
Abstract
Background:
Marrow stimulation for the treatment of osteochondral lesions of the talus (OLTs) is controversial in patients with poor prognostic factors of OLTs. Currently, mesenchymal stem cells (MSCs) are expected to biologically augment the treatment of OLTs.
Purpose:
To compare the clinical and magnetic resonance imaging (MRI) outcomes between an injection of MSCs with marrow stimulation and marrow stimulation alone in patients with OLTs.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 49 patients (50 ankles) with OLTs underwent follow-up MRI after arthroscopic treatment. Among these 50 ankles, 26 underwent marrow stimulation alone (conventional group), and 24 underwent marrow stimulation with an injection of a stromal vascular fraction (SVF) containing MSCs (MSC group). Clinical outcomes were evaluated according to the visual analog scale (VAS) for pain, American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale, and Tegner activity scale. The magnetic resonance observation of cartilage repair tissue (MOCART) score was used for the MRI evaluation of repaired lesions.
Results:
The mean VAS score, AOFAS score, and Tegner score improved from 7.1 ± 1.2, 68.5 ± 5.6, and 3.4 ± 0.6 to 3.9 ± 0.8, 78.3 ± 4.9, and 3.5 ± 0.8, respectively, in the conventional group and from 7.1 ± 0.8, 67.7 ± 4.7, and 3.4 ± 0.5 to 3.2 ± 0.8, 83.3 ± 7.0, and 3.9 ± 0.7, respectively, in the MSC group. All clinical outcomes, including the VAS, AOFAS, and Tegner scores, improved significantly in the MSC group compared with the conventional group (P = .003, .009, and .041, respectively). There was a significant difference (P = .037) in the mean MOCART score between the conventional and MSC groups (49.4 ± 16.6 vs 62.1 ± 21.8, respectively), and significant correlations of the MOCART score with clinical outcomes were found in both groups (P < .05). Patient age (≥46.1 years), large lesion size (≥151.2 mm2), and the presence of subchondral cysts were associated with a worse MOCART score in the conventional group (P = .015, .004, and .013, respectively) but not in the MSC group.
Conclusion:
Clinical and MRI outcomes of an injection of an SVF containing MSCs with marrow stimulation were encouraging, compared with marrow stimulation alone, for the treatment of OLTs. Therefore, an injection of an SVF containing MSCs with marrow stimulation should be considered as a treatment for OLTs, even when poor prognostic factors, including older age, large-sized lesion, or the presence of subchondral cysts, exist.
The surgical treatment options for osteochondral lesions of the talus (OLTs) are controversial and a subject of frequent debate. Loveday et al 38 concluded that there is insufficient evidence from randomized trials to determine the most beneficial surgical procedure for treating OLTs in adults. Various surgical treatments, varying in complexity from simple debridement to osteochondral allograft transplantation, have been described. 11 Among these, arthroscopic marrow stimulation, involving subchondral drilling, curettage, microabrasion, and microfracture, is the most commonly utilized primary treatment strategy for symptomatic OLTs.7,8,18,34,58 This strategy provides acceptable clinical results over midterm follow-up periods but often fails in the long term because of biomechanical insufficiency of the regenerative fibrocartilage and scar tissue that results from this method.3,26 According to the literature, the results of marrow stimulation in the treatment of OLTs are controversial in cases that have poor prognostic factors, such as older patient age,8,18,33 large lesion size,7,8,18,19 or the presence of subchondral cysts.20,37,43 Therefore, we considered, in patients with these poor prognostic factors, that mesenchymal stem cells (MSCs) could be applied as a supplemental augmentation strategy in addition to marrow stimulation to obtain improved outcomes because of their capability to differentiate into articular cartilage and induce the formation of subchondral bone by their injection into the OLT.
