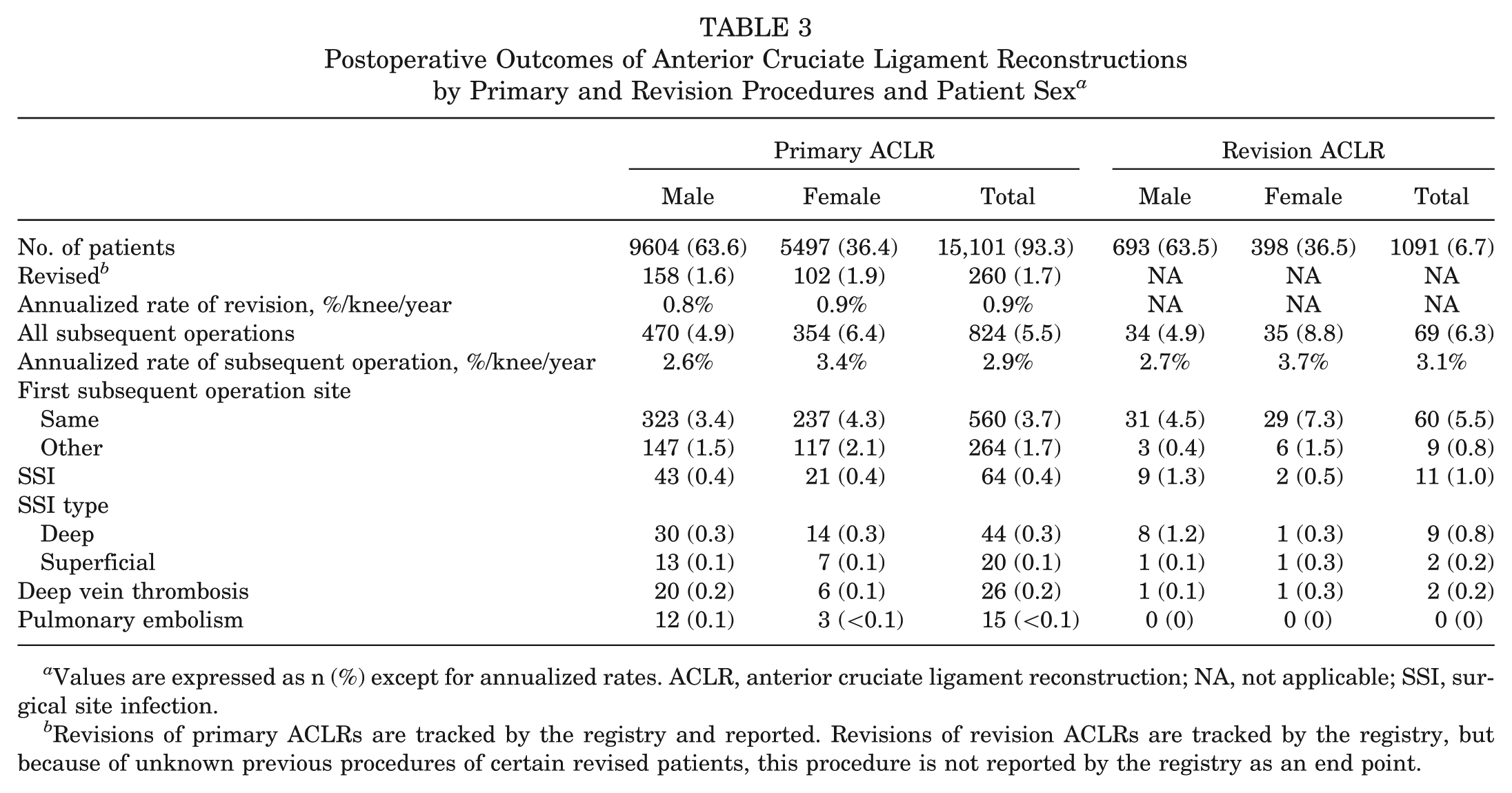
Values are expressed as n (%) except for annualized rates. ACLR, anterior cruciate ligament reconstruction; NA, not applicable; SSI, surgical site infection.
