
Abstract
Background:
Knee arthroscopies are among the most common procedures performed by orthopaedic surgeons, yet little is known about the associated complications and complication rates.
Purpose:
To examine the nature and frequency of complications after the most common arthroscopic knee procedures, with particular attention to fellowship training, geographic location of practice, and age and sex of the patient.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Data were obtained from the American Board of Orthopaedic Surgery database for orthopaedic surgeons who sat for the part II examination from 2003 to 2009. The database was queried to determine the type and frequency of complications for patients who underwent knee arthroscopy and for those who underwent sports medicine knee arthroscopy, including arthroscopic partial meniscectomy, meniscal repair, chondroplasty, microfracture, anterior cruciate ligament reconstruction, or posterior cruciate ligament reconstruction. Factors affecting complication rates that were investigated included type of procedure, fellowship training status, geographic location of practice, and age and sex of the patient.
Results:
There were 4305 complications out of 92,565 knee arthroscopic procedures obtained from the American Board of Orthopaedic Surgery database for an overall candidate-reported complication rate of 4.7%. The complication rates were highest for posterior cruciate ligament reconstruction (20.1%) and anterior cruciate ligament reconstruction (9.0%); complication rates for meniscectomy, meniscal repair, and chondroplasty were 2.8%, 7.6%, and 3.6%, respectively. The complication rate for sports fellowship–trained candidates was higher than for non–sports trained candidates (5.1% sports, 4.1% no sports; P < .0001) and for male patients (4.9% male vs 4.3% female; P < .0001). Younger patients (<40 years; 6.2%) had a higher complication rate than older patients (≥40 years; 3.58%) (P < .0001). Procedure complexity is a likely confounding factor affecting sports-trained candidates and younger patients. There were no geographic differences (P = .125). The overall rate of pulmonary embolus was 0.11%. Surgical complications (3.68%) were more common than medical (0.77%) or anesthetic complications (0.22%), and infection was the most common complication overall (0.84%).
Conclusion:
The overall self-reported complication rate for arthroscopic knee procedures was 4.7%. Knee arthroscopy is not a benign procedure, and patients should be aware of the risk of complications.
Arthroscopic knee surgeries are among the most common orthopaedic procedures, accounting for 3 of the 10 most common orthopaedic procedures, and arthroscopic meniscectomy is the most commonly performed orthopaedic surgery in the United States. 3 The number of arthroscopic knee procedures continues to increase and increased 46% from 1996 to 2006. 7 Despite the frequency of these procedures, little is known about the associated complication rates.
To our knowledge, the only published studies on complication rates of arthroscopic knee surgery in the past 2 decades are from outside the United States.6,10 Much of the information regarding arthroscopic knee surgical complication rates dates back to the 1980s, with rates ranging from 0.8% to 8.2%.1,12-14 There have been many recent changes that may have dramatically altered complication rates, including changes in equipment, technique, frequency of surgery, complexity of arthroscopic procedures, and the shift from inpatient to outpatient procedures.
Accurate estimates of complications are important for informed consent, a surgeon’s personal evaluation and improvement, defining standards for performance-based initiatives, payment for “never events” (certain payers’ refusal to reimburse for the treatment of certain complications), and defining reimbursement in capitated systems. The purpose of this study was to examine the nature and frequency of complications of the most common arthroscopic knee procedures and to determine the effects of type of procedure, fellowship training, geographic location of practice, and age and sex of the patient on complications associated with knee arthroscopy.
Materials and Methods
Data Collection
All cases and complications from orthopaedic surgeons sitting for their American Board of Orthopaedic Surgery (ABOS) part II examination are entered into the ABOS database from April 1 through September 30 of the year before the examination. Complications are entered if they occurred within 30 days of the end of the collection period. We queried the ABOS database by Current Procedural Terminology (CPT) code for all cases of arthroscopic knee surgery (92,565 cases) and sports medicine arthroscopic knee surgery (71,349 cases).
