
Abstract
Background:
Ulnar collateral ligament (UCL) reconstruction aims to restore valgus stability, and numerous techniques have been described in the literature.
Hypothesis/Purpose:
To biomechanically compare the GraftLink (GL) technique with traditional bone tunnels used in the docking (DO) technique. It is hypothesized that the GL method will offer a stiffer, less lax construct compared with the DO.
Study Design:
Controlled laboratory study.
Methods:
Native and reconstructed states were tested in 7 matched pairs of cadaveric arms. To test kinematics, a 1.5-N·m valgus torque was applied and the resultant displacement at 15° to 90° of flexion was measured. Dissipated energy and the torque at the peak of the 10th cycle of preconditioning were analyzed during kinematic tests. Failure testing was performed by internal rotation of the humerus at 4.5 deg/s in 70° of flexion. Ulnotrochlear joint (UTJ) gapping was quantified during failure tests by use of video tracking.
Results:
Kinematics testing revealed no differences between the native state and the reconstructed state in either the DO or the GL group at any flexion angle. Stiffness was lower in the reconstructed specimens in both the DO (39.92 N·m/rad) and GL (50.74 N·m/rad) groups compared with their matched native states (DO Native, 71.41 N·m/rad, P = .005; GL Native, 86.36 N·m/rad, P = .002). There was no difference in stiffness between DO and GL. Reconstructed specimens in the GL group had lower torque at failure compared with native specimens (17.404 N·m vs 24.63 N·m, P = .038), but there was no difference in the DO group at failure. There was no difference in torque at failure between DO and GL. The DO exhibited higher angular displacement at failure compared with the native state (34.21° vs 21.79°, P = .010) and compared with the GL when normalized (1.58-fold vs 1.19-fold, P = .039). Compared with their native states, both DO and GL had significantly higher UTJ gapping at 3 N·m and at failure. The DO had significantly higher normalized UTJ gapping than the GL at 3 N·m (P = .037) and at failure (P = .043).
Conclusion:
The DO and GL both restored joint kinematics under low loading conditions. Although less stiff, the GL exhibited lower joint gapping and laxity than did the DO.
Clinical Relevance:
Understanding the biomechanics of UCL reconstruction has significant implications for postoperative management as it relates to early rehabilitation. Biomechanically inferior constructs could risk graft failure or early loosening during rehabilitation, and comparing the biomechanics of new techniques to established, widely used procedures such as the docking technique can provide important information about the immediate postoperative performance.
Keywords
Valgus elbow stability is derived from the anterior bundle of the ulnar collateral ligament (UCL).20,22 Overhead athletes, such as baseball pitchers, javelin throwers, and tennis players, place large stresses on the UCL,5,10,32 and UCL injury is well described in these athletes. Nonoperative treatment has been described, 23 but surgical reconstruction has been shown to lead to the best clinical outcomes and the fastest return to activity.3,8,24,31
A variety of UCL reconstruction techniques have been described since the original technique by Jobe et al. 14 As surgical management has turned to less invasive and more anatomic techniques, numerous authors have described variations of the UCL reconstructions.13,16,26,28 Techniques can vary regarding the use of interference screws and cortical buttons, the number of ulnar bone tunnels, the number of strands in a graft, and bone tunnel placement. Placement of the ulnar fixation within the native UCL footprint is a desirable reconstruction trait in efforts to recreate native anatomic features. Furthermore, a reconstruction technique that involves limited soft tissue dissection and requires a single reamed socket is less invasive. Several single-socket UCL reconstructions have been described,1,2,15,17 many of which use an interference screw.
The GraftLink UCL reconstruction (Arthrex Inc, Naples, Florida) is a new technique that uses 2 ACL TightRopes (TRs; Arthrex) to create a reconstruction with cortical buttons and self-reinforcing tensioning sutures on both the humeral and the ulnar side. The single ulnar socket used in this technique offers an anatomic reconstruction, and cortical suspension using tensioning sutures and a cortical button places the graft in direct contact with reamed bone within the ulnar and humeral sockets without an interference screw.
The purpose of this study was to biomechanically test the kinematics and failure properties of the new GraftLink UCL reconstruction technique compared with the traditional bone tunnels used in the docking technique. We hypothesized that the GraftLink UCL reconstruction provides a stiffer reconstruction than the docking technique and that both the docking and GraftLink techniques restore valgus stability under low-load kinematic testing.
Materials and Methods
Sample Information
Seven matched pairs of cadaveric arms (6 female, 1 male; age, 56.4 ± 5.8 years; range, 51-64 years) with no documented history of musculoskeletal or metabolic disorders, fractures, dislocations, or ligamentous injuries to the elbow were selected for this study. All specimens were stored at −20° C until the time of testing and underwent only 1 freeze-thaw cycle. Each specimen was dissected to expose the humeral and ulnar/radial diaphysis, and both the humerus and ulnar/radius were potted in a cylindrical mold of potting compound (polyester resin, Evercoat, Cincinnati, Ohio). Each specimen underwent testing of the native UCL, and specimens within a matched pair were then randomized to either the docking group (DO) or the GraftLink group (GL). All reconstructions were performed by 2 sports medicine fellowship–trained orthopaedic surgeons. Fresh bovine extensor tendons were used for all reconstructions to standardize graft strength between groups and to avoid variability in autologous cadaveric tendon grafts, namely the palmaris longus tendon generally used as a graft in UCL reconstruction.
Docking UCL Reconstruction
Medial soft tissue was dissected from the elbow. The flexor pronator mass was removed for visualization of the entire anterior bundle of the UCL. Next, an incision was created in the capsule along the anterior border of the UCL to limit the biomechanical influence or reinforcement that the capsule may add to the anterior bundle of the UCL. After testing of the native UCL, all elbows were randomized to a group. A 5-mm socket was drilled to a depth of 15 mm from distal to proximal at the humeral footprint of the anterior bundle of the UCL. Two converging 2-mm drill holes were made by use of a C-guide (Arthrex) in a proximal to distal direction. The drill holes were anterior to the intermuscular septum. Two loops of suture were then passed by use of a Hewson suture passer and secured at the humeral footprint for graft passage (Figure 1). A UCL guide (Arthrex) was positioned on the sublime tubercle 6 mm distal to the joint line, at the footprint of the native UCL. As the ulna was drilled, a guide was used to ream 4-mm intersecting bone tunnels separated by 6 to 7 mm on the cortex. The bovine extensor tendon graft ends were whip-stitched with No. 2 Fiberwire (Arthrex) and wrapped in saline-soaked towels until the time of implantation. A wire loop was then used to pass the tendon through the intersecting bone tunnels. One end of the whip-stitched graft was pulled into the humeral socket by 1 suture loop. Graft length was estimated in 30° of flexion with a varus force applied by an assistant. The proposed length was marked, and the tendon was cut 1 cm proximal to this demarcation and whip-stitched. The graft was then passed into the humeral socket with the remaining suture loop. Consistent with the surgical description of the docking technique, 24 the elbow was positioned in 30° of flexion with a varus force, and the 4 suture limbs were tied with 4 square knots and then an additional 3 square knots with a single suture from each limb (Figure 1).
