
Abstract
Background:
Osteochondral allograft (OCA) transplantation is an effective treatment for defects in the medial femoral condyle (MFC), but the procedure is limited by a shortage of grafts. Lateral femoral condyles (LFCs) differ in geometry from MFCs but may be a suitable graft source. The difference between articular surface locations of the knee can be evaluated with micro–computed tomography imaging and 3-dimensional image analysis.
Hypothesis:
LFC OCAs inserted into MFC lesions can provide a cartilage surface match comparable with those provided by MFC allografts.
Study Design:
Controlled laboratory study.
Methods:
Twenty MFCs and 10 LFCs were divided into 3 groups: 10 MFC recipients (MFCr), 10 MFC donors (MFCd), and 10 LFC donors (LFCd). A 20-mm defect was created in the weightbearing portion of the MFCr. Two grafts, 1 MFCd and 1 LFCd, were implanted sequentially into each MFCr. Micro–computed tomography (μCT) images of the MFCr were acquired and analyzed to compare the topography of the original recipient site with the MFCd- and LFCd-repaired sites. Three-dimensional transformations were defined to register the defect site in the 3 scans of each MFCr. Vertical deviations from each voxel of the graft cartilage surface, relative to the intact recipient cartilage surface, were calculated and assessed as root mean square deviation and percentage graft area that was proud, sunk, and within the “acceptable” distance (±1.00 mm). The effect of repair (with MFC vs with LFC) on each of the surface match parameters is presented as mean ± SD and was assessed by t test: height deviation over area (root mean square, mm), graft area acceptable (%), area unacceptably proud (%), area unacceptably sunk (%), step-off height over circumference (root mean square, mm), graft circumference acceptable (%), circumference unacceptably proud (%), and circumference unacceptably sunk (%). Percentage data were arcsin transformed before statistical testing. An alpha level of 0.05 was used to conclude if variations were statistically significant.
Results:
MFCr defects were filled with both orthotopic MFCd and nonorthotopic LFCd. Registered μCT images of the MFCr illustrate the cartilage surface contour in the sagittal and coronal planes, in the original intact condyle, as well as after OCA repairs. Specimen-specific surface color maps for the MFCr after implant of the MFCd and after implant of LFCd were generally similar, with some deviation near the edges. On average, the MFCr site exhibited a typical contour, and the MFCd and LFCd were slightly elevated. Both types of OCA—MFCd and LFCd—matched well, showing overall height deviations of 0.63 mm for area and 0.47 mm for step-off, with no significant difference between MFCd and LFCd (P = .92 and .57, respectively) and acceptable deviation based on area (87.6% overall) and step-off (96.7% overall), with no significant difference between MFCd and LFCd (P = .87 and .22, respectively). A small portion of the implant was proud (12.1% of area and 2.6% of circumference step-off height), with no significant difference between MFCd and LFCd (P = .26 and .27, respectively). A very small portion of the implant area and edge was sunk (0.3% of area and 0.6% of circumference), with no significant difference between MFCd and LFCd (P = .29 and .86, respectively).
Conclusion/Clinical Relevance:
The achievement of excellent OCA surface match with an MFCd or LFCd graft into the common MFCr site suggests that nonorthotopic LFC OCAs are acceptable graft options for MFC defects.
Articular cartilage lesions in the knee are a relatively common finding in young patients with knee pain and swelling.9,14,20,49 As articular cartilage lacks the ability to heal, articular cartilage defects can lead to degenerative arthritis and knee dysfunction. There are many treatment options for full-thickness articular cartilage defects, including microfracture,16,18,34,47 osteoarticular autograft transplant,5,18,31 autologous chondrocyte implantation,1,2,40,53 and osteochondral allograft transplant. ¶
Fresh osteochondral allograft transplantation was first described in the early 20th century28,29 and has been a viable treatment option for more than 25 years. # In the past, the availability of suitable grafts and the need to implant them on an urgent basis, once harvested, limited their use. However, with newer technology and storage media, chondrocyte viability can be maintained for several weeks, allowing surgeons to implant grafts on more of an elective basis. 51 Articular cartilage lesions of the medial femoral condyle (MFC) account for the majority of cartilage lesions in the knee, outnumbering lateral femoral condyle (LFC) lesions as much as 6-fold.9,14,20,49 As a result, MFC allografts are in most demand. Statistics from the Joint Restoration Foundation (2012; data on file) indicate that 97% of osteochondral allografts requested were for MFC grafts; in contrast, 75% of the foundation’s grafts that are suitable and made available to surgeons are LFCs.
When performing an osteochondral allograft transplant, most surgeons demand that the graft being used match the site of the defect (ie, right MFC allograft for a right MFC lesion), although some degree of mismatch in geometry appears acceptable. While finite element models of resultant biomechanics predict general trends on the effects of articular geometry, 10 assumptions about actual tissue structure and properties for individual cases necessitate experimental studies. Osteochondral grafts with articular surface recessed by 1 mm or less in human knees appear to lead to acceptable outcomes. 35 Computer simulation and cadaveric/animal specimen studies indicate that slightly recessed grafts could still restore contact pressure to nearly normal levels, whereas elevated grafts 0.5 to 1 mm proud lead to as much as a 50% increase in contact pressure.19,23-25,52 Elevated osteochondral grafts can have deleterious effects, leading to the development of degenerative changes in the knee. 21 Thus, it appears that a geometrical match within 1-mm recession and 0.5- to 1-mm elevation is acceptable.