Sports medicine cases were defined and grouped for comparative purposes by CPT code as designated in Table 1 for CPT codes 29880, 29881, 29882, 29883, 29877, 29879, 29888, 29889. Patient demographic factors were gathered, including patient age (<40 or ≥40 years) and sex, as were surgeon factors, including geographic region of practice (Northeast, Southeast, Midwest, South, Northwest, and Southwest) and sports fellowship training status. Complications were grouped according to type: surgical (hemorrhage, bone fracture, implant failure, implant fracture, infection, limb ischemia, wound dehiscence, nerve palsy/injury, delayed or nonunion, skin ulcer or blister, tendon or ligament injury, surgical procedure intervention, or unspecified surgical complication), medical (cerebrovascular accident, congestive heart failure, myocardial infarction, pneumonia, renal failure, patient expiration, or medical unspecified complication), anesthetic (unspecified), and PE (pulmonary embolus).
Grouping of Sports Medicine Arthroscopic Knee Procedures Based on CPT Code a
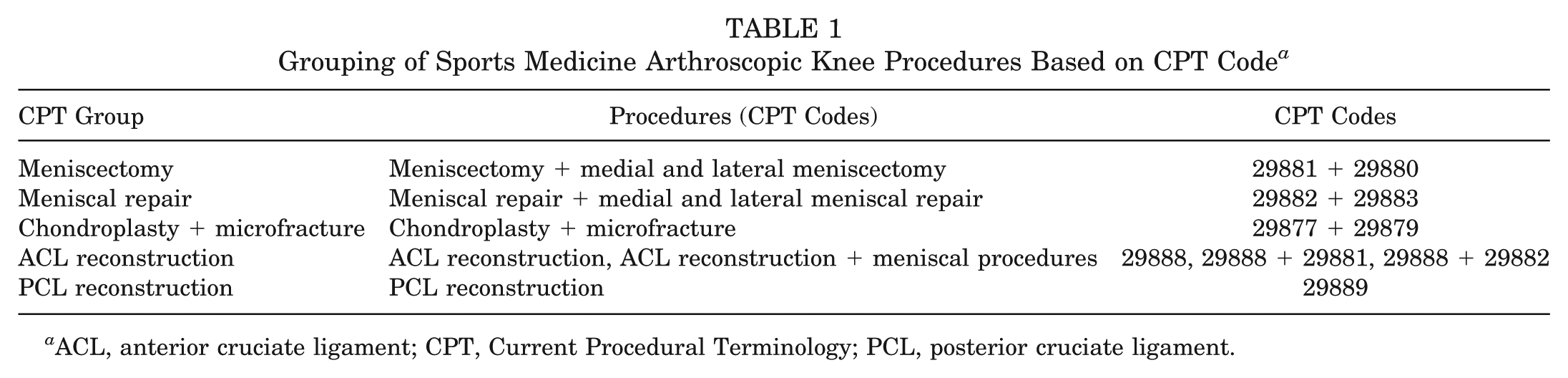
ACL, anterior cruciate ligament; CPT, Current Procedural Terminology; PCL, posterior cruciate ligament.
Statistical Analysis
The frequency and percentage of complications for all knee arthroscopies and sports-related knee arthroscopic procedures (partial meniscectomy, meniscal repair, chondroplasty, microfracture, anterior cruciate ligament [ACL] reconstruction, or posterior cruciate ligament [PCL] reconstruction) were determined. Chi-square tests were used to determine the significance of differences in the rates of complications by patient age and sex and by the geographic location and sports fellowship training status of the physicians. Statistical significance was set at P < .05.