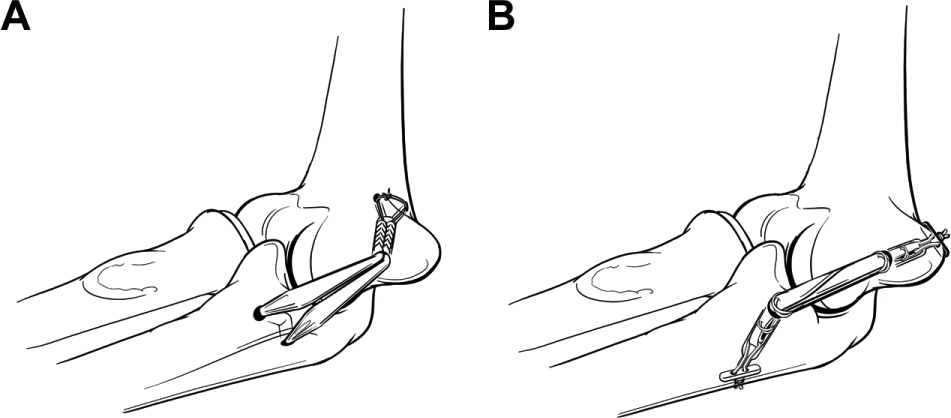
Schematic illustrations of the intersecting bone tunnels on the sublime tubercle as used in (A) the traditional docking technique and (B) the GraftLink technique, which uses 2 TightRopes to secure a folded graft with a single ulnar socket and uses cortical button suspension on both the ulnar and humeral side. In the absence of ulnar nerve transposition, the humeral cortical button should be placed slightly anterior to the humeral midline, and if an ulnar nerve transposition is performed, the button should be placed slightly posterior to the midline.
GraftLink UCL Reconstruction
A 3.5-mm spade-tipped guide pin (Arthrex) was placed on the sublime tubercle 6 mm distal to the joint line at the site of the native UCL footprint. 9 The guide pin was initially directed perpendicular to the sublime tubercle, and a 6-mm cannulated reamer (Arthrex) was used over the spade-tip guide wire to create the ulnar socket. The guide pin was then directed at 30° in both the sagittal and coronal planes, as described by Lee et al, 16 to create a hole in the lateral ulnar cortex. Injury to the proximal radioulnar joint and to the posterior interosseous nerve was avoided by passing carefully through the opposite cortex. Then, a 3.5-mm spade-tipped guide pin was placed on the humeral attachment of the UCL on the inferior aspect to the medial epicondyle. The guide pin was initially directed perpendicular to the attachment and was then directed through the posterior cortex. A 6-mm cannulated reamer was used over the spade-tip guide wire to create the humeral socket.
To prepare the GraftLink graft, the bovine extensor tendon graft was passed through the loops of 2 TRs and folded to a final graft length of 40 mm. While tension is maintained on the graft ends, cerclage-type sutures are passed through and around each end of the graft. Care must be taken to include each strand of graft in these sutures. One cerclage suture is passed at each end of the graft. The cerclage sutures are started from inside so that the knot will be “buried” in the graft center. The final graft diameter was 6 mm, which was verified with a graft sizing guide (Arthrex), which ensures that the graft can pass through a 6-mm hole. Prepared grafts were wrapped in saline-soaked towels without any tension until the time of implantation.
Once the GraftLink construct was prepared, the ulnar TR was passed through the ulnar cortex and the button was flipped while the suture loop was kept loose. Next, the humeral TR was passed through the humerus and the button was flipped on its posterior cortex. During procedures, care should be taken to avoid injury to the ulnar nerve. If an ulnar nerve transposition is performed, the button should be placed slightly posterior to the midline of the humerus. If no transposition is performed, the button should be placed slightly anterior to the midline. Dissection was used to confirm that the buttons had flipped. Next, the TR at the ulnar side was slowly tensioned to position the graft partially into the socket. The humeral TR was then partially tensioned, which positioned some of the humeral side of the graft in its socket. Then, in succession, the ulnar and humeral TR sutures were tensioned to fully position each side of the graft in its socket with the elbow in 30° of flexion with a varus force applied by an assistant. Both TightRope sutures were then tied with 4 square knots and an additional 3 square knots with a single suture from each limb (Figure 1).
Kinematics Testing
Testing was performed with a biaxial servohydraulic materials testing machine (Mini Bionix II, MTS, Eden Prairie, Minnesota). All specimens were secured in neutral forearm rotation in a mechanical testing fixture that could apply a given torque or angular displacement to the humerus to induce valgus displacement and, consequently, valgus stress to the elbow (Figure 2). The fixture enables elbow flexion angles between 15° and 90° and can account for varying carrying angles. Biomechanical testing of UCL reconstructions using torsion about the humerus has been previously demonstrated to be representative of anatomic loading. 25 The elbow was kept moist during the entire testing period with normal saline solution at room temperature. All testing was performed at room temperature. A testing protocol was used to assess the kinematics of each specimen, consistent with previous studies.12,15,19 Testing involved a preload of 0.2 N·m, preconditioning with 10 loading-unloading cycles of 5° of valgus rotation (ie, humeral internal rotation) at a rate of 4.5 deg/s, 1 loading-unloading cycle of 7.5° of valgus rotation at a rate of 4.5 deg/s to assess hysteresis, a 60-second preload of 0.2 N·m, and a 1.5-N·m valgus torque applied for 5 seconds at a rate of 0.5 N·m/s. The resultant angular displacement was recorded as the primary measure of kinematics at the end of this hold. Kinematic testing was repeated at 15°, 30°, 45°, 60°, 75°, and 90° of flexion. Flexion angles were confirmed with a goniometer.
