
Abstract
Background:
Autologous osteochondral plug grafts have been used for capitellar osteochondritis dissecans (OCD), and good clinical results have been described. However, little is known about the optimal timing of return to sports.
Purpose:
To investigate the clinical outcomes of open autologous osteochondral plug grafts for capitellar OCD and to address the timing of return to sports.
Study Design:
Case series; Level of evidence, 4.
Methods:
Thirty-three male patients with a mean age at the time of surgery of 13.6 years (range, 11-17 years) and with advanced lesions of capitellar OCD underwent a procedure using open autologous osteochondral plug grafts. All patients played baseball, and the lesion affected their throwing side. Thirteen lesions were arthroscopically classified as International Cartilage Repair Society (ICRS) OCD III and 20 lesions as ICRS OCD IV. The mean size of the lesions (sagittal × coronal) was 16 × 14 mm. One to 3 osteochondral plug grafts, with a mean diameter of 7 mm (range, 5-9 mm), were harvested from the lateral femoral condyle and transplanted to the defects. Patients were allowed to begin throwing after 3 months and to return to sports after 6 months. The mean follow-up was 28.4 months (range, 12-76 months), during which elbow pain, Timmerman and Andrews scores, return to sports, and radiographs were evaluated.
Results:
After surgery, 30 patients (91%) had no elbow pain, and 3 patients (9%) had occasional mild throwing pain. The mean total arc of elbow motion increased significantly from 116° to 133° (P < .05). The mean Timmerman and Andrews score improved significantly from 143 to 190 (P < .05). All except 2 patients returned to a competitive level at which they had previously played after a mean of 6.9 months (range, 6-14 months). One patient chose another sport, and another retired from baseball after high school graduation. All patients achieved graft incorporation, and there was no postoperative enlargement of osteophytes on radiographs. One patient had mild anterior knee pain at the donor site during exercise. The remaining patients had no knee pain. The mean Lysholm score was 99.8.
Conclusion:
The results of this study indicate that an open autologous osteochondral plug graft allows a return to the previous competitive level of throwing by a mean of 7 months postoperatively.
Osteochondritis dissecans (OCD) of the humeral capitellum is a sports-related disorder in young athletes, especially baseball players and gymnasts. Early or stable lesions of the capitellum are usually managed nonoperatively, and acceptable results are generally achieved.8,9,16 On the other hand, cases with advanced or unstable lesions may be better treated with surgical treatment.1,14
Arthroscopic fragment removal generally has been an accepted standard surgical option for capitellar OCD. Takahara et al 14 advocated that reconstruction of the articular surface should be performed if the osteochondral defect was greater than 50% of the capitellar width. Recently, autologous osteochondral plug grafts from the knee have been used to reconstruct articular defects of the capitellum, and good clinical results have been described.4,13,22 However, the timing of return to sports has been described in only a few reports,4,22 varying from 6 to 12 months, and is still controversial. Moreover, to our knowledge, there has been no report about the timing of return to a competitive level at which athletes had previously played. There has also been no report about a suitable osteochondral plug graft size for OCD of the capitellum.
We used open osteochondral plug grafts with a plug diameter of 5 to 9 mm, which would allow patients to start throwing 3 months after surgery and to fully return to sports at 6 months if they had no pain. The purpose of this study was to investigate the clinical outcomes of open autologous osteochondral plug grafts for patients with a capitellar OCD lesion and to address the timing of return to sports.
Materials and Methods
This study was carried out in accordance with the World Medical Association’s Declaration of Helsinki. We obtained institutional review board approval from the ethical committee of our institution for the present investigation. From 2004 to 2011, we performed arthroscopic fragment removal in 17 patients and used open autologous osteochondral plug grafts in 33 patients. The patients underwent a procedure using open autologous osteochondral plug grafts and were all young baseball players with a mean age of 13.6 years (range, 11-17 years) at the time of surgery. Thirty right and 3 left elbows were affected; all involved the patient’s throwing side. There were 14 pitchers, 6 catchers, and 9 fielders, and positions were unknown in 4 patients. The mean age of the patients at the time of clinical presentation was 12.3 years (range, 10-15 years), and the mean period between the onset of symptoms and the initial visit to the outpatient clinic was 20.4 months (range, 1-48 months). Preoperative symptoms consisted of pain with throwing in all patients, limited range of motion in 6 patients, and elbow catching in 4 patients. One patient had prior surgery: fragment fixation with dynamic staples at 1 year before an open autologous osteochondral plug graft.