The geometries of LFCs and MFCs have been studied extensively and have been shown to differ in shape, curvature, and size.11,36,42,43,46 In addition, articular cartilage thickness on femoral condyles has also been studied extensively, with studies showing differences between LFCs and MFCs, as well as variations with sex, race, weight, height, and applied stress during weightbearing.4,7,13,30,38,39,41,45 However, several characteristics of LFCs make them a potentially suitable graft source for osteochondral lesions in the MFC. The articular cartilage on the LFC, except in the area of the sulcus terminalis, is as thick or thicker than corresponding areas on the MFC. 30 The LFC is wider than the MFC, which can provide the needed tissue for lesions that are larger than 25 mm in the medial-lateral width. Approximately 75% of the grafts that are larger than 26 mm in the medial-to-lateral dimension are LFC (data on file; Joint Restoration Foundation). The LFC has a superficial zone with better function than the corresponding region of the medial side with normal aging, as indicated by higher tensile modulus and strength.37,48
The present study tested the hypothesis that LFC allografts inserted into MFC lesions can provide a cartilage surface match that is equivalent to that provided by MFC allografts and within geometric acceptability. To address this aim, the surface geometries of intact human MFC recipient condyles and those repaired with MFC and LFC allografts ex vivo were compared.
Materials and Methods
We designed a study to determine whether an LFC allograft can favorably compare with an MFC allograft when transplanted into a defect in an MFC. Before the study, a power analysis was computed to help determine sample size. For the primary outcome of comparing surface geometry, we assumed that the standard deviation of the matched MFC allograft relative to the original surface was 0.5 mm. To detect a difference of 0.75 mm, slightly less than the deviation criterion of 1.0 mm, the required sample size is 8, and 10 was chosen to provide a safety factor. In addition, 10 allowed assessment of the percentage (±10%) of grafts that did not meet the tolerance criteria of ±1 mm.
Thirty frozen human knee condyles (20 MFCs and 10 LFCs) were provided by the Joint Restoration Foundation. All specimens were inspected to ensure that there were no visible defects in the articular surfaces. Ten MFCs were used as recipient sites; the other 10 MFCs were used to create donor osteochondral plugs, as were 10 LFCs. All donor and recipient samples that were matched in the study corresponded to different individuals. To ensure that the created 20-mm defect would have normal articular cartilage on the periphery, MFCs that were between 24 and 29 mm were selected to be the MFC recipients. All remaining condyles (MFCs and LFCs) were greater than 20 mm in width, with the LFC grafts all being wider than the MFC donor and recipient grafts. The donor and recipient grafts were not matched by size but side (right and left) to make the MFC donor grafts ipsilateral and the LFC donor grafts contralateral to the recipient condyle (right MFC matched to right MFC; right LFC matched to left MFC recipient).
Osteochondral Recipient Sites
Each of the 10 intact MFC recipient specimens (ie, before creating an osteochondral defect) was photographed and scanned by micro–computed tomography (μCT). Scanning was performed on a Skyscan 1076 at 18-μm isotropic voxel size by applying an electrical potential of 100 kVp and a current of 100 μA and by using a 0.038-mm copper and 0.5-mm aluminum filter.
After the baseline scans, a 20-mm defect was created along the weightbearing portion of each recipient MFC. The defects were created by 3 orthopaedic surgeons experienced in osteochondral allograft transplantation using Allograft OATS Instrumentation (Arthrex). After a drill-tip guide pin was inserted, a defect was drilled to a depth of 6 to 9 mm, with the long axis of the defect perpendicular to the articular surface. The defect was positioned so that the native articular cartilage surrounding the defect was intact, thus creating a contained defect.
Osteochondral Allograft Transplantation
The same 3 orthopaedic surgeons performed the implantations. Osteochondral cylindrical donor cores (20-mm diameter) were harvested from a site-matched region of an MFC allograft and from an area of an LFC allograft that grossly matched the contour along the MFC at the site of the defect. Because of concerns with alterations in the recipient MFC specimens while the first implanted graft was being removed, the order of implants was varied so that half had MFC allografts placed first and the other half had LFC allografts placed first. To match the donor core to the recipient site, the depth of each lesion was measured in 4 quadrants. The donor core plugs were cut to the appropriate depth of the defect and then inserted with a tamp. The surgeons transplanted the grafts to their perceived best fit, attempting to minimize circumferential step-off and optimize surface contour restoration. All surgeons felt that the transplants were anatomic once the procedures were completed.
Each transplanted/repaired recipient MFC was again photographed and imaged by μCT. After insertion of the first donor allograft plug and μCT imaging, the initial allograft plug was atraumatically removed, leaving an empty MFC defect. The defect was then subsequently implanted with the second donor allograft plug. The recipient MFCs were then imaged again with μCT.
Image Analysis
From the μCT image data, geometrical analyses were performed on the 10 recipient MFCs, 10 LFC-repaired MFCs, and 10 MFC-repaired MFCs to characterize the degree of surface match. The software packages DataViewer and CTAnalyser (Skyscan) were used to visualize the data sets, and MATLAB (MathWorks) was used for all image processing. Each set of 3 images was registered to a cylindrical coordinate system, aligned with the axis of the cylindrical defect and the medial-lateral direction defining the angle (180°-0°). The cartilage surface of each image was identified by thresholding. From these surfaces, 2 metrics of surface match were determined.
