
Abstract
Background:
The reported prevalence of radiological osteoarthritis (OA) after anterior cruciate ligament (ACL) reconstruction varies from 10% to 90%.
Purpose/Hypothesis:
To report the prevalence of OA after ACL reconstruction and to compare the OA prevalence between quadrupled semitendinosus tendon (ST) and bone–patellar tendon–bone (BPTB) grafts. The hypothesis was that there would be no difference in OA prevalence between the graft types. The secondary aim was to study whether patient characteristics and additional injuries were associated with long-term outcomes.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
Radiological examination results, Tegner activity levels, and Knee injury and Osteoarthritis Outcome Score (KOOS) values were determined in 135 (82%) of 164 patients at a mean of 14 years after ACL reconstruction randomized to an ST or a BPTB graft. Osteoarthritis was defined according to a consensus by at least 2 of 3 radiologists of Kellgren-Lawrence grade ≥2. Using regression analysis, graft type, sex, age, overweight, time between injury and reconstruction, additional meniscus injury, and a number of other variables were assessed as risk factors for OA 14 years after ACL reconstruction.
Results:
Osteoarthritis of the medial compartment was most frequent, with 57% of OA cases in the ACL-reconstructed knee and 18% of OA cases in the contralateral knee (P < .001). There was no difference between the graft types: 49% of OA of the medial compartment for BPTB grafts and 65% for ST grafts (P = .073). The KOOS results were lower for patients with OA in all subscales, indicating that OA was symptomatic. No difference in the KOOS between the graft types was found. Meniscus resection was a strong risk factor for OA of the medial compartment (odds ratio, 3.6; 95% CI, 1.4-9.3) in the multivariable logistic regression analysis.
Conclusion:
A 3-fold increased prevalence of OA was found after an ACL injury treated with reconstruction compared with the contralateral healthy knee. No differences in the prevalence of OA between the BPTB and quadrupled ST reconstructions were found. An initial meniscus resection was a strong risk factor for OA; the time between injury and reconstruction was not.
Keywords
The prevalence of reported osteoarthritis (OA) after anterior cruciate ligament (ACL) injuries ranges between 10% and 90% in different studies, and it is unclear how ACL reconstruction affects the prevention of OA.9,18,23,25,28,29 When the prevalence of OA after ACL reconstruction is compared between the reconstructed and the healthy noninjured knee, most authors have found more cases of OA in the reconstructed knee.4,11,12,21,23,30,31,42 However, the cause of OA is multifactorial, and long-term outcomes after an ACL injury are largely influenced by the presence of associated injuries, such as meniscus and cartilage injuries.4,16,21,25,30 It has been reported that meniscus injuries requiring resection increase the risk of an inferior functional result and OA after ACL reconstruction7,25 and that a high body mass index (BMI) might also influence the risk of OA after an ACL injury.4,18,20,21 Whether the time elapsed between injury and ACL reconstruction affects the prevalence of OA is not clear.16,22,24,32
The choice of graft for ACL reconstruction has also been discussed as one of the factors influencing long-term morbidity, and bone–patellar tendon–bone (BPTB) grafts have been reported to result in more cases of patella infera and to cause more problems with kneeling and other patellofemoral problems, including OA, compared with hamstring tendon grafts.3,15,26,27,37 In general, randomized controlled trials (RCTs) with a minimum 10-year follow-up, including radiological assessments, after ACL reconstructions are rare, and no clear consensus regarding radiographic OA differences between graft types can be found in the literature.12,16,22,42 The present study is a follow-up of an RCT between BPTB and quadrupled semitendinosus tendon (ST) grafts. At the 2-year follow-up, both groups had similar good functional outcomes, but it was noted that patients with an associated meniscus injury had a worse outcome according to the International Knee Documentation Committee (IKDC) scores. 6 After 8 years, the majority of the patients still had good knee function and good health-related quality of life (HRQoL), but kneeling problems were more common among patients with a BPTB graft than those with an ST graft. Furthermore, patients with early reconstructions (<6 months) had a significantly lower risk for meniscus injuries and better HRQoL compared with all others at 8 years. 3
The primary aim of this study was to report the prevalence of radiological OA after ACL reconstruction and to investigate whether the graft type used affected the radiological and functional outcomes. Our hypothesis was that the prevalence of OA would be similar in the graft types. The secondary aim was to study whether early ACL reconstruction and additional meniscus injuries sustained before the reconstruction were associated with long-term outcomes.
