
Abstract
Background:
The return-to-sport and reinjury rates are not well defined after revision anterior cruciate ligament (ACL) reconstruction.
Hypothesis:
School-age athletes would have a higher rate of return to sports and reinjury to either knee after revision ACL surgery compared with college or recreational athletes.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Patients were prospectively studied after revision ACL reconstruction with bone-patellar tendon-bone (BPTB) autograft. Participants were grouped by competitive sport levels of school age (mean age, 16.6 ± 0.9 years; n = 84), college (19.6 ± 1.2 years; n = 58), or recreational adult (27.6 ± 4.1 years; n = 117). An activity survey was used to determine the specific sport and sport level patients participated in before and after surgery. The International Knee Documentation Committee (IKDC) knee survey and Cincinnati Knee Rating System (CKRS) survey responses were also obtained.
Results:
The rate of return to the same sport at the same level was 62 of 84 school-age athletes (74%), 43 of 58 college athletes (74%), and 73 of 117 recreational athletes (62%) (P = .1065). The number of patients who had a subsequent ACL graft tear rate after revision surgery was 2 of 84 (2.3%) in the high school group, 3 of 58 (5.1%) in the college group, and 4 of 117 (3.4%) in the recreational group (P = .6706). The number of patients who had a subsequent ACL tear in the contralateral knee was 1 of 84 (1.1%) in the school-age group, 1 of 58 (1.7%) in the college group, and 2 of 117 (1.7%) in the recreational group (P = .9501). At 2 years postoperatively, the mean IKDC subjective total score was 86.1 ± 11.7 points and the mean CKRS total score was 89.7 ± 11.1 points.
Conclusion:
Revision ACL reconstruction with BPTB autograft and perioperative rehabilitation allowed high school and college athletes to return to sports at the preinjury level at a rate of 74%; the return rate for recreational-level adults was 62%. Reinjury rates in the first 5 years after revision surgery ranged from 2% to 5%, which is lower than what has been reported for young competitive athletes after primary surgery.
Anterior cruciate ligament (ACL) reconstruction is a common surgical procedure in competitive athletes at the high school and collegiate levels. Given their young age, active lifestyle, and risk of future instability episodes, these athletes are considered ideal candidates for ACL reconstruction. However, return to the previous level of competition after surgery is not a certainty, with some series reporting return-to-sport rates from 50% to 75% after primary ACL reconstruction.4,11 Furthermore, young competitive athletes and athletes returning to strenuous activities are the highest risk with regard to reinjury to either the reconstructed ACL graft or the contralateral ACL. 18 Shelbourne et al 18 reported reinjury rates to either knee for all patients within 5 years after ACL surgery and found that 5.3% tore their contralateral ACL, while 4.3% retore their surgically reconstructed ACL graft. Young athletes younger than 18 years, however, had higher rate of reinjury to either knee, with an incidence of 17.4%. Salmon et al 16 found a similar difference in reinjury rates based on International Knee Documentation Committee (IKDC) activity levels with an overall injury rate of 18% to either knee for patients who returned to level I or II (strenuous or moderate activities) versus a 5% rate for patients who returned to level III or IV (light or sedentary) activities.
Despite the recent literature focus on return to sports as well as reinjury rates in primary ACL reconstruction, these same parameters are not well defined for revision ACL reconstructions, specifically in competitive high school and collegiate athletes. Reinhardt et al 14 reported the first series on return-to-sports rates for competitive athletes younger than 18 years after revision ACL reconstruction and found that only 50% of patients were able to return to their preinjury level of sports. However, their graft choice was allograft tissue in more than half of the patients. Allograft reconstructions have shown higher failure rates in primary ACL reconstruction in multiple studies.1,6,13,23 The effect of allograft tissue on reinjury rates and return to sports is unknown. It is possible that the use of an autogenous bone-patellar tendon-bone (BPTB) graft may improve outcomes with regard to return to sports and risk of subsequent ACL reinjury.