At the time of clinical presentation, the growth plate of the capitellum was open in 4 patients and closed in 29 patients. According to the radiographic classification system of Minami et al, 10 preoperative anteroposterior plain radiographs of the elbow in 45° of flexion (tangential view) showed radiolucency (grade I) in 1 patient, nondisplaced fragments (grade II) in 13 patients, and displaced or detached fragments (grade III) in 19 patients. There was no patient with subluxation of the radial head. Five patients (15%) had visible osteophytes at the site of the coronoid fossa. On the basis of magnetic resonance imaging (MRI) criteria of unstable capitellar OCD lesions, 12 T2-weighted fat-suppressed sagittal and coronal images showed instability in all patients.
Surgical Technique and Operative Findings
The OCD lesions were evaluated arthroscopically and classified as International Cartilage Repair Society (ICRS) OCD III (n = 13) and OCD IV (n = 20). 2 The mean size of the lesions (sagittal × coronal) was 16 × 14 mm (range, 8-20 × 9-20 mm), and the mean defect size was 183 mm2 (range, 59-201 mm2), assuming an ellipse. Intra-articular free fragments (range, 1-7 fragments) were observed in 20 patients (61%). One patient whose preoperative radiographs showed nondisplaced fragments (grade II) had an intra-articular free fragment. All free fragments were removed under arthroscopic surgery. When the OCD lesion was wider than 10 mm, we used open autologous osteochondral plug grafts.14,17 The upper arm was placed on the operative bed with the shoulder abducted and the elbow fully flexed. A 4- to 6-cm posterolateral oblique skin incision13,15 was made, and the anconeus muscle was split to approach the capitellum. After removal of the unstable fragments, osteochondral plug grafts were harvested from the ipsilateral femoral condyle at the level of the patellofemoral joint using a special device (Osteochondral Autograft Transfer System [OATS], Arthrex Inc). The mean size of the osteochondral plugs was 7 mm (range, 5-9 mm) in diameter and 14 mm (range, 9-20 mm) in length. One to 3 plugs (mean, 1.8 plugs) were grafted. We first grafted at the anterolateral area of the articular defect and then at the posteromedial area if the remaining articular defect was large enough to graft. Ten patients received 1 graft, and 20 patients received 2 grafts. Three patients who had extremely large defects received 3 grafts. We inserted the osteochondral plug grafts so that the articular surface should be slightly depressed, rather than prominent, relative to that of the original capitellum, and the step-off of the articular surface was less than 1 mm (Figure 1). The mean percentage of the reconstructed area per lesion was 48% (range, 21%-100%), which was calculated as (total surface area of the grafts × 100%)/(surface area of the lesion). We performed subcutaneous ulnar nerve transposition in 1 patient. We included this single case because the patient’s main problem was lateral pain caused by capitellar OCD, and this subcutaneous ulnar nerve transposition did not affect the results of the autologous osteochondral plug graft. One of 5 patients with visible osteophytes underwent osteophyte resection because of a restriction of elbow motion. The others did not because of no limitation of elbow motion. There were no complications during surgery.

Operative technique. Two 6-mm osteochondral plug grafts were used.
Postoperative Management
The elbow was immobilized in 90° of flexion with the forearm in a neutral position for 2 weeks after surgery. General stretching, such as the sleeper stretch, 20 or core and hip stretches were performed to resolve general tightness, especially of the posterior shoulder, core, and hip. Gentle resistance exercises were begun at 2 months and progressed to full resistance after 3 months. Throwing activity was initiated at 3 months. 22 A full range of sports activities was permitted at 6 months. Regarding the knee joint, weightbearing on the knee was allowed as tolerated, but patients were instructed to protect the knee from vigorous flexion for 3 weeks. When the patients had no symptoms of the donor knee, running was permitted after 1 month. The mean follow-up was 28.4 months (range, 12-76 months).
