
Abstract
Background:
During arthroscopic Bankart repair, inferior anchor placement is critical to a successful outcome. Low anterior anchors may be placed with a standard straight guide via midglenoid portal, with a straight guide with trans-subscapularis placement, or with curved guide systems.
Purpose/Hypothesis:
To evaluate glenoid suture anchor trajectory, position, and biomechanical performance as a function of portal location and insertion technique. It is hypothesized that a trans-subscapularis portal or curved guide will improve anchor position, decrease risk of opposite cortex breach, and confer improved biomechanical properties.
Study Design:
Controlled laboratory study.
Methods:
Thirty cadaveric shoulders were randomized to 1 of 3 groups: straight guide, midglenoid portal (MG); straight guide, trans-subscapularis portal (TS); and curved guide, midglenoid portal (CG). Three BioRaptor PK 2.3-mm anchors were inserted arthroscopically, with an anchor placed at 3, 5, and 7 o’clock. Specimens were dissected with any anchor perforation of the opposite cortex noted. An “en face” image was used to evaluate actual anchor position on a clockface scale. Each suture anchor underwent cyclic loading (10-60 N, 250 cycles), followed by a load-to-failure test (12.5 mm/s). Fisher exact test and mixed effects regression modeling were used to compare outcomes among groups.
Results:
Anchor placement deviated from the desired position by 9.9° ± 11.4° in MG specimens, 11.1° ± 13.8° in TS, and 13.1° ± 14.5° in CG. After dissection, opposite cortex perforation at 5 o’clock occurred in 50% of MG anchors, 0% of TS, and 40% of CG. Of the 90 anchors tested, 17 (19%) failed during cyclic loading, with a similar failure rate across groups (P = .816). The maximum load was significantly higher for the 3-o’clock anchors when compared with the 5-o’clock anchors, regardless of portal or guide (P = .021). For the 5-o’clock position, there were significantly fewer “out” anchors in the TS group versus the CG or MG group (P = .038). There was no statistically significant difference in maximum load among groups at 5 o’clock.
Conclusion:
Accuracy in suture anchor placement during arthroscopic Bankart repair can vary depending on both portal used and desired position of anchor. The results of the current study indicate that there was no difference in ultimate load to failure among anchors inserted via a midglenoid straight guide, midglenoid curved guide, or percutaneous trans-subscapularis approach. However, midglenoid portal anchors drilled with a straight or curved guide and placed at the 5-o’clock position had significant increased risk of opposite cortex perforation compared with trans-subscapularis percutaneous insertion, with no apparent biomechanical detriment.
Clinical Relevance:
The findings from this study will facilitate improved understanding of risks and benefits of several techniques for arthroscopic shoulder instability treatment with regard to suture anchor fixation.
Arthroscopic shoulder stabilization with suture anchors has become an accepted treatment option for management of anterior shoulder instability.1,6,10,31,35,37,46,47 In most cases of traumatic instability, a labral tear is present, which requires repair to the glenoid rim with suture anchors. § Multiple clinical studies have demonstrated favorable long-term outcomes after instability repair with suture anchor fixation.2,5,9,26,43-45 Despite a more evolved understanding of anterior shoulder instability, failure rates leading to repeat instability events are noted to be as high as 20% to 30% for patients after repair of both acute and recurrent instability.26,32,45 For example, Owens and colleagues recently reported on 40 shoulders undergoing arthroscopic Bankart repair with suture anchors for acute (primary) anterior shoulder dislocations. With an average 11.9 years of follow-up, the authors reported a 14.3% recurrent dislocation rate and a 21% recurrent subluxation rate. 26 Similarly, van der Linde et al 45 reported on 70 shoulders undergoing arthroscopic Bankart repair for traumatic recurrent anterior instability with suture anchors and noted a recurrence rate of 35% after 8 to 10 years after surgery. Such failure rates are clearly problematic, especially given the relatively young average age composing the majority of this patient population.
Given that the typical zone of injury in the setting of anterior instability is in the anterior-inferior glenoid quadrant, the zone of injury is between 3 and 6 o’clock (for a right shoulder). 36 For adequate repair, it is critical for the surgeon to achieve inferior anchor placement to address the inferior component of traumatic instability. The standard midglenoid portal, however, can pose difficulty in permitting adequate low anterior-inferior anchor placement. This may be due to the obliquity of the approach, which may ultimately lead to anchor blowout.
Alternative portals and curved drill guide systems have been described to improve inferior anchor placement. The majority of technical articles on arthroscopic Bankart repair describe suture anchor placement with a straight guide through a standard midglenoid portal (above the subscapularis tendon). Other portals, including the percutaneous 5-o’clock trans-subscapularis portal and the 7-o’clock portal, have been advocated to provide more consistent placement of inferior anchors on the glenoid.20,29 These portals allow for a more perpendicular trajectory for pilot hole preparation and subsequent suture anchor placement. More recently, curved guide systems have been developed to facilitate such inferior anchor placement.
