
Abstract
Background:
In posterolateral corner (PLC) injuries in which the lateral collateral ligament (LCL) is intact, there is controversy about whether reconstructing the popliteus tendon (POP), the popliteofibular ligament (PFL), or both structures (POP + PFL) is required to restore normal external tibial rotation.
Hypothesis:
Three reconstruction techniques, POP, PFL, and POP + PFL, are able to restore external tibial rotation to normal.
Study Design:
Controlled laboratory study.
Methods:
Six nonpaired human knees were tested under the following states: POP and PFL intact and sectioned. The 3 different surgical techniques were used to reconstruct the sectioned structures, and the knees were retested. Each knee was subjected to a 5-N·m external rotation torque and tested at 0°, 30°, 45°, 60°, 90°, and 120° of flexion. A navigation system was used to measure motion changes of the tibia with respect to the femur.
Results:
There were small but significant increases in external rotation after sectioning both the POP and PFL. Sectioning of either one of these structures alone produced smaller increases that were not significant. After comparing all of the tested reconstructed states to the intact state, there were significant differences at knee flexion angles from 30° to 90°. The PFL procedure restored external tibial rotation without significant differences compared with the intact knee at 30° to 90° of flexion. The POP and POP + PFL techniques significantly overconstrained external tibial rotation at all tested angles.
Conclusion:
In an LCL-intact PLC injury model, the POP and PFL function as a unit in resisting external rotation. All surgical procedures described and tested were able to reduce the increased external rotational laxity found in the sectioned state. The PFL reconstruction technique was able to restore external rotation to near normal. However, the techniques involving POP reconstruction overconstrained external rotation during laxity testing.
Despite our improved understanding of the anatomy and biomechanical function of the 3 key structures of the posterolateral corner (PLC) of the knee, the optimal treatment of PLC injuries remains controversial.1,3 In PLC injuries in which the lateral collateral ligament (LCL) is intact, there is controversy about which technique is superior: anatomic reconstruction of the popliteofibular ligament (PFL), the popliteus tendon (POP), or both the POP + PFL.
Pasque et al 6 suggested that operative reconstruction of PLC injuries should address all 3 key posterolateral structures (LCL, POP, and PFL) to restore the entire functional unit and prevent isolated restoration of a single structure that is likely to fail or result in residual posterolateral laxity. However, LaPrade et al, 3 in a cadaveric study, concluded that the POP is an important primary restraint to external tibial rotation and that isolated POP reconstruction was appropriate in the setting of PLC injuries where varus rotation is minimally affected. Fanelli and Larson 1 advocated a method in which only the PFL was addressed and reported adequate isometry with satisfying clinical results. The clinical results of this technique have been reported by other authors, which show that it is able to restore posterolateral stability but is less invasive than techniques that restore both the POP and PFL.9,10
There are numerous studies that have investigated the biomechanics of the PLC by sequential sectioning of posterolateral structures in cadaveric specimens. However, most of these studies used an injury model involving sectioning of the LCL and sectioning of the LCL, POP, and PFL together. Only a few studies have investigated the ability of POP and/or PFL reconstructions to restore external tibial rotation in the setting of a PLC injury with an intact LCL. LaPrade et al 3 conducted a cadaveric study and analyzed the static function of the POP and biomechanically validated the effectiveness of an isolated POP reconstruction technique. However, this study did not evaluate the role of the PFL in restoring external tibial rotation. Nau et al 5 used an LCL-intact model and compared the surgical technique of POP reconstruction with the POP + PFL technique. However, this study did not include isolated reconstruction of the PFL. Shahane et al 8 designed an experimental study and proved that in posterolateral disruption in which the LCL is intact, reconstruction of the PFL restored posterolateral stability of the knee. The study did not mention POP reconstruction.
To our knowledge, there have been no published biomechanical studies comparing the ability of POP reconstruction, PFL reconstruction, or combined POP + PFL reconstruction to restore external tibial rotation in the setting of an intact LCL. The purposes of our study were to (1) biomechanically analyze the static function of the POP and PFL and (2) compare 3 different surgical reconstruction techniques (POP, PFL, and POP + PFL) by use of an external rotation instability model (Figure 1). It was hypothesized that all these reconstruction techniques would be able to restore external tibial rotation to that of the intact knee in time zero laxity testing.