First, the height difference between the repair surface and the intact surface was mapped and summarized. Differences between the repair and intact samples were calculated by subtracting the surface positions, and color maps showing surface deviations were created. Thus, positive distances indicated that the repair surface was elevated (proud), and negative distances indicated that the repair surface was recessed (sunk). The overall surface deviation (either proud or recessed) was computed as the root mean square (devRMS). The percentage area of the transplanted plug that was in the range of acceptable tolerance of ±1 mm (Aacc) was calculated, as were the percentage areas that were >1 mm proud and <–1 mm sunk (Aunacc,proud and Aunacc,sunk, respectively).
Second, the step-off in height between the repair surface and the intact surface was mapped and summarized. This height was calculated in 2° increments circumferentially as the local difference in height between implant and host, correcting for the difference in height between these positions in the intact recipient sample. The same sign convention was used for step-off heights to indicate if the graft was locally proud or sunk, relative to the host. Also analogous to the calculations for area, those for step-off were mapped and then summarized as overall circumferential root mean square height deviation (hstep,RMS), percentage circumference in the acceptable step-off range of ±1 mm (Cacc), as well as percentage circumferences that were >1 mm proud and <–1 mm sunk (Cunacc,proud and Cunacc,sunk, respectively).
Statistical Analyses
The effect of repair (with MFC vs with LFC) on surface and step-off match parameters (devRMS, Aacc, Aunacc,proud, Aunacc,sunk, hstep,RMS, Cacc, Cunacc,proud, and Cunacc,sunk) is presented as mean ± SD and was assessed by t test. Percentage data were arcsin transformed before statistical testing. An alpha level of 0.05 was used to conclude if variations were statistically significant.