To date, there is a paucity of data available evaluating anchor placement accuracy with regard to both portal and guide choice. This information would be useful in clinically guiding orthopaedic surgeons in their choices of portal and guide utilization in the setting of anterior shoulder instability repair. It is unknown if insertional techniques affect the biomechanical performance of the anchor and, further, whether the anchor remains in bone after insertion. Finally, it is unknown if the surgeon’s intended anchor placement (eg, 3 o’clock) is affected by portal and/or guide choice. The purpose of this study, therefore, is to evaluate initial biomechanical performance of a conventional glenoid anchor and risk of opposite cortex penetration as a function of portal used and type of guide chosen (straight vs curved). The hypothesis of this study is that use of an accessory trans-subscapularis portal or curved drill guide system will improve low anterior-inferior anchor position and result in improved initial biomechanical properties with lower risk of opposite cortex perforation.
Materials and Methods
This study was classified as exempt from our university’s Institutional Review Board. Thirty fresh-frozen human cadaveric shoulders (90 anchors) underwent quantitative computed tomography scans to assess bone mineralization. The bone mineralization data were used to allocate specimens to 1 of 3 test groups—straight guide via midglenoid portal (MG), straight guide via trans-subscapularis portal (TS), and curved guide via midglenoid portal (CG)—such that there was no difference in bone mineralization among the groups (P = .93). The specimens had an average age of 50.6 years (range, 28-64 years). The average bone mineralization as determined by quantitative computed tomography scan of all specimens was 266.4 ± 158.5 HU (Table 1). There were 13 left shoulders and 17 right shoulders.
Demographic Group Results a
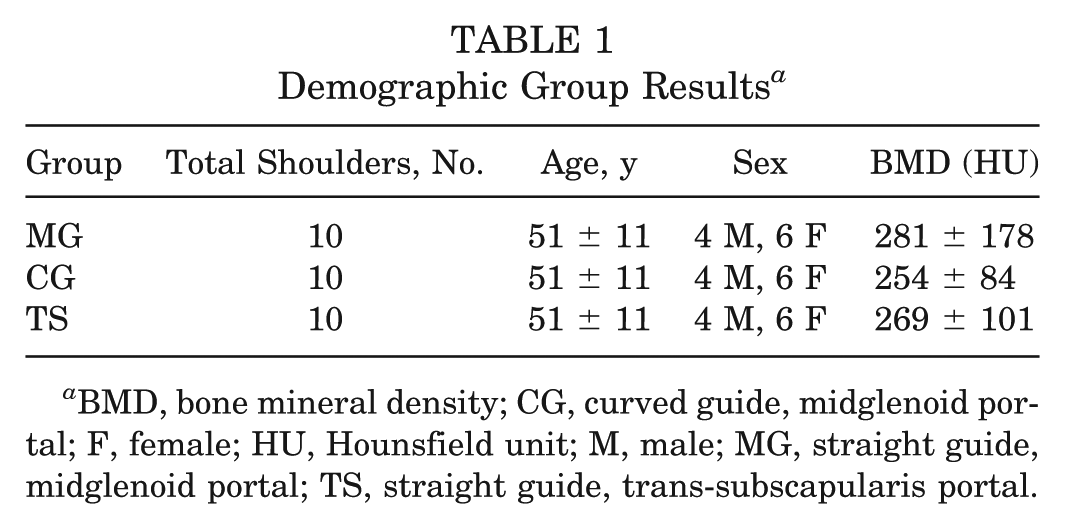
BMD, bone mineral density; CG, curved guide, midglenoid portal; F, female; HU, Hounsfield unit; M, male; MG, straight guide, midglenoid portal; TS, straight guide, trans-subscapularis portal.
All shoulders were then thawed to room temperature and examined arthroscopically by the senior author (N.N.V.). Each shoulder was secured with a shoulder clamp on the extremity holder, placed in the lateral decubitus position, and set in longitudinal and lateral traction (10 lb) with the shoulder abducted to 35° and forward flexed to 20°. The arthroscopic fluid ran continuously from the sink with a pressure equivalent to approximately 30 mm Hg. Specimens subsequently underwent suture anchor placement by the senior author (see videos 1-3 of the online supplement). Three BioRaptor 2.3-mm PK anchors (Smith & Nephew Inc, Andover, Massachusetts, USA) were inserted arthroscopically in each glenoid surface using 1 of 3 approaches: MG, TS, or CG. Three anchors were placed for each specimen to achieve the following positions: 3, 5, and 7 o’clock. For all specimens, the 7-o’clock anchor was placed with a straight guide via an accessory percutaneous posterior-inferior portal (Figure 1). Anterior anchor placement was achieved while viewing from a standard posterior portal, while posterior-inferior anchor placement was achieved while viewing from an anterior-superior portal.