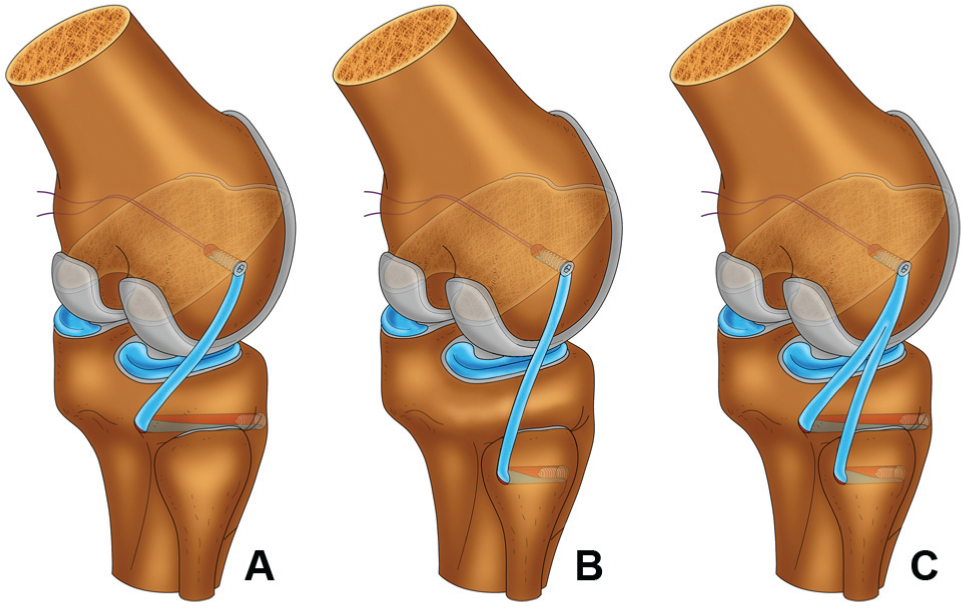
The 3 reconstruction techniques used in the study: (A) the popliteus tendon (POP) reconstruction, (B) the popliteofibular ligament (PFL) reconstruction, and (C) the POP + PFL reconstruction technique.
Materials and Methods
Specimen Preparation
This study used 6 nonpaired fresh-frozen human cadaveric knees. Approval of the study was obtained through the institutional review board at Beijing Jishuitan Hospital. The mean age of the specimens was 39.3 ± 10.0 years (range, 25-52 years). All specimens indicated no evidence of injury or instability by physical examination. The specimens were stored at −20°C and thawed overnight before testing. The hip was disarticulated, and the foot was kept intact to simulate a dial test. The skin and subcutaneous fat were removed from the knees, leaving the superficial fascia intact. The tendon of the tibialis anterior was harvested from each specimen to serve as an autograft for the procedure. The muscle and fascia were kept in situ. The posterolateral knee was exposed to the superficial crural fascia layer, and all individual posterolateral structures were left intact.
The specimens were placed on a custom-made testing apparatus in which the femoral head was rigidly held and was allowed free movement for calibration of the navigation. Two 4.5-mm Schanz screws were inserted into the anteromedial aspect of the tibia for anchoring the tibial trackers of the navigation system (Figure 2). Another 2 parallel 4.5-mm Schanz screws were inserted into the anterolateral aspect of the femur for anchoring the femoral trackers of the navigation system. A 5-N·m torque was applied to the tibia for application of external rotation torque during the test.
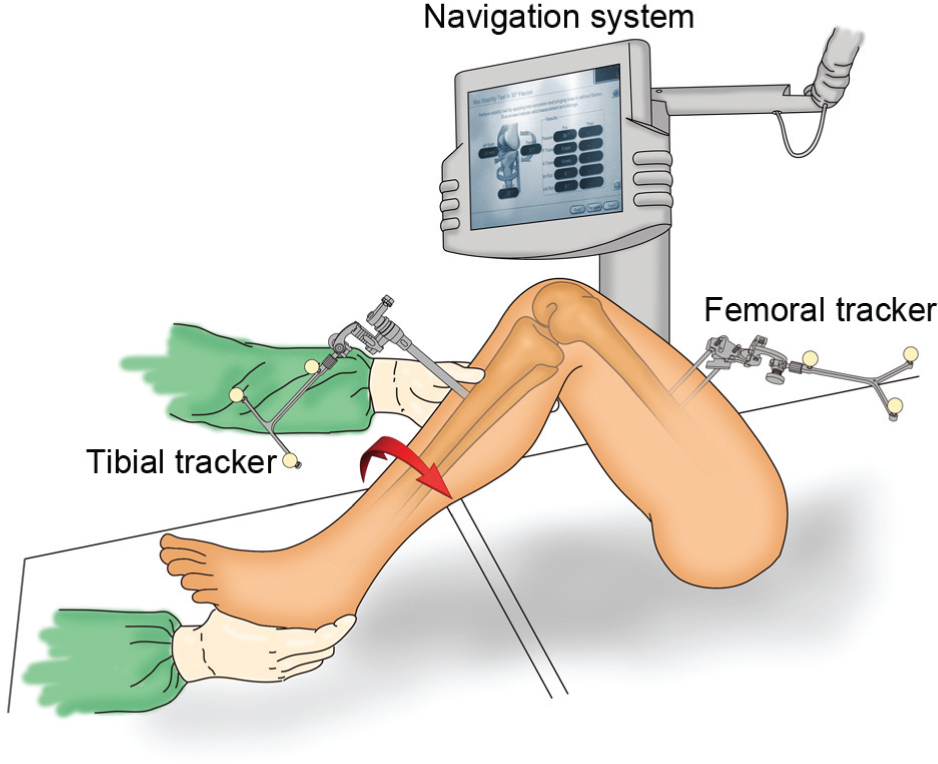
Biomechanical test of a left knee with the navigation system. Two trackers were fixed to the femur and tibia, which were tracked by the navigation system. The real-time changes of flexion and external rotation angle of the knee were calculated by the computer. A 5-N·m torque was applied to the tibia for application of external rotation torque during the test.