It is possible that return-to-sports rates will be lower after revision compared with primary ACL reconstruction. Reinjury rates may be higher among young athletes after revision ACL surgery compared with primary surgery. The purpose of this study was to determine the rate of return to competitive sports after revision ACL reconstruction with BPTB autografts in young, competitive high school and college athletes and recreational athletes. Furthermore, we sought to determine the reinjury rates within 5 years of revision reconstruction to either the reconstructed knee or the contralateral knee. We hypothesized that school-age athletes would have a higher rate of return to sports and higher rate of reinjury to either knee after revision ACL surgery than college or recreational athletes.
Methods
From 1994 to 2007, a total of 3267 patients underwent ACL reconstruction and were enrolled into a prospective study to evaluate outcomes after surgery. The study was approved by the institutional review board at our institution, and informed consent or assent forms were obtained from patients. Of 3267 total patients, 378 underwent revision ACL reconstruction. Inclusion criteria for this study was that the patient was involved in pivoting, twisting, or jumping sport and that the patient had the desire to return to the same sport at the same level after surgery. A subjective activity survey was used prospectively beginning in 1998 to determine what specific sport and sport level patients participated in before and after surgery. 19 The survey asked patients what sport(s) they were participating in and at what level. The same information was abstracted from patient charts for patients before 1998. Patient charts were also reviewed to verify individual goals for returning to sports, confirm that school-age and college-age patients were involved with the schools’ competitive teams, and verify return-to-sport data. Patients were divided into age groups that would capture specific sport competition levels: <17.9 years for school-age competition, 18 to 21.9 years for college-age competition, and ≥22 years for recreational adult competition.
Of the 378 patients who underwent revision ACL surgery, 302 patients met the criteria for the study and we had follow-up data on 259 patients (86%) (Figure 1.) The desired sport activity for each age group was predominantly basketball, soccer, football, and volleyball (Table 1).
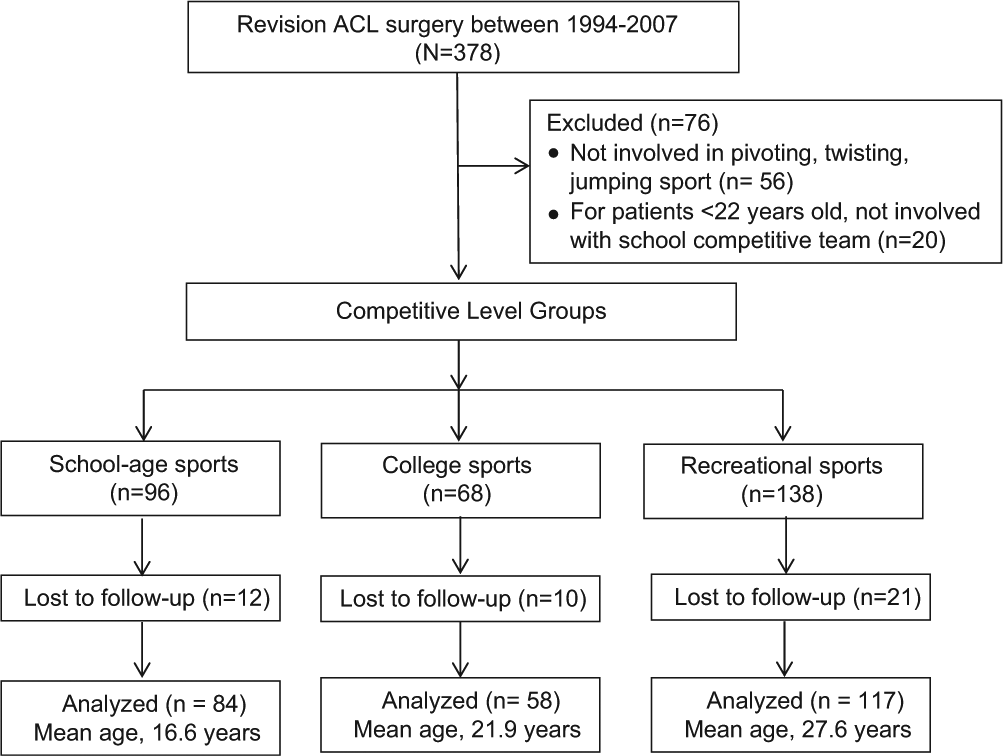
CONSORT flow diagram.
