
Abstract
Background:
Researchers have suggested that there are sex differences in outcomes after sport-related concussions. Factors such as sport type/rules, age, and body mass index (BMI) may influence these differences.
Hypotheses/Purpose:
The purposes of this study were (1) to examine neurocognitive performance after concussions between male and female soccer players and (2) to compare concussion symptoms between male and female soccer players. We hypothesized that female concussed soccer players would report more concussion symptoms and worse cognitive performance compared with male concussed soccer players.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 39 male (mean BMI, 22.21 ± 2.34 kg/m2; mean age, 17.69 ± 2.10 years) and 56 female (mean BMI, 23.47 ± 2.66 kg/m2; mean age, 17.78 ± 2.30 years) concussed soccer players participated in this study. Participants were similar in age, history of concussion, sport, and time since injury. Participants completed computerized neurocognitive tests and symptom reports at baseline and 8 days after injury. Body mass index served as a covariate in all analyses.
Results:
After adjusting for BMI, results from a repeated-measures analysis of covariance (ANCOVA) revealed a group by time interaction for visual memory (F1,82 = 5.50; P = .021). Specifically, female concussed soccer players (mean score, 68.7 ± 15.2) performed worse at 8 days after a concussion compared with male concussed athletes (mean score, 77.2 ± 8.9). Results of another ANCOVA for total concussion symptoms indicated an interaction for group by time (F1,82 = 4.26; P = .04). Specifically, female concussed soccer players (mean score, 11.9 ± 15.7) reported more total concussion symptoms at 8 days compared with male concussed athletes (mean score, 5.3 ± 7.4). There were significant main effects for sex on verbal (F1,82 = 5.98; P = .017) and visual (F1,82 = 4.65; P = .034) memory, with female athletes reporting lower scores than male athletes. Female athletes also reported more symptoms on the migraine-cognitive-fatigue (F1,82 = 10.8; P = .001) and sleep (F1,82 = 9.2; P = .003) clusters than male athletes.
Conclusion:
In contrast to recent studies, after controlling for BMI, female athletes exhibited lower performance on visual memory composite scores and higher scores on total symptoms than male athletes after concussions.
Recently, researchers have suggested that sex differences on concussion outcomes may exist in concussed male and female athletes.4,5,7,8,11 Specifically, female concussed athletes have been reported to have greater neurocognitive impairments on reaction time and visual memory and increased symptoms when compared with male concussed athletes.4,5 However, the majority of these studies have compared male athletes predominantly participating in football with female athletes participating in soccer and basketball. Comparing sexes across these sports is an inherent methodological weakness because of the lack of female participation in football. Moreover, the mechanism of a concussive injury (ie, velocity of collision, involvement of helmets/head protection), sport environment (ie, field size, speed of play/contact), and rules in male sports are different compared with female sports. These differences confound current research that examines sex differences on concussion outcomes. Thus, additional studies examining concussion outcomes between male and female athletes who play the same sport (ie, soccer and basketball) are warranted.