Postoperative Assessment
The postoperative assessment included elbow pain, range of elbow and forearm motion, grip strength, the clinical rating system of Timmerman and Andrews, 19 time to return to sports, evaluation of the radiographs, and functional evaluation of the donor knee.
The assessment of elbow pain as established by the Japanese Orthopaedic Association 3 was modified by dividing results into 3 categories 14 : none (no pain), mild (pain only after intense activity, such as sports or work), and moderate or severe (pain after daily activities or even at rest). The Timmerman and Andrews 19 clinical rating system consisted of both subjective (pain, swelling, locking and/or catching, and return to previous sports activities) and objective (range of motion) evaluations. On the basis of the clinical scores, overall results were classified according to the following 4 categories: excellent (180-200), good (160-179), fair (120-159), or poor (<120). The assessment of return to a former sports activity, as established by the American Shoulder and Elbow Surgeons, 7 was modified by dividing results into 3 categories 14 : competitive (complete return), recreational (incomplete return), and substantial limitation (change or cessation of the sport).
All patients obtained routine anteroposterior, lateral, and tangential view radiographs, which were evaluated for graft incorporation, secondary osteoarthritic changes, deformity of the radial head, and dislocation or subluxation of the radial head. Graft incorporation on plain radiographs was defined by the disappearance of the graft line.
The knee evaluation consisted of local findings of the donor knee using the Lysholm knee scoring scale. 18 The Lysholm score (range, 0-100) was graded as excellent (>94), good (84-94), fair (60-83), or poor (<60).
Statistical Analysis
We performed comparisons between preoperative and postoperative elbow and forearm range of motion, grip strength, and Timmerman and Andrews scores using the paired t test. We compared the time in return to throwing between the patients with and without visible osteophytes and between ICRS OCD III and OCD IV using the Mann-Whitney U test. We also compared the time to return to throwing with the number of plugs using 1-way ANOVA. The level of significance was set at a probability value of <.05.