Revisions of primary ACLRs are tracked by the registry and reported. Revisions of revision ACLRs are tracked by the registry, but because of unknown previous procedures of certain revised patients, this procedure is not reported by the registry as an end point.
Primary Reasons for Subsequent ACLR Operations a
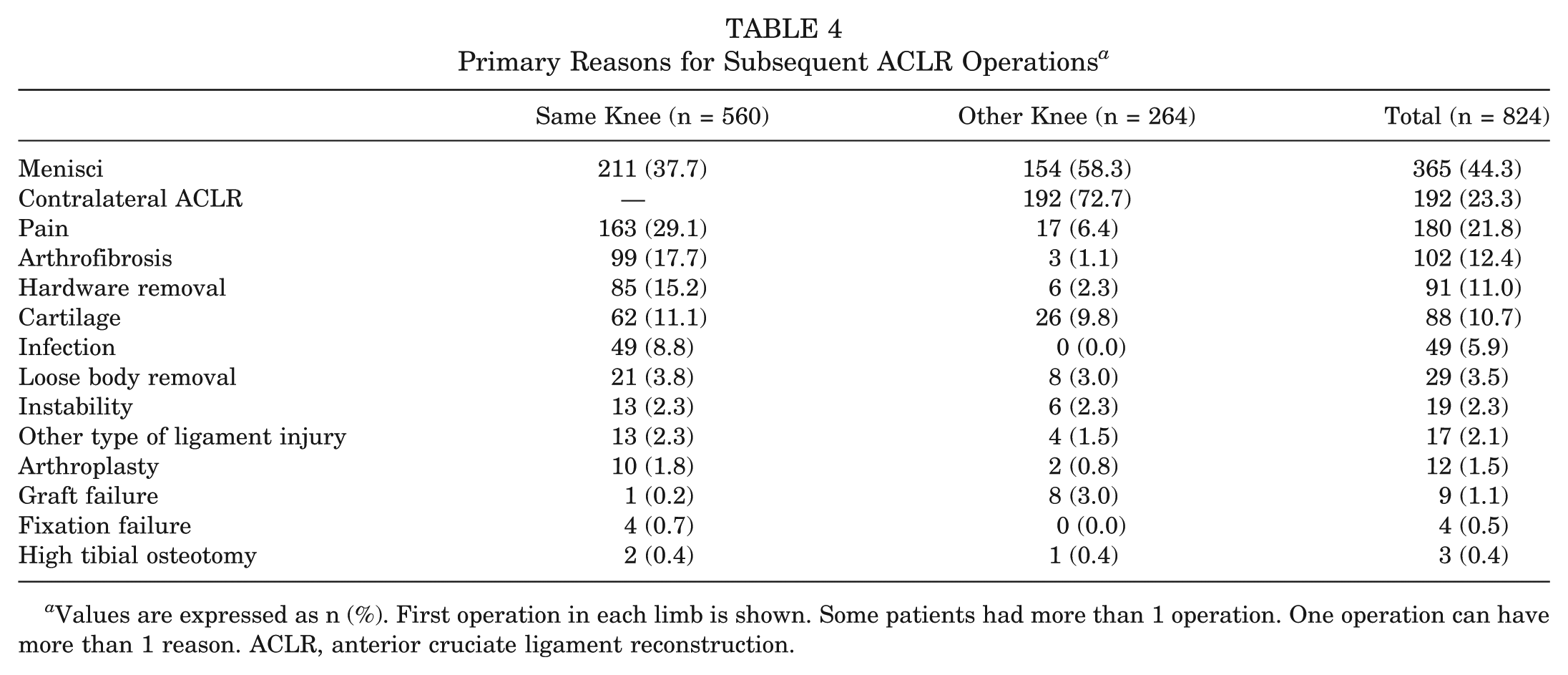
Values are expressed as n (%). First operation in each limb is shown. Some patients had more than 1 operation. One operation can have more than 1 reason. ACLR, anterior cruciate ligament reconstruction.