Location of the accessory posterior-inferior portal placed at 7 o’clock, used for percutaneous anchors via a straight guide.
Pilot hole preparation was performed with a power drill and anchor guide per the manufacturer’s recommendations. Anchors were then impacted into position via the drill guide. The anchors were placed as close as possible to the chondrolabral junction. No labral tear was created. Viewing was from the posterior-superior portal, and the portals were placed under direct visualization with an outside-in technique, localizing with a spinal needle first. The standard midglenoid portal was superior to the subscapularis, in the rotator interval, and an 8.25-mm cannula was utilized for the anchor placement. For the 5-o’clock position (trans-subscapularis approach), a spinal needle was used to localize a trajectory perpendicular to the desired 5-o’clock position on the glenoid face. A stab incision was then made in the skin approximately 1.5 cm inferior to the location of the midglenoid portal and lateral to the conjoined tendon,7,20,29 and the anchor guide with a sharp-tip trocar was used to penetrate the subscapularis; after which, the anchor was placed in a standard fashion. No cannula was used in this position. The 7-o’clock portal was created approximately 4 cm distal to the posterolateral corner of the acromion to access the inferior and posterior quadrants of the glenohumeral joint. The 7-o’clock anchor was placed with a similar percutaneous insertion technique.
After arthroscopic anchor placement, specimens were dissected down to the glenoid-scapula construct, with the humerus, clavicle, and soft tissues removed. Gross visualization of anchor perforation of the opposite cortex was documented (Figure 2). An “en face” method was used to evaluate the actual position of each anchor on a clockface scale via a goniometer. Anchor position was evaluated relative to its position on the clock, and any deviation from intended position was recorded (eg, anchor placed at 3:30 instead of the desired position of 3 o’clock). Clockface deviations were then converted to degrees with a 360° scale, with 1 hour of deviation corresponding to 30°. Two independent observers (blinded from each other’s data) measured all anchor positions in all specimens; results from both observers were averaged.
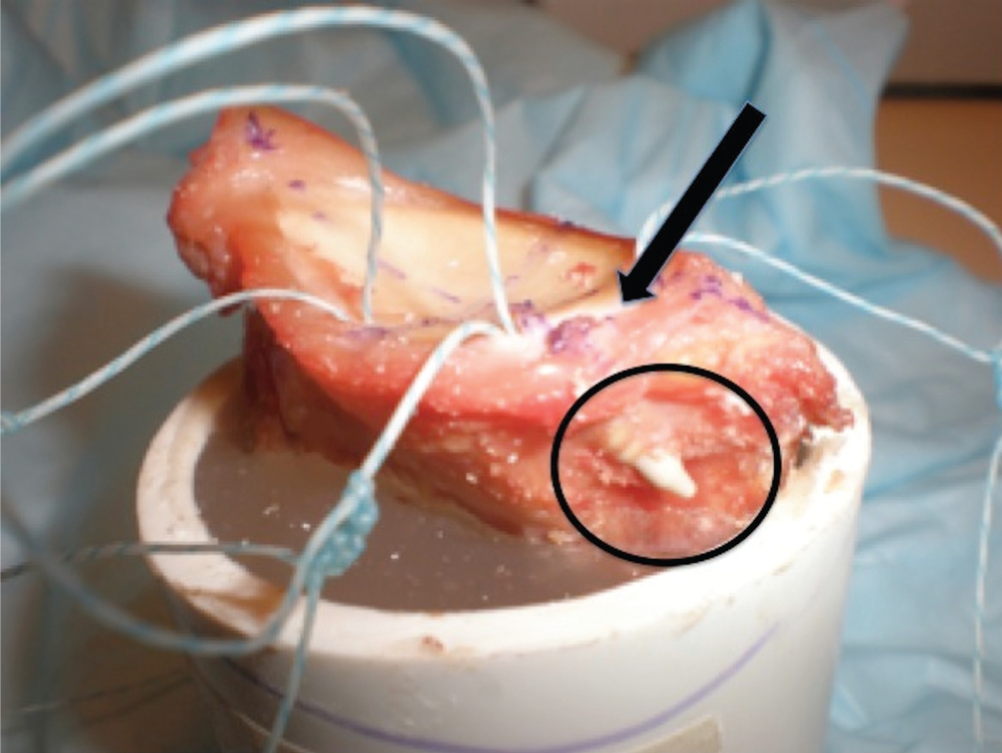
Demonstration of opposite cortex anchor perforation (“out” anchor). The arrow indicates the anchor insertion site, while the circle demonstrates anchor perforation through the opposite cortex.