Materials and Methods
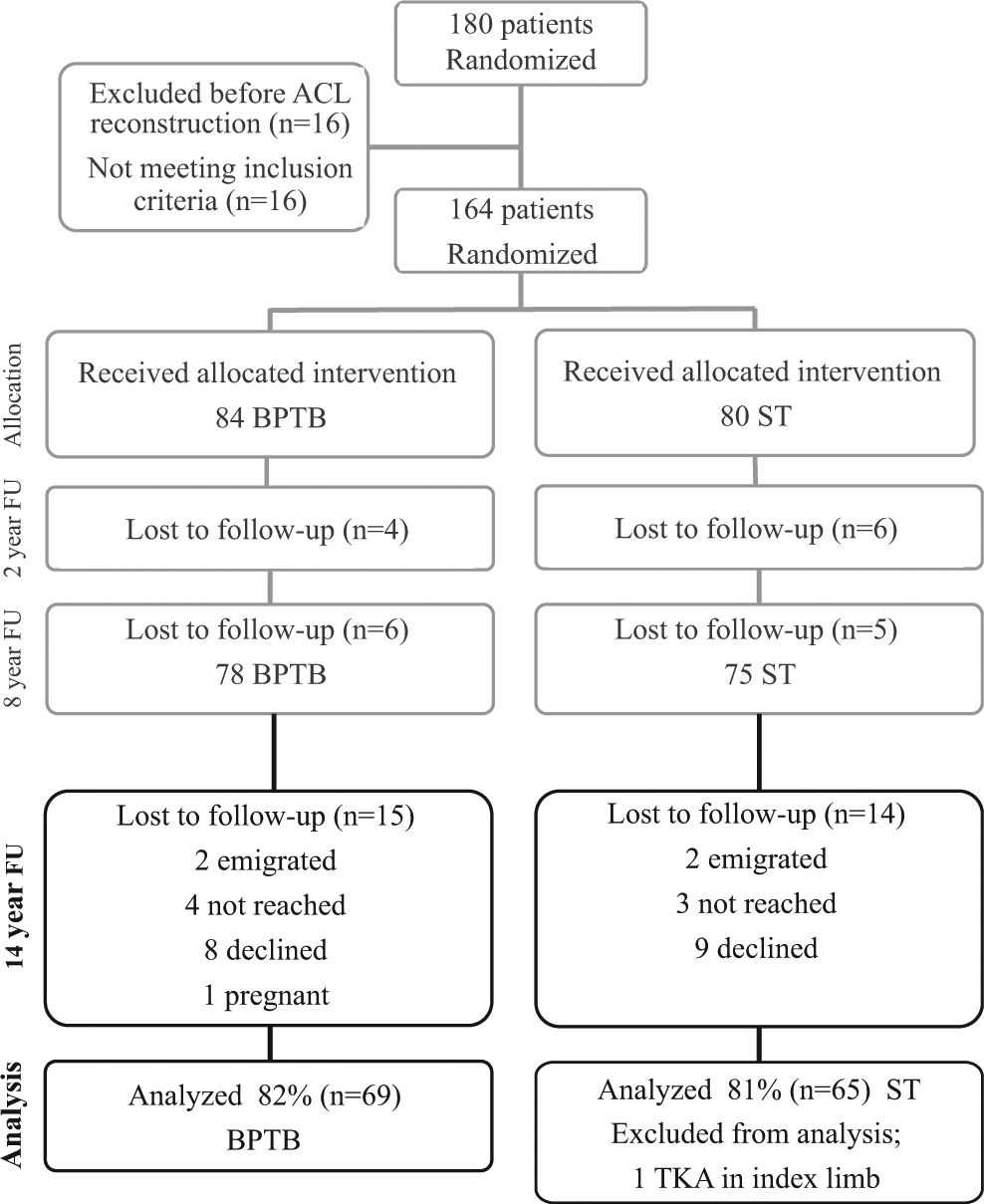
A total of 164 patients were included in an RCT during the years 1995-1997. 6 All of them had a traumatic ACL injury with instability and were previously healthy in the bilateral knee. The patients’ ACL reconstructions were randomized according to the graft used in 2 groups: one using an ipsilateral BPTB graft (n = 84) and the other an ipsilateral quadrupled ST graft (n = 80). They were all assessed with a nonweightbearing preoperative radiograph. None had OA at this assessment. Fourteen years (mean ± standard deviation, 14.1 ± 0.5 years) after ACL reconstruction, 157 patients were identified and contacted, and 135 (82%) agreed to participate (BPTB group, n = 69; ST group, n = 66). The prevalence of OA was analyzed according to the intention-to-treat (ITT) principle. One patient in the ST group had undergone total knee arthroplasty (TKA) during the follow-up period and was excluded from the analysis; thus 65 patients in the ST group were analyzed (Figure 1). At the time of the study, the patients included were between 29 and 57 years of age (mean, 40.0 ± 6.4 years).
In a subanalysis, the effect of contralateral injuries and additional major surgeries on the prevalence of OA was assessed. All patients with major additional surgeries were excluded (ie, 1 TKA, 1 proximal tibial fracture, 5 ACL revisions, 5 contralateral ACL reconstructions, and 1 ACL revision and contralateral ACL reconstruction), resulting in 61 patients in the ST group and 61 patients in the BPTB group.
The regional ethics committee approved this study, and all patients gave their informed consent to participate.
Radiographic Assessment
All patients underwent a radiological examination of the primarily injured knee and the contralateral knee to determine the grade of OA. Weightbearing anteroposterior (AP) and lateral views with the knee joint in full extension and an AP view in 30° of flexion were taken, as well as a skyline view of the patellofemoral compartment. The Kellgren-Lawrence (KL) classification 17 was used, and OA was defined as KL grade ≥2 (ie, significant osteophytes and/or cartilage reduction up to 50%). Three independent radiologists judged the radiographic results. In this study, a consensus by at least 2 of the 3 radiologists was needed to determine OA. The patellar height was measured according to the Insall-Salvati index 13 by the senior author (K.E.). An index difference of >0.05, where the lower index was found in the ACL-reconstructed knee, was defined as patella infera.
Knee Function Assessment
All patients were asked to respond to the question “How does your knee function?” on a visual analog scale (VAS) in which 0 indicated the worst possible score and 100 indicated the best possible score. The patients were also asked to rate their Tegner activity level, 40 and their subjective knee function and HRQoL were assessed with the Knee injury and Osteoarthritis Outcome Score (KOOS). The KOOS is a knee-specific HRQoL instrument developed to assess the patients’ opinions concerning their knee function and knee-associated problems and how this function affects their life. 34 The KOOS has been used previously when studying patients with ACL injuries. It consists of 5 subscales: Pain, other symptoms (Symptoms), function in daily living (ADL), function in sport and recreation (Sport/Rec), and knee-related quality of life (QoL). One patient with a BPTB graft and 3 with ST grafts were excluded from the KOOS analysis because of incomplete questionnaires, thus resulting in 62 patients with ST grafts and 68 patients with BPTB grafts in the analysis.
To analyze symptomatic OA, we used a previously published definition of symptomatic knee problems according to the KOOS 23 combined with the results of radiological OA. According to the published definition, a patient with a KOOS value below a specified threshold level on any subscale (<86.1 for Pain, <85.7 for Symptoms, <86.8 for ADL, <85.0 for Sport/Rec, and <87.5 for QoL) has a symptomatic knee. Patients with symptomatic knee problems according to this definition and with radiological OA were defined as having symptomatic OA.