Sports Activity by Competitive Sport Group a
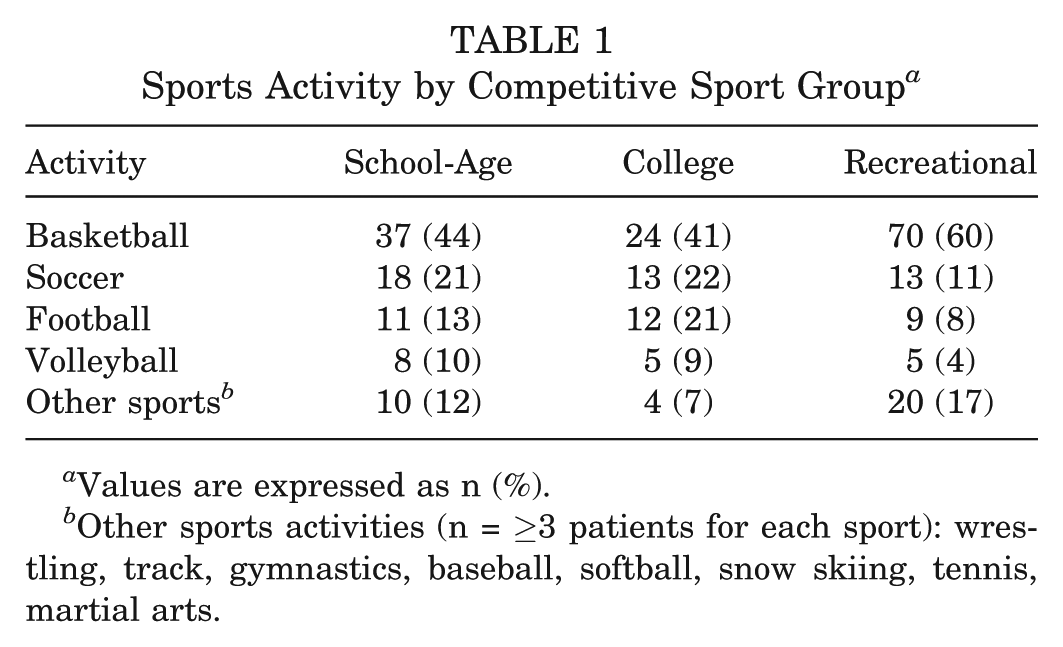
Values are expressed as n (%).
Other sports activities (n = ≥3 patients for each sport): wrestling, track, gymnastics, baseball, softball, snow skiing, tennis, martial arts.
The graft sources used for primary ACL reconstruction was patellar tendon autograft for 210 patients, hamstring graft for 18 patients, and allograft for 11 patients. Nine patients had an ACL repair procedure and 11 patients had an extra-articular procedure.
Patients underwent revision ACL reconstruction with BPTB autograft from either the ipsilateral (n = 122) or contralateral (n = 134) knee with an open mini-arthrotomy technique and button fixation, as described previously.20,21 All patients underwent a perioperative rehabilitation program that emphasized obtaining full range of motion, no swelling, and good quadriceps muscle control before surgery. Postoperatively, rehabilitation emphasized limiting a hemarthrosis, obtaining full knee range of motion, and achieving good quadriceps muscle control before participating in an aggressive strengthening and functional progression program. 17
A specific timeframe for returning to sports was not given to patients. Instead, specific guidelines were prescribed for the progression to return to activities. Once full knee range of motion and limited swelling was obtained, leg strengthening exercises were prescribed to achieve symmetry between knees. If one leg was significantly weaker than the other leg, single-leg strengthening exercises were emphasized. Patients were given a goal of side-to-side difference in quadriceps strength to be less than 15%, at which time they could return to competition gradually. Athletes were advised to participate in team drills and competition every other day at first to minimize swelling and to maintain full knee range of motion and minimal soreness.