Results
Tables 1 and 2 include data on surface area and step-off for all 20 allografts (10 MFC recipients [MFCr]; 10 MFC donors [MFCd]; 10 LFC donors [LFCd]). As shown for a typical sample, MFCr defects were filled with both orthotopic donor MFC and nonorthotopic donor LFC (Figure 1). In sagittal (Figure 2, A-C) and coronal (Figure 2, D-F) planes, the μCT images delineated surface contours for the intact recipient (Figure 2, A and D) and the repair with an MFC donor (Figure 2, B and E) and an LFC donor (Figure 2, C and F). Specimen-specific surface color maps were generally similar for the MFCr after implant of the MFCd (Figure 3A) and after implant of LFCd (Figure 3B). Histogram analyses of the color maps indicated the distribution of surface deviations for the MFCd (Figure 3C) and LFCd (Figure 3D). Circular maps of step-off quantified the extent of deviation near the edges (Figure 3, E and F).
Effect of Donor Condyle on Osteochondral Allograft Repair Topography: Surface Area a
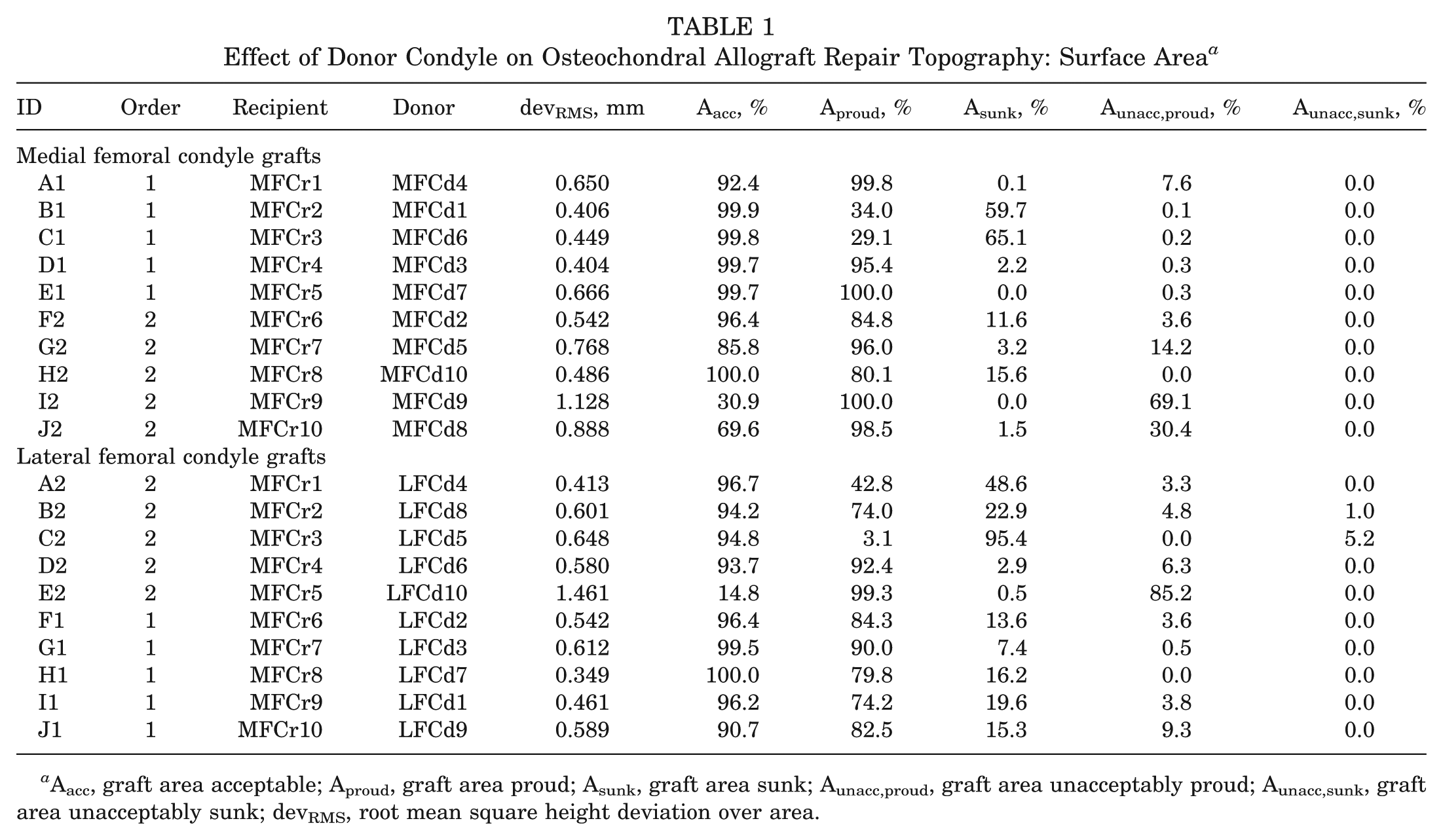
Aacc, graft area acceptable; Aproud, graft area proud; Asunk, graft area sunk; Aunacc,proud, graft area unacceptably proud; Aunacc,sunk, graft area unacceptably sunk; devRMS, root mean square height deviation over area.
Effect of Donor Condyle on Osteochondral Allograft Repair Topography: Circumferential Step-off a
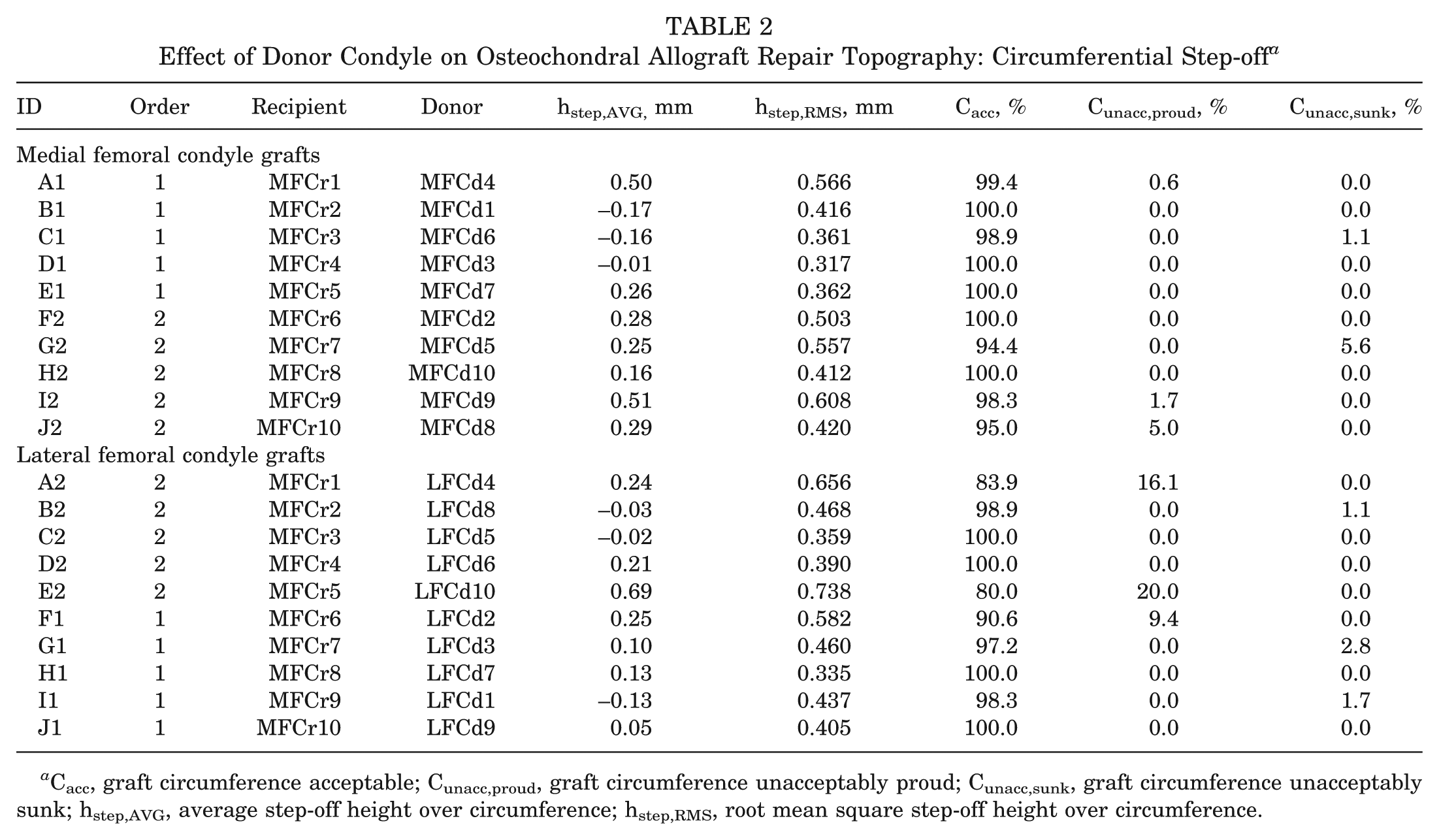
Cacc, graft circumference acceptable; Cunacc,proud, graft circumference unacceptably proud; Cunacc,sunk, graft circumference unacceptably sunk; hstep,AVG, average step-off height over circumference; hstep,RMS, root mean square step-off height over circumference.