Providing Feedback to Surgeons and Hospital
Annual reports of the ACLR registry provide survival estimates by all major risk factors and covariates collected by the registry. See Figure 1 for survival curves by graft type and by age and sex. The survival at 3.2 years is not different by sex but it is by age. Patients younger than 17 years have the lowest survival rate (91.5%; 95% confidence interval [CI], 88.3%-93.4% in males; and 93.3%; 95% CI, 90.8%-95.1% in females), followed by patients 18 to 25 years old (95.1%; 95% CI, 93.6%-96.2% in males; and 96.1%; 95% CI, 94.2%-97.4% in females). Patients older than 25 have the highest survival rate in our cohort (98.4%; 95% CI, 97.8%-98.8% in males; and 98.4%; 95% CI, 97.5%-99.0% in females). At 3 years, the survival by graft is significantly different by graft type, with the lowest survival in allografts (96.2%; 95% CI, 95.3%-96.8%), followed by hamstring tendon autograft (97.2%; 95% CI, 96.4%-97.8%) and BPTB (97.6%; 95% CI, 96.8%-98.3%). Risk factors associated with graft revision currently identified by the ACLR registry include age, race, and graft type. 18 A revision risk calculator tool has been developed based on the risk factors for revision that have been identified by the registry. This tool is available for registry-participating surgeons to use at the patient preoperative visit. This prognostic risk calculator can calculate the probability of failure of a primary ACLR procedure within 1 year based on patient characteristics (age, sex, race, and BMI) and graft choice (allograft, BPTB autograft, hamstring autograft). See Figure 2 for a screenshot of the risk calculator and Figure 3 for a graphical display of specific patient scenarios and probability of failure.
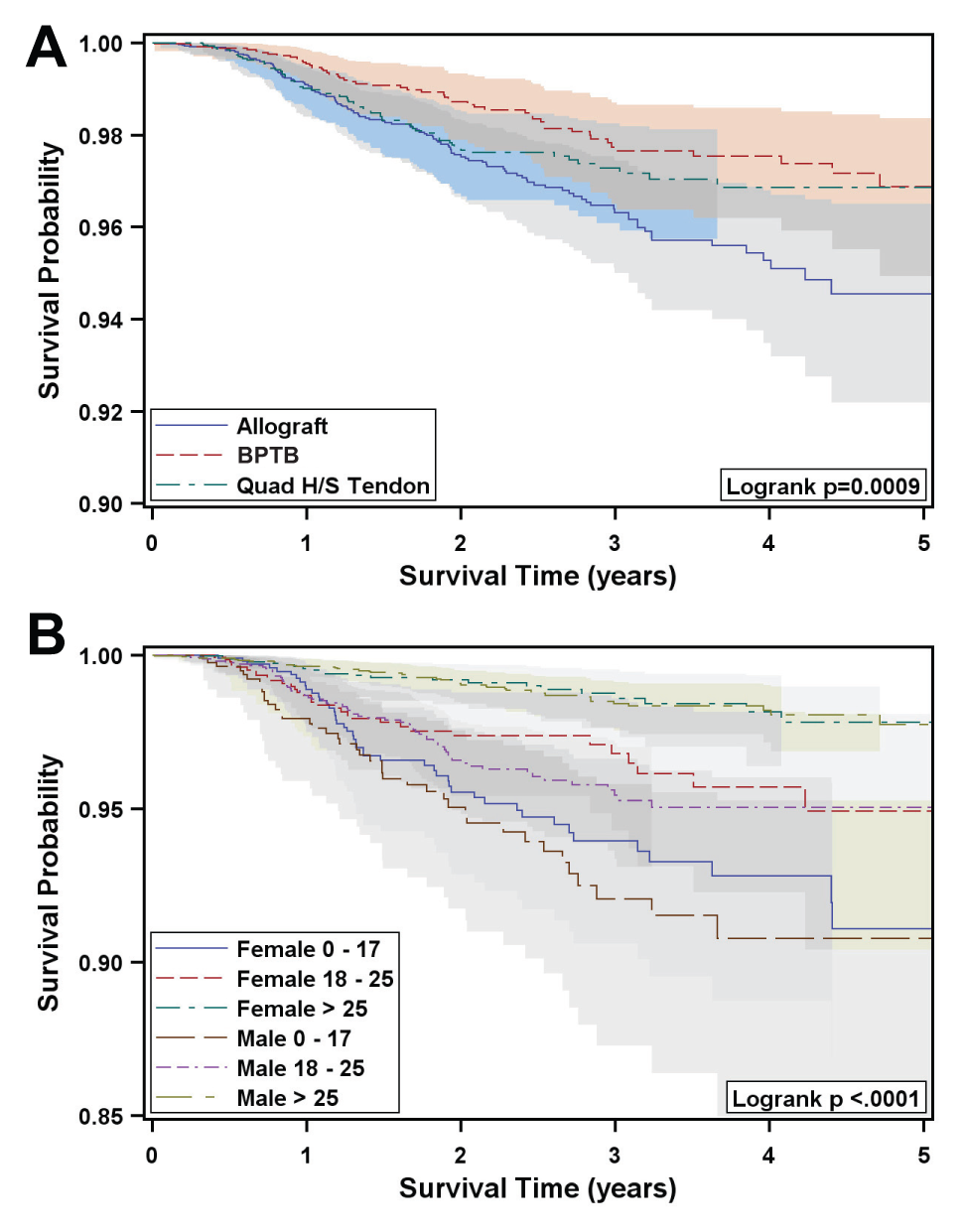
Kaplan-Meier survival estimates and 95% confidence bands of primary anterior cruciate ligament reconstruction procedures by (A) graft type and (B) sex and age groups. The allografts plotted in (A) are inclusive of all allografts registered. The equal-precision approach was used to create the 95% confidence bands. BPTB, bone–patellar tendon–bone; H/S, hamstrings; Quad, quadriceps; Quad H/S Tendon, quadrupled hamstring tendons.
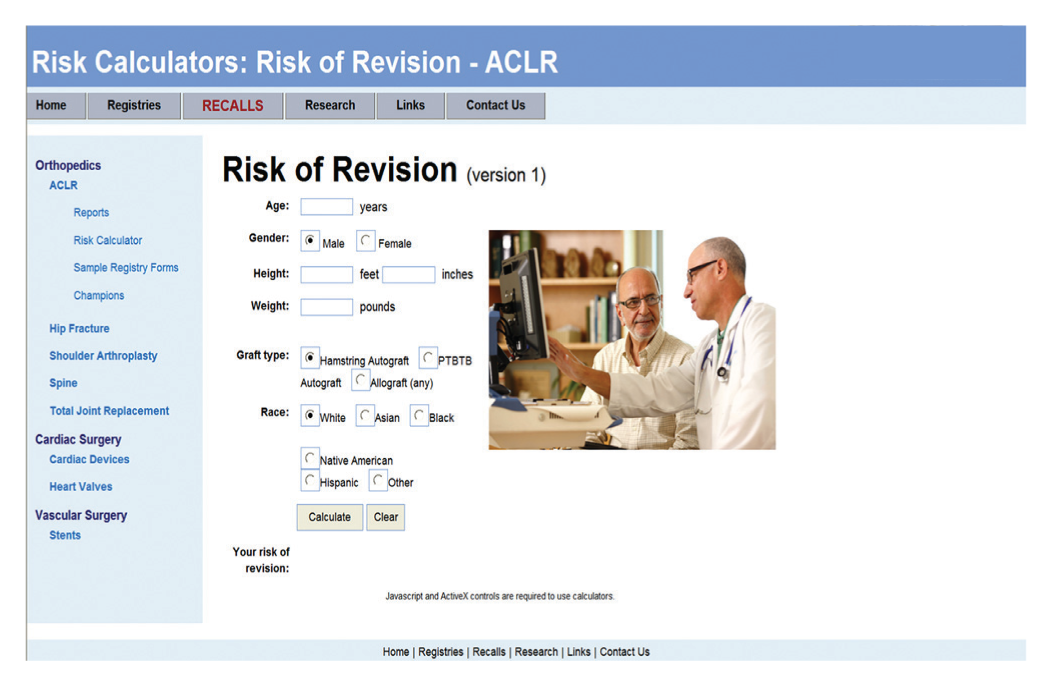
Screenshot of the Kaiser Permanente Anterior Cruciate Ligament Reconstruction Registry Revision Risk Calculator. ACLR, anterior cruciate ligament reconstruction.