Results
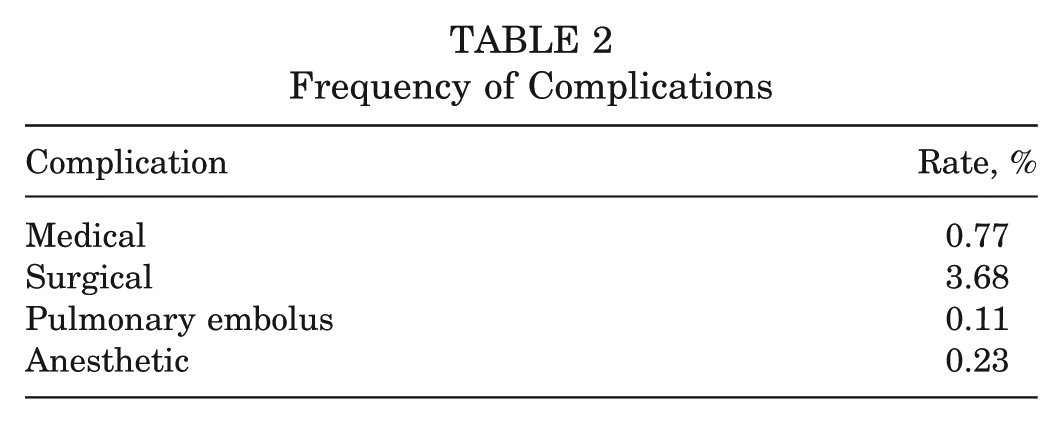
There were 4305 complications out of 92,565 knee arthroscopic procedures for an overall complication rate of 4.7%. Complication rates for various sports medicine arthroscopic knee procedures ranged from 2.8% for meniscectomies to 20.1% for PCL reconstructions (Figure 1). Surgical complications (3.7%) were the most common category of complication (Table 2).
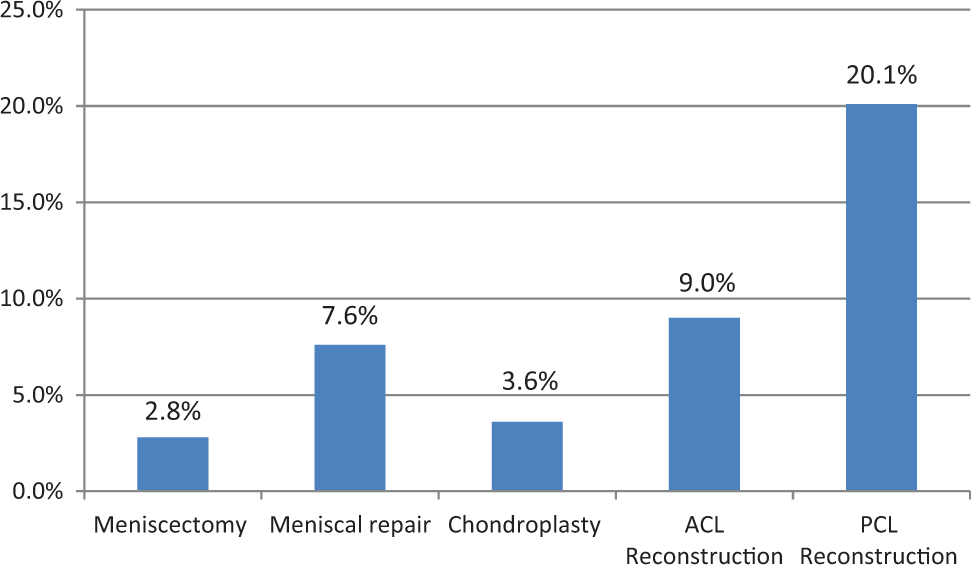
Complication rates by procedure type. ACL, anterior cruciate ligament; PCL, posterior cruciate ligament.
Frequency of Complications
Complication rates by patients’ age and sex and surgeons’ geographic location and fellowship training status are summarized in Table 3. Male patients had a higher rate of complications than females (4.9% vs 4.3%). Patients younger than 40 years had higher complication rates than those older than 40 years (6.2% vs 3.6%). Surgeons who completed a sports fellowship had higher complication rates than those who did not (5.1% vs 4.1%; all P values < .0001). There were no statistically significant differences in the rates of complications by geographic region within the United States.