Numerous studies have supported sex differences in neurocognitive performance after concussions.4,5,7,8 Recently, Covassin and colleagues 8 reported that female concussed athletes performed significantly worse on visual memory compared with male concussed athletes. Broshek et al 4 reported that female concussed athletes were 1.7 times more cognitively impaired and demonstrated slower reaction times compared with male concussed athletes. In recognizing the threat to their study’s internal validity by comparing male and female athletes in different sports, Broshek and colleagues 4 excluded athletes who participated in sports that involved protective equipment (ie, football helmet) in their analyses and only included male and female athletes who did not participate in collision sports. In concordance with other research, 6 Broshek et al 4 reported that 57% of concussed female athletes demonstrated at least 1 reliable change (see Iverson et al 14 for reliable change index) in neurocognitive performance compared with only 27% of male concussed athletes. However, Broshek et al 4 included athletes competing in multiple sports (ie, football, basketball, lacrosse, soccer, cheerleading), which is a weakness in their study. In 1 of 2 studies that compared athletes participating in a sport with similar rules and conditions (ie, soccer), Colvin and colleagues 5 reported worse neurocognitive performance in female concussed soccer athletes compared with male concussed soccer athletes. These results should be interpreted with caution, as Colvin et al 5 did not control for a history of concussion. However, they did discuss the role of body mass index (BMI) on concussion outcomes. Specifically, they speculated that a lower BMI may reflect lower neck strength, thereby potentially underlying reported sex differences. In support of this assertion, Schulz et al 21 reported that a lower BMI was associated with an increased risk of concussion. Furthermore, female athletes tend to have weaker neck muscles (as measured by isometric cervical flexor and extensor strength) than male athletes.16,22 Several studies have shown that stronger and larger neck muscles result in lower head acceleration, given a similar impact force to the head, as the active and passive muscle forces provide more resistance and inhibit head movement response.23,24 Surprisingly, to our knowledge, researchers have not examined BMI in regard to sex differences since the Schulz et al 21 study. More recently, Zuckerman and colleagues 25 compared male and female soccer players and did not report any significant neurocognitive or symptom differences between the sexes. However, they did not control for BMI as indicated by Colvin et al 5 and Schulz et al. 21 In conclusion, there is still debate on whether male and female concussed athletes differ on concussion outcomes.
Previous researchers have stated that male and female athletes report different symptoms after concussions.5,7,11 Concussed male athletes report more amnesia and confusion/disorientation, while concussed female athletes report more drowsiness and increased sensitivity to noise. 11 Other researchers reported that female concussed athletes exhibited greater total concussion symptoms5,7 and poor concentration, seeing stars, increased fatigue, and lightheadedness 4 compared with male concussed athletes. Recently, Frommer and colleagues 11 reported that male high school athletes had more cognitive symptoms and that female high school athletes had more neurobehavioral and somatic symptoms after concussions. Although these studies depict the varying symptoms among male and female athletes, none of these studies exclusively examined male and female athletes playing the same sport.
Concussions have been reported to constitute 2% to 22% of all soccer injuries.1,3,9,12,13,17 Soccer is the only sport that allows for players to intentionally use their head to pass or shoot the ball. Concussions in soccer can occur from direct or indirect impact with the ground or goalpost or head-to-head or ball-to-head contact.1,9 Unlike the majority of high-risk sports for concussions (eg, football, ice hockey), the similar styles of play and uniform rules of the male and female soccer game make this sport ideal for concussion research that examines sex differences on concussion outcomes. Recently, Zuckerman and colleagues 25 matched 40 female and male concussed soccer players on learning disability, attention deficit disorder/attention deficit hyperactivity disorder (ADHD), special education, age, and time of test date. Postconcussion tests were administered at a mean 7.2 ± 6.4 and 5.4 ± 4.4 days from injury for female and male soccer athletes, respectively. Results of their study indicated that there were no sex differences on baseline or postconcussion neuropsychological test scores. This finding is in contrast to the results of other researchers who have reported sex differences in concussion outcomes.4,5,7 The purpose of the current study was to replicate the study of Zuckerman and colleagues 25 using male and female concussed soccer athletes while controlling for BMI. The specific aims of this study were (1) to examine neurocognitive performance after concussions between male and female soccer players and (2) to compare concussion symptoms between male and female concussed soccer players. We hypothesized that female concussed soccer players would report more concussion symptoms and worse cognitive performance compared with male concussed soccer players.