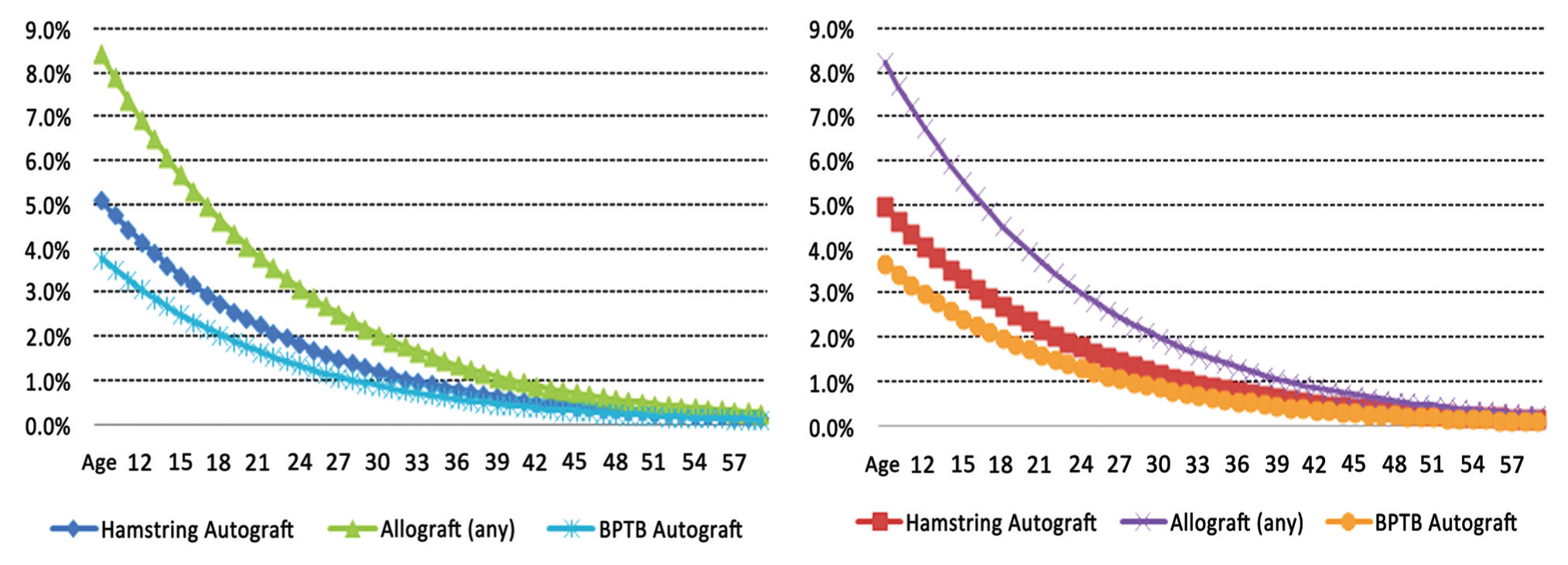
Probability of aseptic revision within 1 year postoperatively determined by use of the risk calculator model. For males (left), body mass index = 23, by age by graft; for females (right), body mass index = 23, by age by graft. BPTB, bone–patellar tendon–bone.