Results
Clinical Evaluation
At the final follow-up visit, 30 patients (91%) had no elbow pain, and 3 patients (9%) had mild elbow pain. Preoperative and postoperative active range of elbow and forearm motion and grip strength are shown in Table 1. The mean postoperative active range of elbow and forearm motion, except supination, significantly increased (P < .05). The mean grip strength compared with that on the unaffected side significantly increased postoperatively (P < .05). The mean subjective, objective, and total scores of Timmerman and Andrews significantly improved from 67 (range, 50-70) to 99 (range, 80-100), 76 (range, 30-100) to 91 (range, 35-100), and 143 (range, 100-170) to 190 (range, 135-200), respectively (all P < .05). The overall evaluation result was excellent in 28 patients (85%), good in 1 patient (3%), and fair in 4 patients (12%).
Comparison Between Preoperative and Postoperative Clinical Evaluations a
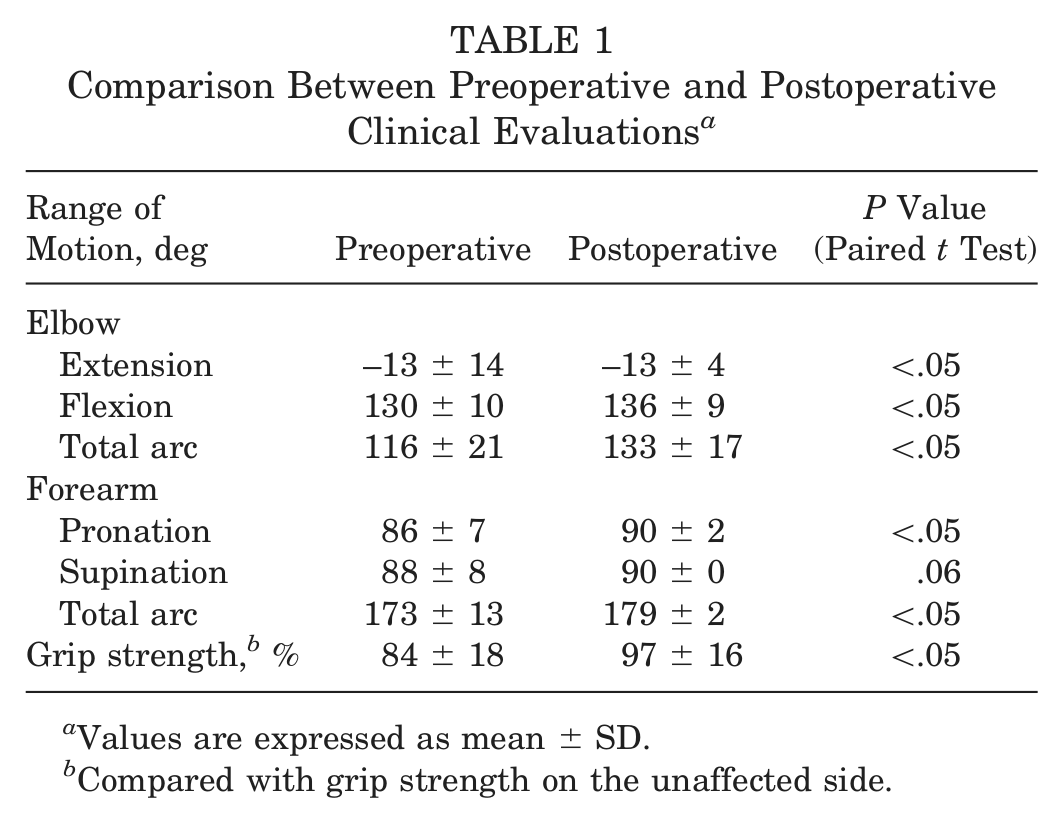
Values are expressed as mean ± SD.
Compared with grip strength on the unaffected side.
Radiographic Evaluation
Plain radiographs showed that the graft line had disappeared at a mean of 3.8 months (range, 3-4 months) postoperatively in all patients. At final follow-up, there was no patient with loose bodies, subluxation of the radial head, or heterotopic ossification. No postoperative radiographs, including 5 patients with visible osteophytes preoperatively, showed new formation or enlargement of osteophytes in the elbow joint (Figure 2).
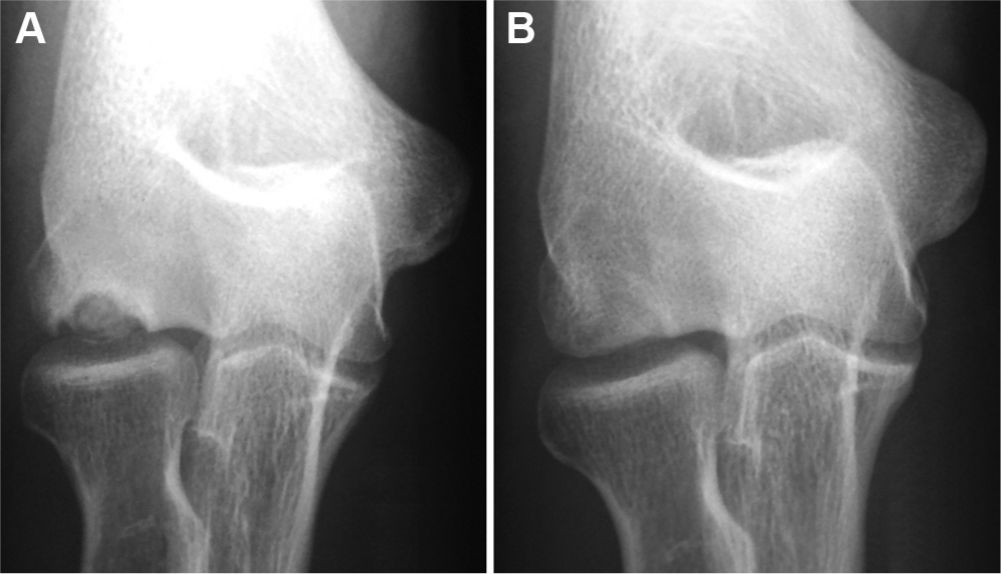
Results for a 15-year-old baseball player with ICRS OCD IV lesion. (A) Preoperative plain anteroposterior radiograph with the elbow in 45° of flexion showing displaced fragments. (B) Plain radiograph at 24 months postoperatively showing local flattening of the capitellum but no visible osteophytes and no progressive secondary osteoarthritic change.
