
Abstract
Background:
Greater neck strength and activating the neck muscles to brace for impact are both thought to reduce an athlete’s risk of concussion during a collision by attenuating the head’s kinematic response after impact. However, the literature reporting the neck’s role in controlling postimpact head kinematics is mixed. Furthermore, these relationships have not been examined in the coronal or transverse planes or in pediatric athletes.
Hypotheses:
In each anatomic plane, peak linear velocity (ΔV) and peak angular velocity (Δω) of the head are inversely related to maximal isometric cervical muscle strength in the opposing direction (H1). Under impulsive loading, ΔV and Δω will be decreased during anticipatory cervical muscle activation compared with the baseline state (H2).
Study Design:
Descriptive laboratory study.
Methods:
Maximum isometric neck strength was measured in each anatomic plane in 46 male and female contact sport athletes aged 8 to 30 years. A loading apparatus applied impulsive test forces to athletes’ heads in flexion, extension, lateral flexion, and axial rotation during baseline and anticipatory cervical muscle activation conditions. Multivariate linear mixed models were used to determine the effects of neck strength and cervical muscle activation on head ΔV and Δω.
Results:
Greater isometric neck strength and anticipatory activation were independently associated with decreased head ΔV and Δω after impulsive loading across all planes of motion (all P < .001). Inverse relationships between neck strength and head ΔV and Δω presented moderately strong effect sizes (r = 0.417 to r = 0.657), varying by direction of motion and cervical muscle activation.
Conclusion:
In male and female athletes across the age spectrum, greater neck strength and anticipatory cervical muscle activation (“bracing for impact”) can reduce the magnitude of the head’s kinematic response. Future studies should determine whether neck strength contributes to the observed sex and age group differences in concussion incidence.
Clinical Relevance:
Neck strength and impact anticipation are 2 potentially modifiable risk factors for concussion. Interventions aimed at increasing athletes’ neck strength and reducing unanticipated impacts may decrease the risk of concussion associated with sport participation.
Keywords
Sport- and recreation-related concussion is a common injury that is now globally recognized as a major public health concern.23,27 As many as 10% to 25% of concussed athletes go on to develop prolonged symptoms,9,19 and there is growing concern surrounding the potential long-term effects of concussion on athletes’ neurocognitive health.14,18,28,34 Risk factor identification and development of injury prevention strategies are therefore critical.
While all athletes are at risk for sustaining concussion, the risk appears to be greater in pediatric and female athletes.7,10,21,26 Low neck strength is a potentially modifiable risk factor that may contribute to an elevated concussion risk in these populations. Stronger muscles are not only capable of generating greater absolute force values but have a greater cross-sectional area, produce greater tensile stiffness at a given activation level, and generate torque more rapidly than weaker muscles. 39 Since studies have shown that women have less neck strength than men and children have less neck strength than adults,13,20,22,24,38 these populations may be at a disadvantage with regard to controlling the head’s response during an impact because of less tensile stiffness to resist cervical muscle stretch. Children may be at an even greater disadvantage than adults because of their greater head mass to body mass ratio. 6
Athletes with smaller, weaker, more compliant necks are more likely to experience greater resultant linear and angular head displacements, velocities, and accelerations after impact. Broglio et al 3 found greater peak linear head accelerations in high school football athletes than were found using similar methods at the collegiate level and attributed this finding to “physical maturation and the associated neck strength and endurance discrepancy between the levels of play.”3,4,30 Similarly, Tierney et al 42 found that physically active adult women exhibited less neck muscle strength and greater sagittal plane head-neck segment peak angular accelerations and displacements than males in response to externally applied forces. Furthermore, Viano et al 45 showed, using video reconstructions of head impacts resulting in concussion in professional football players, that stiffer necks reduce translational head displacement, velocity, and acceleration. In addition, there is evidence to suggest that anticipatory cervical muscle activation to brace for impact may also reduce the head’s kinematic response during a collision. In a study using the Head Impact Telemetry System (HITS) to study in vivo head impact kinematics in youth ice hockey athletes, Mihalik et al 31 reported greater angular accelerations and impact severity profiles when moderately severe collisions were unanticipated and attributed these results to tensing of the cervical musculature during anticipated collisions to mitigate the severity of these impacts.
In contrast, other work has failed to identify a clear relationship between greater neck strength and postimpact head kinematics.25,32 Despite this, the overall body of literature addressing this relationship suggests that interventions aimed at increasing athletes’ neck girth, strength, and stiffness still hold promise as a means of reducing their risk of sport-related concussion. Therefore the purpose of this study was to determine the influence of neck strength and muscle activation status on resultant head kinematics after impulsive loading. These relationships were studied in athletes of both sexes, ranging in age from pediatric to adult, in each of the 3 principal anatomic planes (sagittal, coronal, and transverse). We chose the peak changes in linear and angular velocity of the head, ΔV and Δω, as the primary outcome variables of interest given their close relationships to the Head Injury Criterion and brain tissue deformation patterns,41,45 respectively, to test the following primary hypotheses:
H1: In each anatomic plane, ΔV and Δω will be inversely related to maximum volitional cervical muscle force generated in the opposing direction.
H2: ΔV and Δω will be decreased during anticipatory cervical muscle activation compared with the baseline cervical muscle activation state.
Materials and Methods
Participants
A total of 46 contact sport athletes (24 male; 22 female) aged 8 to 30 years participated in this study. Participant ages were similar between the sexes (16.3 ± 5.0 years for males vs 15.0 ± 4.4 years for females; P = .325), with 14 males and 12 females of high school age or younger and 10 males and 10 females of college age or older. Male participants were taller (167.2 ± 12.4 cm vs 155.9 ± 12.8 cm; P = .004) and heavier (70.3 ± 28.8 kg vs 53.3 ± 14.4 kg; P = .015) than females. Participants represented a broad range of competitive levels and included 15 soccer players, 14 ice hockey players, 9 football players, 5 martial artists, 2 wrestlers, and 1 lacrosse player. Potential participants were excluded if they had a self- or parent-reported history of concussion, neck injury, migraine headache, or stinger/cervical radiculopathy. Additional exclusion criteria were corrected vision less than 20/40, recent exposure to head lice, and known or suspected pregnancy. A brief screening evaluation to rule out any physical examination signs of cervical musculoskeletal injury, cervical radiculopathy, or myelopathy was performed by the principal investigator (PI) before enrollment. All participants provided informed written consent, or assent with parental consent for minors, using institutional review board–approved documentation before participation. Each participant completed a brief set of warm-up exercises consisting of 1 set of static neck stretches in each plane (flexion, extension, left and right lateral flexion, left and right rotation: 1 repetition each for 12 seconds), followed by 1 set of dynamic neck and shoulder circles lasting 12 seconds in each direction before data collection.
Demographic and Anthropomorphic Measurements
Age, sex, and sport participation history were recorded for each athlete participating in the study. Height and weight were measured using a standing scale. Neck circumference (girth) was measured at the level of the thyroid cartilage using a flexible metric tape. Head mass, which was used in estimating the location of the head’s center of mass, was measured with participants lying supine with their cervical musculature relaxed by suspending the head in a custom head support affixed to a cable with an in-line force transducer (TLL-500; Transducer Techniques, Temecula, California, USA) (intraclass correlation coefficient [ICC] = .807). Sonographic cross-sectional area of the right sternocleidomastoid muscle at its midpoint was measured in short axis (cross section) with participants sitting upright using an Ultrasonix RP Touch Research Ultrasound machine (Ultrasonix, Richmond, British Columbia, Canada) with a 38-mm, 14-MHz linear array transducer (ICC = .985).