Complication Rate by Patient Age and Sex, Surgeon Sports Fellowship Training Status, and Geographical Region
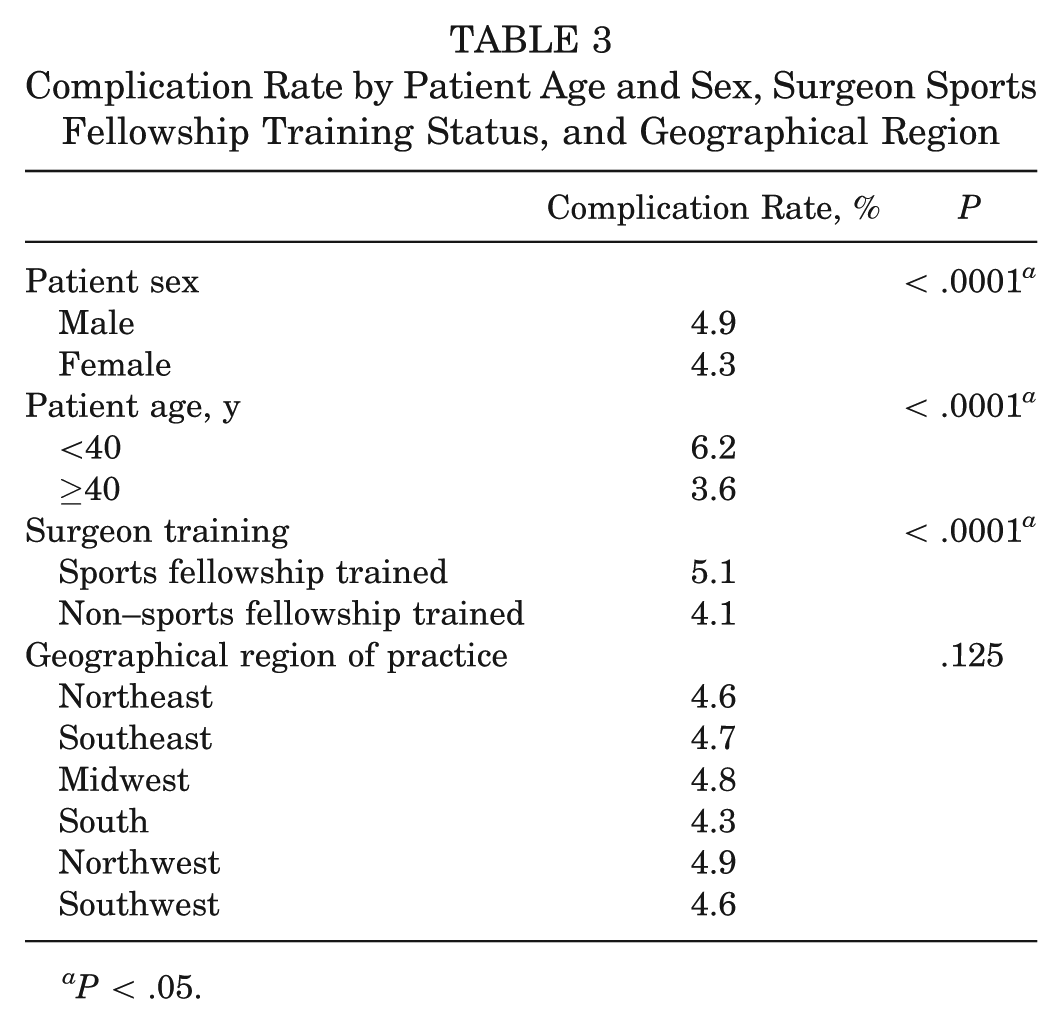
P < .05.
The overall rate of PE was 0.11%; that of deep venous thrombosis (DVT) was not specifically reported. Overall, 18.8% of the reported procedures were performed with a form of chemical prophylaxis for thrombosis. There was no significant difference in the rate of PE in the patients that received chemical prophylaxis (0.15% with prophylaxis and 0.10% without; P = .284).