Each specimen was then mounted in a materials testing system (MTS Insight 5; MTS Inc, Eden Prairie, Minnesota, USA) via a previously described technique.23,24,31 The glenoid was separated from the remainder of the scapula by sawing from 1 cm below the infraglenoid ridge along the infraspinatus fossa in a medial direction, then by cutting along the medial border of the scapula just under the spine. Each specimen was potted in dental acrylic (Isocryl; Lang Dental, Wheeling, Illinois, USA) so that the glenoid fossa was parallel with the surface of the potting container. The potted glenoid was placed in a custom-made adjustable jig that was fixed to the platform of the MTS. The No. 2 Ultrabraid sutures (Smith & Nephew Inc) from the suture anchors fixated in the glenoid rim were tied in a 5-cm loop with 5 alternating half-hitch arthroscopic knots. This loop was placed around a stainless-steel 4-mm horizontal cross-pin attached to a custom clamp, in line with a 1000-N load cell. The angle of pull for the 3- and 5-o’clock suture anchors was positioned such that the loading vector was directed in a 45° anteroinferior direction, aimed at re-creating the in vivo dislocation vector. The angle of pull for the 7-o’clock anchor position was in line with the trajectory of the anchor.
For each shoulder, each anchor was tested individually via a random sequence. Each anchor (3, 5, and 7 o’clock) was preloaded to 10 N for 2 minutes, cyclically loaded from 10 to 60 N at 1 Hz for 250 cycles (increased at an incremental rate of 5.0 mm/s), and subsequently loaded to failure at 12.5 mm/s. Specimens were regularly moistened with a saline mist spray during testing. For all specimens, MTS TestWorks 4 software (MTS Inc) was used to record maximum failure load (N). Gross method of failure was recorded.
Based on published data from a similar methodology, 24 a power analysis was performed before initiation of the study. For a statistical power of 80% with significance set at 0.05 (α) according to an effect size of 1.3, 10 specimens per group were required to detect differences in maximum load (10% difference). For data analysis, mixed effects regression models were fit to compare maximum failure loads across testing conditions, as well as between “out” versus “in” anchors with regard to maximum failure load. Fisher exact test was used to evaluate the categorical data, including anchor perforation rates and failure rates. For interobserver reliability of the anchor clockface measurements, the intraclass correlation coefficient was calculated. Statistical significance was assumed for P < .05.
Results
Mode of Failure
All anchors that survived cyclic loading failed via anchor pullout (Table 2). All anchors that failed during cyclical loading also failed via anchor pullout, with an average failure at cycle number 56 of 250. Of the 90 anchors tested, 17 failed during cyclical loading (19%). No statistically significant differences were noted among the 3 groups with regard to the number of failures sustained during cyclical loading (P = .816). At the 3-o’clock position, 3 of 30 (10%) anchors failed during cyclical loading (MG, 0; TS, 1; CG, 2). At the 5-o’clock position, 7 of 30 (23%) anchors failed during cyclical loading (MG, 3; TS, 3; CG, 1).
Biomechanical Results by Group a
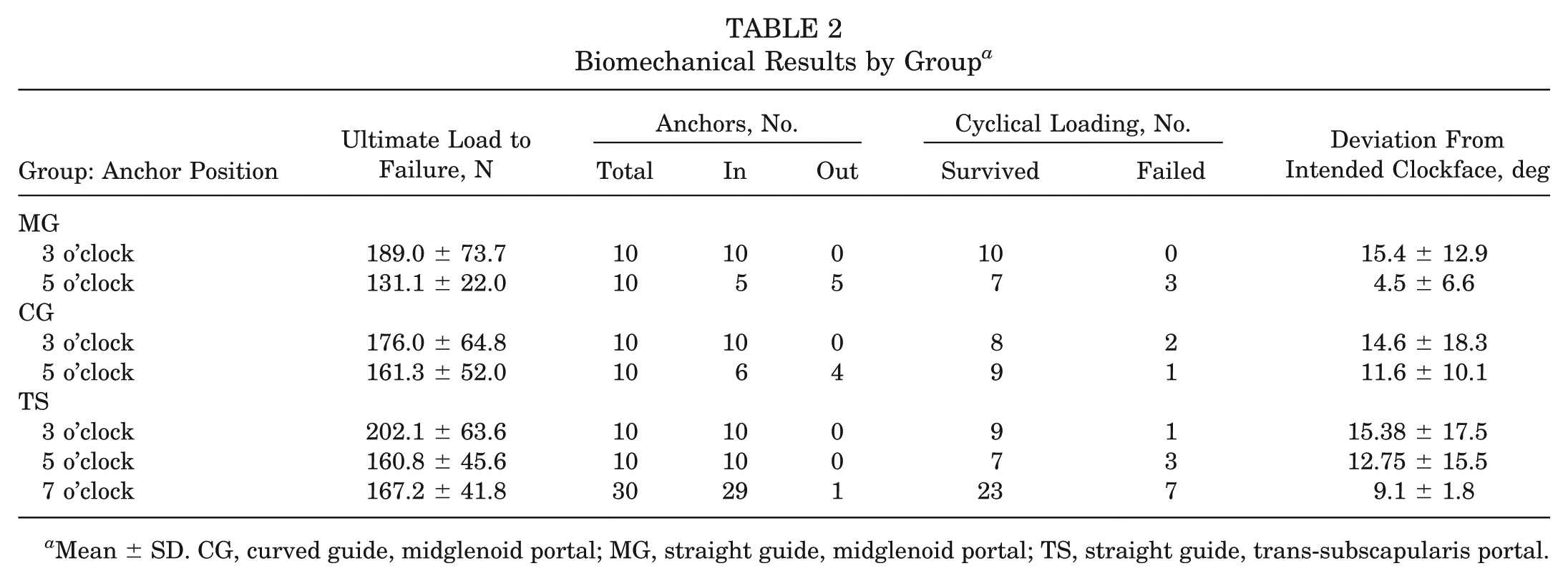
Mean ± SD. CG, curved guide, midglenoid portal; MG, straight guide, midglenoid portal; TS, straight guide, trans-subscapularis portal.