Assessment of Maximum Isometric Neck Strength and Rate of Force Development
Participants sat upright in a rigid-backed seat, with their shoulders and torso stabilized against the seatback by a strap, while wearing customized snugly fitting wrestling headgear attached to an adjustable cable with an in-line force transducer capable of being positioned for pulling against a fixed beam in flexion, extension, left lateral flexion, or right axial rotation (Figure 1). They were instructed to perform maximal isometric neck muscle contractions by gradually increasing the amount of force generated by their neck over 3 seconds until they were pulling with maximal effort in the specified direction. If activation of core or back musculature resulting in obvious torso movement was observed by the study team, the trial was discarded and repeated. The greatest of 3 peak force values in each plane was recorded as the maximum isometric neck strength value. The test-retest reliability of this measure was excellent (ICC = .956). Rate of force development was then assessed by instructing participants to perform similar neck muscle contractions “as rapidly as possible” in each of the specified directions without performance feedback, analogous to rate-of-force generation protocols previously employed in our laboratory for other joints. 40 The rate-of-force development was defined for each trial as the maximum absolute instantaneous slope of the force vs time curve, with the greatest of the 3 peak rate-of-force development values in each plane taken as the maximum rate-of-force development value. The test-retest reliability of this measure was also high (ICC = .832).
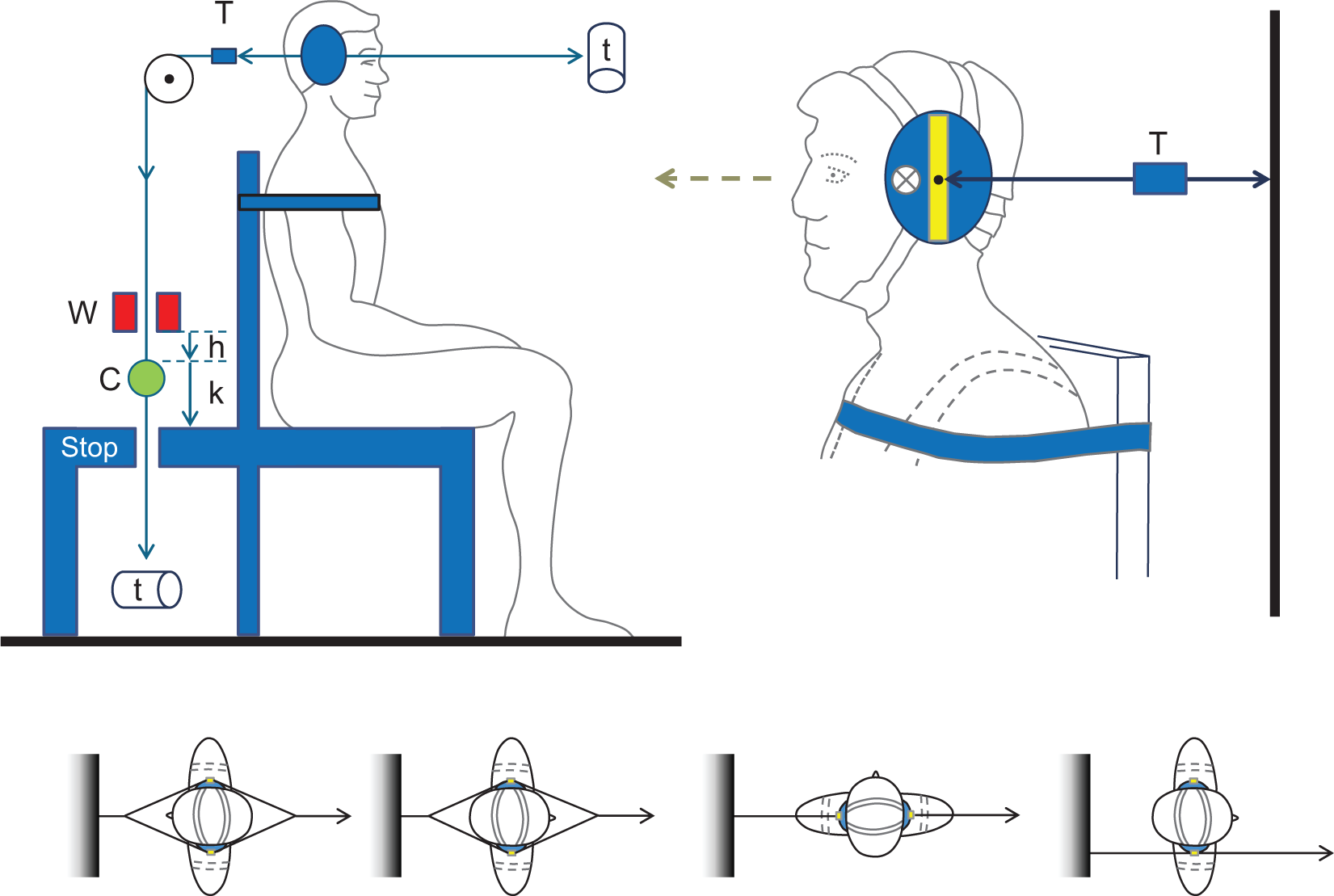
(Top left) Impulsive loading apparatus configured for forced-extension head pulling. Constant force springs (t) apply light, counterbalanced pretension to maintain the cables taut at any head position. The 1-kg drop weight (W) is released from a height (h) onto the cable clamp (C) such that both the weight and clamp fall from height (k) onto the safety stop, applying an impulsive test force to the head, with cable tension recorded by the in-line force transducer (T). (Top right) Close-up view of the modified wrestler’s headgear illustrating the relative positions of the cable connecting pin and the estimated head center of mass (X), with the posteriorly directed cable and in-line force transducer (T) configured for flexion strength testing. (Bottom, from left to right) Differential cable configuration for impulsive loading in sagittal plane extension and flexion, coronal plane right lateral flexion, and axial plane left rotation.
Method of External Force Application to the Head
Participants again sat upright with their shoulders and torso stabilized against a rigid-backed seat. The snugly fitting wrestling headgear was attached to an adjustable cable with an in-line force transducer capable of being positioned to pull the head in flexion, extension, right lateral flexion, or left axial rotation (Figure 1). The seat height was positioned so that the cable ran horizontally from the headgear to a pulley directing it downward to an in-line cable clamp and constant force spring attached to the opposite end. A 1-kg weight located above the cable clamp was free to slide up and down the vertical portion of the cable, such that upon its release, the weight free-fell until it contacted the cable clamp, applying a force through the cable to the headgear, proportional to the height from which the weight was dropped. A safety constraint consisting of a weight “landing pad” was positioned 2.5 cm directly below the 1-kg mass to limit the maximum displacement of the participant’s head-neck segment to prevent injury. A second cable attached to the headgear ran horizontally in the opposite direction to a constant force spring to counterbalance the weight of the first cable. The custom loading apparatus was similar to experimental devices previously developed to apply impulsive loads to subjects’ heads in the sagittal plane.25,37,42
Normalized impulsive loads were applied to the headgear by dropping the 1-kg weight from a height that was directly proportional to the participant’s body mass so as to deliver loads of sufficient magnitude to induce measurable head motion in participants of widely varying body mass, while remaining well below the magnitude necessary to induce injury. Drop heights varied in 0.5-cm increments for every 9.1 kg of participant body weight from 1.5 cm (for participants weighing 18.6-27.2 kg) to 8.0 cm (for participants weighing 136.5-145.2 kg). The orientation of the athletes with respect to the weight-drop apparatus was varied to systematically apply loads to the head in each direction (Figure 1). Participants were initially instructed to relax their cervical musculature during load application to simulate an unanticipated head impact. They were then instructed to perform a maximal isometric neck muscle cocontraction before load application to stabilize their head as if bracing for a sport collision. Before testing, they demonstrated both the baseline and anticipatory cervical muscle activation states to the PI, to ensure differential levels of cervical muscle activation. The procedure was repeated over 3 trials in each orientation under both muscle activation conditions, with at least a 30-second rest break between trials.