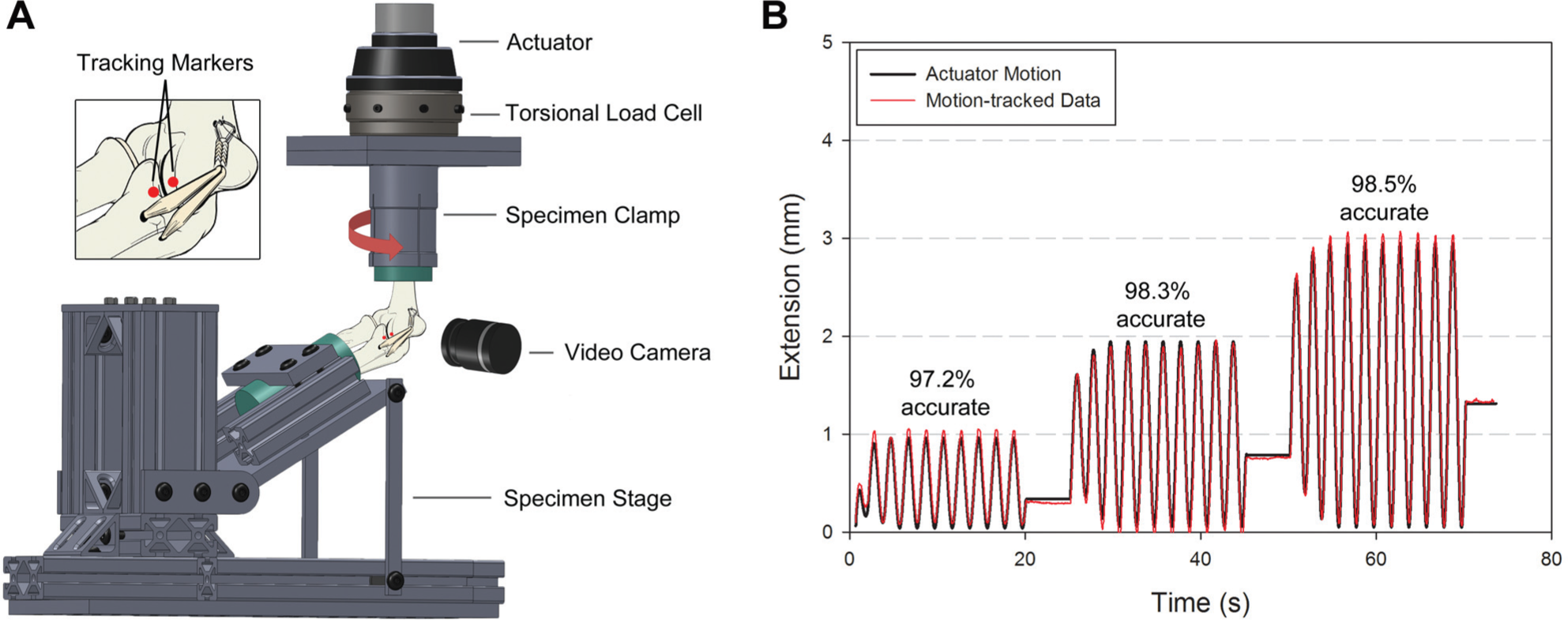
(A) A custom testing fixture used to apply a given torque or angular displacement to a clamped humerus (ie, internal humeral rotation). The fixture is adjustable for flexion angles between 15° and 90° and is able to account for variability in carrying angle. A video camera was mounted perpendicular to the ulnotrochlear joint to record the motion of 2 tracking markers placed at the periphery of the joint (inset). (B) Video tracking software was used to quantify ulnotrochlear joint gapping, and this method was optimized and verified to be 97.2% accurate during 1-mm displacement cycles, 98.3% accurate during 2-mm cycles, and 98.5% accurate during 3-mm cycles.
Failure Testing
After kinematic testing, failure testing was performed by preloading each specimen to 0.2 N·m for 10 seconds and applying a valgus rotation to failure at 4.5 deg/s at 70° of elbow flexion. Failure was characterized by a drastic decrease in torsional torque recorded by the load cell, at which point the test was terminated.
Suture Pull-out Testing of Bovine Extensor and Palmaris Longus Grafts
To compare the suture pull-out properties of cadaveric palmaris longus (PL) tendon grafts and fresh bovine extensor (BE) tendon grafts, a suture pull-out test was performed. Five PL tendon grafts chosen from random cadavers in this study and five 6-mm BE tendon grafts were cut to a length of 50 mm and whip-stitched with No. 2 Fiberwire. The free limbs of the sutures were securely clamped in tensile testing grips in a uniaxial electromechanical materials testing machine (Insight, MTS). After a 10-second 5-N preload, each specimen was loaded to failure at a rate of 0.5 mm/s, corresponding to 1% strain per second. Ultimate failure load, stiffness, and strain at failure were calculated from generated load-displacement curves, and these variables were compared between PL and BE grafts by use of t tests with alpha = 95%.
Ulnotrochlear Joint Gap Quantification
Ulnotrochlear joint gapping (UTJ) was quantified during failure testing by use of video tracking techniques. At 70° of elbow flexion, two 1-mm-diameter, 4-mm-long stainless steel pins with 3-mm colored heads were inserted into the bone immediately anterior to the native ligament or the reconstruction. One pin was placed approximately 3 mm proximal to the ulnotrochlear joint line, and the other pin was placed approximately 3 mm distal to the ulnotrochlear joint line. This positioning was previously shown to be optimal for joint gapping quantification because no soft tissue such as the capsule, the native ligament, or the reconstruction graft interfered with the pin or caused any unwanted motion of the pin.
Digital video data of each failure test were obtained with a high-definition video camera at 1080-pixel resolution, 30 frames per second (fps) (Canon Rebel T2i, Canon, Tokyo, Japan). The camera was mounted on a static tripod and oriented perpendicular to the ulnotrochlear joint surface at the site of the reconstruction. The UTJ gapping was quantified from obtained video data by use of video analysis software able to track the relative motion of specified objects (Tracker v 4.72, Open Source Physics, Davidson College, Davidson, North Carolina). A scale was calibrated by placing a digital caliper at a known caliper gap (10.00 mm) immediately next to the colored pins and at the same camera-to-object distance. This method is similar to previously published UTJ gap quantification methods that use video tracking. 2 We tested the accuracy of this method by displacing the pins cyclically to 3 separate, known displacements (5 cycles at 1-mm total displacement, 5 cycles at 2-mm total displacement, and 5 cycles at 3-mm total displacement) using an electromechanical testing machine (Insight). Video data were collected at a similar camera-to-object distance. The videos were calibrated with the same calibration method as described above, and displacement quantification was performed with the Tracker software. The method was found to be 97.2% accurate at 1-mm cyclic displacement, 98.3% accurate at 2-mm cyclic displacement, and 98.5% accurate at 3-mm cyclic displacement. Gapping of the UTJ was analyzed only during failure tests at 3 N·m of applied torque and at ultimate failure.
Data and Statistical Analysis
Data were sampled at 100 Hz during each mechanical test. Video data were sampled at 30 fps. Data sets from kinematic testing were analyzed to obtain the torque at the peak of the 10th conditioning cycle at each elbow flexion angle, the hysteresis (defined as the energy dissipated by the ligament or graft during a loading-unloading cycle), and the angular displacement attributable to an applied 1.5-N·m valgus torque. Hysteresis was calculated by subtracting the area under the curve of the unloading curve from the area under the curve of the loading curve on a torsional torque versus radian plot. Stiffness, torque, and angular displacement were analyzed from failure testing. Stiffness was calculated by deriving the slope of the linear region of a load/torque-angular displacement graph. Initial stiffness is defined as the stiffness between 1 and 3 N·m and corresponds to the toe region of the torque-displacement graphs. Total stiffness was calculated in the linear elongation region, which was found between ~5 N·m and immediately before the yield point. Torsional torque was analyzed at both 5° and 15° of valgus rotation as well as at ultimate failure. We chose 5° of rotation to analyze torque at a low displacement point. We chose 15° of rotation because this was the highest point at which all but 1 torque-displacement graph remained linear and it corresponds to high prefailure displacement. Failure torsional torque was defined as the highest point before a rapid decrease in torque. Angular displacement was analyzed as a measure of joint laxity at 3 N·m, to analyze low-loading laxity, and at ultimate failure. Gapping of the UTJ was analyzed during failure tests both at 3 N·m and at ultimate failure.