Materials and Methods
Participants
There were a total of 39 male (height, 70.50 ± 2.73 inches; weight, 167.12 ± 28.30 pounds; BMI, 22.21 ± 2.34 kg/m2; age, 17.69 ± 2.10 years) and 56 female (height, 63.20 ± 13.10 inches; weight, 120.10 ± 34.70 pounds; BMI, 23.47 ± 2.66 kg/m2; age, 17.78 ± 2.30 years) high school and collegiate concussed soccer players participating in this study. Athletes were part of an ongoing Mid-Michigan sport concussion program. The Mid-Michigan sport concussion program has been ongoing for the past 5 years, encompassing numerous high schools and universities. Any athlete who incurs a concussion is asked to volunteer for the study. To date, the program includes over 400 athletes in the Mid-Michigan area who have incurred a concussion. Athletes who had a learning disability, history of brain surgery, ADD/ADHD, color blindness, or history of chronic migraine headaches were excluded from this study.
Operational Definition of Concussion
A concussion was operationally defined as “a complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces.”2,18,19 All concussions were required to meet the following diagnostic criteria: (1) the presence of on-the-field signs (eg, posttraumatic amnesia, loss of consciousness) and symptoms (eg, dizziness, headache) as determined by a certified athletic trainer or team physician and (2) a decrease from baseline levels in at least 1 postconcussion neurocognitive score determined by reliable change estimates. 14
Neurocognitive Function
To determine an athlete’s neurocognitive function, the Immediate Post-concussion Assessment and Cognitive Test (ImPACT) battery was used for this study. The ImPACT neurocognitive battery consists of a demographic section, a list of 22 concussion symptoms that are self-reported using a 7-point Likert scale, and 6 neurocognitive test modules that evaluate the participants’ attention process, visual working memory, verbal recognition memory, visual processing speed, reaction time, numerical sequencing ability, and learning. The ImPACT yields composite scores for verbal memory, visual memory, motor processing speed, and reaction time. A higher score by the athlete on verbal and visual memory and motor processing speed indicates better performance. Verbal and visual memory scores are presented as a percentage of 100 and processing speed as a number composite score. A lower score on reaction time indicates better performance. Sensitivity (the likelihood that the test result will be positive when a concussion is present) of the ImPACT has been established at 81.9%, and specificity (the likelihood that the test result will be negative when a concussion is not present) has been established at 89.4%. 20
Body Mass Index
Body mass index was calculated using the following formula: BMI = mass (kg)/height (m2). Mass was self-reported by the athletes in pounds and converted to kilograms. Height was self-reported in feet and inches and then converted to meters.
Procedures
The study was approved by the university’s institutional review board before enrolling any participants. Informed parental consent and child assent were obtained for all minors, while consent was obtained from all athletes aged ≥18 years. All athletes were informed of the testing procedures and then were administered a baseline computerized neurocognitive test before the start of their soccer season. All concussed athletes were administered the computerized neurocognitive test approximately 8 days (male: mean, 7.68 ± 3.20 days; range, 2-19 days; female: mean, 8.64 ± 3.70 days; range, 3-17 days) after a concussion.
Data Analysis
Data were analyzed using descriptive and inferential statistics. Separate independent t tests were conducted to evaluate differences in age, days since injury, and history of concussion between male and female concussed athletes. Separate repeated-measures (baseline, 8 days) multiple analyses of covariance (ANCOVAs) were performed on verbal and visual memory, motor processing speed, and reaction time composite scores. The covariate was BMI to control for differences in height and weight between male and female soccer players. Post hoc univariate tests were performed to determine which composite scores were significant.
For the concussion symptoms, a series of repeated-measures (baseline, 8 days) ANCOVAs was performed on total symptom scores and 4 symptom clusters (cognitive-migraine-fatigue, affective, somatic, sleep), 15 with sex as the between-group factor. 15 The cognitive-migraine-fatigue cluster includes headache, dizziness, fatigue, drowsiness, sensitivity to light/noise, feeling slowed down, and difficulty remembering/concentrating. The affective symptom cluster includes sadness, nervousness, and feeling more emotional. The somatic cluster includes vomiting and numbness/tingling. Finally, the sleep cluster includes trouble falling asleep and sleeping less than usual. A Bonferroni confidence interval adjustment was applied to both analyses to correct for multiple comparisons. The level of significance was set at an uncorrected P = .05. All analyses were conducted using the Statistical Package for the Social Sciences version 19.1 (SPSS, IBM, Armonk, New York).