Recently, MSCs were proposed as a new option for the treatment of articular cartilage defects because of their ability to differentiate into various lineages, including osteoblasts and chondrocytes.4,14,44 In the literature, several studies have reported on the application of MSCs in the treatment of OLTs.15,17,29 In our previous study, 29 we found that an injection of a stromal vascular fraction (SVF) containing MSCs with marrow stimulation was encouraging compared with marrow stimulation alone in patients with OLTs. However, significant weaknesses of our prior research were that only patients aged older than 50 years were enrolled, and the outcomes of OLT treatment were investigated only using clinical scores. Therefore, in the present study, we aimed to (1) assess the clinical and magnetic resonance imaging (MRI) outcomes of an injection of an SVF containing MSCs with marrow stimulation in patients with OLTs, (2) compare the outcomes thereof with those of marrow stimulation alone, (3) investigate the associations between clinical and MRI outcomes, and (4) identify the prognostic factors associated with MRI outcomes.
Materials and Methods
Patient Enrollment
In this retrospective cohort study, the inclusion criteria were a full-thickness chondral defect of the talar dome with symptoms of ankle joint pain or functional limitations despite a minimum of 3 months of nonsurgical management, including ankle bracing, physical therapy, and nonsteroidal anti-inflammatory drugs. Patients with previous surgical treatments and patients with arthritic changes in their ankle joint or deformity of the axis of the ankle on plain radiographs were excluded.
From August 2008 to July 2012, 143 patients (152 ankles) with OLTs were treated with arthroscopic marrow stimulation. Patients were informed about MSCs before surgery and decided whether to use them at the time of surgery. Decisions were solely up to the patients. Moreover, we suggested to all patients that they undergo follow-up MRI for evaluation of the OLT. Of the 143 patients (152 ankles), 94 patients (102 ankles) were excluded; 15 patients did not meet the inclusion criteria, and 79 patients refused to undergo follow-up MRI. Accordingly, 49 patients (50 ankles) underwent follow-up MRI at a mean of 21.9 months postoperatively (range, 16-25 months); these patients were finally included in this study. Twenty-six of these patients were included in our prior study of patients older than 50 years. 29 Among these 50 ankles, 26 underwent arthroscopic marrow stimulation alone (conventional group), and 24 underwent arthroscopic marrow stimulation with an injection of an SVF containing MSCs (MSC group). In patients who had a history of recurrent sprains or chronic ankle instability, ankle bracing and taping were recommended to decrease the occurrence of ankle sprains, and a structured physical therapy program focused on peroneus strengthening exercises and proprioceptive-based rehabilitation of the ankle also was conducted. If instability was not improved after these treatments and the ruptured anterior talofibular or calcaneofibular ligament was identified on MRI, lateral ligament reconstruction was performed, as described by Kim et al. 27 This study was approved by the institutional review board of our hospital.
Sample Collection and Isolation of an SVF Containing MSCs
Sample collection and isolation of an SVF containing MSCs were performed as described previously.28,29 In brief, 1 day before arthroscopic surgery, adipose tissue was harvested from the patient’s buttock through tumescent liposuction. The liposuction material was aspirated by gentle suction, and a mean of 28.6 g (range, 22.3-34.2 g) of buttock fat pad was collected. We aimed to routinely collect 140 mL of liposuctioned adipose tissue, of which 120 mL was used for the injection, and 20 mL was subjected to laboratory analysis to examine the plastic-adherent cells that form colony forming units–fibroblast (CFU-F) and to confirm the multilineage differentiation of adipose-derived stem cells. In the operating room, 120 mL of adipose tissue was suspended in phosphate-buffered saline (PBS), placed in a sterile box, and transported to a laboratory. Mature adipocytes and connective tissue were separated from the SVF by centrifugation, as