In the analysis, a meniscus injury was defined as an injury diagnosed at the initial arthroscopic procedure and/or at the primary ACL reconstruction, regardless of what type of treatment the injury necessitated. Furthermore, the subgroups of patients undergoing repair or meniscus resection because of their meniscus injury were compared with one another and with those without meniscus surgery.
Variables tested for their significance as a risk factor for OA at the 14-year follow-up were the following data from inclusion: sex, age at injury, preinjury Tegner activity level, frequency of medial or lateral meniscus injuries, meniscus resections and meniscus sutures, manual labor at the time of injury, time between injury and reconstruction as a scale variable and as dichotomized variables before or after 6 months and before or after 12 months, and graft type.
Variables tested from the 2-year follow-up were as follows: side-to-side laxity difference using a Stryker arthrometer (OSI Stryker, Kalamazoo, Michigan, USA), pivot shift (dichotomized to absent or grade ≥1), BMI dichotomized according to the World Health Organization definition of overweight of <25 or ≥25 kg/m2, patellofemoral score according to Werner et al 41 (aggregated functional patellofemoral score), IKDC 14 score dichotomized to AB or CD, extension deficit of 3° to 5°, flexion deficit of 6° to 15°, additional arthroscopic procedure after the index reconstruction, current Tegner activity level, VAS response to “How does your knee function?” (VAS1), and VAS response to “How does your knee affect your level of activity?” (VAS2).
Variables tested from the present follow-up were as follows: age at follow-up; time from injury to follow-up; time from reconstruction to follow-up; radiologic OA in the medial, lateral, and patellofemoral compartments; OA (tibiofemoral) in the medial or lateral compartment and OA in any compartment in the index or contralateral knee; KOOS; Insall-Salvati patellar index; and current and desired Tegner activity levels.
Statistical Analysis
The statistical software used was SPSS v 20 for Macintosh (SPSS Inc, Armonk, New York, USA) except for the analysis of collinearity, consistency, and interrater correlation in which R v 2.14.2 was used (R Foundation for Statistical Computing, Vienna, Austria). Nominal variables were tested using the χ2 test or Fisher exact test. Ordinal variables and nonnormally distributed interval and ratio scale variables were evaluated using the Mann-Whitney U test, and the Student t test was used for normally distributed interval and ratio scale variables in independent groups. The related-samples t test and the Wilcoxon matched-pair signed-rank test were used for variables with measurements from more than a single time point. The tests were 2-sided, and results were considered significant at P < .05. Logistic regression was used to estimate the risk of OA for all selected variables. The risk was estimated using odds ratios (ORs), which are presented with 95% confidence intervals (CIs) (If the OR is <1, the risk is lower than in the reference category, and if the OR is >1, the risk is higher. The deviation from 1 [no association] is statistically significant at the 5% level if the 95% CI does not include 1.) A P value <.1 after univariable regression analysis was used to select variables to be included in the multivariable analysis. Time since reconstruction was not included in the multivariable analysis because of its low predictive value. When more than one risk factor of the same type was significant in the univariable analysis, the most significant risk factor was evaluated