Results
Independent t tests revealed that there were no significant differences in age (t = 0.652; P = .652), days since injury (t = 1.34; P = .182), or concussion history (t = 0.911; P = .365) between male and female concussed soccer players. Consequently, these variables were not used as covariates. Results of an independent t test indicated that BMI was significantly different between male and female athletes (t = 2.70; P = .008). Consequently, and per the reported differences associated with this variable, BMI was used as a covariate in the analyses.
Computerized Neurocognitive Performance for Male and Female Concussed Athletes
After adjusting for the covariate (BMI), results from the repeated-measures ANCOVAs with Bonferroni correction revealed a significant group by time interaction for visual memory (F1,82 = 5.50; P = .021) (Table 1). Specifically, female concussed soccer players (mean score, 68.7 ± 15.2) performed worse at 8 days after a concussion compared with male concussed athletes (mean score, 77.2 ± 8.9). There was a significant between-patient main effect for sex on verbal memory (F1,82 = 5.98; P = .017); however, there was no significant interaction for time by group on verbal memory (F1,82 = 0.610; P = .437). There was also a significant between-patient main effect for visual memory (F1,82 = 4.65; P = .034). Overall, both between-patient main effects for sex indicated that female athletes scored lower than male athletes when combining both baseline and 8-day posttest scores together. There were no significant sex by time interactions for motor processing speed (F1,82 = 1.37; P = .24) or reaction time (F1,82 = 3.43; P = .069). There were also no significant between-group differences on motor processing speed (F1,82 = 0.39; P = .54) or reaction time (F1,82 = 1.95; P = .169).