Return to Sports
Thirty-one patients (94%) returned to baseball at a mean of 6.9 months (range, 6-14 months) postoperatively. All 31 patients returned to the competitive level at which they had previously played. The remaining 2 patients did not return to baseball. One patient with an excellent outcome chose to play kyudo (Japanese archery) at 3 months postoperatively and played at a competitive level at 5 months postoperatively. Another patient with a fair outcome retired from baseball after high school graduation.
There was no significant difference between patients with and without visible osteophytes (with visible osteophytes: mean, 6.6 months [range, 6-8 months]; without visible osteophytes: mean, 7.0 months [range, 6-14 months]; P = .71) and between ICRS OCD III and ICRS OCD IV (ICRS OCD III: mean, 7.2 months [range, 6-14 months]; ICRS OCD IV: mean, 6.7 months [range, 6-13 months]; P = .67). There was no significance in the number of plugs (1 plug: mean, 6.7 months [range, 6-10 months]; 2 plugs: mean, 7.2 months [range, 6-14 months]; 3 plugs: mean, 6.0 months [all 6 months]; P = .61).
Functional Evaluation of the Donor Knee
One patient had mild anterior knee pain during exercise but no local findings in the donor knee. No restriction in range of knee motion was found in any patient. The mean Lysholm score was 99.8 (range, 95-100), and all knees were graded as excellent. The donor knee was not evaluated on plain radiographs because none of the patients had disturbances in the donor knee.
Discussion
The diameters of osteochondral plug grafts reported in the literature range from 3.5 to 9 mm for capitellar OCD, and the results from using them are reported generally to be excellent.4,13,22 We used osteochondral plug grafts with a mean diameter of 7 mm, and the mean Timmerman and Andrews scores improved significantly from 143 to 190, with excellent or good clinical results in 88%. These results were similar to those of previous reports (Table 2). To our knowledge, there were no reports about the timing of return to the previous competitive level of sports; however, 94% of patients in our study returned to their previous competitive level at a mean of 6.9 months.
Results of Osteochondral Autograft Reconstructions a
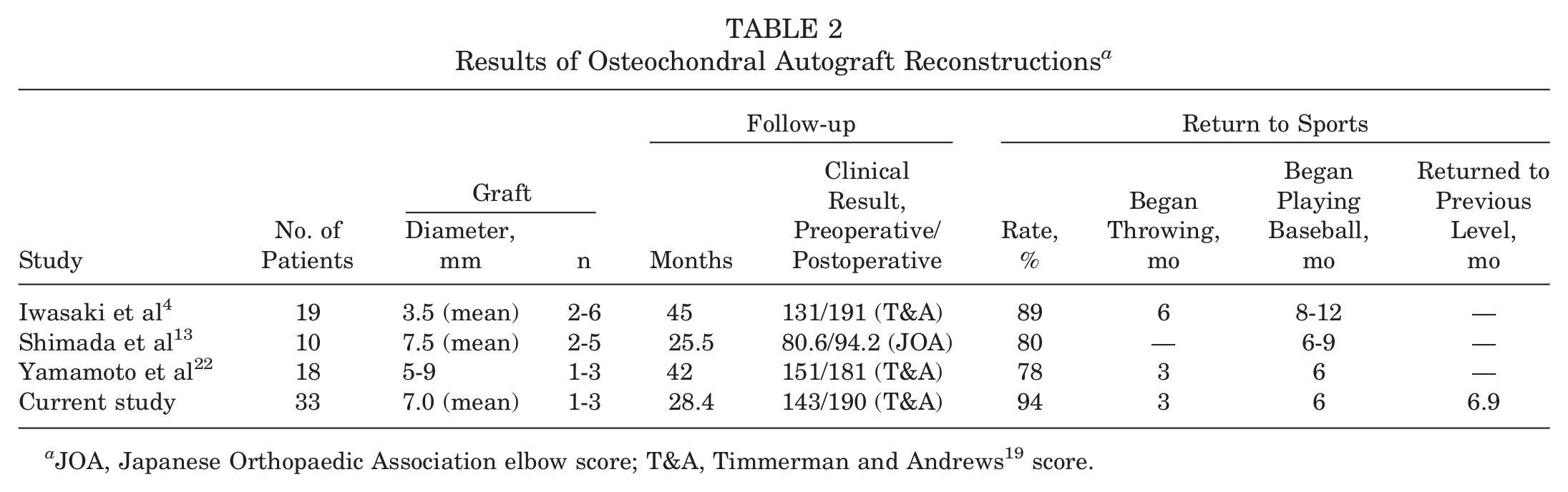
JOA, Japanese Orthopaedic Association elbow score; T&A, Timmerman and Andrews 19 score.