As per the protocol of the study, patients were asked to complete subjective surveys postoperatively at 6 months, 1 year, and yearly thereafter. Subjective surveys obtained after surgery included the Cincinnati Knee Rating Scale (CKRS) survey 22 and the International Knee Documentation Committee knee survey 9 (beginning in 2000 when the survey was available). Patients also responded to a question asking them at what time after surgery were they able to return to their sport at the same level they played before surgery.
Ligament stability was evaluated with a KT-1000 arthrometer (MEDmetric Corp, San Diego, California, USA), and the maximum manual difference between knees was measured.
Statistical Analysis
Descriptive statistics were obtained. Analysis of variance (ANOVA) of parametric data was performed to determine if there were statistically significant differences between groups for KT-1000 values, subjective survey scores, and the time after surgery when patients reported they had returned to the same sport at the same level as before their injury. Chi-square analysis was used to determine differences in nominal data between groups, with Yates correction applied when the frequency of observations was below 5. A P value of <.05 was considered statistically significant.
Results
Of 84 school-age athletes, 62 (74%) returned to play the same sport in high school, and 18 (24%) of these 62 athletes went on to play the same sport at the college level. Of 58 college athletes, 43 (74%) returned to play the same sport at the college level, and 2 of these 43 athletes went on to play professional football. Of 117 recreational athletes, 73 (62%) returned to the same sport at a recreational level (Table 2). There was no statistically significant difference between groups for the rate of return to the same sport at the same level (P = .1068) or for the time when patients reported that they returned to sports (P =.4112).
Return to Sports After Surgery a
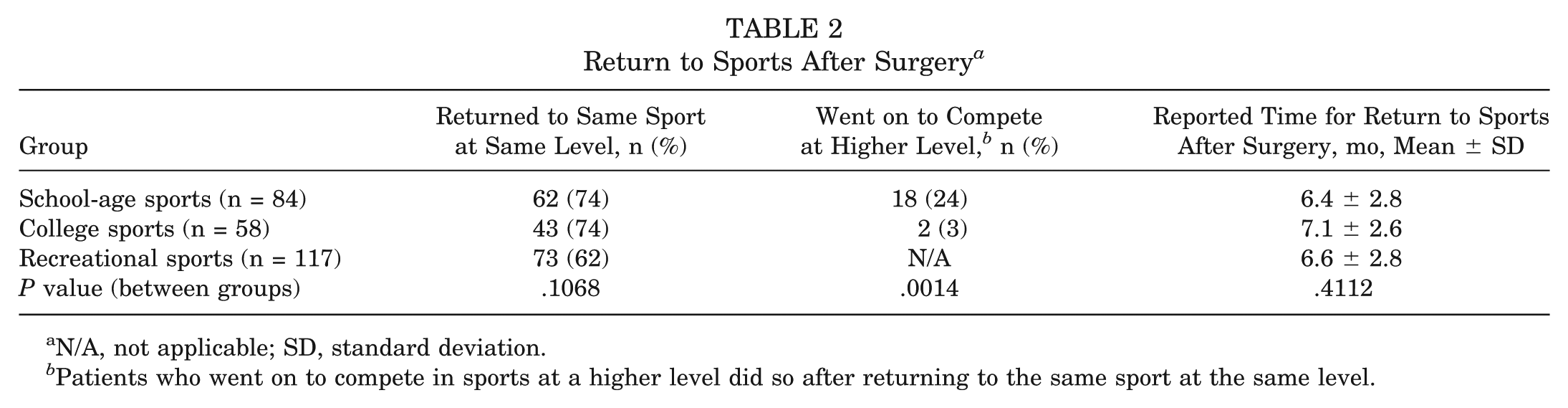
N/A, not applicable; SD, standard deviation.
Patients who went on to compete in sports at a higher level did so after returning to the same sport at the same level.