Kinematic Measurements and Signal Processing
Head kinematics was measured using an Optotrak motion capture system (Northern Digital, Waterloo, Ontario, Canada) that tracked a triad of optoelectronic markers (infrared-emitting diodes) attached to participants’ foreheads, directly above the left or right eye, depending on the direction of impulsive loading and the associated orientation of the kinematic camera. Kinematic data were measured at 400 Hz to a resolution of 0.1 mm. The onset-of-force application was defined from the force transducer data, measured at 2 kHz. Raw force transducer and kinematic signals were processed and analyzed in Matlab (MathWorks, Natick, Massachusetts, USA) using a fourth-order Butterworth low-pass filter with cutoff frequencies of 70 Hz and 25 Hz, respectively, while the head mass, neck strength, and rate of force development were filtered at 10 Hz. To define the anatomic reference coordinate system of the head, a handheld Optotrak digitizing wand was used to identify the 3-dimensional locations of the following anatomic landmarks: left and right infraorbital notches, external auditory meatuses, mastoid processes, nasion, and occiput. The origin of the reference coordinate system was then defined at the center of mass of the head, using the position of the infraorbital notches to define the Frankfort (x-y) plane. 46 Head center of mass in the y-axis (left-right) was defined at the midpoint of the external auditory meatuses, while head center of mass in the x-axis (anterior-posterior) and z-axis (cephalad-caudad) was estimated using regression equations derived from published anatomic data (COMx = −0.0224 * head mass + 0.9258; COMz = 0.6081 * head mass + 0.516). 1
Head kinematics was calculated with respect to the head position and orientation at t = 0, assuming a fixed torso position. For each trial, peak linear and angular displacements, velocities, and accelerations of the head projected onto its center of mass were calculated in each of the 3 principal anatomic planes. Because of negligible axial translation during rotational impulsive loading, the linear component of head motion in this plane was not included in the statistical analyses. Representative kinematic tracings illustrating typical postloading linear and angular velocity patterns in each direction of motion are illustrated in Figure 2. To account for differential impulsive load magnitudes between participants, all kinematic outcome variables were normalized by dividing by the energy associated with the impulse (Epotential = mgh). Mean normalized kinematic head response values were then calculated for each parameter in each orientation under both muscle activation conditions for every participant. As participants’ heads were at rest before impulse delivery, peak and change values are equivalent for all kinematic parameters. Throughout this report, the normalized peak linear and angular velocities of the head are referred to as ΔV and Δω, respectively.
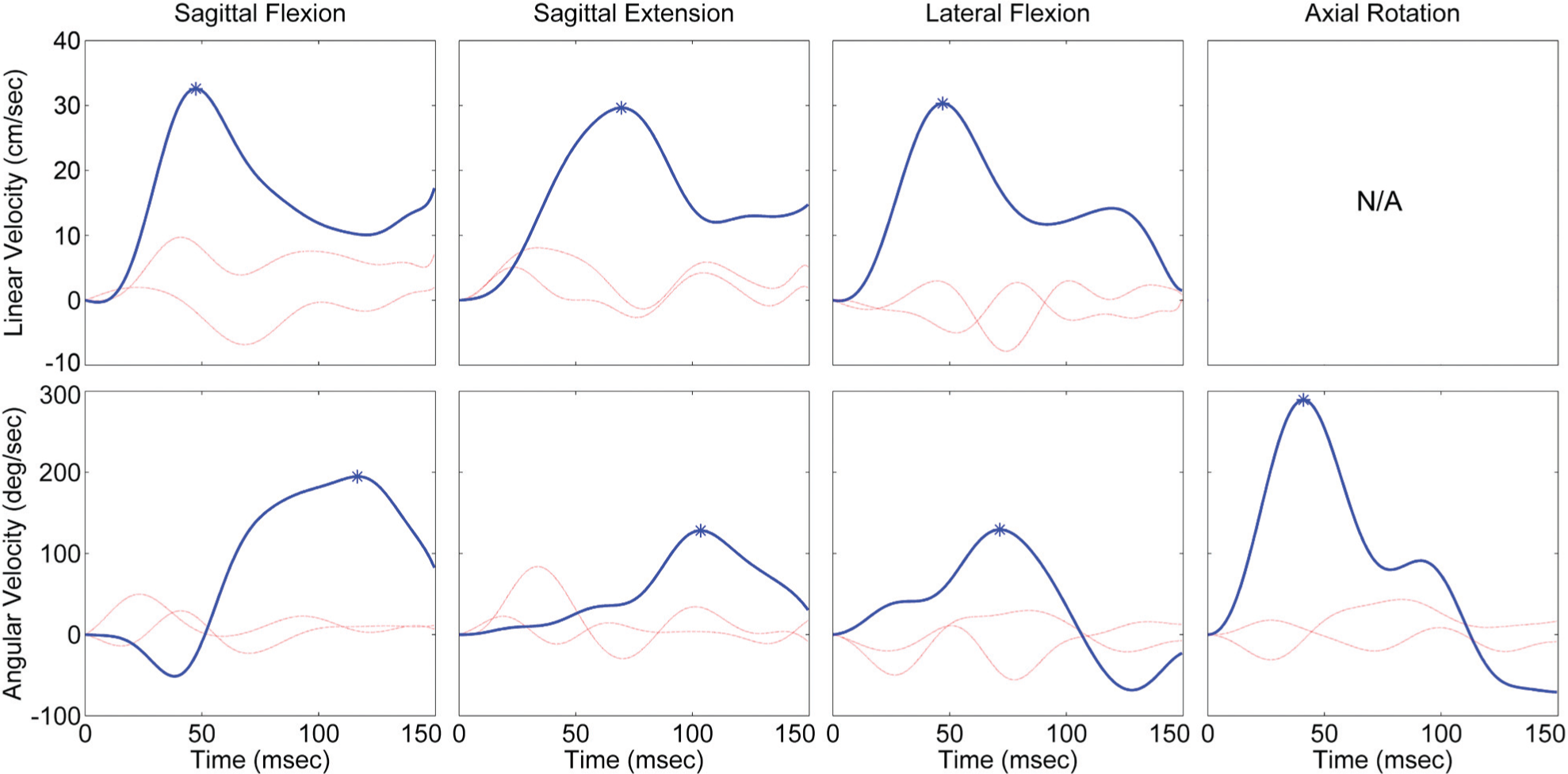
Representative kinematic tracings illustrating typical linear velocity (top row) and angular velocity (bottom row) vs time plots over the first 150 ms after impulsive loading in each direction of head motion. Motion in the plane of force application is represented by the thick line (sagittal plane for flexion and extension, coronal plane for lateral flexion, and axial plane for rotation), while the components of motion in the 2 nonprimary planes are represented by the thin lines. For each tracing, positive velocity in the primary plane of motion is associated with motion in the same direction as external force application (forward for sagittal flexion, backward for sagittal extension, etc). Asterisks at peak linear and angular velocity points represent ΔV and Δω values. N/A, not applicable.