Performance Scores on Verbal Memory, Visual Memory, Motor Processing Speed, and Reaction Time for Concussed Male and Female Soccer Athletes a
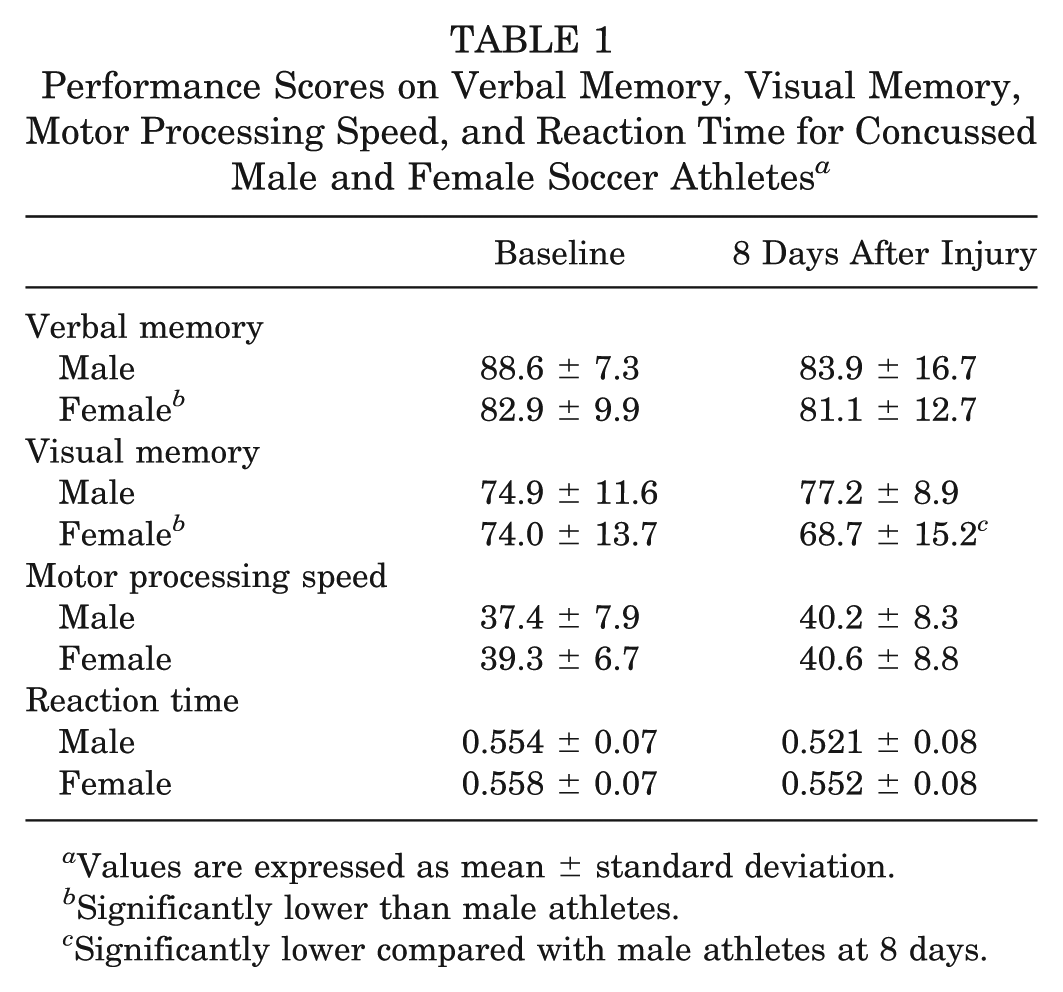
Values are expressed as mean ± standard deviation.
Significantly lower than male athletes.
Significantly lower compared with male athletes at 8 days.
Postconcussion Symptoms for Male and Female Concussed Athletes
After adjusting for the covariate (BMI), results of the ANCOVA for total concussion symptoms indicated a significant interaction for group by time (F1,82 = 4.26; P = .04) and a main effect for sex (F1,82 = 9.12; P = .003). Specifically, female concussed soccer players (mean score, 11.9 ± 15.7) reported a greater number of total concussion symptoms at 8 days after a concussion compared with male concussed athletes (mean score, 5.3 ± 7.4) (Table 2). There were no significant interactions between group and time for the symptom clusters of migraine-cognitive-fatigue (F1,82 = 1.50; P = .22), affective (F1,82 = 0.117; P = .73), somatic (F1,82 = 3.40; P = .06), and sleep (F1,82 = 0.001; P = .98). However, there were significant main effects for sex on the sleep cluster (F1,82 = 9.2; P = .003) and migraine-cognitive-fatigue cluster (F1,82 = 10.8; P = .001). There were no significant main effects for sex on the affective (F1,82 = 0.015; P = .90) and somatic (F1,82 = 3.40; P = .068) clusters.