A subsequent ACL graft tear after revision surgery occurred in 2 of 84 (2.3%) in the school-age group, which occurred in 2 women at 22 and 24 months after surgery while playing basketball. For the college group, 3 of 58 (5.1%) had subsequent ACL graft tears, which occurred in 2 men at 10 months and 3 years after surgery while playing football and in 1 woman at 2 years after surgery while playing basketball. For the recreational group, a subsequent ACL graft tear occurred in 4 of 117 patients (3.4%), and the injuries occurred in 2 men while playing basketball at 15 months and 4 years after surgery, in 1 man while playing soccer at 3 years after surgery, and in 1 woman playing basketball at 6 years after surgery. There was no statistically significant difference in the rate of subsequent ACL graft tear after surgery between groups (P = .6706) (Table 3).
Subsequent ACL Injury to Either Knee After Surgery a
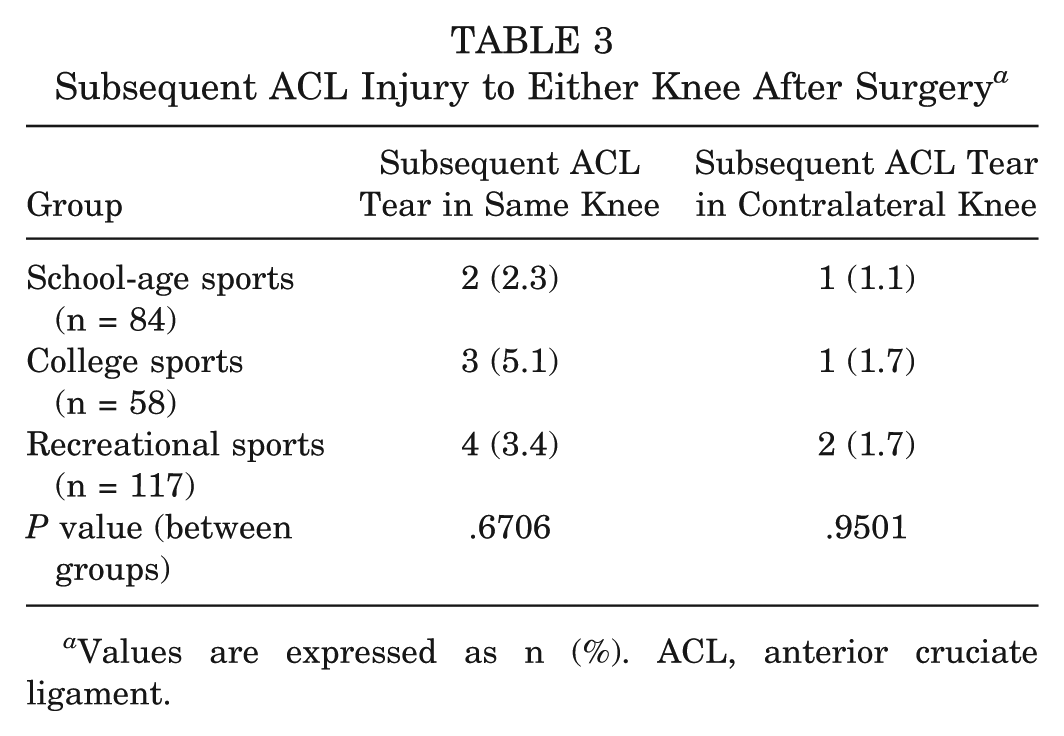
Values are expressed as n (%). ACL, anterior cruciate ligament.
A subsequent ACL tear in the contralateral knee occurred in 1 of 84 patients (1.1%) in the school-age group, and the injury occurred in a woman at 2.4 years after surgery while playing basketball. In the college group, 1 of 58 patients (1.7%) suffered an ACL tear in the contralateral knee, and the injury occurred in a man at 11 years after surgery while playing soccer. For the recreational group, 2 of 117 patients (1.7%) suffered an ACL tear in the contralateral knee, and the injuries occurred in 1 man at 3 years after surgery while playing soccer and in 1 man at 9 years after surgery in a motorcycle accident. There was no statistically significant difference in the rate of subsequent ACL tear to the contralateral knee after surgery between groups (P = .9501).
Overall, of 178 patients who reported they returned to the same sport at the same level, 10 had a subsequent ACL injury to either knee (5.6%). Of 81 patients who reported they did not return to the same sport at the same level, 3 patients had a subsequent injury to either knee (3.7%; P = .7284); however, all but 1 of the subsequent injuries occurred while playing basketball, soccer, or football.