Part 1: Selective Cutting Tests
The measurements of external tibial rotation were first performed on the intact knee and then repeated to document the laxity of the sectioned knee. The specimens were divided into 2 groups. In group 1, the POP was cut first, and then the PFL was cut. In group 2, the PFL was cut first, and then the POP was cut.
Surgical exposure to the posterolateral aspect of the knee was previously described by LaPrade et al. 3 The musculotendinous junction of the popliteus as well as the fibular attachment of the PFL were visually identified (Figure 3A). The POP was initially cut at the popliteus musculotendinous junction (Figure 3B), distal to the PFL, to ensure the integrity of the PFL function. The PFL was cut at its fibular insertion (Figure 3A).
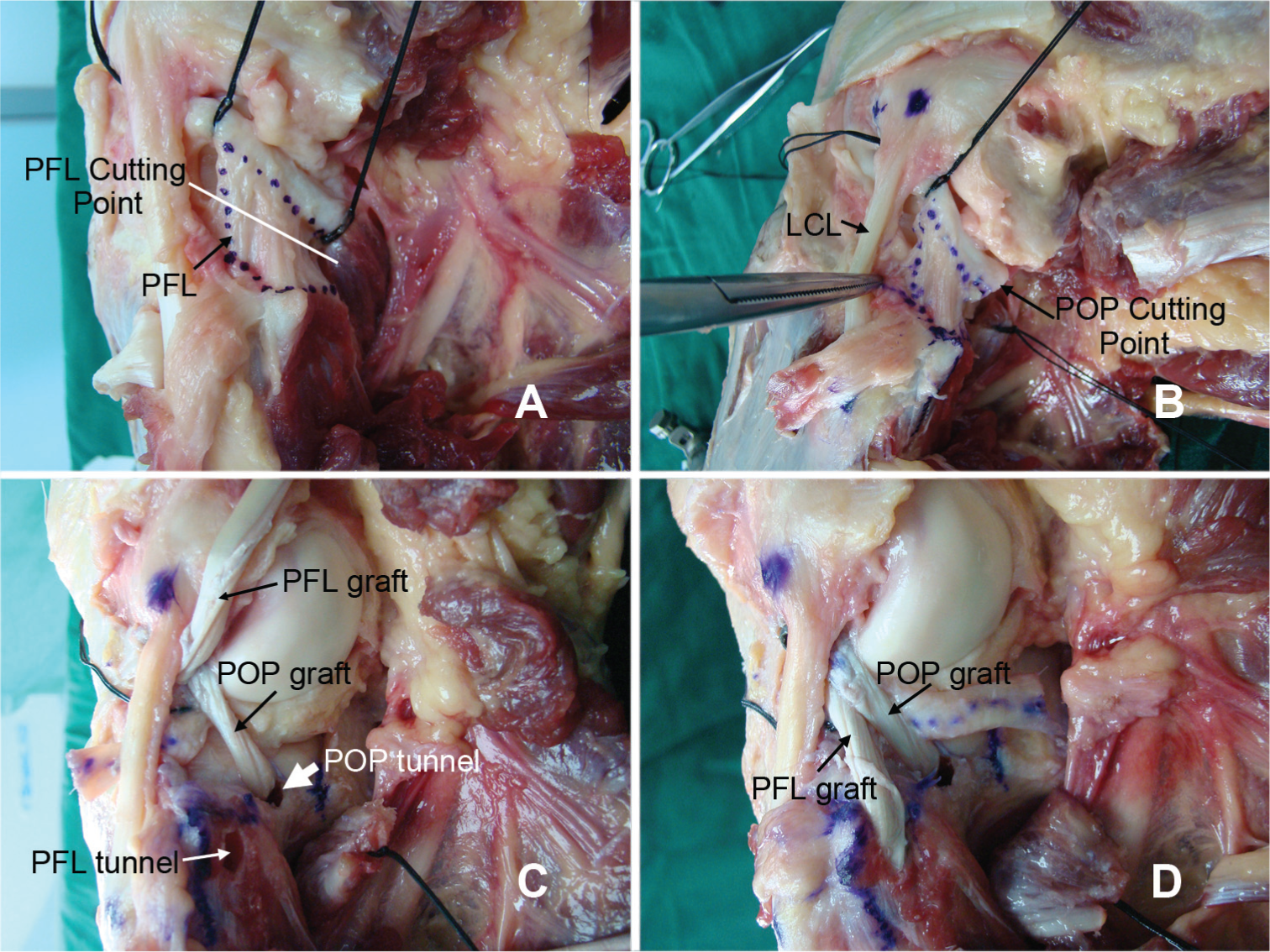
The selective cutting and reconstruction techniques. (A) The anatomy of the popliteofibular ligament (PFL). The white line indicates the cutting point, which was close to the PFL’s fibular insertion. (B) The cutting point of the popliteus tendon (POP), which was at the popliteus musculotendinous junction distal to the PFL (dotted area), to ensure the integrity of the PFL function. The lateral collateral ligament (LCL) was kept intact during the test. (C) The tibial tunnel for the POP reconstruction (thick white arrow) and fibular tunnel for the PFL reconstruction (thin white arrow). The POP graft was introduced into the tibial tunnel, and the PFL graft was loosened to simulate the POP reconstruction. (D) The POP + PFL reconstruction technique in which 2 grafts were introduced into the tibial and fibular tunnels and fixed individually.