Differences in each assessed variable between the native and reconstructed state were determined with repeated-measures analysis of variance. Corrections for alpha in post hoc comparisons were performed with a Bonferroni test, with alpha = 95%. Differences in each assessed variable between the DO and GL group were determined by normalizing data from reconstruction tests to the paired native test and comparing the ratio with a paired t test with alpha = 95% (SigmaPlot v11.0, Systat Software Inc, Chicago, Illinois).
Results
Suture Pull-out Properties of Bovine Tensor and Palmaris Longus Tendon Grafts
Results of suture pull-out tests demonstrated equivalence of fresh-frozen bovine extensor tendons and cadaveric palmaris longus tendons. There was no significant difference in stiffness (15.64 ± 4.9 N/mm [PL] vs 19.95 ± 4.3 N/mm [BE], P = .182), ultimate failure load (132.94 ± 13.3 N [PL] vs 200.03 ± 56.7 N [BE], P = .052), or displacement at failure (11.66 ± 3.8 mm [PL] vs 16.08 ± 5.1 mm [BE], P = .181).
Kinematics Results
Data from native, DO, and GL tests all demonstrate decreasing angular displacement due to the applied 1.5 N·m torque with increasing flexion angle. This pattern is consistent with normal elbow kinematics, with tightening of the posterior band of the anterior bundle and the entire posterior bundle at increasing flexion angles. There was no significant difference in angular displacement due to an applied 1.5 N·m torque between either reconstruction technique and their paired native specimens at any flexion angle. Furthermore, there was no significant difference in normalized angular displacement between the DO and GL group at any flexion angle (Figure 3). There was a significant difference in torque at the peak of the 10th cycle of preconditioning between the reconstructed state and the native state in the DO group at 60° of flexion (Native, 3.09 ± 1.2 N·m vs DO, 2.30 ± 0.9 N·m; P = .046). There was no significant difference in torque at the peak of the 10th cycle of preconditioning between the reconstructed state and the native state in either the DO or the GL group in any other flexion angle (Figure 3). There was no significant difference between normalized torque at the peak of the 10th cycle of preconditioning when we compared the DO and GL groups directly at any flexion angle.
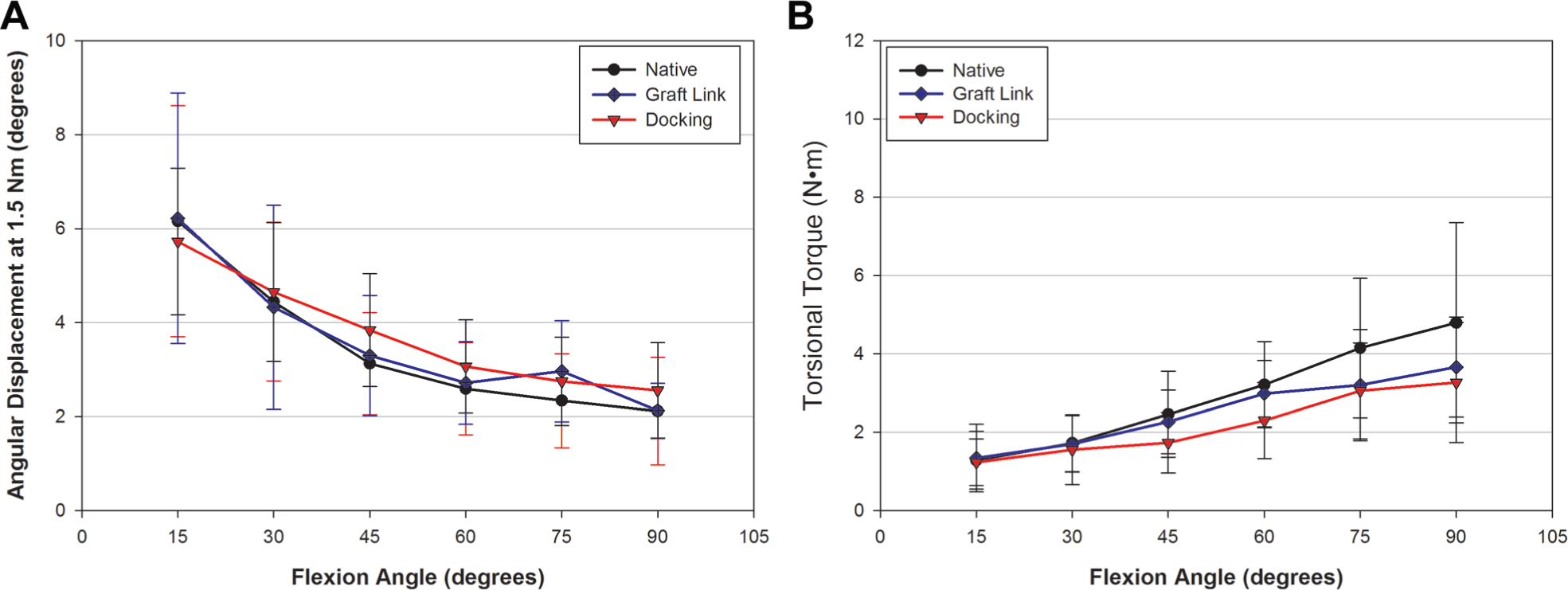
(A) Angular displacement attributable to a 1.5-N·m constant torque applied to the native ulnar collateral ligament (UCL) and specimens reconstructed with the GraftLink (GL) and docking (DO) techniques. There was no significant difference in angular displacement at any flexion angle. (B) The torsional torque at the 10th cycle of preconditioning (5° applied rotation) of the native UCL and the DO- and GL-reconstructed specimens. There was a significant difference in torque between the native state and the DO group at 60° of flexion. All other comparisons showed no difference.
Energy dissipated by the native ligament or reconstruction graft was analyzed at 15°, 45°, and 75° of flexion. Total dissipated energy increased with increasing flexion angle, demonstrating normal elbow kinematics. There was no difference in the dissipated energy between the native and reconstructed state in either the DO or the GL group at any flexion angle. In addition, there was no difference in normalized dissipated energy between the DO and GL groups directly (Figure 4).