Long-term subjective follow-up was obtained for 210 patients at a mean of 7.2 ± 5.3 years after surgery. The mean CKRS total score was 89.7 ± 11.1 points at 2 years after surgery and 83.7 ± 16.2 points at long-term follow-up. The mean IKDC subjective total score was 86.1 ± 11.7 points at 2 years after surgery and 76.7 ± 18.3 at long-term follow-up. The recreational group had statistically significantly lower CKRS and IKDC total scores than patients in the other 2 groups (Table 4). The mean KT-1000 arthrometer maximum manual difference was 2.3 ± 1.7 mm, and there was no statistically significant difference between age groups (P = .530).
KT-1000 Arthrometer Maximum Manual Difference Between Knees and Subjective Scores by Group a
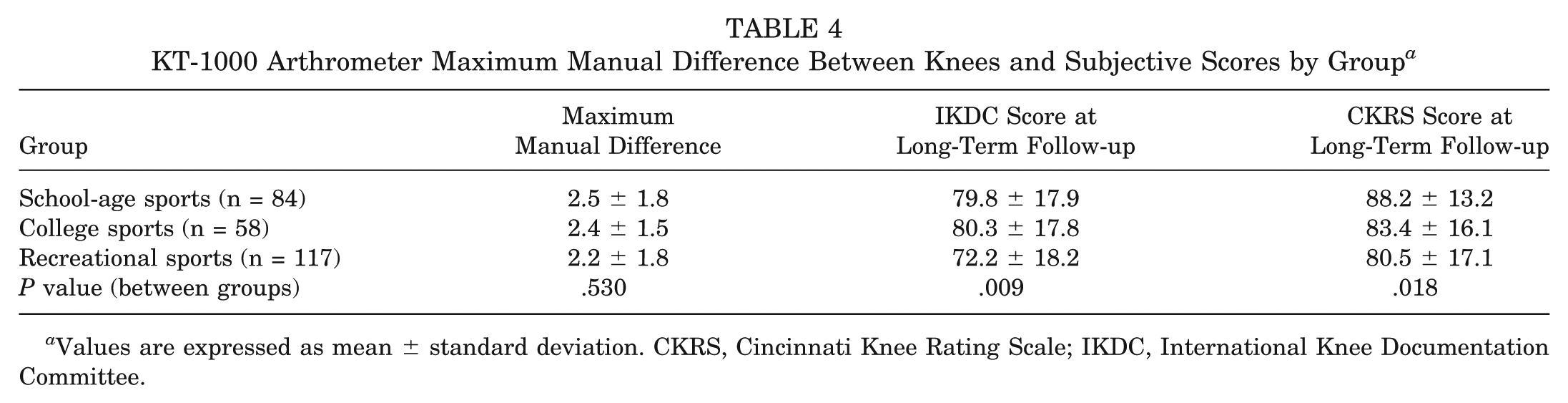
Values are expressed as mean ± standard deviation. CKRS, Cincinnati Knee Rating Scale; IKDC, International Knee Documentation Committee.
Thirty-eight subsequent surgeries were performed on 26 patients (10.0%). One patient required 2 operations for evacuation of hematoma and wound debridement. There was 1 patellar fracture treated with ORIF, followed by a revision ORIF for hardware failure. One patient had a septic knee 2 years after ACL revision, which was treated with incision and drainage followed by IV antibiotics. One patient had a TKA done elsewhere, 12 years after ACL revision surgery. One patient underwent removal of prominent hardware. The remaining 31 surgeries were arthroscopic procedures for partial meniscectomy and/or chondroplasty with or without microfracture. Arthrofibrosis requiring scar resection for motion loss occurred in no patients.
Discussion
The results of this study show that patients who underwent revision ACL reconstruction with BPTB autograft and perioperative rehabilitation were able to return to their desired sport at preinjury level at a rate of 62% to 74%, while having a lower ACL reinjury rate than primary surgery, 18 and there were no statistically significant differences in these rates between groups based on competitive sport levels. The return-to-sports rates in this current study are similar to results found in other studies of soccer and football athletes after primary ACL reconstuctions.4,11 This information is useful not only for counseling patients who inquire about these specifics of their recovery, but also for the treating surgeon when faced with various graft choices and rehabilitation protocols. Furthermore, it serves as an important benchmark for comparison against other available surgical and rehabilitation treatment methodologies.