reported by Zuk et al. 59 The remaining 20 mL of adipose tissue was processed by the same method and used for cell analysis. To evaluate the frequency of mesenchymal-like progenitors in the SVF, cells were cultured in T-25 flasks at a final concentration of 16 cells/cm2. Colonies consisting of ≥50-cell aggregates were scored under an optical microscope, and the immunophenotype of adipose-derived stem cells was analyzed. Phenotyping of MSC markers using the following antibodies was performed: PerCP-conjugated anti-human CD14 (BD Biosciences), allophycocyanin (APC)–conjugated anti-human CD34 (BD Biosciences), fluorescein isothiocyanate (FITC)–conjugated anti-human CD90 (BD Biosciences), PerCP-conjugated anti-human CD105 (BD Biosciences), and mouse control IgM (Southern Biotech). For the isotype control, FITC-, PerCP-, or APC-coupled nonspecific mouse IgG (BD Biosciences) was substituted for the primary antibody. The cells were collected from culture and incubated with CD14, CD34, CD90, and CD105 antibodies or negative control antibodies for 30 minutes at 4°C. The data were acquired using a FACSCalibur instrument (BD Biosciences) and analyzed with CellQuest software (BD Biosciences). Adipose-derived stem cells were plated (at cells/cm2) in Dulbecco’s modified Eagle medium (Sigma) containing 10% fetal bovine serum (Lonza) and allowed to adhere for 24 hours. The culture medium was then replaced with specific inductive media to determine the adipogenic, osteogenic, and chondrogenic differentiation potential. For adipogenic differentiation, the cells were cultured in an adipogenic induction medium containing 100 nM dexamethasone (Sigma-Aldrich), 0.5 mM isobutyl-methylxanthine (Sigma-Aldrich), and 50 mM indomethacin (Sigma-Aldrich) for 14 days. The adipogenic cultures were fixed in 4% paraformaldehyde for 10 minutes, rinsed twice with PBS, stained with fresh 0.3% Oil Red O solution for 10 minutes, and washed with distilled water. To determine the specificity of the responding cells for adipogenesis, we examined Oil Red O staining of lipid droplets. For osteogenic differentiation, the cells were cultured in an osteogenic induction medium containing 1 nM dexamethasone, 10 mM β-glycerol phosphate (Sigma-Aldrich), and 50 mg/mL ascorbate-2-phosphate (Sigma-Aldrich) for 14 days. The osteogenic cultures were stained using the Von Kossa method as follows. The culture plates were rinsed with PBS, fixed in 4% paraformaldehyde for 10 minutes, and then rinsed with distilled water. Silver nitrate solution (5%) was added, and the plate was exposed to ultraviolet light for 3 minutes, after which it was washed well with distilled water. For chondrogenic differentiation, the cells were cultured at 37°C with 5% CO2 in a chondrogenesis medium containing 10 ng/mL transforming growth factor–β3 (Sigma-Aldrich), 1× insulin-transferrin-selenium + premix (Gibco BRL), and 100 nM dexamethasone (Sigma-Aldrich). The medium was replaced every 3 or 4 days for 21 days. For histological and immunohistochemical analyses, samples were collected at the indicated time points, fixed with 10% paraformaldehyde, and embedded in paraffin. The sample paraffin blocks were then sectioned using a 5-μm microtome. The samples were deparaffinized and stained with hematoxylin and eosin, toluidine blue O, and Masson trichrome. We evaluated the capacity of human subcutaneous adipose tissue to generate mesenchymal progenitors using CFU-F. Thus, after isolation, adipose-derived stem cells represented a mean of 9.1% of SVF cells (range, 7.4%-11.2% of SVF cells). After the SVF was isolated, a mean of 3.94 × 106 stem cells (9.1% of 4.34 × 107 SVF cells; range, 2.83-4.76 × 106) were prepared. Characterization of fluorescence-activated cell sorting indicated the positive expression of surface markers CD90 and CD105 and the negative expression of CD34 and CD14. Adipose-derived stem cells treated with conditioned media demonstrated characteristics of adipogenic, osteogenic, and chondrogenic differentiation after staining. Stepwise multivariate linear regression was used to assess the association between the number of MSCs and the weight of the collected buttock fat pad. For the number of MSCs, the weight of the collected buttock fat pad accounted for 85.7% of the variability (P < .001).