Discussion
Limited information exists on the current rates of complications in arthroscopic knee surgery performed in the United States. In 1985, Small 14 surveyed orthopaedic surgeons in the United States and reported an overall complication rate of 0.56% in 375,069 knee arthroscopies. Three years later, he published a 19-month prospective study including 10,262 arthroscopic procedures (86% involving the knee) with an overall complication rate of 1.68%; the most common complication was hemarthrosis, which accounted for 60% of all complications. 13
More recent European literature has also examined complication rates in knee arthroscopy. A small retrospective study from a community hospital in Norway evaluated the complication rates of 876 simple arthroscopic procedures from 1999 to 2001; it reported an overall complication rate of 5.00%, of which 0.68% had therapeutic consequences necessitating additional unplanned surgery or medical intervention. 10 Jameson et al 6 evaluated 30-day reoperation and readmission rates based on 301,701 knee arthroscopies performed from 2005 through 2010, utilizing the English National Health Service data. They found a 0.64% 30-day readmission rate, a 0.26% 30-day wound complication rate, a 0.40% 30-day reoperation rate, and a 0.08% 90-day PE rate.
We reported an overall complication rate of 4.7%, which was higher than all of the above studies, except for the Norwegian study with a small sample size. Arthroscopic techniques have evolved significantly since the 1980s. Procedures once performed primarily in open fashion, such as ACL and PCL reconstructions and meniscal repairs, are now most often performed arthroscopically. This could explain the higher complication rates observed in our study. In addition, compared with that of the more recent European literature, our study complication rate may be higher because of the prospective nature of data reporting, which may capture a higher percentage of complications. Last, ABOS applicants may be less experienced surgeons than their ABOS-certified counterparts, which could account for the higher complication rate.
Despite an overall complication rate of 4.7%, we found significant variation among procedures, ranging from 2.8% for meniscectomies to 20.1% for PCL reconstructions. In general, the increasing complexity of cases—from chondroplasty to meniscal repair to ACL reconstruction—corresponded with increasing complication rates (3.6%, 7.6%, and 9.0%, respectively). This relationship was also seen in the 1985 survey, which had an overall complication rate of 0.56% but a rate of 1.8% for ACL repair/reconstruction and 2.4% for meniscal repair. 14
When comparing the different patient and surgeon characteristics, we found higher complication rates for male patients, patients under 40 years, and surgeons with a sports medicine fellowship; we found no difference based on US geographic region. The male complication rate of 4.9% versus the female rate of 4.3% is statistically significant, although the small difference in rates may not have clinical relevance. Similar results were found in the British registry, with male patients having a higher 30-day readmission and reoperation rate. 6
The 6.2% complication rate in younger patients (<40 years) was nearly double (3.6%) that of patients older than 40 years; similar results were seen in the Jameson et al 6 registry study. A difference of this magnitude could affect informed consent in younger patients. The difference observed in age-related complication rates may be explained by differences in surgical complexity. For example, meniscal repairs and ACL and PCL reconstructions, which have higher complication rates, are generally performed in a younger patient population than are chondroplasties and meniscectomies, which are performed more often in patients older than 40 years. The increased complexity of cases may also explain the increased complication rate (5.1% vs 4.1%) observed in surgeons with sports medicine fellowships training compared with those without. Because we are unable to obtain patient-specific data for the 92,565 procedures, we cannot perform a multivariate analysis to determine if case complexity is the sole explanation for the observed increased complication rates in younger patients and with sports medicine fellowship–trained surgeons.
We anticipated finding minor regional geographic differences in complication rates secondary to regional variation in types of procedures performed, as there is high regional variation among orthopaedic procedure rates in general, especially in regard to the rates of spine and knee arthroplasty.11,15 Specifically, Musahl et al 9 reported that in combination with ACL reconstruction, 18.6% of patients in the Southwest underwent concomitant meniscal repair, as opposed to only 11.3% in the Northwest. Because of the difference in complication rates between meniscectomy and repairs, this may have led to varied regional complication rates. However, we did not find any regional differences in complication rate.