Few published studies specifically address return to sports after revision ACL reconstruction in young athletes. Wright et al 24 reviewed 21 studies of revision ACL reconstruction and found 54% of the 485 athletes were able to return to unrestricted sports. Battaglia et al 2 reported a series of 63 athletes in which 37 (59%) were able to return to unrestricted sports. However, the mean age of patients was over 30 years old in both studies, reflecting more of a recreational age group. The return to sport rate of around 50% to 60% in these studies is similar to the return rate of patients in the 22- to 35-year-old recreational group in our current study, but is lower than the return rate of the younger-age and competitive sports groups.
Reinhardt et al 14 are the only authors that we are aware of to report return-to-sports data on a series of competitive athletes under the age of 18 who underwent revision ACL reconstruction. They found that 52% of athletes in their series were able to return to sports. However, in all of these studies the graft choice was either a mix of allografts and autografts or a mixture of different autografts (BTPB, hamstrings, quadriceps tendon). Consequently, the ability to generalize these findings to patients of different ages and graft choices is very difficult.
Several graft choices are available in the revision setting, including BPTB, hamstring, or quadriceps autograft, both ipsilateral and contralateral; reharvested BPTB autograft; and allograft tissue from BPTB, hamstrings, Achilles tendon, or tibialis anterior, among others. Allograft tissue has become increasingly popular for ACL reconstruction, especially in the revision setting. Few studies have specifically reported results of allograft revision reconstruction. Fox et al 8 reported a series of allograft BPTB revision ACL reconstructions with a postoperative Cincinnati subjective rating score of 70 at 4.8 years after surgery, with a higher rate of grade 1+ or higher pivot shift results; this study did not report a return-to-sports rate. Lind et al 10 reported results from the Danish registry and found that allograft revision ACL reconstructions had a relative risk of failure 2.05 times that of autograft revisions; return to sports was not reported.
Multiple authors have reported higher failure rates after primary ACL reconstruction with allograft tissue.1,6,13,23 Barrett et al 1 reported 2.6 to 4.2 times higher failure rates among young active individuals who underwent allograft ACL reconstruction compared with autograft. Similarly, 2 separate studies reported increased failure rates in young patients treated with primary ACL reconstruction with allograft.13,23 Ellis et al 6 studied a population of 70 athletes 18 years of age or younger and found 2-year graft survivorship of 96% with autograft tissue versus 65% with allograft tissue. Given these data from primary allograft ACL reconstructions in young athletes, coupled with registry data highlighting higher failure rates in revisions with allograft tissue, it is our preference to use autograft tissue in revision ACL reconstructions, particularly in young athletes with a desire to return to high-level competitive sports.
Previous reports have established the results of revision ACL reconstruction with hamstring autografts. Ferretti et al 7 reported a series of 30 patients (mean age 34) with mean 5-year follow-up after hamstring autograft ACL revision surgery and found a postoperative Lysholm score of 77, with only 20% return to previous level of sports and a 10% failure rate. Salmon et al 15 found in their series of 50 patients a 10% failure rate and a 52% return to IKDC grade 1 or 2 activities. The current study with patellar tendon autografts reports higher return to sports and lower failure rates than these reports in hamstring autograft revision reconstructions.
The use of BPTB autograft has also been studied in revision ACL reconstruction. Noyes and Barber-Westin 12 reported on a series of these reconstructions in 54 patients and found significant improvements in subjective scores as well as an increase in sports participation, albeit with a 24% failure rate. However, 67% of these cases included other procedures, including collateral ligament reconstruction in 31% and high tibial osteotomy in 16%, thus limiting its comparison value with the current study. Colosimo et al 5 used reharvested BPTB and found 9 of 13 (69%) athletes were able to return to their preinjury level of sports. It is our preference to use BPTB autograft for revision ACL reconstruction, especially in young athletes who desire return to sports at a competitive level, and there were 11 patients in this study who received reharvested BPTB grafts.