Discussion
This study described the cohort of 16,192 patients currently registered in the largest US ACLR registry. We also summarized SSI and thromboembolic events as well as short-term revision and subsequent operations associated with ACLRs and highlighted some of the ways this information has been used within our institution. The annualized rate of revision in this group is 0.9% per year, and the annualized rate of subsequent operation is 2.9% per year per knee. We have identified both age and graft type as risk factors that affect graft survival and have developed tools to inform surgeons using the registry of this information. In this particular study, patients younger than 17 years and patients undergoing allografts had lower rates of graft survival.
The utility of patient and device registries is being expanded successfully to ACLR surgery. Information derived from registries can be valuable because of the generalizability of the results. Registries represent large patient populations, making the results more applicable to the general population. Studies with limited cohorts may only be applicable to patients who have the same characteristics as those of the study and have surgical interventions performed in the same manner as that particular study. Before inferences can be made from registry studies, it is important to understand whether the sample is representative of the population of interest. The largest and most well-published ligament registries in the world are from Scandinavia, and their cohorts have both similarities to and differences from our cohort. In the KPACLRR, the mean age at primary ACLR was 29.5 years and 64% were male. This is a slightly larger proportion of males compared with the Scandinavian registries (Danish 60%, Swedish 57.5%, and Norwegian 55.8%) but is a similar age profile.1,6,15 Meniscal injuries were fairly common in our cohort and were identified in 60.8% of primary procedures and 53.2% of revisions, rates that are higher than the 48.5% and 35.5%, respectively, reported by the Norwegian registry. 6 Chondral injuries were identified in 25.2% of primary ACLRs, a rate identical to the prevalence reported by the Norwegian registry. 6 Slightly higher rates of chondral injury were reported in the Swedish and Danish registries (28% and 31%, respectively).1,16 We noted an increase in the prevalence of chondral injury to 37.5% at revision surgery. This may be a result of new articular cartilage damage due to a new traumatic giving-way episode or the normal progression of articular cartilage damage with time after initial ACL injury.
The main end point of the registry, graft failure rate, seems to be similar among most of the registries’ cohorts. At a short-term follow-up time of 1.6 years, our reported revision rate is 1.7%, with an annualized revision rate of 0.9% per year (or estimated 4.5% at 5 years). Both the Swedish and Danish registries have reported 5-year estimated revision rates of 4.1%.1,15 Other registries have not reported on subsequent operations other than ACLR (revision or other knee operations), but in our cohort subsequent operations (eg, for meniscal procedures, cartilage procedures, hardware removal, arthrofibrosis) have occurred in 5.5% of the patients, with an annualized rate of subsequent operations of 2.9% per knee per year. The Multicenter Orthopedic Outcome Network (MOON) cohort study, with longer follow-up, has reported a fairly high rate of subsequent operations (19% at 6 years, which is comparable with our estimated 17.4% for the same period). 22 Similarly, surgical site infections are not reported by other registries. But published clinical and observational studies report rates between 0.14% and 5.7%,2,9,13,21and our rates fall within the lower estimations of that range (0.4% in primary procedures and 1.0% in revisions). Finally, the incidence of DVTs (0.2% of both primary and revision ACLRs) was very low in our cohort and again similar to reported incidents of arthroscopic procedures in the literature.10,19
As initial registry reports are published, several surgery and patient factors are being identified (or simply confirmed from previous cohort and clinical studies) as risk factors for ACLR failure. Graft choice was identified as a risk factor for early revision surgery in a recent study. 18 That study, in which a multivariable analysis was performed (adjusting for age, sex, graft, BMI, and race) as opposed to the univariate survival curves presented here, showed that allografts had a 3 times higher risk of revision compared with BPTB autografts. This is similar to the report from the MOON group. 