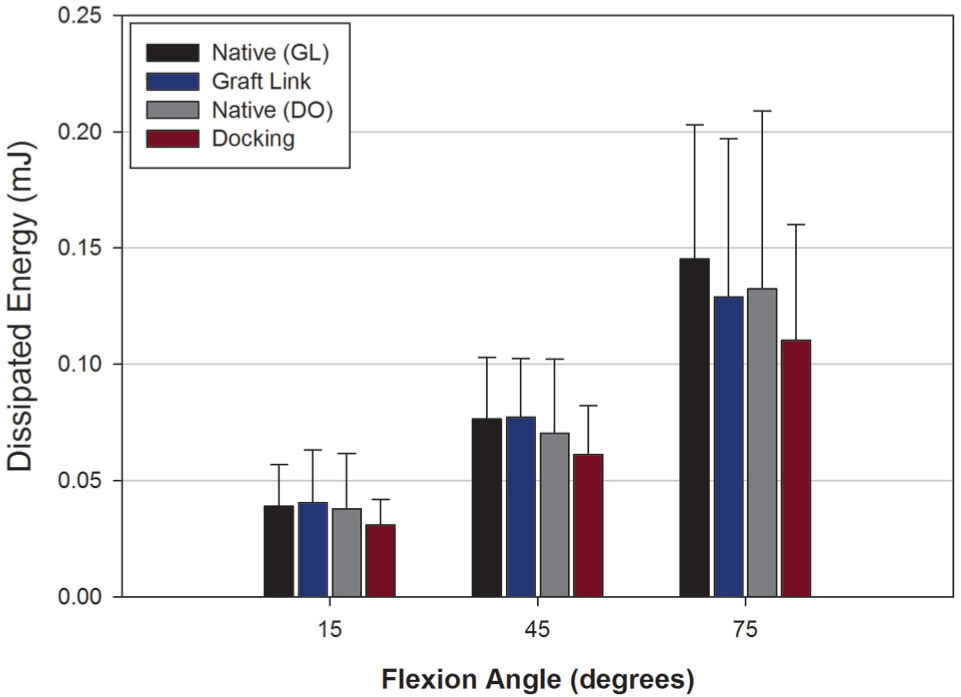
Energy dissipated by the ligament or graft during a loading-unloading cycle. There was no significant difference in dissipated energy between the reconstructed state and the native state in either the GL or the DO group.
Failure Results
Reconstructed specimens in both the DO and the GL group had significantly lower initial stiffness and lower total stiffness compared with their matched native specimens (initial stiffness: 37.07 ± 15.8 N·m/rad [DO] vs 56.53 ± 16.9 N·m/rad [Native], P = .013; 47.66 ± 18.5 N·m/rad [GL] vs 65.59 ± 24.3 N·m/rad [Native], P = .005; total stiffness: 50.74 ± 26.2 N·m/rad [GL] vs 86.36 ± 38.3 N·m/rad [Native], P = .002; 39.92 ± 17.6 N·m/rad [DO] vs 71.41 ± 27.5 N·m/rad [Native], P = .005) (Figure 5). There was no significant difference in normalized initial stiffness or normalized total stiffness when the DO and GL groups were compared directly.
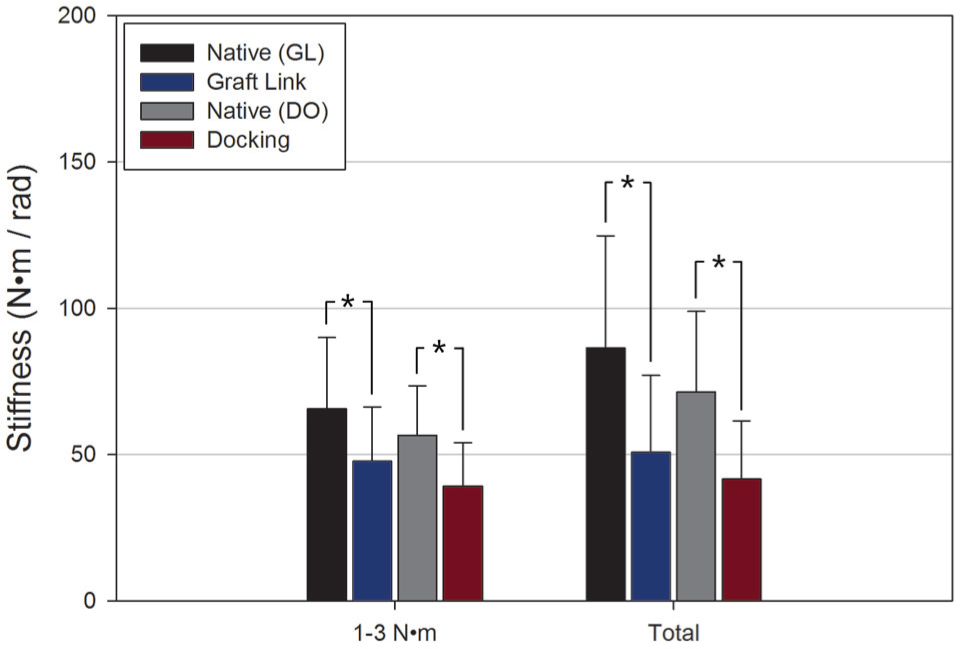
Stiffness of the native ulnar collateral ligament and the GraftLink (GL) and docking (DO) reconstructions during failure testing. Both the DO and the GL group exhibited significantly lower stiffness at 1 to 3 N·m and at high loading (total). There was no difference in normalized stiffness between the DO and GL groups. *Significant difference (P < .05).
Compared with their native values, reconstructed specimens in the DO group exhibited significantly lower torsional torque only at 15° of valgus rotation (10.28 ± 3.9 N·m [DO] vs 16.63 ± 6.1 N·m [Native], P = .006), but there was no significant difference at 5° of valgus rotation (2.84 ± 1.3 N·m [DO] vs 4.75 ± 2.1 N·m [Native], P = .053) or at ultimate failure (18.86 ± 7.9 N·m [DO] vs 23.27 ± 4.6 N·m [Native], P = .068). Reconstructed specimens in the GL group exhibited significantly lower torsional torque at 5° of valgus rotation (4.35 ± 1.8 N·m [GL] vs 6.23 ± 2.7 N·m [Native], P = .022), at 15° of valgus rotation (12.21 ± 4.5 N·m [GL] vs 19.36 ± 6.9 N·m [Native], P = .006), and at ultimate failure (17.404 ± 5.4 N·m [GL] vs 24.63 ± 8.0 N·m [Native], P = .038). When normalized torsional torque was compared between DO and GL, no significant differences were found at any valgus rotation or at failure (Figure 6).