Anterior cruciate ligament reconstruction with BPTB autografts have specific complications that other grafts do not, most notably patellar fractures and patellar tendon ruptures. One patient in this cohort experienced a patellar fracture after a fall, which ultimately required 2 operations to attain healing. A previous study 3 reported an experience with over 5000 ACL reconstructions with BPTB autografts and there was 1 patellar fracture and 13 patellar tendon ruptures (0.24%). These complications, while certainly unwanted, can be managed and still achieve excellent clinical outcomes, as discussed in that report. Furthermore, the rate of subsequent meniscal surgery was relatively low at 10%.
It is our opinion that the higher return-to-sports rates in this current study compared with other published reports are due to several factors. First, the perioperative rehabilitation protocol stressing preoperative symmetry, early return of full range of motion without immobilization, and progression to activities is identical to our protocol for primary ACL reconstructions. Also, our chosen graft allows for this unrestricted rehabilitation in a way that other grafts may not. Allografts, hamstring grafts, and other soft tissue grafts may require longer time periods for incorporation and, as such, may lead the surgeon to delay rehabilitation progression. Furthermore, surgeons may see the relatively higher failure rates associated with allograft reconstruction in the primary setting and consequently further limit return to sports for this reason. Our data show that revision surgery using BPTB autograft from either knee can restore knee stability and lead to an easier return to competitive sports with low reinjury rates.
Reinjury rates have been documented after primary ACL reconstruction by many authors. Shelbourne et al 18 reported ACL reinjury rates to either the same or the contralateral knee within the first 5 years of primary ACL surgery and found a rate of 4.3% in the reconstructed knee and 5.3% in the contralateral knee, for a combined rate of 9.6%. However, when separated by age group, young athletes under 18 years suffered a combined reinjury rate to either knee of 17.4%, versus 7% in athletes aged 18 to 25 years and 4% in athletes older than 25. This increase in reinjury is likely due to the high-impact demands that young athletes place on their knees combined with increased athletic exposure and intensity of competition compared with recreational athletics.
Given this information with primary ACL reconstruction, we believed that the reinjury rates after revision ACL reconstruction would meet or exceed those found after primary ACLs. Furthermore, we expected the same trend as in primary ACL reconstruction, with the youngest age group having the highest reinjury rates. However, the combined 5-year reinjury rate that we found in the revision setting was actually lower than the primary setting (5.0% vs 9.6%), especially in young, competitive high school (3.6% vs 17.4%) athletes. It is possible that the lower reinjury rate found in this current study indicates that athletes are able to return to the same sport at the same competition level, but may not do so with the same intensity and confidence, thus leading to less reinjury. Furthermore, repeat ACL injury requiring revision reconstruction occurred later in the athletic career of high school athletes, thus decreasing the amount of remaining athletic exposure, and possibly the risk of reinjury, after revision surgery.
A limitation of this study is that the results can only be applied to patients undergoing revision ACL surgery with a patellar tendon autograft, as no other graft sources were used. Also, the findings of this study cannot be directly compared statistically with other published reports due to differences in study design. A randomized controlled study of patellar tendon, hamstring, and allograft reconstructions would be optimal for direct comparison. Additionally, the data analyzed were limited to patient responses to surveys asking whether they had returned to their sport at the same level. The patients’ perceptions of their function may be lower than what they report.
Conclusion
Revision ACL reconstruction with BPTB autograft and perioperative rehabilitation allowed high school and college athletes to return to sports at the preinjury level at a rate of 74%; the return rate for recreational-level adults was 62%. Reinjury rates in the first 5 years after revision surgery ranged from 2% to 5%, which is lower than what has been reported for young competitive athletes after primary surgery.
Footnotes
Acknowledgements
The authors thank Kanitha Phalakornkule, MS, MIS, MBA, for her statistical analysis of the data.
Presented at the 39th annual meeting of the AOSSM, Chicago, Illinois, July 2013.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.