11 In the KPACLRR, 42.4% of primary ACLRs were performed with allografts, 31.5% with hamstring autograft, and 25.7% with BPTB autograft. This is dramatically different than the Scandinavian registries, which show that hamstring autograft is the graft of choice (Swedish 82%, Danish 71%, Norwegian 68%), and allografts are rarely used.1,6,16 The information regarding poorer short-term outcomes with allografts was disseminated to surgeons via the registry’s internal website, presentations at internal conferences, implementation of the revision risk calculator, and an external publication. 18 However, allografts continue to be highly prevalent in the primary cohort and are used in 78.8% of revision cases. Since the study findings were recently disseminated, we have not yet been able to measure the impact of this finding in the graft use pattern of our cohort, but we expect to see differences within the next few years. We anticipate a decrease in the use of allografts in primary ACLRs but expect that the use in revisions will stay somewhat constant since often one of the autograft choices has already been used for the primary surgery. Age is another risk factor that we have found to be associated with increased risk of revision, which has been similarly reported by the Danish registry and the MOON group.5,22
There are specific limitations with using registry data. For a registry to be successful there must be high participation, but this limits the amount of data that can be collected. Because of this limitation, we are unable to report on patient-reported outcomes, functional testing, or radiographic findings. Variables including return to sport and level of sport are also not available. Revision surgery is the primary outcome of the registry. Clinical failures that do not result in revision surgery are not captured in the registry. There is value in using revision as the outcome since it is a hard end point, and for a revision to occur, both patient and surgeon have agreed that there is a failure. When subjective outcomes such as KOOS or objective measures such as KT-1000 arthrometer or pivot shift are used, consensus from both the patient perspective and the surgeon perspective has not been reached on the definition of a failure. Attrition is also a limitation of a registry, especially one with a young patient population like ours. A total of 19% of the originally registered cohort has been lost to follow-up. We attempt to minimize this lost to follow-up yearly by contacting patients who have left the health plan to determine whether they have undergone subsequent surgery.
The strengths of this study are the size of the cohort, the community-based and racially diverse sample, the large number of contributing surgeons and hospitals, and the prospective standardized method of data collection. The large number of patients in this cohort provides the ability to evaluate not only multiple infrequent events (eg, revision, thromboembolic events, surgical site infections) in this group of patients but also multiple risk factors associated with these events. The diversity of the patient sample captured by our registry allows us to generalize our findings to many different subgroups and communities, and it is representative of the geographic population it covers.12,14 Additionally, the variety of surgeon skills, as well as surgeon and hospital volumes, makes our findings more applicable to a larger group of practices. Most published ACLR literature is from high-volume centers and surgeons, treating higher level athletes, characteristics that are not necessarily representative of the larger orthopaedic community. Given the wide range of surgeons and hospitals in our sample, our results provide a better indication of how these procedures are performed in a more general setting (affecting a large number of patients).
Conclusion
The KPACLRR has provided the participating surgeons with valuable information concerning their cohort of patients, such as the annualized rate of revision surgery in their patients (0.9% per knee per year) and the annualized rate of subsequent operation (2.9% per knee per year). It has also provided information regarding risk factors of revision ACLR surgery, such as use of allografts and younger age. An ACLR registry is a highly valuable tool that provides unique opportunities to understand the population undergoing ACLR in the United States and the current practices of the orthopaedic community performing these procedures, and it allows for procedure outcome evaluation. A successful registry is also engaged in continuous feedback with its participant surgeons and other stakeholders.
Footnotes
Acknowledgements
We acknowledge all the Kaiser Permanente orthopaedic surgeons who contribute to the ACLR registry and the Surgical Outcomes and Analysis Department, which coordinates registry operations. We also acknowledge Tom S. Huon, BS, and Ursula C. Cardenas, for their ongoing support with the ACLR registry database and quality control management, and Alan L. Schepps, MS, for his contribution preparing the figures for this article.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.