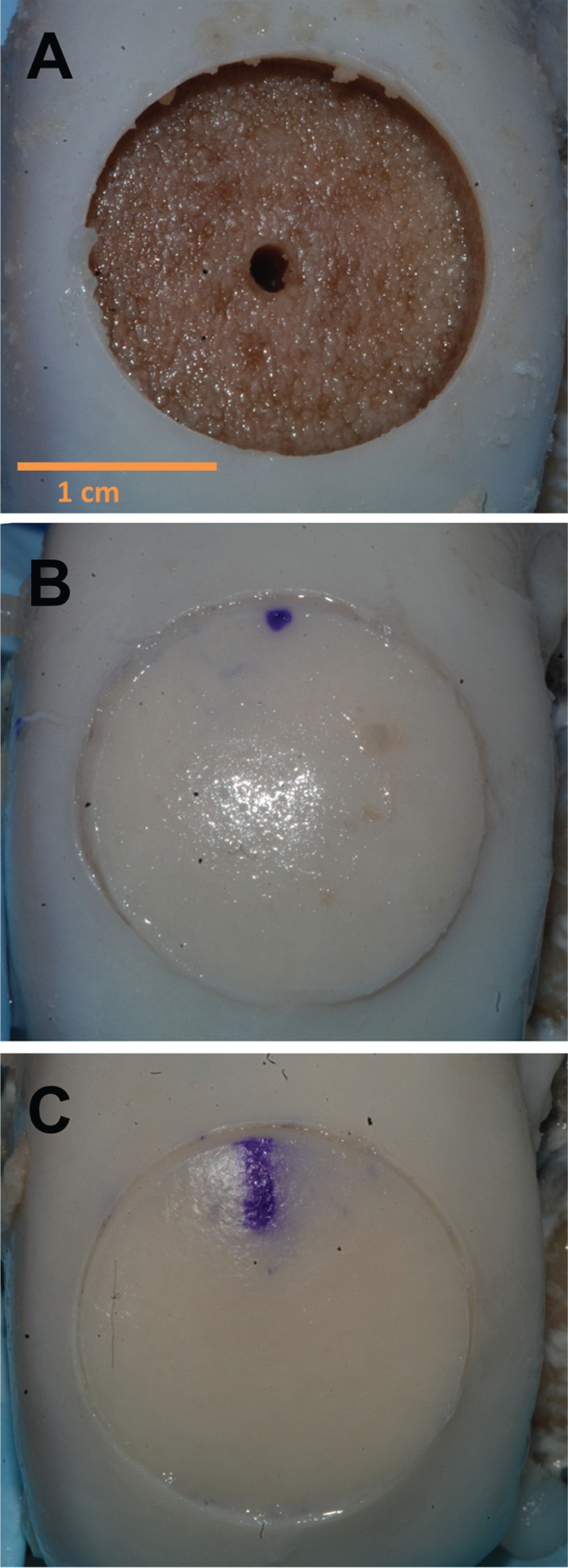
En face gross images of a representative recipient medial femoral condyle sample. (A) Medial femoral condyle recipient after creation of a defect, showing the remaining guide wire hole at the center. (B) Defect filled with an osteochondral allograft from a medial femoral condyle donor. (C) Defect filled with an osteochondral allograft from a lateral femoral condyle donor.