Part 2: PLC Reconstruction Techniques
The musculotendinous junction of the POP and the fibular attachment site of the PFL were identified. Bone tunnels were drilled at the anatomic musculotendinous junction of the POP and the fibular attachment site for the PFL. These tunnels were drilled using a posterior cruciate ligament (PCL) femoral aimer (Arthrex Inc, Naples, Florida). A 2.4-mm guide pin was drilled from the anterolateral aspect of the fibular head, exiting at the PFL attachment site on the posteromedial aspect of the fibular head. A 7-mm tunnel was reamed over this guide pin (Figure 3C). A second 2.4-mm guide pin was drilled from a point distal and medial to the Gerdy tubercle, exiting at the posterior tibial popliteus sulcus at the level of the popliteus musculotendinous junction (approximately 10 mm distal to the margin of the articular cartilage). A 7-mm reamer was used to prepare the tibial tunnel by reaming over the guide pin with a large curette, protecting the neurovascular bundle posteriorly as the reamer was drilled (Figure 3C).
For the femoral side, an eyelet-tipped guide pin was drilled into the center of the POP attachment site, aiming in an anteromedial direction through the distal femur. A 9-mm femoral tunnel was then reamed over the guide pin to a depth of 30 mm.
The tibialis anterior tendon grafts were then prepared by tubularization using a No. 2 Ethibond Excel polyester suture (Ethicon, Somerville, New Jersey) and sized to pass through a 7-mm tunnel. The tibialis anterior tendon graft was then looped on itself, thus doubling the graft and in the process creating 2 distal arms. The shorter arm was approximately 7 cm in length for the PFL reconstruction, and the longer arm was approximately 10 cm in length for the POP reconstruction. The diameter of the looped end of the graft was 9 mm. The looped end of the graft was tubularized for 2.5 cm using a No. 2 suture. The tubularized end of the tibialis anterior tendon graft was pulled into the previously prepared tunnel at the POP femoral attachment site and neutral tibial rotation and fixed with a 7 × 25–mm bioabsorbable interference screw (ConMed Linvatec Inc, Largo, Florida).
The longer arm of the tibialis anterior tendon graft was passed through the tibial tunnel from posterior to anterior, thus reconstructing the POP. The shorter arm was passed through the fibular tunnel in a medial-to-lateral direction, thus reconstructing the PFL (Figure 3C and 3D). In accordance with the order of reconstruction technique tested, the POP graft and/or PFL graft were tensioned at 30° of flexion and the foot in neutral position and then fixed with a 7 × 25–mm cannulated bioabsorbable interference screw (ConMed Linvatec Inc).
Testing Protocol and Measurements
An intraoperative navigation system (Brainlab, Feldkirchen, Germany) was used for measurement of the testing parameters. The Brainlab Anterior Cruciate Ligament (ACL) Reconstruction System, version 2.0, was used to measure the degree of external rotation and the angle of knee flexion in each specimen. 2
After each sectioning and reconstruction, biomechanical testing was performed using the same testing protocol. By a Schanz screw that inserted into the anterior aspect of the tibia, just 10 cm proximal to the ankle joint, the torque wrench was attached to the screw, and external rotation torque was applied to the tibia. The tibial external rotation laxity was measured with a 5-N·m external rotation torque applied to the tibia at 0°, 30°, 45°, 60°, 90°, and 120° of flexion, respectively. The knee range of motion was guided by the navigation system, which was measured according to the guide pins and trackers inserted.
Pilot Study
A pilot study was performed on 2 knees to establish the study design and determine the initial setup, navigation system, testing procedures, cutting order of the PLC of the knee, and specific forces and torques used in the study. Pilot testing was performed at 0°, 30°, 45°, 60°, 90°, and 120° of knee flexion with applied loads of 5-N·m external torques. Increased external tibial rotation occurred after sectioning of the POP and PFL.
Data Analysis
For part 1 of this study, statistical analysis of variance (ANOVA) using a split–split plot model was performed. The whole plot was the cutting sequence. The first split-plot factor was the cutting sequence/anatomic structure cut (POP, PFL). The second split-plot factor was the flexion angle (6 levels, from 0° to 120°). Specimens were modeled as random factors, and interactions with other factors were included in the model. Note that the amount of tibial rotation at 0° was negligible, and therefore, data were not obtained at this position. Maximum increases in movement limits were reported at the flexion angle of occurrence without further statistical analysis. All reported probabilities for the post hoc comparisons were made after application of the Bonferroni correction for multiple comparisons. A type I error of .05 was maintained for all comparisons with the same applied load and cutting state.