Maximum Failure Load
The mean maximum failure load of the specimens that completed the entire protocol (n = 73) was 170.7 ± 54.2 N. The maximum load of the specimens in the MG group was 189.0 ± 73.7 N at 3 o’clock and 131.1 ± 22.0 N at 5 o’clock. The maximum load of the specimens in the TS group was 202.1 ± 63.6 N at 3 o’clock and 160.8 ± 45.6 N at 5 o’clock. The maximum load of the specimens in the CG group was 176.0 ± 64.8 N at 3 o’clock and 161.3 ± 52.0 N at 5 o’clock. Finally, the maximum load at the 7-o’clock position was 167.2 ± 41.8 N (all were performed via a percutaneous approach with straight guide). There was no statistically significant difference in maximum load among the groups at 5 o’clock (P = .602). Overall maximum load was significantly higher in the 3-o’clock anchors than the 5-o’clock anchors in all 3 groups (P = .021), regardless of portal or guide (Figure 3). Specifically, maximum load was estimated to be 37.7 N greater in the 3-o’clock position compared with the 5-o’clock position (P = .021; 95% confidence interval: 5.6, 69.8).
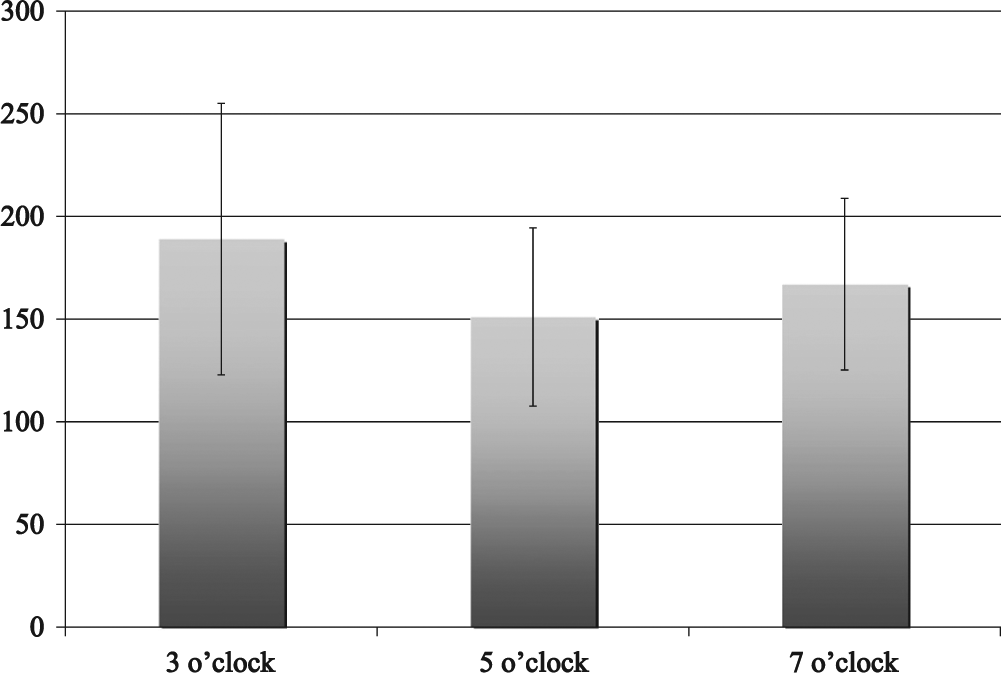
Maximum failure load results plotted by position (3, 5, and 7 o’clock). Overall maximum load was significantly higher in the 3-o’clock anchors than the 5-o’clock anchors in all 3 groups (P = .021), regardless of portal or guide.