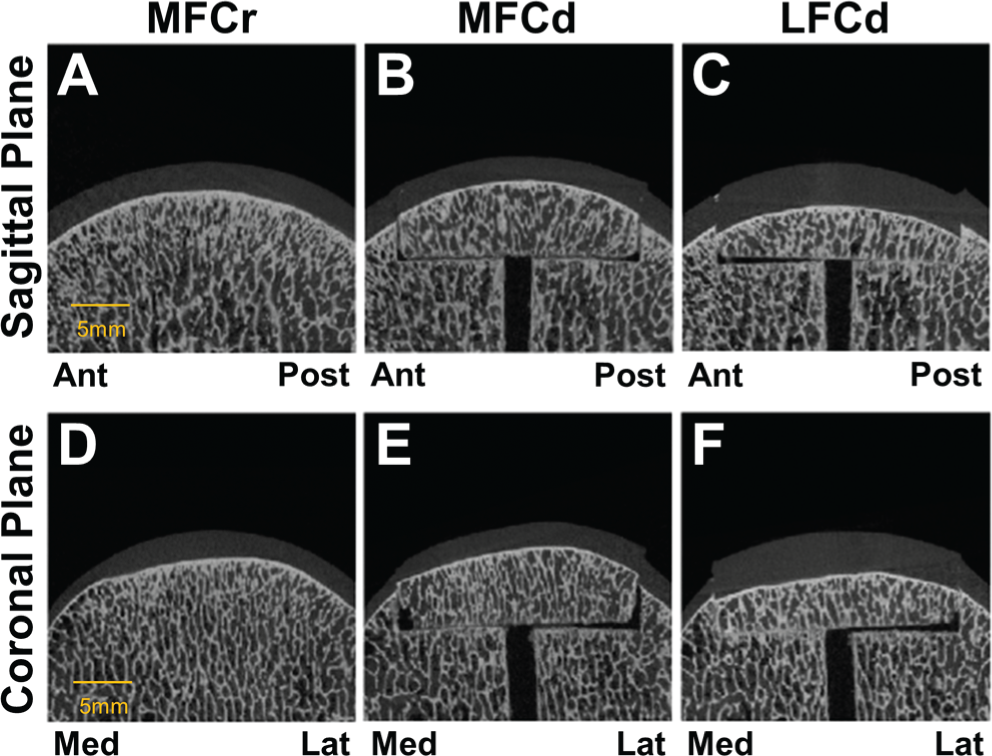
Registered micro–computed tomography images of a representative sample. (A, B, C) Sagittal slices and (D, E, F) coronal slices of a medial femoral condyle recipient (MFCr) sample. The black region is air, the white areas are subchondral bone, and the gray region between air and bone is articular cartilage. (A, D) Intact MFCr before defect creation. (B, E) Recipient site after repair with medial femoral condyle donor (MFCd) tissue. (C, F) Recipient site after repair with lateral femoral condyle donor (LFCd) tissue.
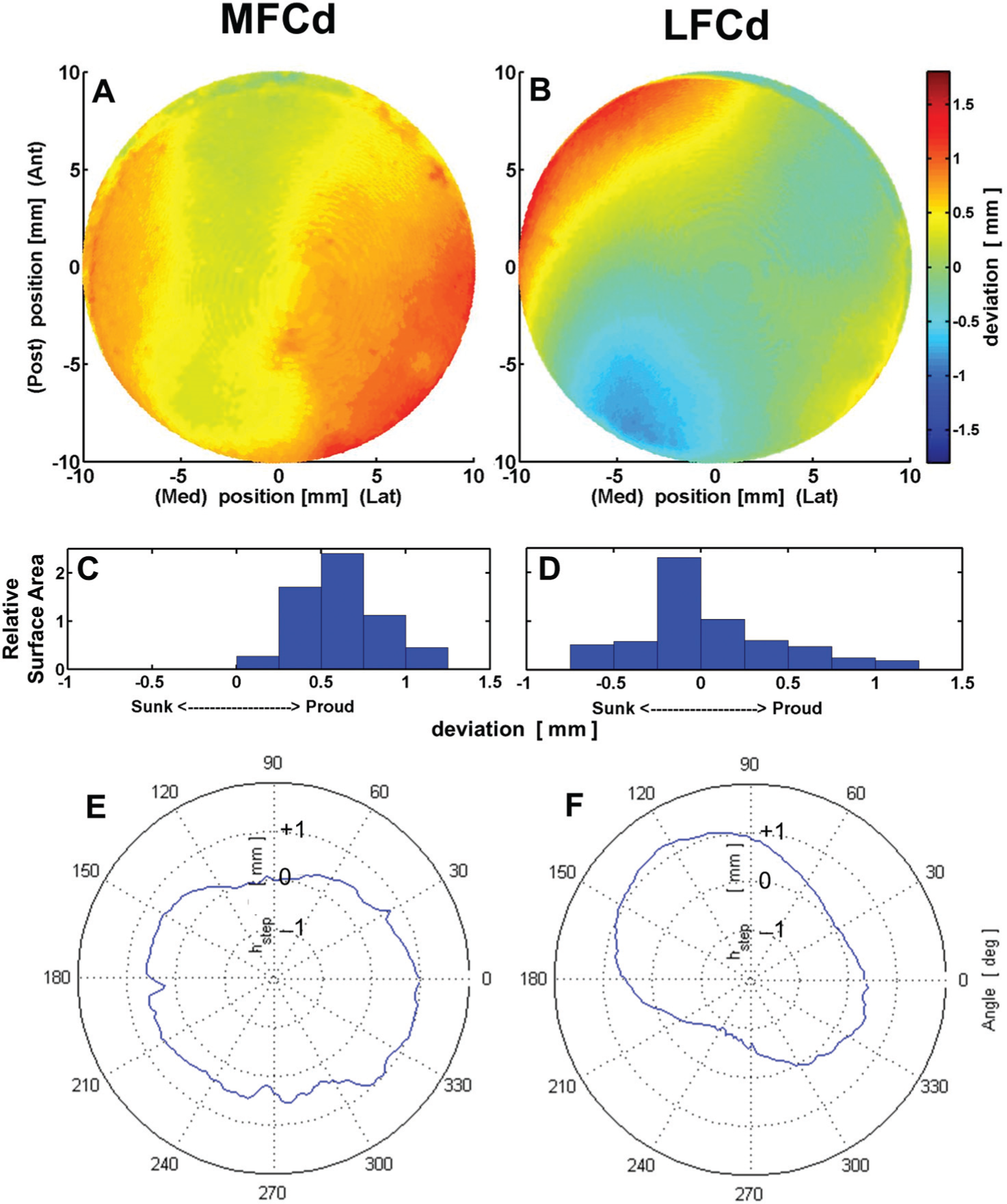
Cartilage surface deviation from intact recipient for representative (A, C, E) medial femoral condyle donor (MFCd) and (B, D, F) lateral femoral condyle donor (LFCd) implants, shown in Figure 2. (A, B) Color maps of height deviation. (C, D) Histograms of height deviation. (E, F) Polar plots of step-off heights.