For part 2 of the study, statistical analysis using standard ANOVA was performed to compare angulation analysis data between the intact condition, POP reconstruction, PFL reconstruction, and POP + PFL reconstruction. Comparisons were made for knee specimens at each knee flexion state based on a 5-N·m external rotation moment applied in the testing condition. Statistical significance was assumed for P < .05. The post hoc comparisons were limited to flexion angles of 30°, 45°, 60°, and 90° to minimize the effects of multiple comparisons.
Results
Selective Cutting Effect on Tibial External Rotation Limits
The mean external rotations in the intact knee were 13.4° ± 3.4° to 7.2° ± 8.5° at 30° to 120° of flexion, respectively. In group 1, cutting the POP in the intact knee (first cut, PFL intact) resulted in increases in external tibial rotation of 0.5° to 2.0° (at 30°-120° of flexion) (Figure 4 and Table 1). These changes were not statistically significant (P > .05). Additional sectioning of the PFL (second cut) resulted in a greater increase in external tibial rotation of 2.8° to 5.0°. This increase, while small, was statistically significant (P = .029).
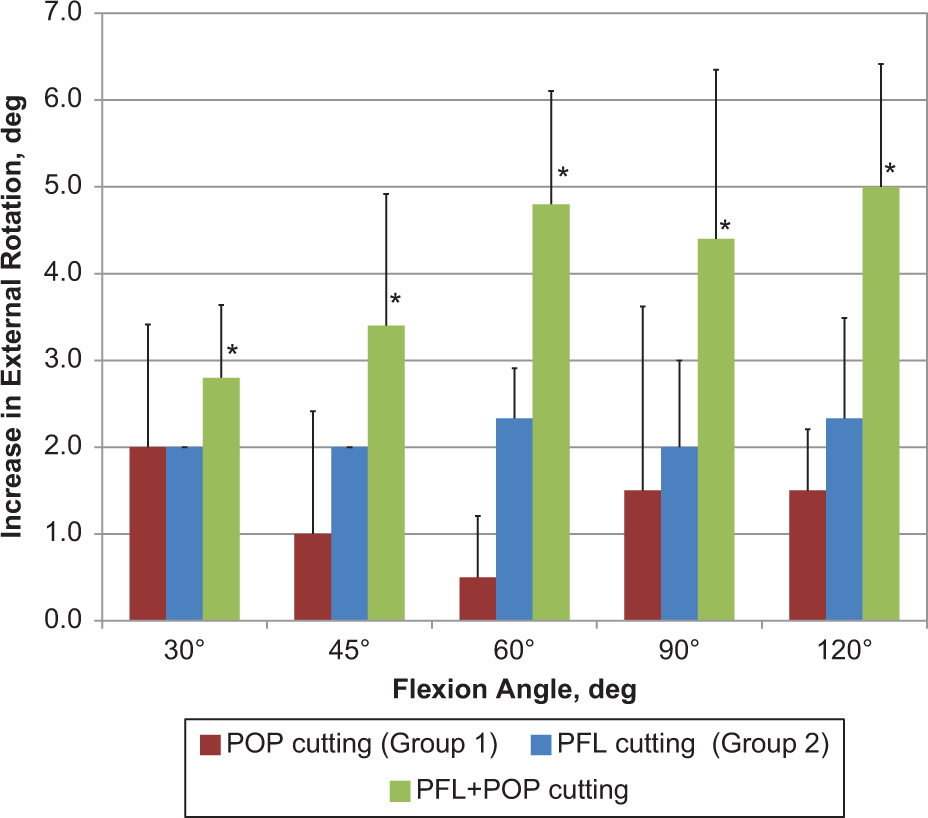
Analysis of selective cutting effect on tibial external rotation limits: comparisons between the isolated popliteus tendon (POP) cutting (group 1), isolated popliteofibular ligament (PFL) cutting (group 2), and PFL + POP cutting. *Statistically significant difference.