in the multivariable analysis. When the Tegner activity level was included in a regression, the variable was categorized as 0-3, 4-6, or 7-10. The interrater agreement was calculated using the Fleiss κ for n raters. There was no indication of multicollinearity: a variance inflation factor of <2 for all variables in the regression model. There were no outliers affecting the model: Cook’s distance was <1 for all observations in the model. The discrimination of the model was acceptable (c statistic, .773). Goodness of fit according to the Hosmer-Lemeshow test was acceptable (P = .656). No interactions were found that changed the significance of the model.
Results
Patient Characteristics
The ST and BPTB groups were comparable regarding baseline data, except that there were more female patients and more extension deficits after 2 years in the BPTB group and more lateral meniscus resections had been performed at inclusion and the patients were older at the current follow-up in the ST group (Table 1).
Patient Characteristics According to Randomization Group a
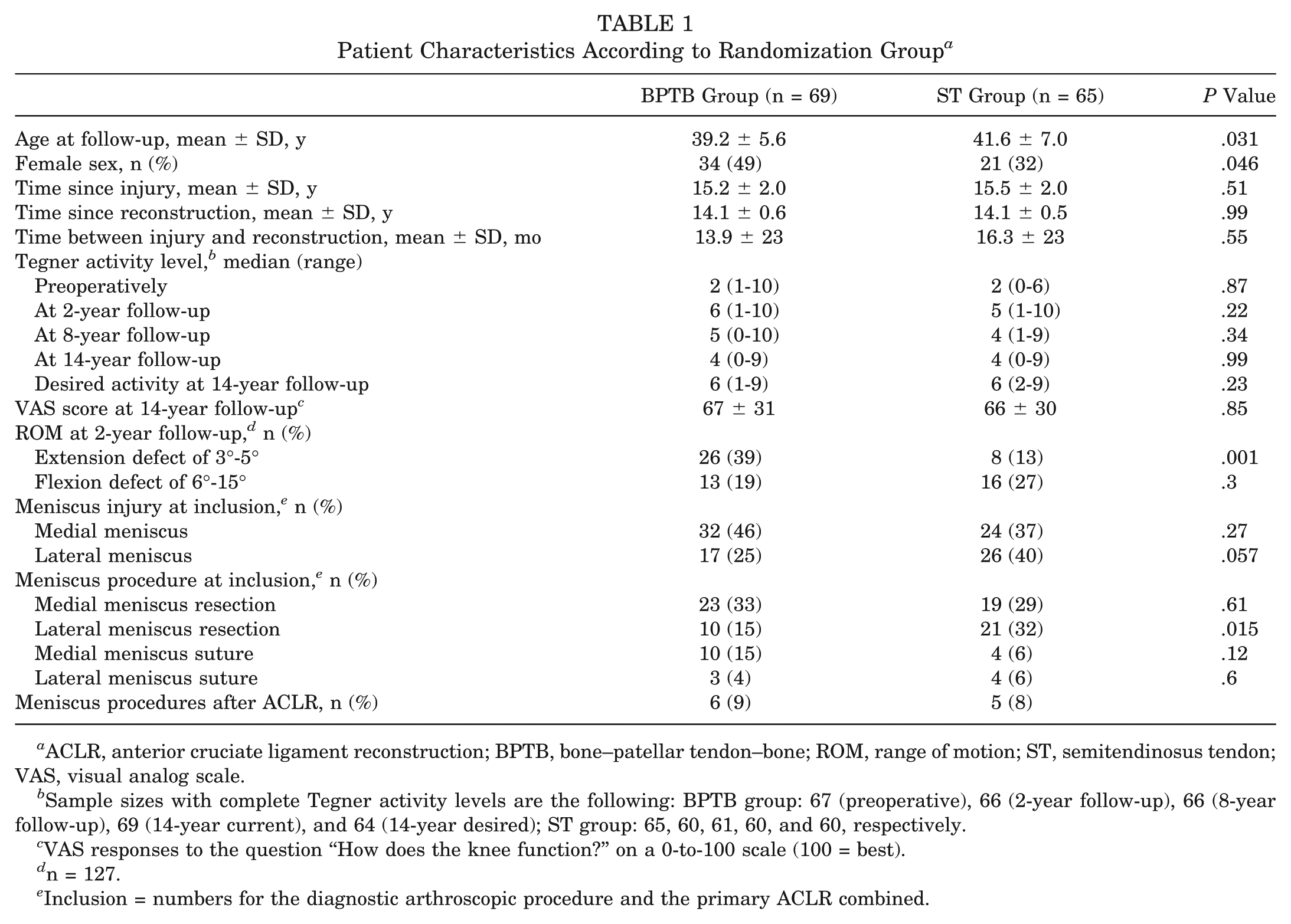
ACLR, anterior cruciate ligament reconstruction; BPTB, bone–patellar tendon–bone; ROM, range of motion; ST, semitendinosus tendon; VAS, visual analog scale.
Sample sizes with complete Tegner activity levels are the following: BPTB group: 67 (preoperative), 66 (2-year follow-up), 66 (8-year follow-up), 69 (14-year current), and 64 (14-year desired); ST group: 65, 60, 61, 60, and 60, respectively.
VAS responses to the question “How does the knee function?” on a 0-to-100 scale (100 = best).
n = 127.
Inclusion = numbers for the diagnostic arthroscopic procedure and the primary ACLR combined.
Lost to Follow-up
The 29 patients (14 ST, 15 BPTB) who did not attend the 14-year follow-up had fewer medial meniscus injuries and more lateral meniscus injuries at the initial diagnostic arthroscopic procedure or the index ACL reconstruction compared with all others. Patients not attending the 14-year follow-up had better outcomes at the 8-year follow-up compared with the patients who were assessed at the 14-year follow-up on Lysholm (mean, 90 vs 83, respectively) and Werner patellofemoral scores (mean, 44 vs 39, respectively). There were no significant differences in all other variables between the groups.
Additional Procedures
Before the present follow-up, 5 patients (2 ST and 3 BPTB) had their ACL reconstruction revised, and 5 patients (2 ST and 3 BPTB) underwent ACL reconstruction on the contralateral side; 1 patient with a BPTB graft underwent both a revision and a contralateral ACL reconstruction. One patient with a BPTB graft had a tibial plateau fracture in the primarily injured knee, and 1 patient with an ST graft underwent total knee replacement in the primarily injured knee. Because of recall bias, no further data on additional procedures are reported.
The subanalysis, with patients with major additional surgeries excluded, did not reveal any significantly different results than the ITT analysis did; only results for the ITT analysis are presented. There were more cases of patella infera in the ACL-reconstructed knee according to the Insall-Salvati index, but there were no other differences according to graft group or OA location. The median Insall-Salvati index was 1.00 (95% CI, 0.67-1.33) for the ACL-reconstructed knee and 1.06 (95% CI, 0.76-1.33) for the contralateral knee (P < .001).
Prevalence of OA
Osteoarthritis was significantly more frequent in the ACL-reconstructed knee than in the contralateral knee. The prevalence of OA with comparisons between the graft groups is presented in Figure 2.