The 0.11% rate of PE was used as a proxy for DVT, which is reported in a range of 0.14% to 17.9% for knee arthroscopies. DVTs are not categorically reported in ABOS data; thus, we were unable to determine the DVT rate. Furthermore, the asymptomatic nature of DVTs may underestimate the real DVT rate in a study such as this. A meta-analysis from 2005 found a DVT rate of 9.9% in patients who did not receive prophylaxis and a rate of 2.1% for proximal DVTs. 5 A retrospective study of more than 20,000 elective knee arthroscopies in a single health system reported a symptomatic DVT rate of 0.25% and a PE rate of 0.17%. 8 In our study, 18.8% of the patients received chemical DVT prophylaxis, which likely represents a combination of variation among surgeons as well different prophylaxis strategies based on patient and surgical risk factors. We found a PE rate of 0.15% in patients receiving chemical prophylaxis, compared with 0.10% in those not receiving prophylaxis (P = .284). Although not statistically significant, the trend toward a higher rate of pulmonary emboli in patients receiving chemical prophylaxis may reflect the fact that the patients receiving prophylaxis are at a higher risk of thrombosis.
This study is a retrospective query of broadly and prospectively gathered data that included all ABOS applicants across the United States between from 2003 to 2009. Unlike some surgical databases, this captures all procedures performed at surgery centers as well as inpatient facilities. The ability to include surgery center data is increasingly important, as 51% of knee arthroscopies were performed in surgery centers in 2006 as compared with only 15% in 1996. 7 This study design is more comprehensive than others that evaluate preexisting databases that capture only data from hospital or surgery centers, as this captures all complications seen by the surgeon regardless of the location where the complication was identified or treated.
The main weakness of this study is that the complications are self-reported, which may lead to underreporting of complications. However, given the stakes of the examination process, it is also possible that ABOS candidates may overreport rather than underreport their complications in their board collection period. One additional weakness is that the surgeons who are in their board collection period are likely less experienced than their ABOS-certified peers, which may threaten the generalizability of these results to ABOS-certified surgeons. Finally, the length of the collection period can be both a strength and a weakness; the length of time during which complications are reported is not fixed. Depending on when the procedure was performed within the ABOS collection period, the complication collection time could range from 30 to 210 days. Although it is not a standardized collection period, the length of time in which complications are collected is longer than the commonly published 30-day follow-up period.
One potential weakness of this study relates to the differences among surgeon-reported outcomes, patient-reported outcomes, and objectively assessed outcomes. All prior large studies on complication rates after arthroscopic knee surgery,1,4,8,10,11,14 including this one, are based on surgeon-reported outcomes. Objectively assessed outcomes, such as use of Doppler ultrasound for presence of DVT, may result in higher rates of DVT; however, not all these DVTs may be clinically relevant. However, patient-reported complications, which are certainly relevant and the most likely to affect informed consent, may differ significantly from surgeon-reported outcomes and complication rates.
Despite the comprehensiveness of this study design, a national registry for arthroscopic (or any) procedures would provide the most comprehensive and prospective data to date on diagnosis, treatment, outcomes, and complications. Mandatory (Denmark) and voluntary (Norway and Sweden) ACL registries exist in Scandinavia and could exist in the United States. 4 The Mulitcenter Orthopaedic Outcomes Network (ie, MOON group) has demonstrated the ability of multiple US centers to collaborate to prospectively gather data. 2 A national registry could be possible in the United States if tied to reimbursement or billing, and it could provide more complete and potentially more accurate data.
Conclusion
The overall complication rate for arthroscopic knee procedures was 4.7%, with a range of 2.6% for meniscectomies to 20.1% for PCL reconstructions. Knee arthroscopy is not a benign procedure, and patients should be aware of the risk of complications. These data can be utilized to inform patients, for personal improvement, for research-based comparisons, and for performance-based initiatives.
Footnotes
Presented at the 39th annual meeting of the AOSSM, Chicago, Illinois, July 2013.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.