Anchor Placement Accuracy (Perforation)
After dissection, a total of 80 anchors were classified as “in,” while 10 anchors were classified as “out,” with regard to perforation of the opposite cortex (Figures 2, 4). At the 3-o’clock position, 100% of anchors were found to be “in.” At the 5-o’clock position, 5 of 10 anchors were “out” in the MG group, and 4 of 10 were “out” in the CG group; significantly fewer anchors (0 of 10) were “out” in the TS group (P = .038). In the 7-o’clock position in the TS group, 1 anchor was found to be “out,” while the remaining 29 were deemed “in.” Finally, regardless of technique, there was no anchor intersection among any of the groups, as determined by gross visual inspection. No significant difference in ultimate load to failure or failure during cyclic loading was noted among anchors contained in the glenoid vault versus those that perforated opposite cortex at any position (P = .287).
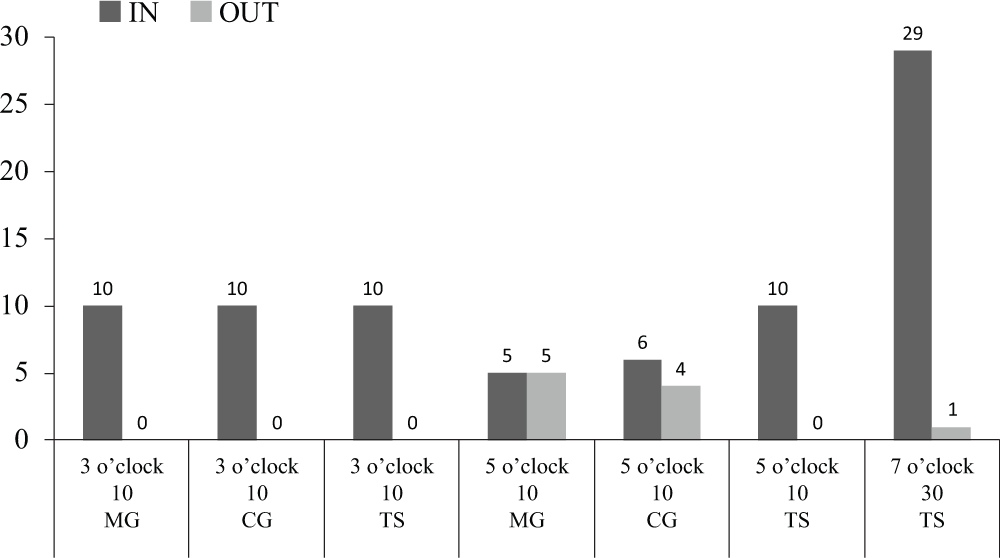
Graph demonstrating the distribution of anchors “out” versus “in.” Overall, 10 of 90 anchors were classified as “out,” and 9 of 10 occurred at the 5-o’clock position, with no perforations occurring at the 3-o’clock position.
Clockface Measurements
The intraclass correlation (r) coefficient for the 2 independent observers measuring deviation from the intended anchor position on the clockface for all positions was 0.932. Overall, for all positions and for all approaches, anchor insertion on the clockface deviated from the intended position by an average of 11.3° ± 13.4°. There was no statistically significant difference in clockface accuracy among the 3 groups: CG, 13.1° ± 14.5°; MG, 9.9° ± 11.4°; TS, 11.1° ± 13.8° (P = .749). There was also no statistically significant difference in clockface accuracy among the intended anchor positions for all groups: 3 o’clock, 15.1° ± 15.9°; 5 o’clock, 9.6° ± 11.6°; and 7 o’clock, 9.1° ± 11.8° (P = .151). Finally, there was no statistical difference among any of the subgroups in clockface deviation, as noted in Table 2 (P = .43).
Discussion
The principal findings of this study suggest that there was no difference in ultimate load to failure among anchors placed via a midglenoid approach with a straight or curved guide or percutaneous guide via a trans-subscapularis approach. Furthermore, there was no statistical difference in deviation of intended clockface position among any of the groups at any of the positions. However, anchors placed via a trans-subscapularis approach had a significantly decreased risk of opposite cortex perforation compared with either guide (curved or straight) used via midglenoid position. In addition, anchors placed in the 3-o’clock position are biomechanically stronger with statistically significantly higher loads to failure compared with anchors placed in the 5-o’clock position. As noted by Roth et al, 34 glenoid rim cortical thickness decreases from 2 to 6 o’clock; thus, the thicker cortical bone at the 3-o’clock position may provide better fixation.