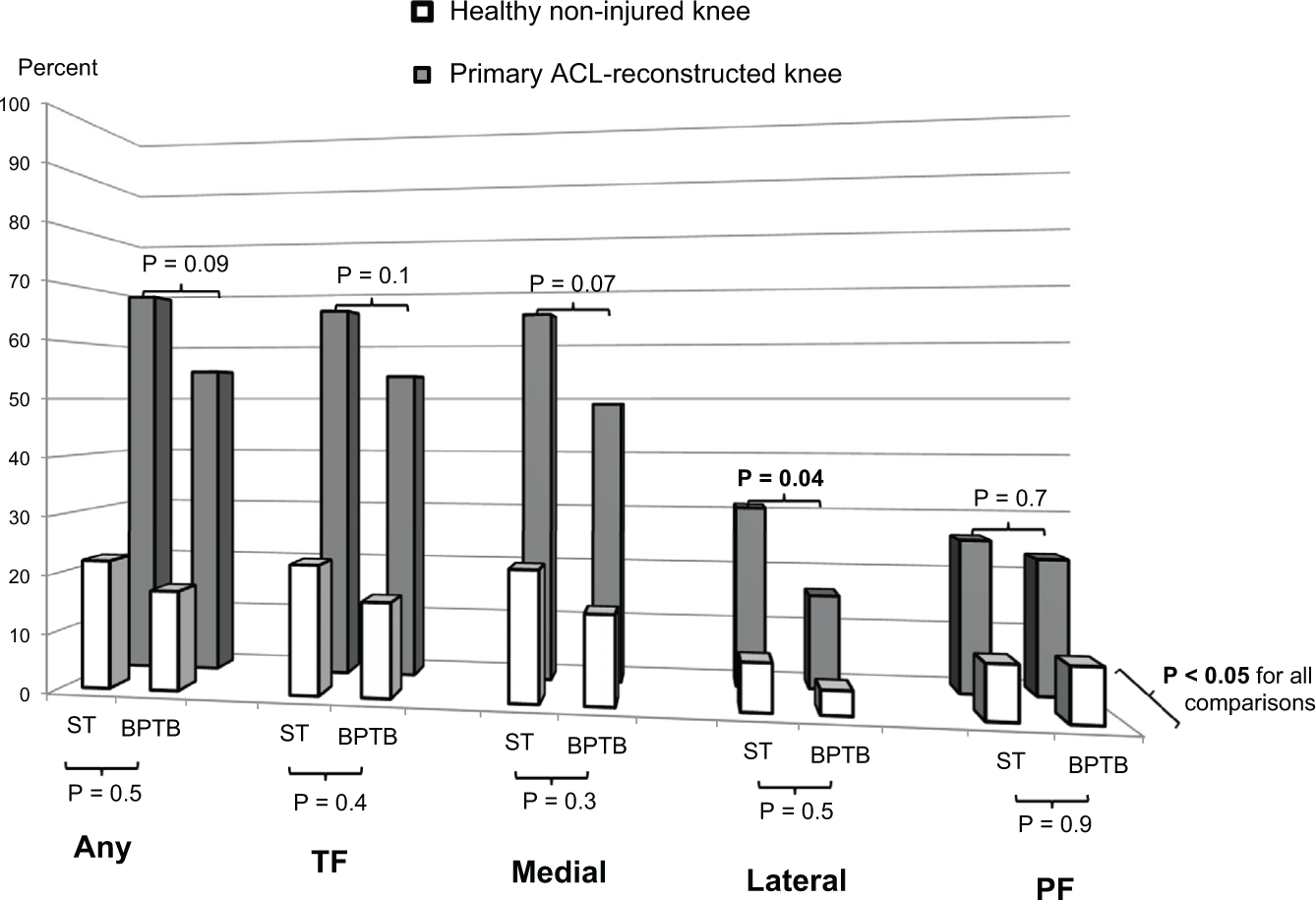
Osteoarthritis in relation to the randomization groups of bone–patellar tendon–bone (BPTB) or semitendinosus tendon (ST). Osteoarthritis was defined as Kellgren-Lawrence grade ≥2 according to a consensus by at least 2 of 3 radiologists. The graph shows the prevalence of osteoarthritis in any compartment (Any), lateral or medial compartment (TF), medial compartment (Medial), lateral compartment (Lateral), and patellofemoral compartment (PF).
The interrater agreement between the radiologists was highest for OA of the lateral compartment (Fleiss κ = .52) and lowest for OA of the medial compartment (Fleiss κ = .024). Patients with OA in the medial or patellofemoral compartment rated their knee function according to the VAS as lower compared with those without OA: mean of 74 ± 27 for patients without OA of the medial compartment versus 60 ± 31 for those with OA (P = .010) and 69 ± 28 for patients without patellofemoral OA versus 56 ± 32 for those with OA (P = .029).
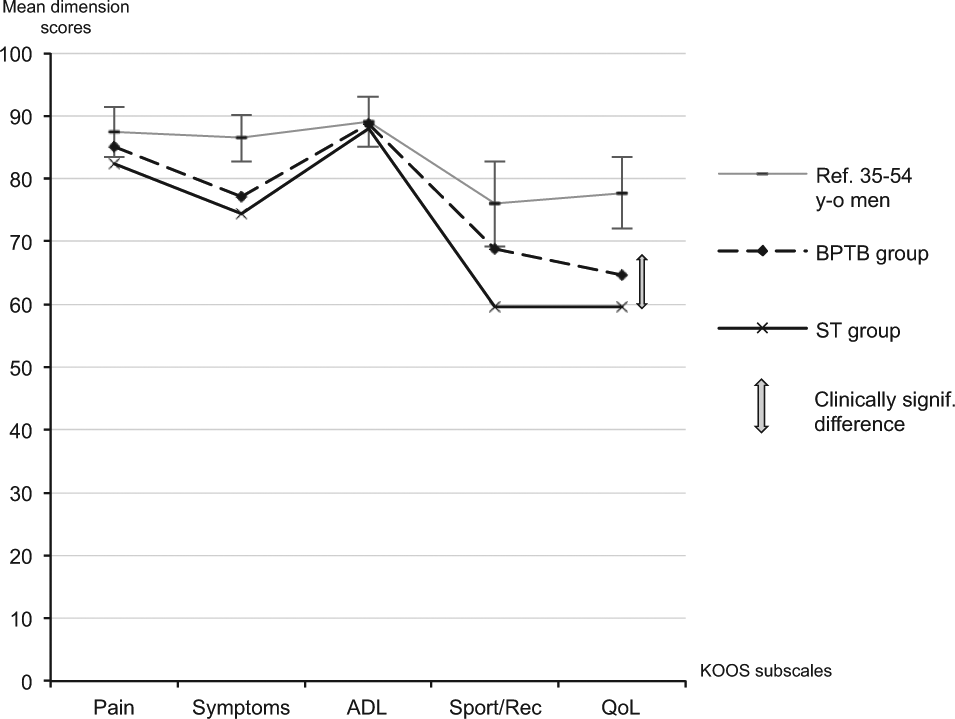
The KOOS results showed that patients with OA in any compartment in any knee had significantly worse scores than patients without OA (Figure 3). There were no significant differences in the KOOS between the graft groups (Figure 4).