Plain radiographs showed graft incorporation at a mean of 3.8 months postoperatively. Yamamoto et al 22 used grafts with a mean diameter of 5 to 9 mm, and the abnormal signal in the subchondral bone on MRI became normal at 3 months after surgery for all patients. On the other hand, Iwasaki et al 5 used osteochondral plug grafts with a mean diameter of 3.5 mm and reported that fluid surrounding the graft on MRI was found in all 10 patients at 3 months postoperatively and in 4 of 10 patients after 6 months. These results indicate that graft size may affect graft incorporation.
We reconstructed almost half of the area of the articular defects in this study and obtained clinically good results. In previous reports, the outcomes of fragment removal were satisfactory if the articular defect was less than 10 mm.14,17 These findings indicate that it is not clinically required to reconstruct all of the articular defect and that reconstruction of a large articular defect results in a small articular defect of less than 10 mm. Therefore, we believe that a few large plug grafts are enough to reconstruct a capitellar articular defect.
Reports vary on the time required to return to sports. Iwasaki et al4,5 allowed patients playing baseball to begin to throw after 6 months and to fully return to the previous level of throwing activity by 8 to 12 months. On the other hand, Yamamoto et al 22 allowed gentle overhand throwing after 3 months and full throwing after 6 months. The former used grafts with a diameter of 3.5 mm, and the latter used 5- to 9-mm grafts. We allowed throwing after 3 months and a full return to sports after 6 months, with 94% of patients returning to their previous competitive level at a mean of 6.9 months. The results of Yamamoto et al 22 and ours would indicate that osteochondral plug grafts with a diameter of 5 to 9 mm allow a return to the previous competitive level. The timing of return to sports is dependent on the bony union of the grafts. Our results suggest that a few large grafts may obtain bony union earlier and allow an earlier return to sports.
Short- to medium-term follow-up studies of osteochondral transplantation have shown no progressive or secondary osteoarthritic changes in the elbow radiographically.4,13,22 Vogt et al 21 reported 8 cases at 8- to 14-year follow-up and found 2 patients who showed mild radiographic signs of osteoarthritis. Our patients might have a progression of osteoarthritic changes over years, which we have not yet observed in the short-term observation period.
An obvious disadvantage of the described procedure is the necessity of exposing the knee joint. Iwasaki et al 6 reported functional recovery of the donor knee at a mean follow-up of 26 months after small (2.7-6.0 mm) osteochondral plug graft harvest. The Lysholm knee score was 99.6, and the International Knee Documentation Committee (IKDC) evaluation form characterized healing as normal. Nishimura et al 11 reported that they harvested 6- to 8-mm grafts, and the mean Lysholm score of donor knees after 2 years was 100, with no osteoarthritic change recognized on radiographs. We harvested 5- to 9-mm grafts, and the mean Lysholm score of donor knees at final follow-up was 99.8. Harvesting osteochondral plug grafts did not exert adverse effects on the donor knee. However, Vogt et al 21 harvested 9- to 11-mm grafts, and 3 patients had occasional mild knee pain, with a mean Lysholm score of 89.9 after 8 to 14 years. The risks of donor site problems may increase if the graft diameter is larger and the follow-up time is longer.
In summary, various autologous osteochondral plug graft sizes have been used for advanced large lesions of capitellar OCD with good clinical results. However, our results indicate that open autologous osteochondral plug grafts with a few plugs with a mean plug diameter of 7 mm obtains early union and allows a return to the previous competitive level of throwing by a mean of 7 months.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.