Arthroscopic management of anterior shoulder instability is an accepted surgical technique with good to excellent clinical outcomes. Nevertheless, despite advances in implant design and techniques, the risk of recurrence remains, with rates reported as high as 20% to 30%.26,32,45 As discussed earlier, potential reasons for failure may be attributable to patient-related factors, technical factors, and anatomic factors. Previous studies have noted that placement of fewer than 3 anchors may be associated with increased risk of instability. 32 The surgeon’s ability to place multiple anchors and achieve appropriate capsular tension is predicated on the ability to place the first anchor low on the anterior-inferior glenoid rim. 32
Technical demands of suture anchor placement include inferior placement on the glenoid face and with the proper trajectory to achieve stable fixation without damaging the articular surface. Clinically, the standard midglenoid portal may pose difficulty in achieving adequate low anterior-inferior anchor placement, possibly because of the obliquity of the approach. In the present study, however, no differences were found with regard to anchor placement accuracy regardless of intended position or approach used. Lim and colleagues 18 performed a biomechanical study assessing opposite cortex perforation of anchors placed via the anteroinferior portal at the clockface positions of 4:00 and 5:30 to 6:00 and noted a high risk of perforation with insertion of the inferior anchors. The authors found no difference between the 2 anchor positions in ultimate failure strength after cyclical loading. 18 Alternative portals, including the 5-o’clock trans-subscapularis portal and the 7-o’clock portal, have been advocated to provide more consistent placement of inferior anchors on the glenoid.20,29 The results of the current study indicate that there was no difference in ultimate load to failure among anchors inserted via a midglenoid straight guide, midglenoid curved guide, or percutaneous trans-subscapularis approach. However, midglenoid portal anchors drilled with a straight or curved guide and placed at the 5-o’clock position had significant increased risk of opposite cortex perforation compared with trans-subscapularis percutaneous insertion with no apparent biomechanical detriment.
The implications, if any, of opposite cortex perforation remain unclear. While anchors placed via a percutaneous approach had a significantly decreased risk of opposite cortex perforation compared with either guide used via midglenoid position, the biomechanical performance of the “out” versus “in” anchors was not significantly different. Perforation with drill or anchor may place at risk anatomic structures such as the axillary nerve. Further factors that may influence anchor performance and require additional evaluation include percentage of anchor within bone, size of anchor, length of anchor, and anchor material. In addition, while there is a potential benefit of less cortex perforation by anchor placement via the trans-subscapularis portal, the risks associated with using this portal must be considered. Specifically, the axillary nerve and cephalic vein are at risk during placement of this portal. 21 As with all shoulder surgery, the neurovascular status of the patient must be assessed after the procedure, particularly in the distribution of the axillary nerve. Given the described technique, with spinal needle localization and blunt entry of the trocar into the capsule, we believe that the risk to the nerve or vascular structures is minimized.13,19,33,36 Finally, while rare, open approaches to the anterior shoulder can place both the upper and lower subscapular nerves at risk for injury. 16 To date, however, there have been no reports of injury to these specific nerves during arthroscopic placement of a trans-subscapularis portal.
In addition, while arthroscopic anchor placement is minimally invasive, anchor placement itself requires the creation of multiple holes within the glenoid rim, most often in a linear arrangement. Given multiple cortical perforations, a stress riser can be created within the glenoid rim, and reports of glenoid rim fracture after redislocation after arthroscopic stabilization have been described.3,12 As noted elegantly in these case reports,3,12 various factors related to the anchors, including size, composition, and number used, may play a role in the creation of stress risers, but ultimately anchor configuration/insertion may be a significant factor as well. An additional potential risk may be bicortical versus unicortical drill penetration during anchor insertion.
Despite the relatively close position of anchors placed during arthroscopic stabilization, we did not find any case of anchor intersection within the glenoid vault or anchor destabilization by adjacent anchor placement. In designing the study, we elected to place a 7-o’clock anchor, which we commonly use for posterior-inferior capsular plication or labral repair during anterior stabilization. The purpose of including the 7-o’clock anchor was to assess if there was any intersection of anchors within the glenoid vault when placing anchors at both 5 and 7 o’clock via each technique. In such situations, if anchor intersection during anchor drilling occurred, anchor loosening may occur. As stated in our results, we did not see any anchor intersection with any technique that would influence choice of drilling technique for a 5-o’clock anchor when simultaneous placement of a 7-o’clock anchor is undertaken. Overall, our results suggest minimal risk of anchor intersection regardless of technique chosen. However, our results are specific to the anchor used during this study, based on drill and anchor length and diameter.