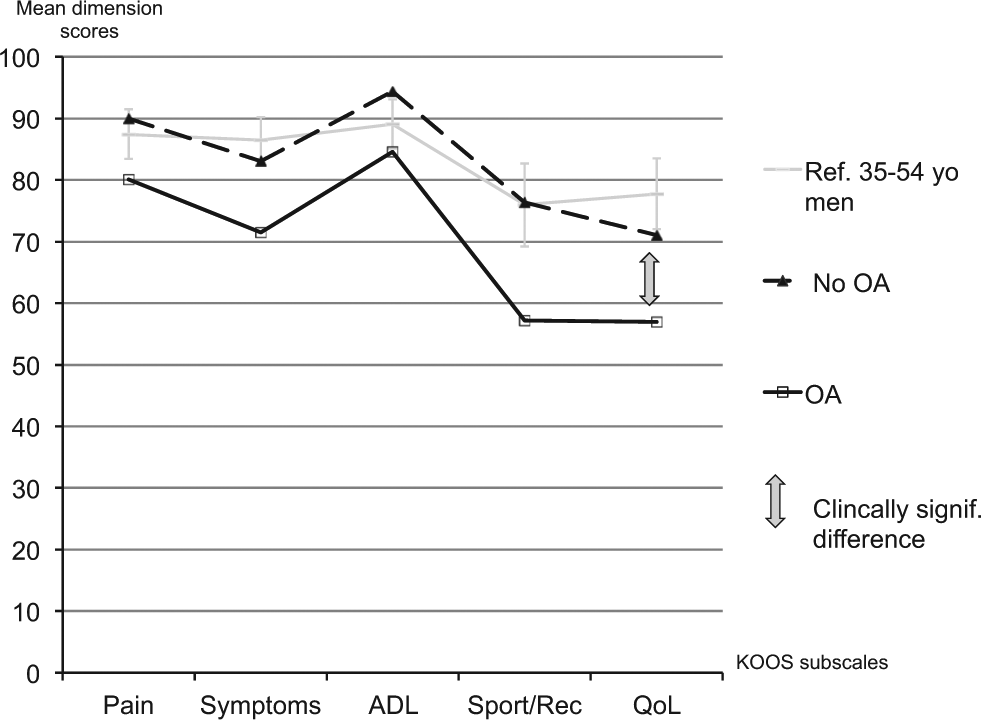
Clinically significant difference in the Knee injury and Osteoarthritis Outcome Score (KOOS). Mean KOOS results are shown for patients with osteoarthritis (OA) in any compartment (n = 81; dashed line) compared with patients without OA in any knee (n = 49; solid black line). Shown for comparison are results from a reference population of 35- to 54-year-old men (solid gray line) (from Paradowski et al 33 ), and a gray 8-point arrow indicates the minimal clinically noticeable difference. KOOS subscales: Symptoms, other symptoms; ADL, function in daily living; Sport/Rec, function in sport and recreation; QoL, knee-related quality of life.
Similar Knee injury and Osteoarthritis Outcome Score (KOOS) values for the graft groups. Mean KOOS results are shown for the bone–patellar tendon–bone (BPTB) group (dashed line) and semitendinosus tendon (ST) group (solid black line). Shown for comparison are results from a reference population of 35- to 54-year-old men (solid gray line) (from Paradowski et al 33 ), and a gray 8-point arrow indicates the minimal clinically noticeable difference.
According to our definition, 76 patients (59%) had symptomatic knee problems. Fifty-one (70%) of the patients with OA of the medial compartment in the index limb were symptomatic versus 25 (44%) without medial OA (P = .003). There was no significant difference in symptomatic knee problems between patients with and without OA in the lateral or patellofemoral compartment.
Risk Factors for OA
Risk factors for OA are presented in Table 2.
Risk Factors for Osteoarthritis a
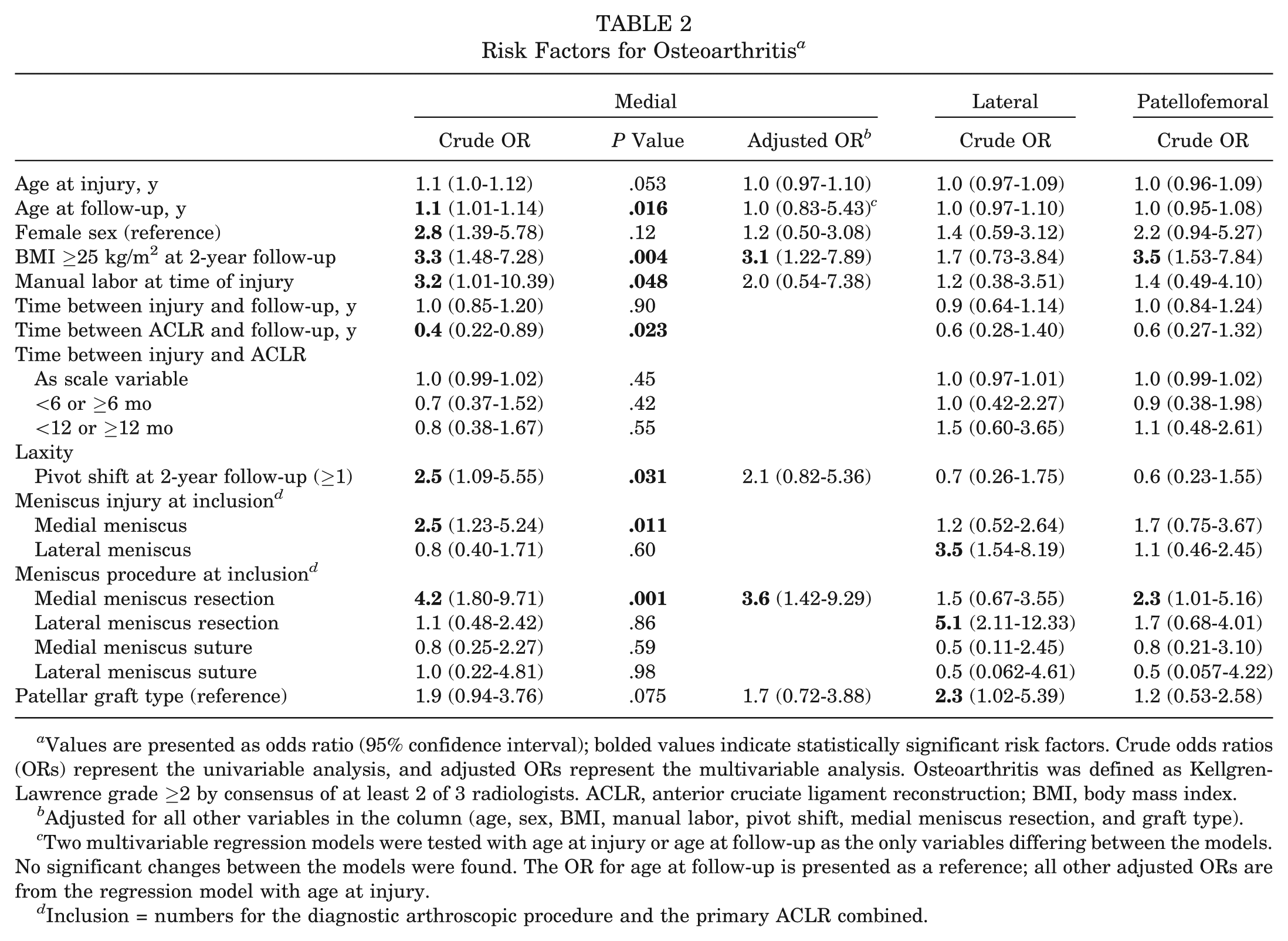
Values are presented as odds ratio (95% confidence interval); bolded values indicate statistically significant risk factors. Crude odds ratios (ORs) represent the univariable analysis, and adjusted ORs represent the multivariable analysis. Osteoarthritis was defined as Kellgren-Lawrence grade ≥2 by consensus of at least 2 of 3 radiologists. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index.
Adjusted for all other variables in the column (age, sex, BMI, manual labor, pivot shift, medial meniscus resection, and graft type).
Two multivariable regression models were tested with age at injury or age at follow-up as the only variables differing between the models. No significant changes between the models were found. The OR for age at follow-up is presented as a reference; all other adjusted ORs are from the regression model with age at injury.
Inclusion = numbers for the diagnostic arthroscopic procedure and the primary ACLR combined.
The Werner patellofemoral score and IKDC grade at 2 years were not risk factors for OA at 14 years, nor were additional arthroscopic procedures after the primary reconstruction, AP laxity (Stryker), VAS1, VAS2, or deficits in range of motion either in extension or flexion at 2 years. The preoperative Tegner activity level was higher for patients with OA of the lateral compartment (median, 9; 95% CI, 3-10) compared with patients without OA (median, 8; 95% CI, 2-10) (P = .038). However, the Tegner activity level was not found to be a risk factor for OA in any compartment in the univariable analysis.
In a univariable analysis using patients with medial meniscus repairs as a reference, the risk of OA did not significantly differ from that for patients with no medial meniscus injury (P = .9). Patients with a resected medial meniscus had an increased risk compared with patients with a repaired medial meniscus (OR, 4.3; 95% CI, 1.1-16.0) (P = .030).