Comparison of Increases in Tibial External Rotation After the POP Cutting (Group 1), PFL Cutting (Group 2), and PFL + POP Cutting a
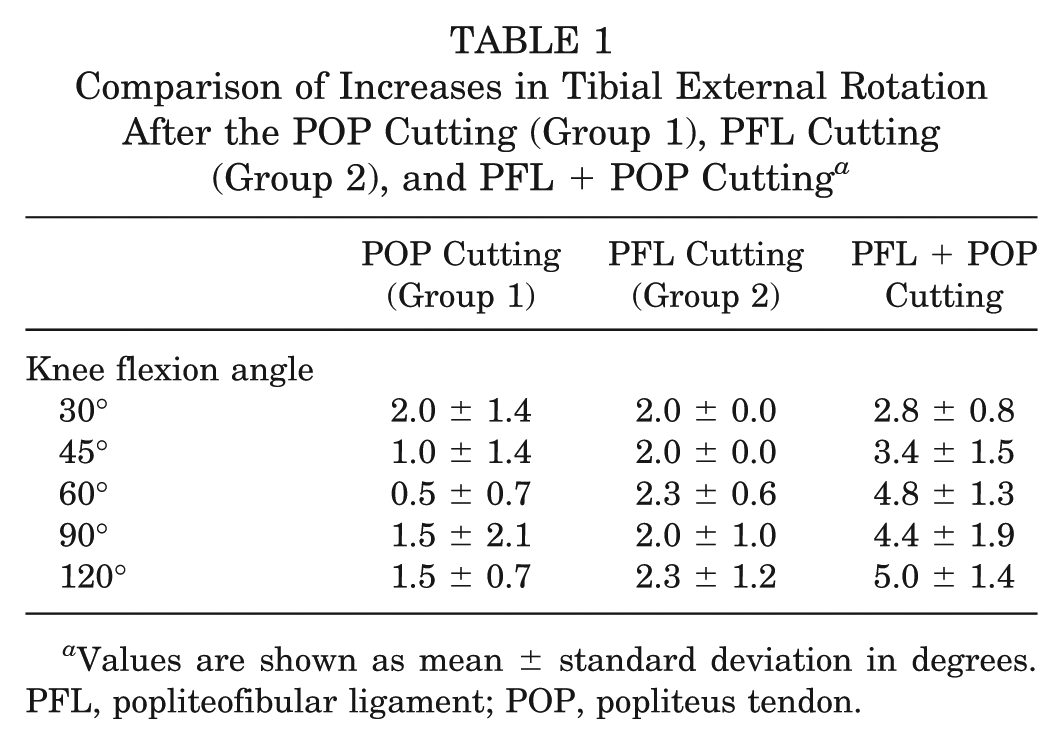
Values are shown as mean ± standard deviation in degrees. PFL, popliteofibular ligament; POP, popliteus tendon.
In group 2, cutting the PFL in the intact knee (first cut, POP intact) produced only a slight increase in external tibial rotation from 2.0° to 2.3° (at 30°-120° of flexion) (Figure 4 and Table 1). These changes were not statistically significant (P > .05). Subsequent sectioning of the POP led to a statistically significant increase in external tibial rotation, ranging from 2.8° to 5.0° (P = .030).
PLC Reconstruction Effect on Tibial External Rotation Limits
Compared with the external tibial rotation of the POP + PFL cut state, the mean external tibial rotation of the intact knee decreased 3.9° ± 1.6° (range, 1°-7°), and the PFL-reconstructed knee decreased 6.2° ± 3.8° (range, 1°-14°) at knee flexion angles from 30° to 90° of flexion. After comparing the PFL-reconstructed to the intact state, there were no significant differences (P > .05) (Figure 5 and Table 2). After POP reconstruction, the mean external tibial rotation decreased 10.2° ± 3.7° (range, 5°-18°) from 30° to 90° of flexion. After POP + PFL reconstruction, the mean external tibial rotation decreased 11.6° ± 4.2° (range, 4°-21°) from 30° to 90° of flexion. Comparing the POP or POP + PFL reconstruction to the intact state, there were statistically significant differences (P < .05) (Table 2). Comparison of the POP and the POP + PFL reconstructions showed no significant differences in external rotation between the 2 states from 30° to 90° of flexion (P > .05) (Table 2).
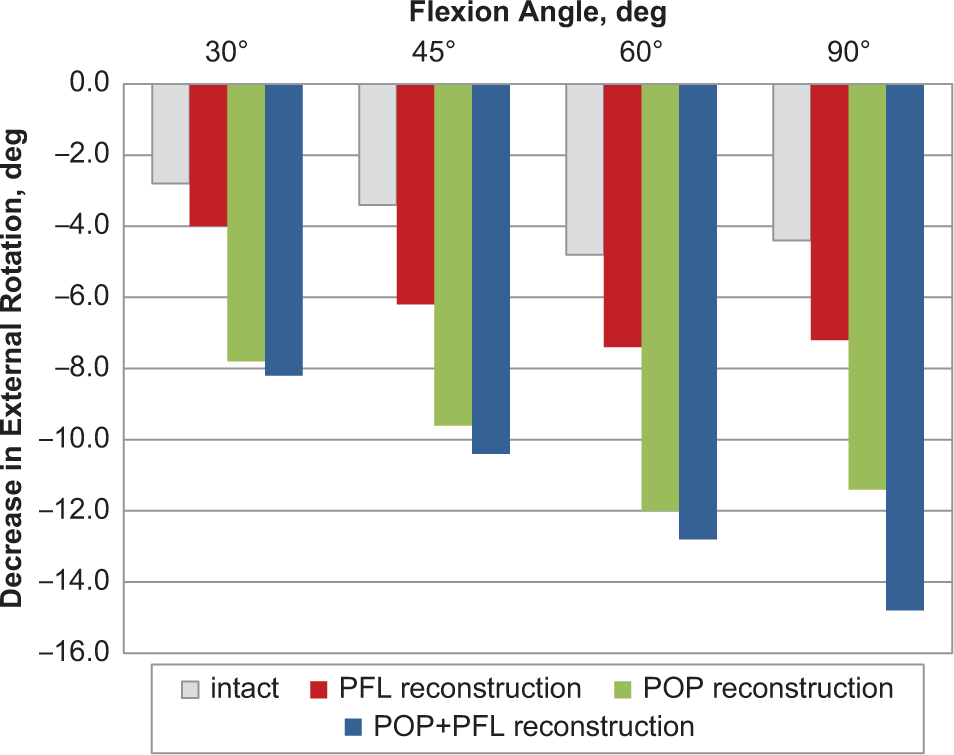
Tibial external rotation limits of the 3 posterolateral corner reconstruction techniques compared with the intact knee. PFL, popliteofibular ligament; POP, popliteus tendon.