The cartilage surface locations indicated that the repairs resulted in acceptable matches both in absolute terms and in comparing MFCd and LFCd (Table 3). On average, the MFCr site exhibited a typical contour, and the MFCd and LFCd were slightly elevated. Both types of osteochondral allograft, MFCd and LFCd (Figure 3), matched well, showing an overall height deviation of 0.63 mm for area and 0.47 mm for step-off, with no difference between MFCd and LFCd (P = .92 and .57, respectively) and acceptable deviation based on area (87.6% overall) and step-off (96.7% overall) with no significant difference between MFCd and LFCd (P = .87 and .22, respectively). A small portion of the implant was proud (12.1% of area and 2.6% of circumference step-off height), with no significant difference between MFCd and LFCd (P = .26 and .27, respectively). A very small portion of the implant area and edge was sunk (0.3% of area and 0.6% of circumference) with no significant difference between MFCd and LFCd (P = .29 and .86, respectively). A trend was observed toward better restoration of the topographic surface area with the first implant, but it did not reach statistical significance when compared with order 2 implants (P = .07). Comparing the circumferential step-off (Cacc) between order 1 and order 2 implants, there was no statistical difference (P = .24).
Surface Area and Circumferential Step-off Height Parameters of Recipients Implanted With Medial and Lateral Femoral Condyle Grafts a
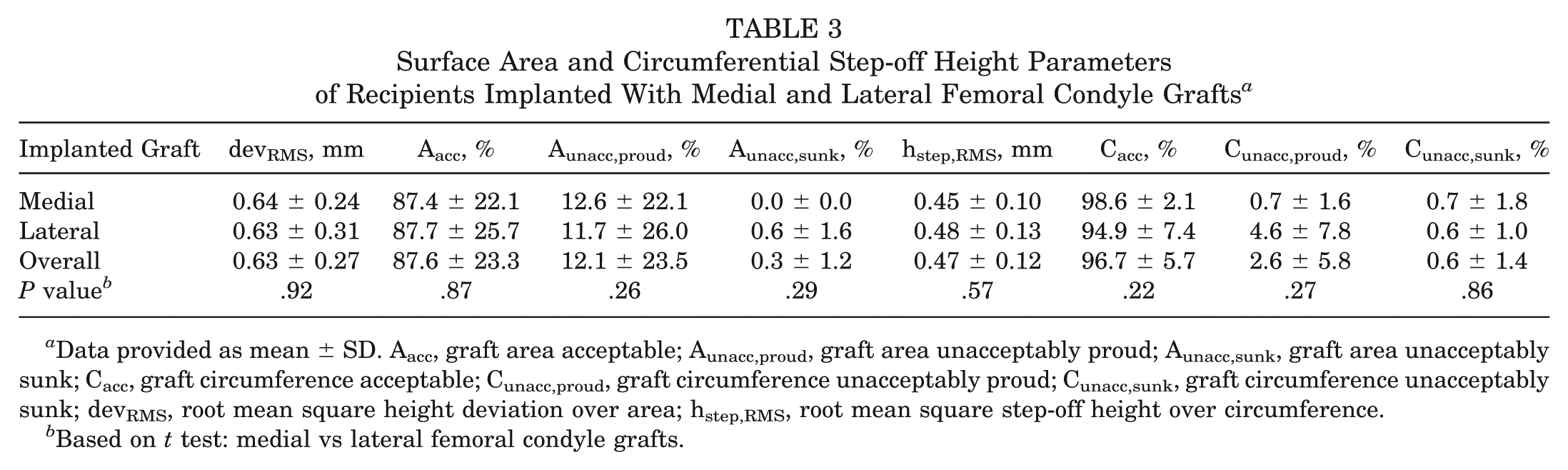
Data provided as mean ± SD. Aacc, graft area acceptable; Aunacc,proud, graft area unacceptably proud; Aunacc,sunk, graft area unacceptably sunk; Cacc, graft circumference acceptable; Cunacc,proud, graft circumference unacceptably proud; Cunacc,sunk, graft circumference unacceptably sunk; devRMS, root mean square height deviation over area; hstep,RMS, root mean square step-off height over circumference.
Based on t test: medial vs lateral femoral condyle grafts.
Discussion
The purpose of this study was to determine whether an osteochondral allograft from an LFC could be transplanted into an MFC defect with restoration of the articular surface as well as an MFC graft. The achievement of excellent osteochondral allograft surface match with an MFC or LFC donor graft into the common MFC recipient site suggests that nonorthotopic LFC-to-MFC transplants could lead to outcomes similar to orthotopic MFC-to-MFC transplants. The placement of grafts—while generally within the 1-mm deviation target but more often proud than sunk for both MFCd and LFCd—may reflect the surgeons’ experience. With postsurgical joint loading, an osteochondral allograft may settle slightly into the recipient site. The reason for the slight difference in topographic surface area restoration due to the order of implants remains to be established, but it may be due in part to the inability to visualize the native articular surface when the order 2 plug is selected to fill the defect.