Statistical Analysis
All statistical analyses were performed using SAS (version 9.3; SAS Institute, Cary, North Carolina, USA). Descriptive statistics were calculated for continuous variables, which are presented as mean ± SD throughout this report. Multivariate linear mixed models were used to test H1 and H2 across all directions of head motion, with adjustment for age and sex by their inclusion as covariates in the models. For the primary analysis, maximum isometric neck strength in the opposing direction (continuous variable, H1) and cervical muscle activation status (binary variable, H2) were considered the primary predictor variables, while ΔV and Δω (both continuous variables) were considered the primary kinematic outcome variables. Age was treated as a continuous variable for the primary statistical analyses, but participants were dichotomized into 2 age groups (high school or younger athletes and collegiate or older athletes) for the purposes of data presentation in 2 tables. Pearson product-moment correlation coefficients were then calculated to describe the individual relationships between neck strength and ΔV and Δω in each direction, under each cervical muscle activation state. To account for sign differences arising from arbitrary axis label definitions, the convention used throughout this report is to present inverse correlations as positive r values. Secondary analyses assessed the relationships between neck circumference and ΔV and Δω in each direction of motion as well as between sternocleidomastoid cross-sectional area and ΔV and Δω in sagittal extension.
Results
Significant main effects were present for neck strength (H1) and cervical muscle activation status (H2) for both ΔV (P < .001 each) and Δω (P < .001 each) across all directions of motion. No interaction effects were present between neck strength and muscle activation status for ΔV (P = .838) or Δω (P = .914). All neck strength and cervical muscle activation effects remained significant when adjusting for age and sex as covariates in the models (all P < .001). In the expanded models, age but not sex also had a significant independent effect on both ΔV (P < .001 for age; P = .165 for sex) and Δω (P < .001 for age; P = .926 for sex). When the strength-kinematics relationships were assessed separately for sagittal plane flexion and extension, coronal plane lateral flexion, and axial plane rotation, significant strength effects remained present for 5 of the 7 models: strength–sagittal extension ΔV (P = .012), strength–sagittal extension Δω (P = .016), strength–sagittal flexion ΔV (P < .001), strength–sagittal flexion Δω (P = .014), and strength–axial rotation Δω (P < .001); the relationships between strength and ΔV and Δω failed to reach significance for coronal plane lateral flexion (P = .090 and P = .079, respectively). Similarly, when the anticipatory cervical muscle activation-kinematics relationships were assessed separately in each direction of motion, significant anticipatory activation effects remained present for 6 of the 7 models: activation–sagittal extension ΔV (P < .001), activation–sagittal extension Δω (P < .001), activation–sagittal flexion ΔV (P < .001), activation–lateral flexion ΔV (P = .008), activation–lateral flexion Δω (P < .001), and activation–axial rotation Δω (P = .028); the relationship between muscle activation state and Δω failed to reach significance for sagittal plane flexion (P = .205).
The relationships between neck strength and ΔV and Δω, in each plane of motion, under both cervical muscle activation states are illustrated in Figure 3, with the associated correlation coefficients presented in Table 1 (H1). The analogous results for rate-of-force generation in each direction are similar, but of smaller magnitude, and reached statistical significance in each direction of motion except for coronal plane lateral flexion (r = .405 to r = .540 for sagittal flexion; r = .425 to r = .581 for sagittal extension; r = .163 to r = .235 for lateral flexion; r = .592 to r = .595 for axial rotation) and therefore are not separately presented in this report due to space considerations. Table 2 presents maximum isometric neck strength in each direction, as well as neck circumference and sternocleidomastoid cross-sectional area, by sex and age group, while Table 3 presents ΔV and Δω during anticipatory cervical muscle activation by sex and age group. Similar trends in ΔV and Δω as are reported in Table 3 were present during baseline levels of cervical muscle activation but are not separately presented in this report because of space considerations. Figure 4 illustrates the effect of anticipatory cervical muscle activation on head ΔV and Δω (H2). Mean ΔV decreased 12.3%, while mean Δω decreased 9.7% with anticipatory activation, as compared with the baseline cervical muscle activation state.
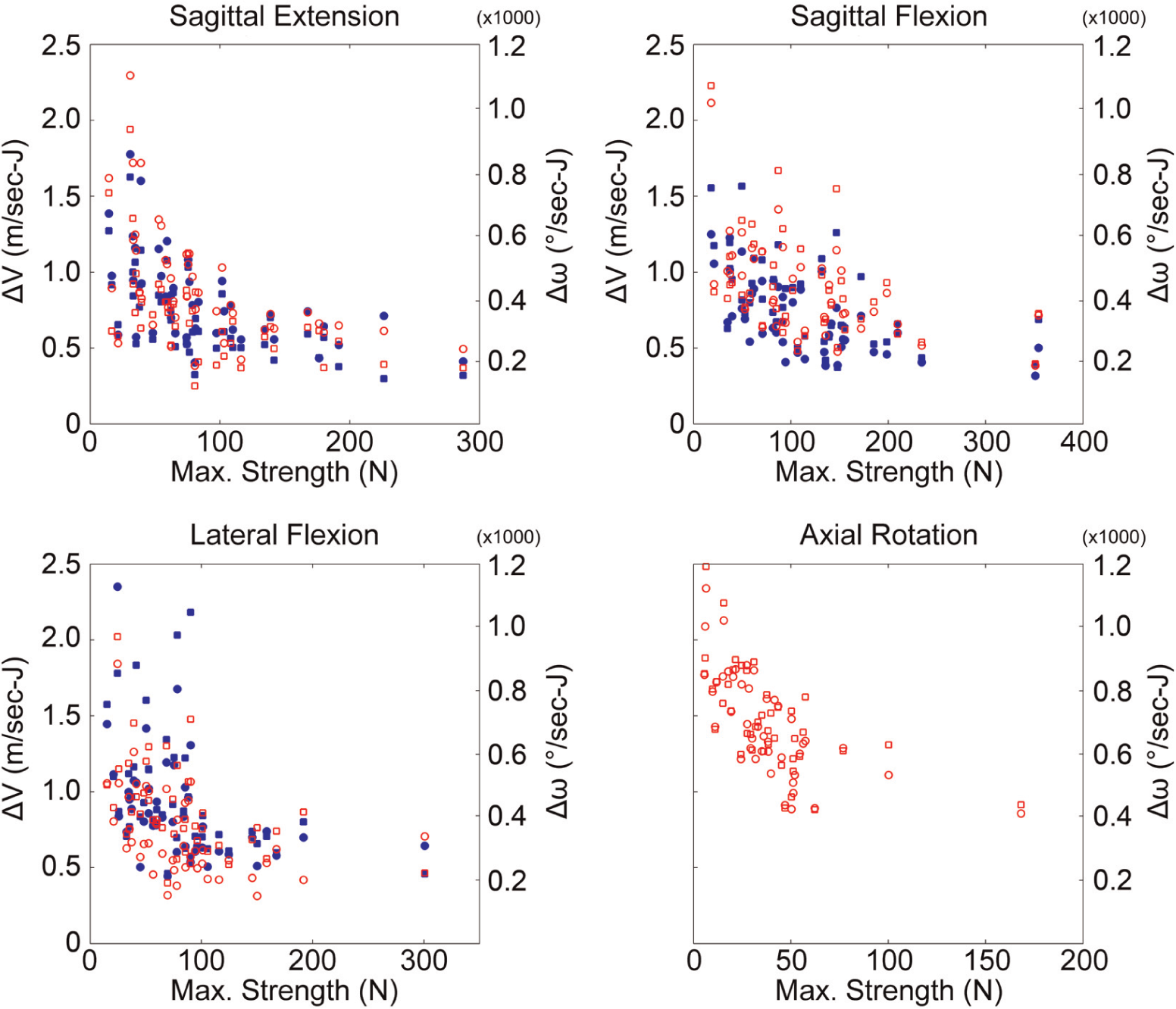
Scatterplots illustrating the inverse relationships between maximum isometric neck strength and the primary kinematic outcomes (ΔV and Δω) in each plane of motion. For each plot, ΔV (left vertical axis scale) is illustrated in solid symbols, Δω (right vertical axis scale) is illustrated in open symbols, the baseline cervical muscle activation condition is depicted by squares, and the anticipatory cervical muscle activation condition is depicted by circles.