Total Symptom, Migraine-Cognitive-Fatigue, Affective, Somatic, and Sleep Clusters for Concussed Male and Female Soccer Athletes a
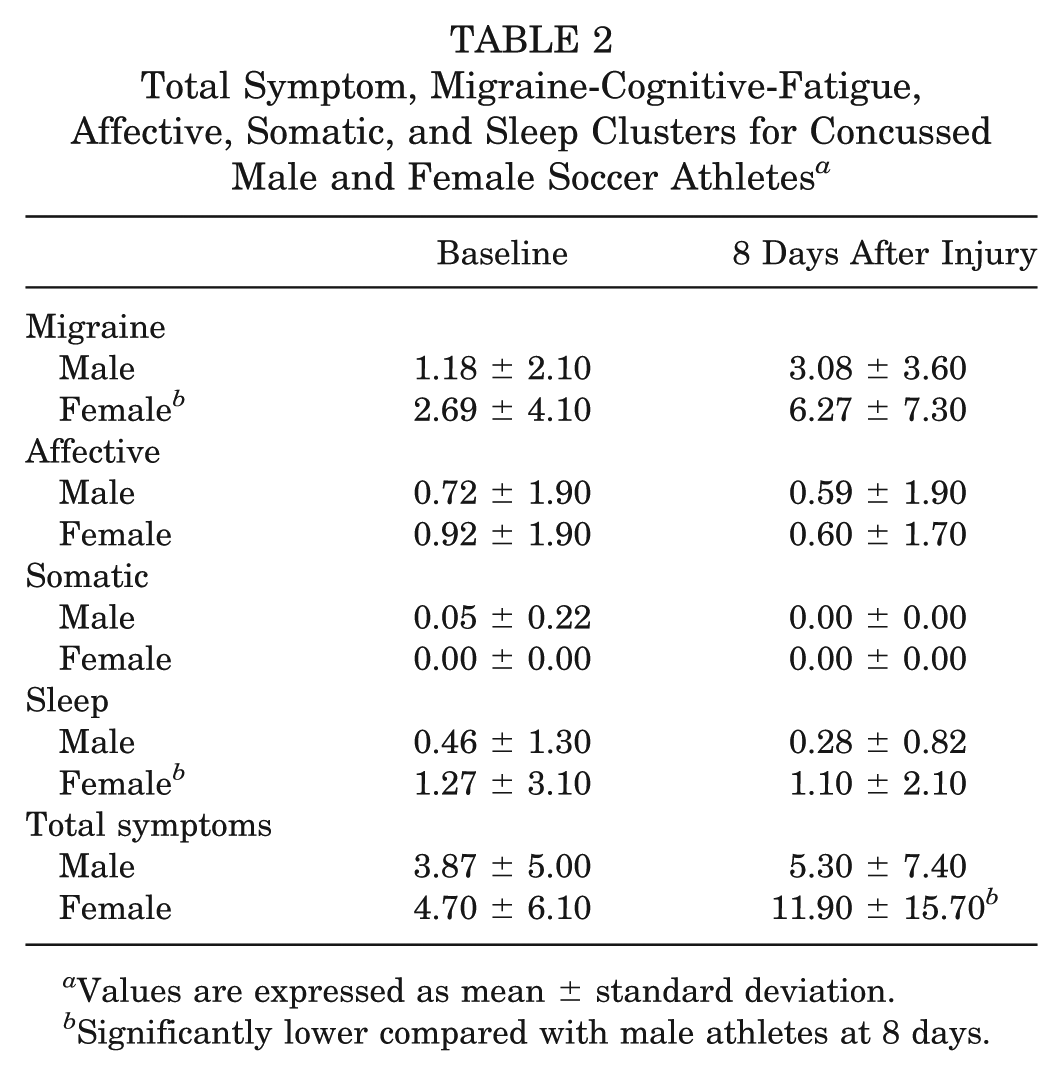
Values are expressed as mean ± standard deviation.
Significantly lower compared with male athletes at 8 days.
Discussion
Overall, this study demonstrated partial support for sex differences in male and female concussed soccer athletes. Specifically, female concussed soccer athletes scored lower on visual memory compared with male concussed soccer athletes at 8 days after a concussion. Female concussed athletes also had a significantly greater number of total postconcussion symptoms than male concussed athletes. Although there were no significant interactions for sex by time, there were between-sex differences on verbal memory, visual memory, the sleep cluster, and the migraine-cognitive-fatigue cluster. Specifically, female athletes scored lower on memory and higher on symptoms than male athletes.