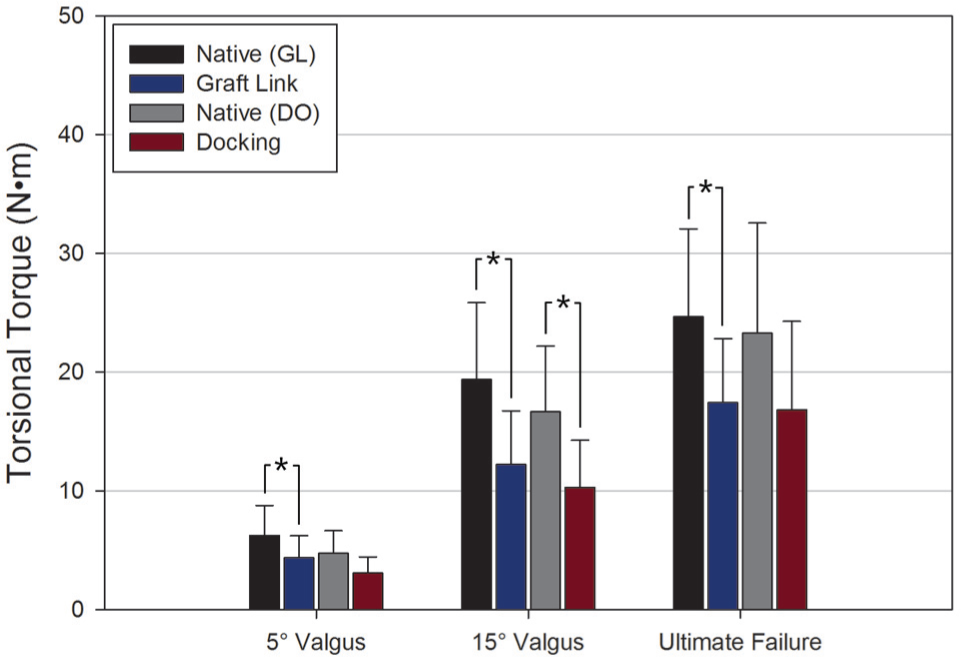
Torque analyzed at 5°, at 15°, and at ultimate failure during failure testing. Both the GraftLink (GL) and docking (DO) techniques had lower torque at 15° compared with their native values, but only the GL had lower torque at 5° and at ultimate failure compared with its native state. There was no significant difference in normalized torque between the DO and GL techniques at any point of analysis. *Significant difference (P < .05).
Both the DO and the GL group had significantly higher angular displacement at 3 N·m (5.67° ± 1.5° [DO] vs 3.86° ± 1.7° [Native], P = .035; 4.18° ± 1.5° [GL] vs 3.06° ± 1.4° [DO], P = .020), but only the DO group exhibited significantly higher angular displacement at failure compared with its matched native state (34.21° ± 7.9° [DO] vs 21.79° ± 4.8° [Native], P = .010). There was no significant difference in angular displacement at failure between the GL reconstruction and its matched native state (24.87° ± 5.7° [GL] vs 21.70° ± 4.5° [Native], P = .347) (Figure 7). The DO group had significantly higher normalized angular displacement compared with the GL group only at failure (1.58-fold ± 0.2 [DO] vs 1.19-fold ± 0.2 [GL], P = .039).
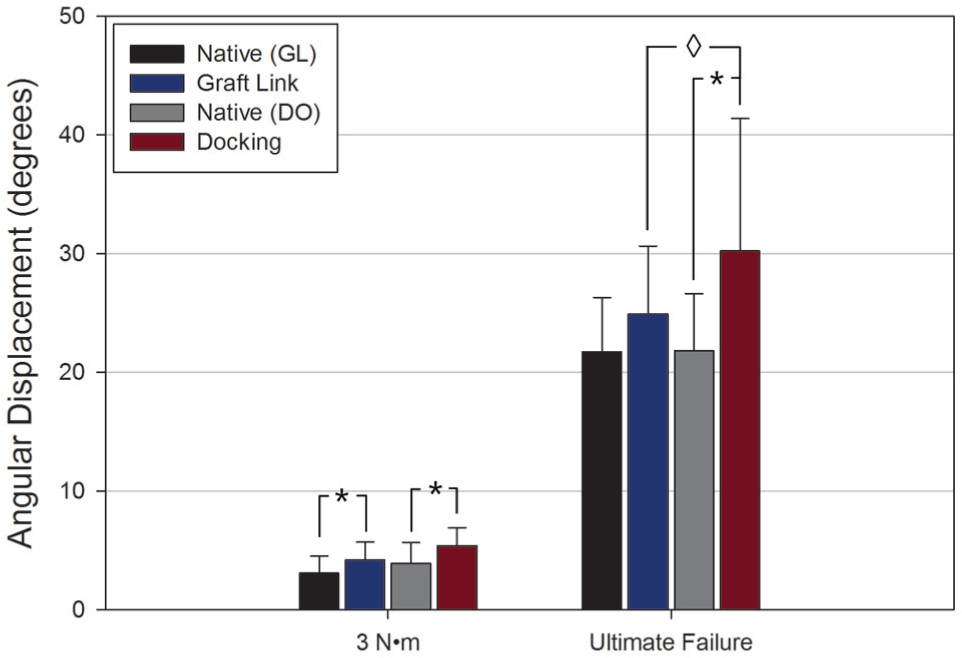
Angular displacement analyzed at 3 N·m and at ultimate failure collected during failure testing. Both the GraftLink (GL) and docking (DO) techniques exhibited higher angular displacement at low loading (3 N·m) compared with their native values, while only DO exhibited higher angular displacement at failure. The DO technique exhibited significantly higher normalized angular displacement compared with the GL. *Significant difference between native and reconstructed state (P < .05). ⋄Significant difference in normalized angular displacement between DO and GL specimens (P < .05).
The DO group exhibited significantly greater UTJ gapping compared with its native state at 3 N·m (1.59 ± 0.3 mm [DO] vs 0.64 ± 0.2 mm [Native], P = .009) and at ultimate failure (10.08 ± 2.5 mm [DO] vs 3.1 ± 0.4 mm [Native], P = .004). The GL group had significantly greater UTJ gapping at ultimate failure (8.21 ± 2.8 mm [GL] vs 3.6 ± 1.2 mm [Native], P = .004) but not at 3 N·m (1.32 ± 0.5 mm [GL] vs 0.99 ± 0.5 mm [Native], P = .065) (Figure 8). The DO group had significantly greater normalized UTJ gapping compared with the GL group at 3 N·m (2.63-fold ± 0.9 [DO] vs 1.55-fold ± 0.6 [GL], P = .037) and at ultimate failure (3.28-fold ± 0.8 [DO] vs 2.41 ± 0.8 [GL], P = .043).