Correlation Grid of Relationships (Pearson r) Between Normalized Kinematic Head Responses (ΔV and Δω) and Maximum Neck Strength in the Opposing Direction (in Newtons) a
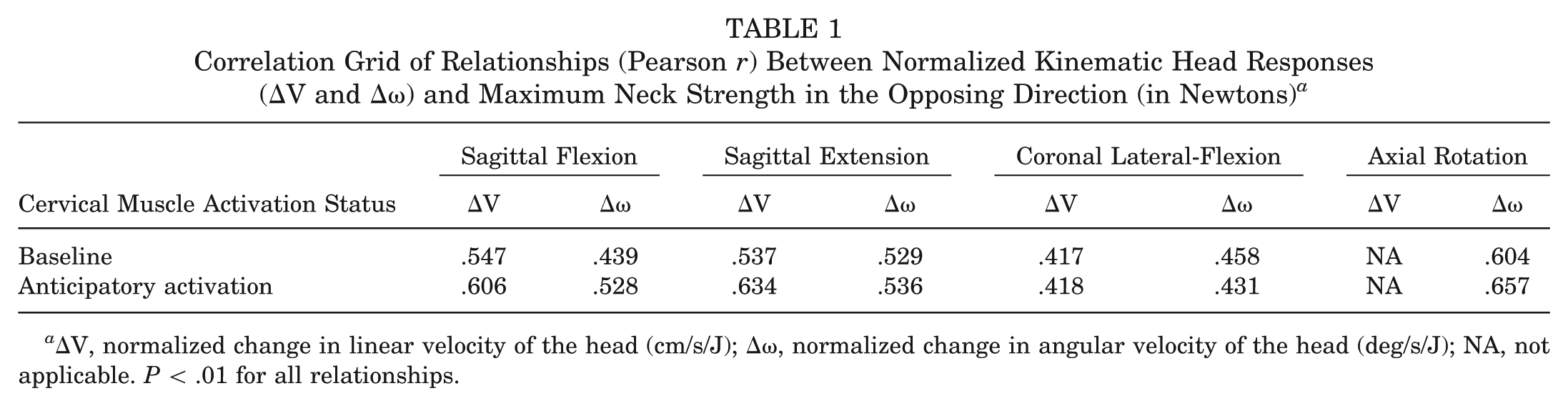
ΔV, normalized change in linear velocity of the head (cm/s/J); Δω, normalized change in angular velocity of the head (deg/s/J); NA, not applicable. P < .01 for all relationships.
Primary and Secondary Cervical Predictor Variables Presented by Sex and Age Group a
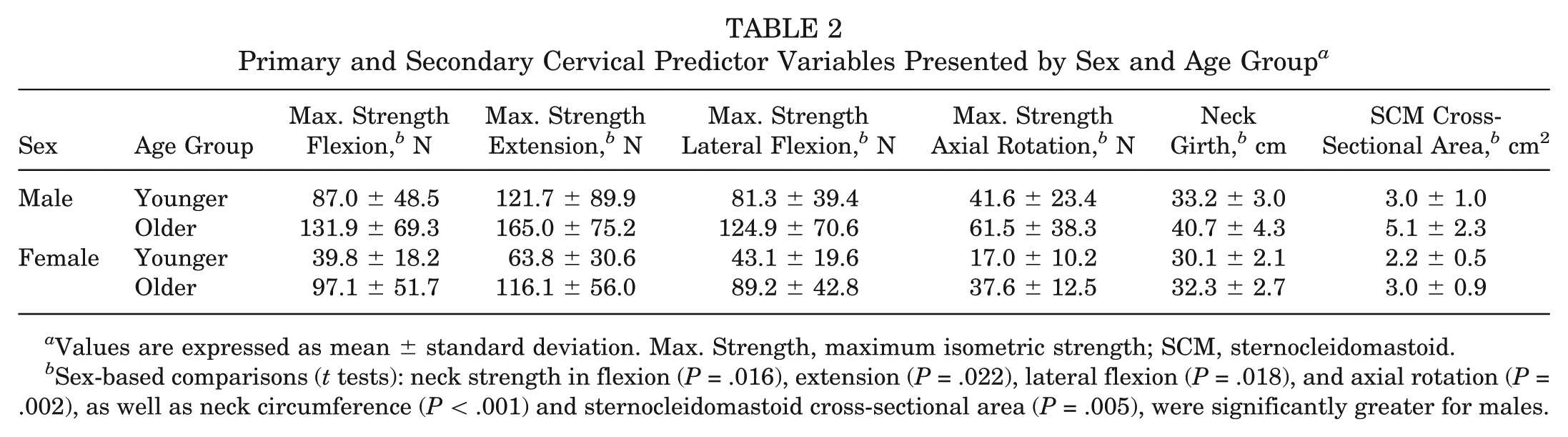
Values are expressed as mean ± standard deviation. Max. Strength, maximum isometric strength; SCM, sternocleidomastoid.
Sex-based comparisons (t tests): neck strength in flexion (P = .016), extension (P = .022), lateral flexion (P = .018), and axial rotation (P = .002), as well as neck circumference (P < .001) and sternocleidomastoid cross-sectional area (P = .005), were significantly greater for males.