The data allowed an additional multivariable analysis of the risk factors for OA of the medial compartment; this analysis is presented in Table 2. When the graft type was adjusted for the frequency of lateral meniscus resections, only lateral meniscus resection was a significant risk factor for OA of the lateral compartment (OR, 4.5; 95% CI, 1.8-11.1) (P = .001). When medial meniscus resection was adjusted for BMI, only BMI was a significant risk factor for OA of the patellofemoral compartment (OR, 3.4; 95% CI, 1.5-7.7) (P = .004).
Discussion
The major finding of this study was that ACL reconstruction did not protect the knee from secondary OA. The study also showed that the choice of graft or the time between injury and reconstruction did not affect the risk of OA after 14 years and that meniscus resection was a strong risk factor for OA.
In this study, ACL reconstruction was performed using a transtibial approach, which was typical for that time and resulted in nonanatomic graft placement. The reconstruction did not give any protection against secondary OA in line with the published literature.12,18,23,31 However, many of the published studies with 10- to 15-year follow-ups report results after using surgical techniques that are no longer in use.2,6,25 There are some reports of claimed anatomic reconstructions with long-term follow-ups and favorable results regarding OA,10,42 but there are too few reports to determine whether the anatomic ACL reconstruction used today will protect the knee from OA.
There was no difference in the prevalence of OA between the graft types in this study. The results are similar to those in 2 other RCTs comparing the patellar tendon with the hamstring tendon.12,42 Sajovic et al 36 found a higher prevalence of OA in BPTB reconstructions in their RCT. However, the difference in age and meniscus resections between the graft groups was not assessed. 36 Keays et al 16 found a higher prevalence of OA in their prospective cohort study, while Liden et al 22 did not. The cause of OA is multifactorial, and one explanation for the divergent results might be that confounding factors such as age and BMI have not been considered. One way to take the multifactorial influence into account is to use multivariable regression analysis. Several of the theoretical risk factors that might influence the development of OA increased the risk for OA in the univariable analysis in this study, but only overweight and meniscus resection were true risk factors for OA in the multivariable analysis. Graft type was not found to be a risk factor for OA, nor was residual laxity, sex, or age at injury. It should be noted that this study was not originally designed for the purpose of the multivariable analysis of risk factors for OA; therefore, the study population might be too small to find true risk factors. A high BMI has been reported to be a risk factor for OA.5,8 Kessler et al, 18 Lebel et al, 20 and Li et al 21 have all found a high BMI to be a risk factor for OA after ACL injuries. In the light of the published data and the results of this study, it is our opinion that it is important for patients with a known ACL rupture to avoid being overweight to protect their knee function in the long term.