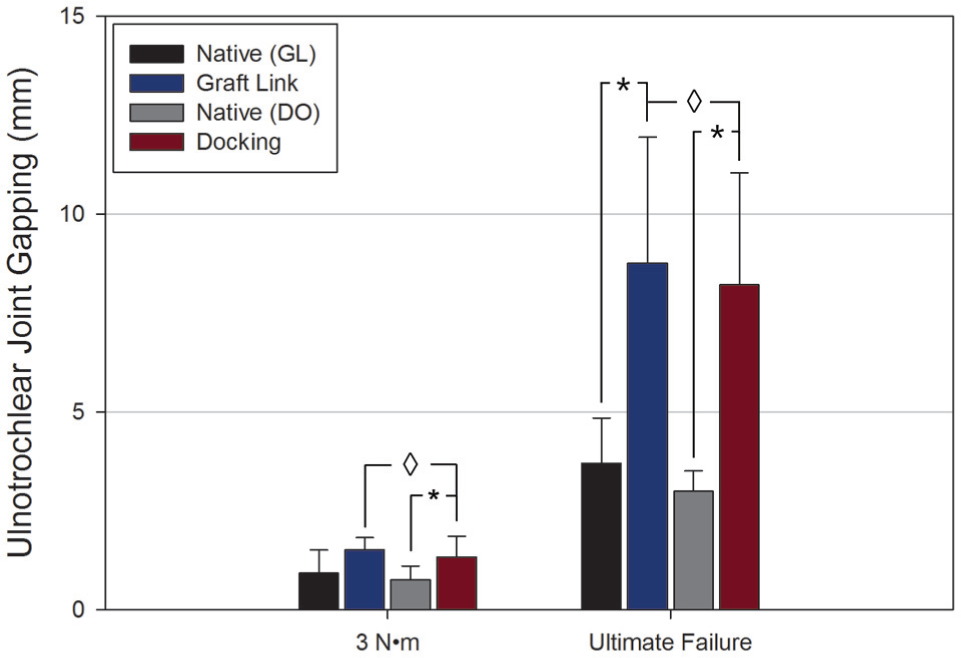
Quantitative ulnotrochlear joint (UTJ) gapping analyzed at 3 N·m and at ultimate failure during failure testing. Compared with the native specimens, both the GraftLink (GL) and docking (DO) techniques exhibited significantly greater UTJ gapping at failure, but only DO showed greater UTJ gapping at 3 N·m of loading. The DO technique exhibited significantly greater normalized UTJ gapping compared with the GL at 3 N·m and at ultimate failure. *Significant difference between native and reconstructed state (P < .05). ⋄Significant difference in normalized angular displacement between DO and GL specimens (P < .05).
Failure Modes
The failure modes differed greatly between the DO and GL reconstructions. The primary mode of failure in the DO group was at the tendon-suture interface at the humeral side. The suture tightened around and cut through the tendon graft, causing elongation, a loss of stiffness, and ultimate failure. This occurred in 5 DO specimens. One DO specimen exhibited a fracture of the bony bridge between the 2 ulnar bone tunnels on the sublime tubercle, a failure mode previously described in clinical studies.4,21 One DO specimen exhibited failure in the tendon graft, in which intersubstance tearing was noted. The GL group exhibited a larger variety of failure modes. Three specimens exhibited a fracture of the sublime tubercle, oriented perpendicular to the long axis of the ulna, propagating in the axial plane. The fractures all had articular involvement, and the graft, sutures, and TightRopes remained intact. The fracture consistently originated in the ulnar graft socket and appeared to split the socket in half. Upon further analysis, it was determined that this fracture was caused by the lever action that the graft caused onto the sublime tubercle. The sharp angle between the ulnar socket and the inserting graft (estimated at 80°-100°) caused the elongating graft to apply a tension onto the graft socket, causing tensile failure of the bone and fracture elongation into the articular surface. One GL specimen failed at the suture-tendon interface at the humeral side. One GL specimen failed by midsubstance tearing of the graft. One GL specimen failed at the tendon-tendon interface, where the 2 free limbs of the graft are sutured together. Last, in 1 GL specimen, the humeral cortical button was pulled through the bone, causing elongation of the graft and ultimate failure. Upon further inspection, it was noted that the reconstruction was completely intact and that all elongation was caused by the button pulling through the bone.
Discussion
The evolution of UCL reconstruction has enabled even elite throwing athletes to return to activity after injury. 21 Biomechanical studies are used to assess the immediate postoperative strength of surgical techniques, and studies assessing UCL reconstruction biomechanics are widespread. The GraftLink UCL reconstruction is a new technique that uses a TightRope on both the humeral and the ulnar side. The use of cortical buttons and suture loops eliminates the need for interference screws, which are popular implants to improve fixation in UCL reconstruction1,2,8,15,17 but have also been shown to cause mechanical damage to the graft2,11,18 and to displace the graft to one side of the tunnel, 29 which could limit the soft tissue-to-bone area necessary for healing. The clinical effects of these observations from laboratory studies remain to be fully elucidated. Furthermore, interference screws have been implicated as a potential cause of stress risers and increased risk for fracture, 30 but this has not been shown in the context of UCL reconstruction. The communicating ulnar bone tunnels in the popular docking technique have been shown to fracture in both clinical4,21 and laboratory studies,7,12,15 and the GraftLink technique eliminates the risk of this type of fracture. A potential disadvantage of the GraftLink technique is the fact that by placing the reconstruction at the footprint of the anterior bundle, the reconstruction is addressing mainly the stability afforded by the anterior bundle, whereas the docking technique is feasibly recreating more of the fan-shaped native UCL structure, although this remains unclear. In addition, a disadvantage of the GL may be hardware-related complications, such as the cortical button fracture, which are absent in the DO technique, and/or symptoms due to potential prominence of the cortical buttons. The GL also requires greater precision in graft length preparation compared with the DO. Furthermore, our tests showed that the GraftLink group exhibited fractures through the ulnar graft socket, propagating in the axial plane and involving the articular surface. This happened in 3 GL specimens, and we conclude that the angle with which the graft inserts into the tunnel causes a stress of a magnitude sufficient to cause tensile failure of the bone through the socket during internal rotation of the humerus. Interestingly, the reconstruction was completely intact in all 3 specimens, indicating that the cadaveric bone was the weakest component in these constructs, and it is not clear whether this type of fracture would happen in healthy bone in the clinical setting. Future studies are necessary to investigate whether altering the angle between the graft and the socket could reduce this stress by reducing the transfer of force from the graft onto the most proximal sublime tubercle.
Results from our study demonstrate that both the DO and GL techniques restore joint kinematics under low loading in a range of flexion angles between 15° and 90° and that there is no difference in kinematics between the DO and GL techniques. Our hypothesis that the GL technique offered a stiffer reconstruction was disproved because the DO and GL had equivalent stiffness. The hypothesis that the GL technique was less lax was confirmed, however, because the GL technique exhibited significantly lower normalized angular displacement at failure and significantly lower normalized UTJ gapping at both 3 N·m and ultimate failure compared with the DO technique. The torque at failure was significantly lower in the GL group compared with its native state, but this was not the case in the DO group. This indicates that the DO technique fails at higher torques, even though there was no significant difference in the normalized failure torque between the 2 groups. Although the DO is more lax and exhibits more UTJ gapping at failure than does the GL, it is difficult to conclude whether there is a benefit of the high-torque failure.