Normalized Kinematic Head Response Outcomes (ΔV and Δω) During Anticipatory Cervical Muscle Activation Presented by Sex and Age Group a
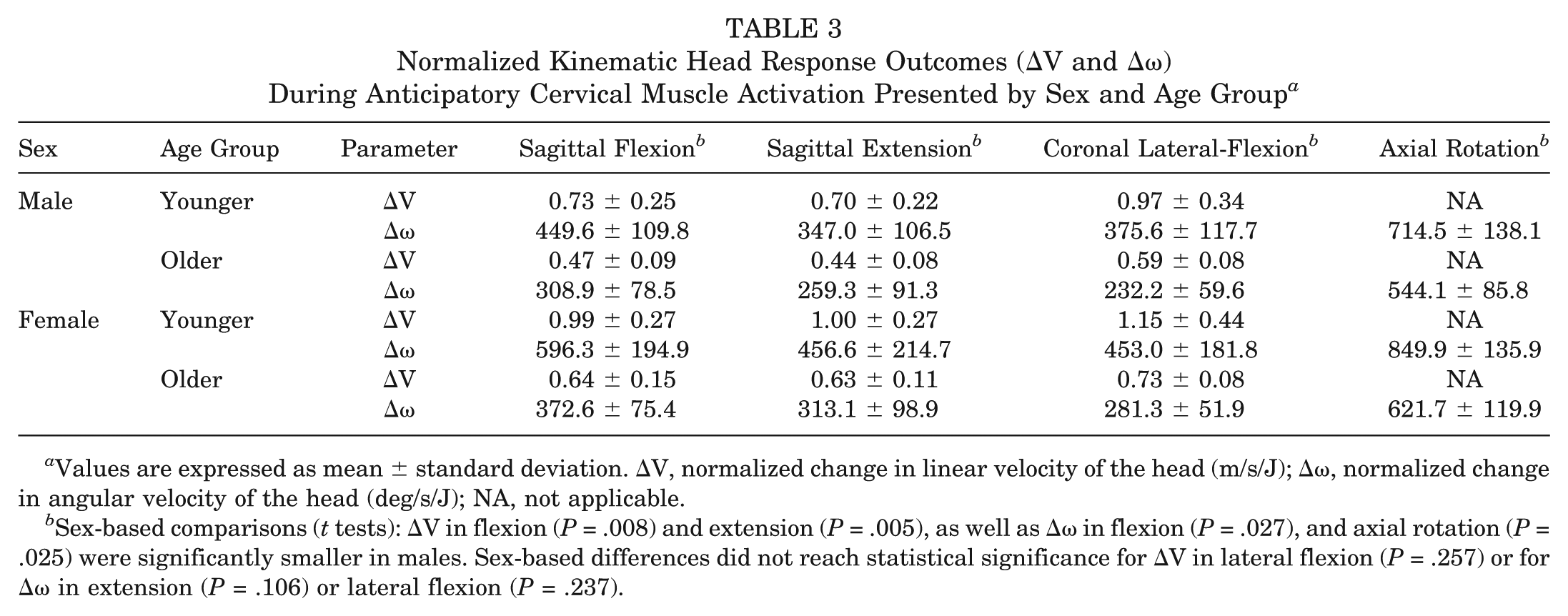
Values are expressed as mean ± standard deviation. ΔV, normalized change in linear velocity of the head (m/s/J); Δω, normalized change in angular velocity of the head (deg/s/J); NA, not applicable.
Sex-based comparisons (t tests): ΔV in flexion (P = .008) and extension (P = .005), as well as Δω in flexion (P = .027), and axial rotation (P = .025) were significantly smaller in males. Sex-based differences did not reach statistical significance for ΔV in lateral flexion (P = .257) or for Δω in extension (P = .106) or lateral flexion (P = .237).
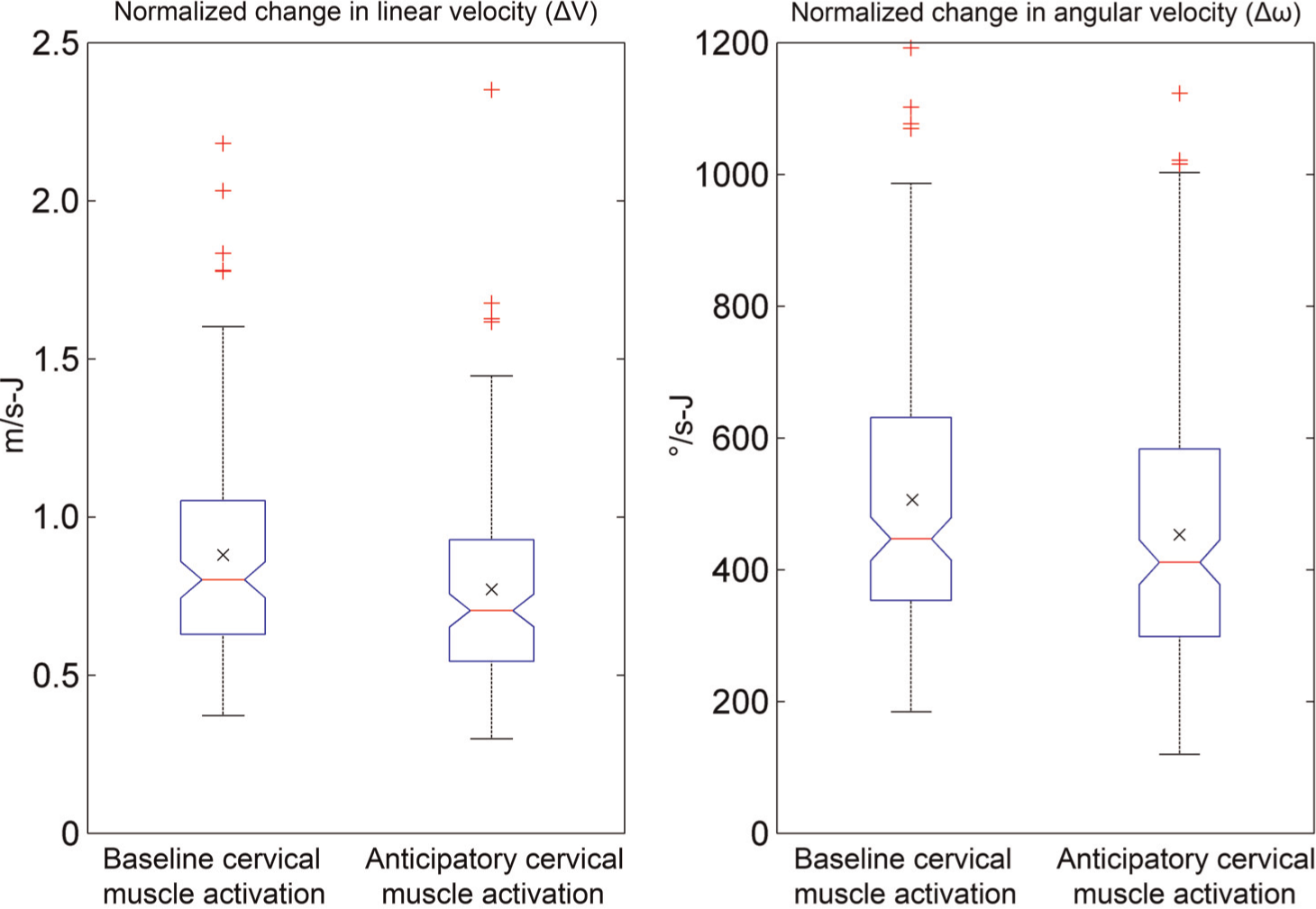
Boxplots illustrating the effect of anticipatory cervical muscle activation on ΔV and Δω. Center box line = median value; center X = mean value; box limits = interquartile range; whisker limits = 1.5*interquartile range (corresponding to approximately 2.7 standard deviations from the mean, truncated to the most extreme data point); outer plus signs = outlier data points.