The decision to choose an acceptable range of ±1 mm with respect to the 3-dimensional surface topography and recipient-allograft articular step-off was based on biomechanical and clinical studies.10,19,21,23 -25,35,52 From a clinical standpoint, surgeons who perform osteochondral allograft transplants attempt to minimize recipient-graft articular step-off. As our results indicate, we were able to implant grafts within the desired ±1 mm of step-off in 98.6% of the circumferences of the 10 MFC grafts and 94.5% of the LFC grafts. Five of 10 (50%) MFC grafts and 4 of 10 (40%) LFC grafts were 100% within the acceptable range. For the grafts that did not have 100% of the circumference within the acceptable range of step-off, only a small percentage of each graft was greater or less than 1 mm proud or recessed. Shortening the graft height for grafts that were proud or inserting bone graft deep to the graft for those that were recessed might improve the areas of the graft that were not within the acceptable range but would result in undesired changes in the areas of the graft that were acceptable.
In clinical situations, we are of the opinion that an implanted graft that has more than 90% of the circumference within ±1 mm of step-off is very acceptable and a situation that we would not attempt to improve. The surgeon’s ability to achieve 100% acceptable circumferential step-off is dependent of many factors, including the surface topographies of the recipient and donor condyle, the angle of the created recipient socket with respect to the articular surface, and the angle that the osteochondral plug was harvested from the donor condyle. Slight deviations from perpendicular when the recipient socket is created or the allograft plug is harvested can lead to areas of the transplant that can become proud or recessed.
Our study is the first to assess the 3-dimensional surface contour of osteochondral allografts and compare them to the recipient condyle. There are no published data on surface geometry restoration and no way, clinically, for surgeons to ensure adequate restoration of the articular surface contour. As our data show, we were able to match the original MFC articular surface contour within ±1 mm in 87.4% of the MFC grafts and 87.7% of the LFC grafts. The ability to accurately assess the exact match of surface contour with the eye is certainly not as accurate as the assessment done by μCT. As there are no two condyles with the exact surface contour, some variability and tolerance should be expected with osteochondral allograft transplants. Restoring the surface area topography is dependent on the topography of the donor condyle, but as we have shown, acceptable restoration of the surface contour of the MFC can be accomplished with an MFC or LFC allograft for lesions ≤20 mm.
The results of this study have a number of clinical implications. The MFC is the most common location for full-thickness chondral defects in the knee, and most surgeons who perform osteochondral allograft transplantation request an MFC allograft for these defects. Since many factors contribute to differences in condyle geometry, even a size-matched orthotopic allograft does not ensure that the surface contour will be similar to that of the recipient femoral condyle. The Joint Restoration Foundation’s 2012 statistics reveal that nearly 75% of available and suitable allograft condyles are LFCs. The limited availability of MFC grafts can result in prolonged waiting for surgeons and patients, which in some cases can lead to further joint deterioration. The present results suggest that an LFC graft can be used to restore the articular surface of an MFC as well as an MFC graft for moderate-sized contained defects.
There are several limitations to the present study. Only 20-mm defects were assessed. Although this size is not inclusive of all osteochondral allograft transplants, 20 mm represents a common-size allograft transplanted as a single plug in our clinical experience. These results are also relevant to larger lesions treated with osteochondral allografts. Lesions that are larger than 25 mm are usually larger in the anterior-posterior dimension. Given that 75% of the harvested MFCs are less than or equal to 27 mm in the medial-lateral dimension (data on file; Joint Restoration Foundation), our preferred method of transplant in cases of larger lesions is to stack 1 to 3 allograft plugs of less than or equal to 20 mm to better match the native articular surface. The lesions in this study were also created in the weightbearing portion of the MFC and were contained; lesions were not assessed that were uncontained or on the edge of the condyle. The articular surface contour along the lateral-most portion of the MFC, a common location for an osteochondritis dissecans lesion, differs substantially from the medial side of the LFC. Using an LFC allograft in this situation may be more challenging. The study also assessed only the surface contours at time zero and did not address potential graft settling, as the subchondral bone potentially resorbs and revascularizes. Finally, the study did not examine the quality of the articular cartilage or the subchondral bone. Differences in cartilage stiffness between donor and graft may affect load transmission on the recipient condyle. 26 We chose to focus on surface congruity, as it has been identified as an important factor in the success of osteochondral allograft transplantation.
In summary, an LFC allograft fits as well as an MFC allograft for 20-mm defects in the MFC. Clinical studies comparing MFC-to-MFC and LFC-to-MFC grafts would be of interest. If the similar articular surface match of nonorthotopic LFC-to-MFC and orthotopic MFC-to-MFC osteochondral allografts translates into similar surgical efficacies in the long term, there will be increased availability of osteochondral allografts for MFC defects.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: The project was funded by Joint Restoration Foundation and surgical instrumentation was provided by Arthrex. Joint Restoration Foundation reimbursed the surgeons (T.S.M., M.T.P., W.D.B.) for their travel and time to conduct the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.