P Values of Multiple Comparisons Among the Intact and Reconstructed States at Different Knee Flexion Angles a
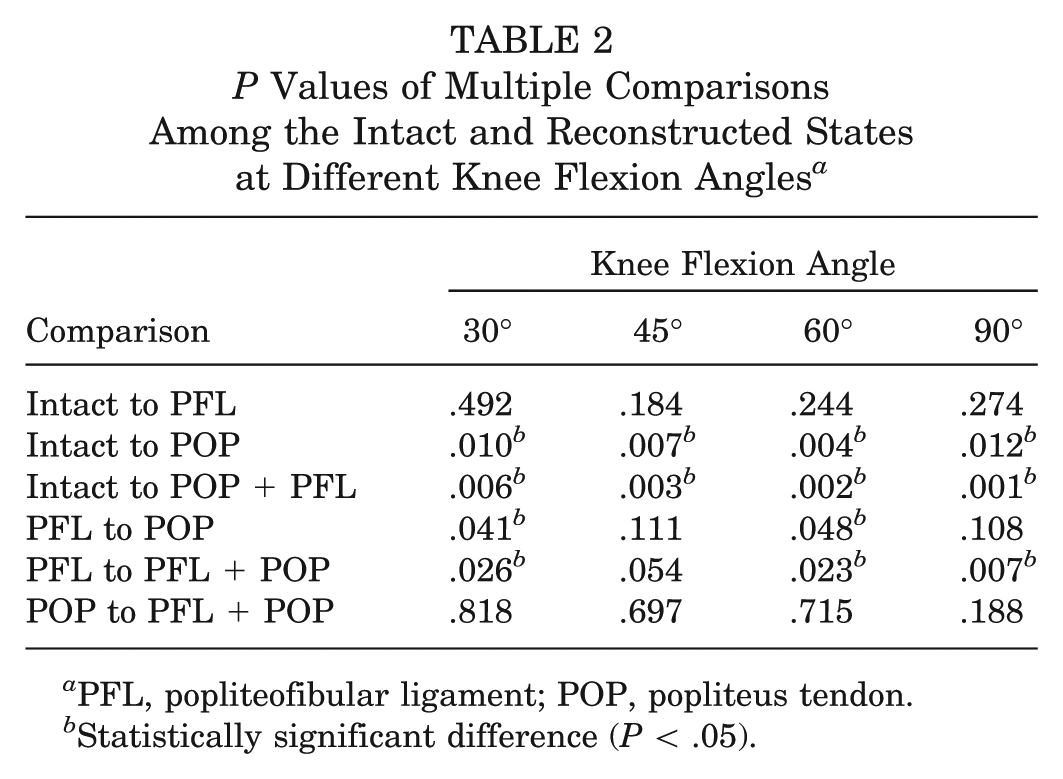
PFL, popliteofibular ligament; POP, popliteus tendon.
Statistically significant difference (P < .05).
Discussion
The most important finding of this study was that all the surgical procedures that we described and tested were able to reduce the increase in external tibial rotation that occurred after sectioning of the POP and PFL in an LCL-intact PLC injury model, thus confirming our original hypothesis. The PFL reconstruction technique was able to restore external rotation to near normal. However, the techniques involving POP reconstruction overconstrained external rotation during laxity testing. Moreover, the POP and PFL together provide the primary tibial external rotation stability, allowing these structures to be clinically considered as a single functional unit.
Reviewing the literature, we found that only a few in vitro studies focused on the biomechanical function and surgical reconstruction of the POP and PFL with an intact LCL. LaPrade et al 3 analyzed the static function of the POP and evaluated the anatomic reconstruction technique for POP. Nau et al 5 conducted a 3-dimensional kinematic study to compare the effects of the POP with the POP + PFL reconstruction. Shahane et al 8 designed an experimental study that focused on the assessment of PFL function and reconstruction on the status of an intact LCL and disruption. The published works only focused on the function of the individual structure (POP or PFL); the current study was the first in vitro study that compared the biomechanical function and surgical reconstruction of both the POP and PFL with an intact LCL.
The chosen injury pattern in the present study may not be applicable for all PLC injuries that are observed clinically. The reason that we chose to not include LCL laxity in our PLC injury model is that, in the senior author’s (H.Z.) clinical practice, there is a subset of patients who have increased external tibial rotation of at least 10° compared with the opposite knee as measured by the dial test with an intact or minimally affected LCL. Additional findings in this subset of patients included a grade 3 posterior drawer sign and no increase in varus laxity as measured by stress radiographs. These findings suggest that these patients have a combined PCL and PLC injury with an intact or minimally affected LCL.