In secondary analyses using separate models, neck circumference and sternocleidomastoid cross-sectional area both had significant main effects for ΔV (P < .001 each) and Δω (P < .001 each) across all directions of motion, and these effects remained significant when adjusting for age and sex in the models (P < .001 for both circumference and sternocleidomastoid-ΔV associations; P = .005 for circumference-Δω association; P = .001 for sternocleidomastoid cross-sectional area–Δω association). When the neck circumference-kinematics relationships were assessed separately for sagittal plane flexion and extension, coronal plane lateral flexion, and axial plane rotation, significant circumference effects remained present for all 7 models. Since the sternocleidomastoid muscles have been estimated to account for 69% of neck flexion strength but contribute substantially less to moment generation in extension, lateral flexion, and axial rotation, 43 the relationships between sternocleidomastoid cross-sectional area and head kinematics were assessed only in sagittal extension. In these models, significant sternocleidomastoid size effects remained present for both the ΔV and Δω. The correlations between neck circumference and ΔV and Δω, in each plane of motion, under both cervical muscle activation states are presented in Table 4. The correlations between sternocleidomastoid cross-sectional area and head kinematics in sagittal extension were r = .584 (P < .001) and r = .616 (P < .001) for ΔV and r = .505 (P < .001) and r = .520 (P < .001) for Δω, under baseline and anticipatory cervical muscle activation conditions, respectively.
Correlation Grid of Relationships (Pearson r) Between Normalized Kinematic Head Responses (ΔV and Δω) and Neck Circumference (in Centimeters) a
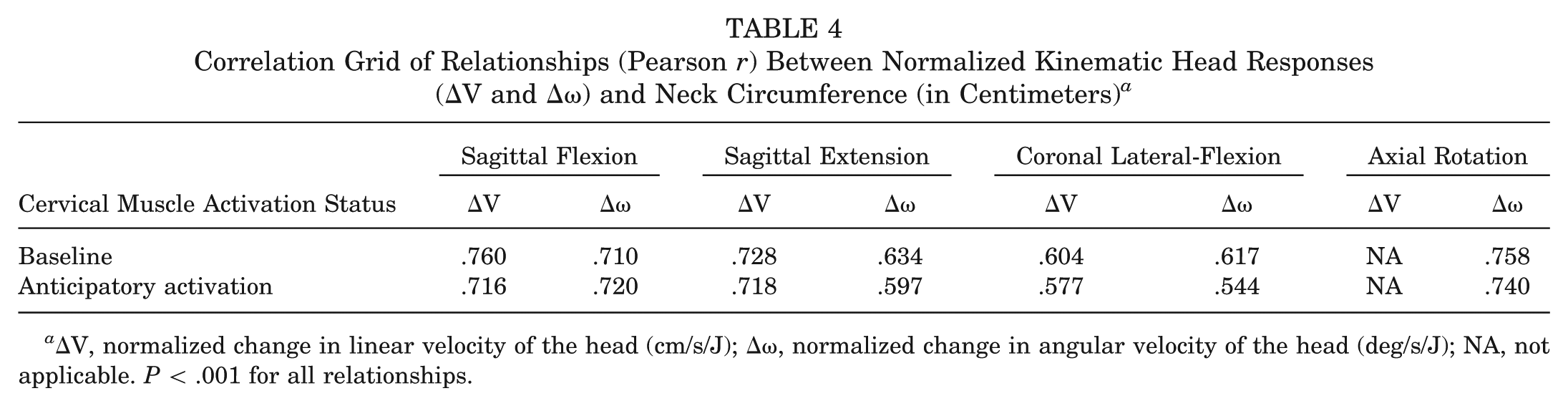
ΔV, normalized change in linear velocity of the head (cm/s/J); Δω, normalized change in angular velocity of the head (deg/s/J); NA, not applicable. P < .001 for all relationships.
Discussion
Our results support the theory that greater neck strength and anticipatory muscle activation are associated with an attenuated kinematic response to impulsive force(s) acting on an athlete’s head. This is consistent with prior work by Tierney et al 42 addressing dynamic head-neck stabilization in the sagittal plane, but the present study also assesses these relationships in coronal plane lateral flexion as well as axial plane rotation. This is significant because sport-associated head impacts in the real world occur in all planes of motion, and there is evidence to suggest that coronal plane lateral flexion may be more injurious than head motion primarily involving sagittal plane flexion and extension.15,35 In addition, the present study recruited athletes of both sexes from 8 to 30 years of age, while prior work was limited to an adult population. 42
Regarding the influence of neck strength (H1), the magnitude of the inverse relationship between neck muscle strength and ΔV and Δω fell between r = .417 and r = .657. The strength of these associations varied between the directions of motion and cervical muscle activation states. These values are generally considered moderately strong. 8 The applied forces and the associated head kinematic responses were, by design, well below those necessary to induce concussion. To our knowledge, the lowest magnitude of linear acceleration (the injury metric most commonly reported by in vivo impact sensing systems) associated with a concussive head impact measured in an athlete instrumented with HITS is 31.8 g, 31 and most concussions result from head impacts in the 90- to 150-g range. In contrast, the greatest linear acceleration recorded for any single trial during this study was 4.0 g. Assuming that these relationships hold true at greater impulse magnitudes, these results may indicate the neck’s protective role in controlling an athlete’s dynamic head response to sport-associated trauma and suggest that interventions aimed at increasing neck strength may reduce an athlete’s concussion risk. To date, only a single study has reported on the effects of a cervical resistance training program in a population of collegiate soccer athletes. 25 Additional research is necessary to investigate the effects of other training strategies and to include additional athlete populations. Recent epidemiological data also support the notion that greater neck strength may have a protective effect with respect to concussion. Indeed, as discussed in Gregory, 17 Comstock reported an inverse relationship between neck strength and concussion in a prospective study of 6704 high school athletes, independent of sex and sport.
Regarding the influence of cervical muscle activation (H2), we found that anticipatory activation to brace for impact significantly decreased ΔV and Δω. This independent effect was consistent across the spectrum of participants’ neck strength. This is not surprising given that the stiffness of striated muscle in tension is linearly proportional to its activation level and its isometric strength. 2 Based on this relationship, it would be expected that cervical muscle cocontraction should increase the neck’s resistance to head motion because of external forces. In this regard, our results are similar to those of Simoneau et al, 37 who used a similar impulsive loading apparatus to study the effect of preloading on neck stiffness and viscosity. This group found that decreased peak angular velocities of the head resulted during increased cervical muscle activation in response to preloading. Collectively, these studies suggest that “bracing for impact” may be an effective strategy for decreasing the risk of concussion associated with a sport collision by reducing the magnitude of postimpact head kinematics. Furthermore, these results suggest that “heads up” coaching and training strategies aimed at improving athletes’ sense of awareness of their surroundings and their anticipation of body collisions may be an effective means for improving player safety by facilitating cervical muscle activation to brace for impact. This is consistent with in vivo research by Mihalik et al 31 demonstrating that head impact magnitudes in pediatric ice hockey athletes were greater during unanticipated collisions, presumably because of the effect of bracing for impact.