Suture anchors themselves have been associated with several significant complications, including glenoid rim fracture, osteolysis, enlargement of drill holes, infection, articular cartilage damage, and stiffness, among others. ‖ In a biomechanical analysis of suture anchor performance in the glenoid, Barber and colleagues 4 analyzed 8 matched pairs of human cadaveric glenoids with an average age of 54 years. The authors used 7 suture anchors inserted in rotation on clockface of the glenoid: 12:00, 1:30, 3:00, 4:30, 6:00, 7:30, and 9:00 (right shoulder). Before pull-to-failure testing, the authors cycled their specimens for 500 cycles at 10 to 60 N and found that 44% of anchors failed during cyclical loading. This is in contrast to our study, in which 19% failed during cyclical loading.
Koulalis et al 17 performed a basic science study in an effort to determine the role of a navigation system in improving the accuracy of glenoid anchor positioning in cases of anterior instability. The authors used plastic shoulder models and compared insertion angles of 3 suture anchors as performed by surgeons with and without the use of computer navigation. Interestingly, the authors did report a statistically significant difference among the groups, favoring the navigation group, with regard to anchor placement accuracy. However, the authors noted that there was likely no significant clinical advantage over the freehand technique. 17
There were several limitations to the present study. As with any cadaveric study, this was a “time zero” ex vivo model, and there was no opportunity for anchor-bone healing to occur. Thus, the results from this study may differ from what occurs in an in vivo setting. In addition, despite visually and arthroscopically inspecting each specimen to ensure that it was free of glenohumeral articular cartilage disease, it is unknown whether the specimens had any history of osseous disorders that may have influenced anchor pullout strength. However, in the present study, specimens were distributed into different experimental groups of similar bone mineral density to minimize the potential confounding effect of bone density. The average age of our specimens (50.6 years) was somewhat older than the patient population that might undergo instability repair and, as such, may have worse bone quality and be more likely to fail at lower biomechanical loads. However, as bone mineral density was similar among all 3 groups, the age of the specimens is unlikely to affect the overall results in this study. Finally, the study analyzed an intact glenoid, whereas various degrees of bone deficiency may be encountered in clinical cases of instability. The effect of bone loss on the reported results can be examined in future studies. It should also be noted that some anchors, such as the 3-o’clock anchors in the TS group, were inserted in such a way that may not reflect actual clinical practice, as the TS portal is more commonly utilized for inferior anchor placement’ (eg, 5 to 6 o’clock) as opposed to more anchors placed more superiorly on the glenoid.7,20,29
Our results suggest that comparable anchor positioning within the cortical glenoid bone can be achieved via multiple different techniques. For all approaches, anchor insertion on the clockface deviated from the intended position by an average of 11.3° ± 13.4°. The clinical implications of placing anchors up to 25° off from their intended position are still unclear. Overall, while the hypothesis was not confirmed—namely, that use of an accessory trans-subscapularis portal or curved drill guide system would improve low anterior-inferior anchor position and result in improved initial biomechanical properties—there was a lower risk of opposite cortex perforation via the percutaneous trans-subscapularis approach. Thus, while biomechanical performance is similar, the risk of cortical perforation can be decreased by use of a percutaneous trans-subscapularis approach. The findings from this study will facilitate improved understanding of arthroscopic shoulder instability treatment with regard to suture anchor fixation. Overall, percutaneous anchor insertion at the 5-o’clock position may be preferred over midglenoid portal anchors drilled with a straight or curved guide. Clearly, the potential reasons for recurrent instability after suture anchor fixation are multifactorial. Patient factors, biological factors, and surgeon factors are all likely to contribute.
Footnotes
Acknowledgements
The authors acknowledge Theodore Karrison, PhD: statistician.
Presented at the interim meeting of the AOSSM, Chicago, Illinois, March 2013.
One or more of the authors has declared the following potential conflict of interest or source of funding: Anchors for this study were donated by Smith & Nephew. Nikhil N. Verma, MD, is on the Smith & Nephew Shoulder Advisory Board and the Vindico Medical Board; receives royalties from Smith & Nephew; is a paid consultant for Smith & Nephew; receives research support from Major League Baseball and the Arthroscopic Association of North America; has stock in Omeros; received other financial support from Arthrex, Smith & Nephew, Ossur, and Linvatec. This author, their immediate family, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article. Anthony A. Romeo, MD, receives royalties from Arthrex Inc; is on the speakers bureau for Arthrex Inc; is a paid consultant for Arthrex Inc; receives research support from Arthrex Inc, DJO Surgical, Smith & Nephew, and Ossur; received other financial support from Arthrex Inc and DJO Surgical; receives publishing royalties from Saunders/Mosby-Elsevier; serves on the editorial board for the Journal of Shoulder and Elbow Surgery and SLACK Incorporated; and serves as a board member for the American Orthopaedic Society for Sports Medicine, the American Shoulder and Elbow Surgeons, the Arthroscopy Association of North America, and Techniques in Shoulder and Elbow Surgery. All authors declare no relevant financial conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.