Our study used a testing model that entailed application of torsional loading or angular displacement to the humerus rather than application of an axial force to the distal forearm. First used by Ruland et al, 25 this torsional model offers a more anatomic way of loading the UCL, and other studies have used this principle.7,13 Comparisons of our data with those of previous studies should be limited if the previous studies did not use a torsional testing model. Ruland et al used a testing fixture and protocol most similar to ours, and they noted native UCL failure at 21.43 N·m, similar to our native mean 24.06-N·m failure torque. Ciccotti et al 7 also used a torsional-loading model and noted native UCL failures at 14.9 N·m, a much lower value than the 24.06-N·m mean failure torque in our study. This difference could be explained by the much higher cadaver age of 79.2 years in Cicotti’s study versus our mean cadaver age of 56.4 years. Furthermore, Cicotti et al used 5-N·m preconditioning cycles (~33% of ultimate failure), which could have led to fatigue loading of the UCL and a resultant lower failure torque. Lee et al 16 applied a uniaxial load to the distal forearm to create a valgus stress in the elbow and calculated a 24.6-N·m failure torque of the intact UCL, a value very similar to our data. The mean torsional stiffness of the native UCL in our study (80.13 N·m/rad) is lower than previously reported native torsional stiffness. Lee and coworkers found native stiffness of 137.5 N·m/rad, and Ruland et al noted 114.59 N·m/rad. Cicotti et al did not assess torsional stiffness. We attribute this to differences in testing protocols such as the flexion angle and/or preconditioning/preloading. Ruland and colleagues tested all specimens in 90° of flexion, which can cause a higher torsional stiffness attributable to tighter fibers in the anterior bundle at that flexion angle. Lee et al tested their specimens at 70° of flexion, but their kinematic testing protocol did not use numerous loading-unloading cycles, which could have fatigued native UCLs in our study, causing decreased stiffness during failure testing. Ruland and coworkers, who studied a variety of reconstructions, noted that failure torques ranged from ~12 to 20 N·m, values that are comparable to our mean DO and GL failure torques of 16.79 N·m and 17.40 N·m, respectively. Additionally, in Ruland’s work, stiffness ranged from 35.5 to 49.2 N·m/rad, also comparable to our DO and GL stiffness of 41.59 N·m/rad and 50.73 N·m/rad, respectively. Interestingly, Lee et al noted a lower failure torque (10.3 N·m) but higher stiffness (63.02 N·m/rad) compared with our data. The difference in failure torque can be attributed to the nature of Lee and colleagues’ revision reconstruction technique, in which they simulated extensive ulnar bone loss to assess a revision technique that could, inherently, have inferior mechanical strength. We tensioned our grafts at 30° of flexion, consistent with the surgical description of the docking technique 24 and with the protocols of other studies,3,7,12,15,21 and we kept this method consistent in the GL reconstructions. We then tested all specimens at 70° of flexion, consistent with previous studies that assessed UCL reconstruction biomechanics.12,15,19 Ruland et al tensioned their reconstructions at 90° and tested at 90°, and Lee et al both tensioned and tested their grafts in 70° of flexion, which can explain small differences in results between their data and ours. No consensus exists regarding the optimal tensioning and testing combination. Studies assessing native elbow kinematics have demonstrated that valgus stability increases with increasing flexion angle.6,10,32 Tying the reconstruction at a low flexion angle could cause excessive strain in the reconstruction at higher flexion angles, which may lead to early failures; conversely, tying the reconstruction at high flexion angles could cause insufficient stability at low flexion angles, where the reconstruction may be too lax. Future studies are necessary to elucidate how tying and tensioning UCL reconstructions at various flexion angles affect overall joint kinematics.
We used video analysis software to track the relative motion of 2 markers placed anterior to the native UCL or the reconstruction graft to derive quantitative ulnotrochlear joint gapping. This method is similar to the methods of previous studies that used video tracking to quantify UTJ gapping. 2 In our data, native specimens exhibited a mean 3.4 mm of UTJ gapping at ultimate failure, whereas the DO and GL groups exhibited 8.75 mm and 8.2 mm, respectively. Limited published data exist with which to compare these results. Armstrong et al 2 used 5 mm of joint gapping as an indicator of failure, at which they compared the mean force of each reconstruction type in a testing model in which uniaxial force is applied to the forearm. Because of differences in testing and analysis methods, it is difficult to compare the results of their study to our data. Hurbanek and coworkers 12 used differential variable reluctance transducers to quantify UTJ gapping. They analyzed the moment at 3 mm of UTJ gap formation, which they noted can be used as an indicator of clinical failure. Gapping at the UTJ is an important variable to assess during both biomechanical testing and clinical evaluations. Although UTJ gapping is an important surgical aspect of UCL reconstruction, no clinical study has delineated whether such gapping is fully reduced after UCL reconstruction. Therefore, it is unknown whether the outcomes of UCL reconstruction are primarily attributable to pain relief or whether the UTJ gap is restored to native values even after several postoperative years. More research is necessary to properly relate quantitative UTJ gapping from biomechanics studies to the clinical scenario.
Results from our study should be interpreted in the context of limitations inherent to cadaveric biomechanics and specific study protocols. We used cadavers with a mean age of ~56 years, much older than the typical patient undergoing UCL reconstruction. Because it is very difficult to obtain young cadaveric specimens, using middle- and old-aged cadavers is common practice in orthopaedic biomechanics; the use of matched pairs, internal controls, and repeated-measures statistics enables accurate comparison of a reconstruction technique to a native ligament or other reconstruction techniques, and we used all these strategies. Furthermore, we did not perform bone densitometry measurements on any specimens to assess osteoporosis. However, we took steps to ensure that our specimens were free of musculoskeletal disorders by reviewing pertinent medical and surgical history of each donor. Additionally, there were no significant differences in any assessed variable among native specimens, reaffirming that we used a consistent specimen population. Since the palmaris longus tendon can be absent in as much as 20% of the population, 27 and given that extensive variability in size and quality could result in measurable variability in biomechanical strength, we chose to use fresh-frozen bovine extensor tendons as tendon grafts in this investigation. Our experiments comparing the suture pull-out properties of PL and BE tendons demonstrated equivocal biomechanical properties, but the results exhibited high variability. Lack of significant differences could, thus, be due to low sample size, and subsequent studies assessing differences between PL and BE grafts are merited. We used angular displacement of the humerus caused by an applied torque to the humerus as the primary measure of elbow laxity during kinematic testing. While our testing apparatus enables semidynamic adjustment of elbow flexion and accounts for the elbow carrying angle, true kinematics could be better assessed with the use of a dynamic elbow simulator. Furthermore, elbow kinematics before and after reconstruction may be more accurately assessed with 3D motion analysis systems to track relative motions of bony landmarks.
This study assessed immediate postoperative kinematics and failure strength of the traditional bone tunnels used in the docking technique and the new GraftLink technique. Our results demonstrate that (1) both techniques restore kinematics to a state that is similar to that of the native UCL; (2) the GraftLink technique exhibited lower failure torque than its native control, whereas the docking technique did not, indicating that the DO fails at higher torque; and (3) the docking technique exhibited greater laxity and UTJ gapping. Cyclic testing, failure testing at numerous loading rates, and kinematic testing using an elbow simulator could further elucidate similarities and differences between these and other UCL reconstruction techniques, and such future studies are merited. From the data presented in this report, we conclude that the GraftLink technique is a reasonable option for surgeons who prefer to place the graft within the footprint of the native UCL but would like to avoid interference screw fixation.
Footnotes
Acknowledgements
The authors acknowledge Arthrex Inc for the donation of cadaveric specimens and surgical materials, supplies, and medical illustrations.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.A. receives consulting fees and research support from Arthrex Inc. A small unrestricted academic grant, surgical supplies and materials, and cadaveric specimens for this study were provided by Arthrex Inc.