The results showed no direct effect of time between injury and ACL reconstruction on the prevalence of OA. However, results from the literature and in this study are consistent with an increasing frequency of meniscus injuries with increasing time between injury and surgical intervention,3,4,6,25 and the effect of meniscus resection on OA is well established in the literature and in this study.7,22,31,35,38 There is also a report of increased OA among patients with longer times between injury and reconstruction. 22 At present, there is no better way to protect the meniscus after an ACL rupture than undergoing ACL reconstruction. 4 A noninjured meniscus decreased the OR for OA in this study. The fact that meniscus repair had a significantly lower OR for OA than resection is also worth noting. Time in and of itself is not important but rather what activities in which the patients take part during that time. Activity modification as a treatment option after ACL ruptures has been reported to result in few cases of OA. 28 However, this is probably only true for patients who comply with the activity modification regimen. Treatment recommendations after an ACL injury are not clear, especially in view of the future risk of OA. Early reconstruction might be recommended because of a perceived high risk for additional injuries in patients who continue participation in pivoting sports or with instability, or nonoperative treatment could be recommended for patients who comply with activity modification and are at a low risk for additional injuries. Fithian et al 9 used an algorithm for selecting patients for early reconstruction owing to pivoting activity and instability and nonoperative treatment for those not selected. They found that more additional meniscus surgeries were performed in the nonoperative group and that there were more cases of OA in the early reconstructed group. 9 We found that the level of activity after the injury (Tegner) was not a risk factor for OA. However, the patients in this study are a mix of patients scheduled for ACL reconstruction at the time of an ACL rupture and patients with failed nonoperative treatment. An in-depth analysis of the relationship between the activity level and OA is therefore not feasible.
The KOOS has been shown to be a valid method for measuring HRQoL in patients with knee injuries and OA. 34 Oiestad et al 31 found significantly lower subscale symptom scores for patients with KL grade ≥2, adjusted for age, BMI, and sex in their cohort of patients with their ACL reconstructed after 10 to 15 years. In our study, there were larger differences between patients with OA defined as KL grade ≥2 and patients without OA (with the highest effect on the KOOS for OA of the medial compartment) compared with the results reported by Oiestad et al, 31 who however presented data for all compartments combined, while in this study, OA was separated for the different compartments. Two other recently published long-term studies on OA after ACL ruptures have used the KOOS in their evaluation; however, they have presented the KOOS as a combined score and made no comparison between knees with and without OA, which makes a comparison impossible.10,11
The reason for the variation between studies in the prevalence of OA after ACL reconstruction appears to be multifactorial. Reasons for the variation are different treatment regimens, different times to follow-up, and different study populations, as well as different OA grading systems. The most usual radiographic classification systems for grading OA changes in the knee joint are those of Kellgren and Lawrence, 17 Ahlback, 1 Fairbank, 7 and the IKDC. 14 Cartilage loss and osteophyte formation are both features of a degenerative process in the knee joint, and systems that take such processes into account have higher validity in the OA definition. 19 Regardless of the classification system used, they all have an interobserver variation because of the subjective interpretation of each radiographic view. In this study, the interobserver agreement is low; we interpret this as an effect of having 3 radiologists in the study. There is also a wide variation in the literature on the reported results of symptomatic OA, again to a large extent because of different classifications. Some authors have defined symptomatic OA according to additional aspects of knee pain, 30 some according to the KOOS, 23 and some according to the level of OA found at the radiological assessment. 39 Because we used the KOOS, we analyzed the data according to the definition used by Lohmander et al. 23 In our study, the majority of the patients had symptomatic knee problems, and 39% had symptomatic OA of the medial compartment, similar to that in the study by Lohmander et al, 23 who found 42% of symptomatic OA cases in their cohort of female soccer players 12 years after an injury, and similar to that reported by Oiestad et al, 30 who found 32% to 46% of symptomatic OA cases according to KL grade ≥2 and pain in the ACL-injured knee ascribable to additional injuries in their cohort of 221 patients with BPTB reconstructions. Struewer et al 39 defined symptomatic OA as KL grade ≥3 and found 20% of symptomatic OA cases among 73 patients who had undergone ACL reconstruction with a patellar graft 13.5 years after their injury; however, they had excluded patients with additional injuries.
Earlier reports15,27,37 of more cases of patella infera after ACL reconstruction with a BPTP graft are contradicted by the results from this study and those from Wipfler et al. 42 In our study, it was clear that ACL reconstruction affected patellar height, but the clinical implication is not clear.
There are some strengths, but also limitations, in this study. The strengths are the randomized controlled study design with a large study population and a follow-up rate of more than 80% more than 10 years after reconstruction. The fact that the data were assessed both according to the ITT principle and with the exclusion of patients with major additional injuries is also a strength of the study. Further strengths were that the radiological follow-up was performed on both knees and the fact that 3 radiologists assessing the radiographs can be expected to decrease the effect of subjectivity on the reported radiological prevalence of OA.
One limitation is that no power analysis was conducted before the start of the original study. However, the original study design did not include a comparison of OA after more than 10 years; thus, a power analysis would not have taken the objectives of this study into account. Another limitation is that because the method of fixation for the graft types was different, no blinding of the radiologists to the procedure performed was possible, even though the radiologists were blinded to the clinical data and outcomes. The lack of chondral status assessments at the time of the diagnostic arthroscopic procedure or at ACL reconstruction is another limitation. The number of variables tested for their effect as risk factors is also a limitation because randomly significant results might be present in the univariable analysis.
Conclusion
A 3-fold increased prevalence of OA was found after an ACL injury treated with reconstruction compared with the contralateral healthy knee. No differences in the prevalence of OA between the BPTB and quadrupled ST reconstructions were found. An initial meniscus resection was a strong risk factor for OA; the time between injury and reconstruction was not.
Footnotes
Acknowledgements
The authors thank statistician Lina Benson at the Department of Clinical Science and Education, Södersjukhuset, Karolinska Institutet, for statistical analyses and model control.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.