The primary ligamentous restraint for external tibial rotation has been debated by various authors.3,4,6,8 Pasque et al 6 reported that sectioning of the PFL alone produced no significant changes on the limits of knee movement; however, sectioning of the PFL and POP at the femoral attachment produced a small but significant increase of 5° to 6° in external rotation from the flexion angles of 30° to 120°. The authors concluded that the POP, PFL, LCL, and posterolateral capsular structures function as a unit. No individual structure alone is the primary restraint. 6 However, LaPrade et al 3 reported that significant increases (3° to 6°) in external rotation were found after sectioning the POP and concluded that the POP has important primary stabilization roles at the knee. Shahane et al 8 found that sectioning of the PFL alone can cause excessive primary external rotation, whereas isolated sections of the belly of the POP does not cause significant posterolateral instability. The results of the current study agreed with those of the study of Pasque et al 6 : Sectioning both the PFL and POP produced small (2.8° to 5.0°) but statistically significant increases in external rotation.
Combined injuries to the POP, PFL, and LCL are commonly found in PLC injuries, and various surgical procedures such as direct repair, augmentation with the iliotibial band or biceps tendon, 1 recess procedures, and reconstruction with autograft or allograft tissue1-4,9,10 have been described to treat posterolateral laxity resulting from this injury pattern. However, there are no clear guidelines or consensus on how to treat the injury pattern of increased external tibial rotation in which the LCL is intact.
On the basis of the recognition of the 3 key components functioning together as a unit, Pasque et al 6 recommended that operative reconstruction should address all of the posterolateral structures because restoration of only an individual structure may result in residual instability. However, the authors did not prove the opinion with experimental comparison between the different surgical techniques. 6
LaPrade et al 3 and Ricchetti et al 7 both found that an isolated popliteus reconstruction may be used in cases of posterolateral knee injuries with a primary external rotation instability pattern in which varus rotation is minimally affected. Nau et al 5 reported that POP reconstruction as well as POP + PFL reconstruction can restore external rotation to near normal at 30° and 90° of knee flexion. Shahane et al 8 performed a cutting and reconstruction study and concluded that reconstruction of the PFL restores posterolateral stability in posterolateral disruption in which the LCL is intact. The results of the present study demonstrated that all of the 3 tested reconstruction techniques were able to eliminate increased external tibial rotation after sectioning of the POP and PFL with an intact LCL. Moreover, this result showed that, although the PFL and POP were found to resist external rotation together, reconstruction of a single structure could restore stability. We speculate that the findings in our study can be explained by the fact that the reconstructed POP graft was better able to resist external tibial rotation compared with the native POP and that the PFL reconstruction placed the graft in a more favorable alignment for resisting external tibial rotation compared with the native PFL.
Regarding the techniques involving POP reconstruction (POP reconstruction and POP + PFL reconstruction), the results in the present study demonstrated an overconstraint of external rotation, which was comparable to the results reported by LaPrade et al, 3 who compared the reconstructed state with the intact state and found no significant differences at knee flexion angles of 0° and 20° but significant decreases of external rotation at angles of 30°, 60°, and 90°. Our results are also comparable with the results reported by Nau et al, 5 who reported that there was a tendency to overconstrain tibial external rotation for POP reconstruction and POP + PFL reconstruction procedures.
In close agreement with the previous findings by Shahane et al, 8 the results of the present study further confirmed the effectiveness of the PFL reconstruction technique, which was able to restore external rotation to near normal. In addition, this technique was shown to have favorable clinical outcomes9,10 and have advantages of a mini-open procedure, 10 use less amount of graft material, and minimize the intervention of the native posterolateral structures. Therefore, regarding its mechanically and clinically approved reliability as well as the minimally invasive advantage, PFL reconstruction could be an optimal surgical alternative for knees with isolated external rotation instability.
Strengths and Limitations
The current study offers 3 advantages. First, this is the first study to compare the POP and/or PFL reconstruction techniques in an LCL-intact injury model. Second, given the features of accurate and dynamic measurements provided by the navigation system developed for ACL reconstruction, it was used in our study to measure knee kinematics. The real-time changes in knee kinematics presented by the system provided valuable information to examine the intact, sectioned, and reconstructed status. Third, use of the whole length of the lower limb made it possible to determine the foot position and therefore indicate the neutral position of the knee joint in rotation. During PLC reconstruction, it is important to fix the grafts in neutral rotation to avoid overconstraining the knee in external rotation during surgical procedures.
There are 3 experimental limitations to our tests that deserve comment. First, the function of the dynamic stability provided by the posterolateral structures was not addressed in this study. It is possible that the magnitude of the in situ forces loaded on these structures may be different compared with in vivo conditions. Second, the time zero biomechanical tests were not able to fully simulate in vivo conditions, where graft healing and maturation are the most important clinical issues. Third, varus rotation was not measured in this study.
Conclusion
In an LCL-intact PLC injury model, the POP and PFL function as a unit in resisting external rotation. All surgical procedures that we described and tested were able to reduce the increased external rotational laxity found in the sectioned state. The PFL reconstruction technique was able to restore external rotation to near normal. However, the techniques involving POP reconstruction overconstrained external rotation during laxity testing.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.