Previous researchers have reported various sex differences on cognitive performance after a concussion.4,5,7,8 While other researchers reported similar findings to ours with regard to cognitive impairments in visual memory, our results are in contrast to those of a recently published study by Zuckerman and colleagues. 25 Using the same neurocognitive measure as the current study (ie, ImPACT), Zuckerman and colleagues 25 did not report any differences in postconcussion neurocognitive performance between male and female soccer athletes. Although the current study and that by Zuckerman et al 25 both controlled for sport type, age, time to postconcussion test, and concussion history, only the current study controlled for BMI. This finding suggests that BMI may play a role in mitigating any reported sex difference in outcomes related to concussions, as noted by Schulz et al. 21 However, more research examining the role of BMI and neck strength on sex differences in concussion outcomes is needed to confirm the current study’s findings. Another potential reason for the difference between the current study and that of Zuckerman et al 25 may be the age differences of the participants in the 2 studies. Participants in the current study were on average 18 years old, whereas participants in the study of Zuckerman et al 25 were slightly younger than 16 years old. Thus, it may be plausible that sex differences on postconcussion neurocognitive and symptom outcomes are more pronounced with age. One explanation for this age-related difference is that disparities in neck strength between male and female athletes become more substantial later in high school and in college than they are early in high school. Similarly, the nature of concussions in soccer at slightly older and more skilled levels may be more significant compared with those at younger and less skilled levels.
The findings from the current study indicated that female concussed soccer athletes self-reported more total concussion symptoms at 8 days after a concussion than do male concussed soccer athletes. These findings are similar to those of other researchers who also reported that female athletes had more total concussion symptoms compared with male athletes.4,5 However, the current findings are in contrast to those of Frommer and colleagues, 11 who described that male concussed athletes reported more amnesia, confusion, and disorientation after a concussion, although it is unclear when the concussed athletes in their study were tested for postconcussion symptoms. The current study was one of the first to examine sex differences on the revised concussion symptom factors. 15 Our study did not find sex differences for any of the symptom clusters across time. This finding suggests that although female athletes report more total concussion symptoms than do male athletes, there are no specific symptom clusters in which they differ across time. This finding is somewhat surprising given the speculation that female athletes report higher levels of affective and migraine symptoms than male athletes. However, the between-group differences in the current study suggest that female athletes do in fact report higher levels of these types of symptoms but that these differences do not relate to change across postinjury time intervals. Further examination of sex differences in symptom clusters is warranted.
Results from this study may encourage sports medicine clinicians to be more cautious when allowing female concussed soccer athletes to return to participation. Moreover, health care professionals need to be aware that female athletes could report more total concussion symptoms compared with male concussed athletes. While sex differences may exist in symptoms, clinicians treating a concussed athlete should tailor the treatment to the specific symptoms reported by the injured athlete, despite the empirically supported differences between the sexes. Finally, clinicians need to consider that neurocognitive assessment measures that take sex differences into account reduce the risk of misinterpreting neurocognitive data on the basis of sex bias norms within the clinical setting.
There are limitations of the current study that need mentioning. First, this research was limited to a small sample size, thereby limiting the external validity and generalizability of the results to other age ranges (ie, youth and adult soccer players). These specific age groups have been found to differ on neurocognitive outcomes after concussions, 10 and these differences may influence the current results. Symptom data and BMI were self-reported by athletes and may reflect biases associated with self-reported measures. We assumed that participants completed the neurocognitive tests with full effort; however, we did not assess effort during these tests. We did not obtain data about return to participation. As a result, it is unclear how long the athletes in the current study took to recover from their concussion. In addition, we only used symptom reports, neurocognitive test scores, and clinical examination findings to determine a concussion. We did not include balance testing and imaging, which are also suggested for the management of a concussion. Finally, only high school and collegiate soccer athletes from the Mid-Michigan area were included in this study, thereby limiting the generalizability of the current findings to other geographical locations.
Conclusion
In the current study, female concussed soccer players exhibited lower performance on visual memory composite scores compared with male concussed soccer players. In addition, female athletes also reported a greater number of total symptoms after concussions than male athletes. Although we controlled for BMI and used a sport with similar rules, more research is needed before we can draw any definitive conclusions on sex differences and concussion outcomes.
Footnotes
Acknowledgements
The authors thank all the certified athletic trainers for their contributions to this study.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.