In this study, we chose to vary the magnitude of the load applied to participants’ heads by the weight-drop apparatus in direct proportion to their body mass. This differs from prior studies employing similar impulsive loading techniques.25,37,42 This protocol decision was largely driven by participant safety considerations, especially in the pediatric athletes. Given the significant size heterogeneity among study participants, there was concern that the load magnitude required to generate sufficient head motion for kinematic analysis in the largest adult participants could be potentially injurious to the smaller pediatric participants. To account for the unequal impulsive load magnitudes between participants, we normalized the raw head kinematic outcome values by dividing ΔV and Δω by the magnitude of their causative impulsive loads. This is mathematically equivalent to scaling ΔV and Δω up to the values that would be expected to result if an equivalent impulsive load had been applied to all participants, assuming that neck stiffness lay in the linear portion of the force-displacement curve at the load magnitudes employed during this study. If the primary analyses are repeated using raw ΔV and Δω values without normalization for applied load magnitudes, significant main effects are still present for muscle activation state for both ΔV and Δω, and a significant, but weaker, main effect remains for muscle strength for Δω but not for ΔV.
We selected ΔV and Δω as the primary kinematic outcome variables in this study. There is a lack of consensus in the concussion biomechanics literature regarding the kinematic variable(s) most directly associated with injury, and there is still debate about the relative contributions of linear vs angular motion. 29 As such, many kinematics-based injury metrics exist, including peak linear and angular displacements, velocities, and accelerations of the head; integrated functions of the head’s linear acceleration over time (eg, Head Injury Criterion, Gadd Severity Index)12,44; and composite functions incorporating both linear and angular accelerations (eg, head impact power, weighted principal component score, combined probability of concussion).16,33,36 Given that both the linear and angular components of head motion appear to contribute to brain injury risk, and that our study protocol resulted in head motion with significant linear and angular components in flexion, extension, and lateral flexion, we elected to include both a linear and an angular kinematic outcome variable in our analyses. Peak linear velocity, ΔV, was selected as our linear kinematic metric because of its exponential relationship with the head injury criterion (HIC). 45 Because HIC, which has long been the standard brain injury criterion in the automotive industry, is proportional to ΔV of the head to the fourth power, small increases in ΔV may be associated with large increases in brain injury risk. Peak angular velocity, Δω, was selected as our primary angular kinematic metric because prior modeling work suggests that it is the single kinematic parameter most closely associated with brain tissue deformation patterns. 41 Because brain tissue shear strain, which results from tissue deformation, is thought to be the underlying mechanical parameter responsible for causing concussion, Δω is likely the best individual injury metric derived from angular head kinematics.
This study is not without limitations. Measuring neck muscle strength accurately is challenging, and potential error associated with this measurement is a limitation inherent to any research involving neck strength assessment. 11 While neck girth and strength are closely related, we suspect that neck muscle strength is the more important variable in terms of controlling the head’s dynamic response to impact. The stronger associations of ΔV and Δω with neck circumference than neck strength may reflect inaccuracies inherent to the measurement of neck strength. In our experimental apparatus, some inaccuracy may have resulted from incomplete stabilization of the torso during maximum isometric strength assessment. Although we tried to constrain the torso as well as possible, some degree of torso motion due to soft tissue and/or seat cushion displacement cannot be avoided. As a result, athletes could potentially accelerate their torso within the constraints of the stabilizing belt in the same direction as force measurement while maintaining the original head position to set up a phasic stretch of precontracted neck muscles (effectively “cocking” their head-neck segment), allowing them to significantly increase the force subsequently generated in those muscles. 5 While there is likely some measurement error associated with the neck strength values contained in this report, we think it is unlikely that the significant associations identified between neck strength and head kinematics are due to inaccurate neck strength measurements given the internal consistency of this finding across directions of motion and muscle activation states, as well as the external consistency of this finding with prior research, as previously described. Given anticipated difficulties with neck strength assessment, we also included neck circumference and a sonographic measure of sternocleidomastoid cross-sectional area in our study protocol as proxy measures for neck strength in our secondary analyses. While the sternocleidomastoids are responsible for most neck moment generation in forward flexion, they contribute to a much lesser degree during lateral flexion, axial rotation, and extension. 43 As such, future work should consider additional imaging methods to individually assess the morphology of the cervical muscles responsible for force generation in each direction.
Another study limitation is that we did not use electromyography to quantify the degree of muscle activation during the baseline and anticipatory cervical muscle activation conditions. While participants were required to demonstrate both neck activation conditions to the PI before testing and we confirmed differential neck muscle activation during the procedure by visual inspection, we cannot confirm that the degree of cervical muscle cocontraction during the anticipatory activation condition represented the athlete’s true maximum, nor can we quantify the degree of differential cervical muscle contraction between the baseline and anticipatory muscle activation conditions. We also did not use tetanic electrical stimulation of the muscles being tested during a maximum contraction because of the discomfort this would have imposed on participants. Nonetheless, on the basis of our observations during data collection, we are confident that participants achieved greater cervical muscle activation during the anticipatory activation condition than the relaxed baseline posture and that the lesser ΔV and Δω values observed during this condition represent a real effect. An additional limitation is that the order of testing was the same for all subjects. While randomizing the direction of load delivery for each trial would have minimized the potential for systematic bias due to a possible order or fatigue effect, this was impractical because of the logistics associated with setting up the testing apparatus and kinematic camera system for testing in each direction of head motion. Given the minimal physical demands associated with the study protocol, it is unlikely that a significant order or fatigue effect was present, but some bias is possible. Imperfect headgear fit is a final study limitation that merits discussion. While the headgear’s Velcro straps were adjustable and it is marketed as a “one-size-fits-all” product, the headgear fit was tighter for some participants than others. Our subjective impression was that the headgear tended to slip more in those participants whose heads were smaller and who had more hair, resulting in some relative headgear motion that was not directly coupled to the motion of the head. While not quantified, our subjective impression was that this generally resulted in greater headgear-to-head motion in the younger athletes and the female athletes, who tended to have more hair and smaller heads. Despite this subjective trend, younger and female athletes tended to have greater ΔV and Δω magnitudes. As such, the relationships between neck strength, anticipatory cervical muscle activation, and head kinematics in response to impulsive loading presented in this article may actually represent an underestimation of the true magnitude of these relationships, as greater relative headgear-to-head motion in those participants with smaller, weaker necks may have obscured the true effect sizes.
In conclusion, the results of this study suggest that greater neck strength attenuates the head’s dynamic response to external forces. These relationships hold true in all planes of head motion and across the age spectrum in athletes of both sexes. In addition, these results suggest that anticipatory cervical muscle activation acts independently from neck strength to further attenuate head kinematics in response to loading.
Footnotes
Acknowledgements
The authors thank Mr Mark Shafer and Mr Ryan Perkins for their contributions to the development of the impulsive loading device used in this study. They also thank Mr Andrew Schuldt for his assistance with initial participant screening and test scheduling.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.T.E. has declared a potential conflict of interest as specified in the AJSM Conflict of Interest Statement. He has received funding for this study through a K12 Career Development Award from the Rehabilitation Medicine Scientist Training Program (5K12HD001097).