Surgical Procedure and an Injection of an SVF Containing MSCs
The arthroscopic marrow stimulation procedure was performed in a standardized manner in all cases. After accurate debridement of all unstable and damaged cartilage in the lesion, microfracture was performed 3 to 4 mm apart in areas where the subchondral bone was intact (Figure 1C). Multiple perforations perpendicular to the joint surface were made by using a 2.5-mm, 90° microfracture awl (Linvatec) as described by Steadman et al. 54 For areas with subchondral bone loss, abrasion arthroplasty was performed by removing loose chondral or osteochondral fragments with a ring-shaped or curved curette and by trimming damaged cartilage with a power shaver until a stable, smooth articular surface was created. When there were subchondral cysts, the cysts were decompressed by the removal of cystic material (Figure 2C). The tourniquet was released after the procedure, and adequate bone bleeding at microfracture holes was confirmed (Figure 1D). For the MSC group, an injection of an SVF containing MSCs isolated 1 day before surgery was performed after the arthroscopic procedure (see the online Video Supplement); an injection of an SVF containing MSCs (mean, 3.94 × 106 stem cells) was performed after the extraction of arthroscopic fluid within the joint (Figure 2D). After the operation, a short leg splint was applied for 2 weeks, and after sutures were removed, tolerable weightbearing activities were recommended for patients without associated lesions. Fifteen patients (8 in the conventional group, 7 in the MSC group) underwent lateral ligament reconstruction along with the arthroscopic treatment. For those patients, we recommended postoperative immobilization with a short leg walking cast with partial weightbearing for 4 weeks. Patients began active and passive ankle range of motion exercises at 4 weeks after surgery. Sports or high-impact activities were limited for at least 3 months.
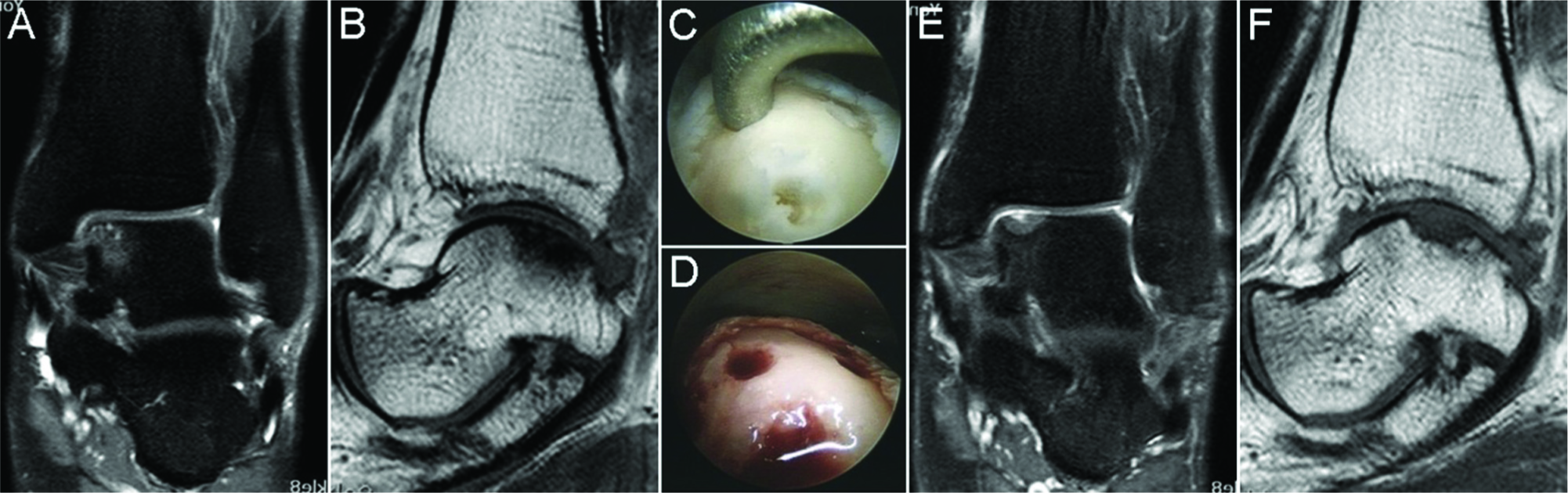
(A) Preoperative fat-saturated proton density coronal image and (B) T1-weighted sagittal image of the right ankle in a 42-year-old female patient. An osteochondral lesion of the talus with subchondral bone marrow edema was observed in the medial talar dome. (C) Arthroscopic microfracture without an injection of mesenchymal stem cells was performed. (D) Adequate bone bleeding at microfracture sites was confirmed. (E) Follow-up fat-saturated proton density coronal image and (F) T1-weighted sagittal image at 24 months after surgery. A chondral defect and broken subchondral lamina with adjacent bone marrow edema were observed.
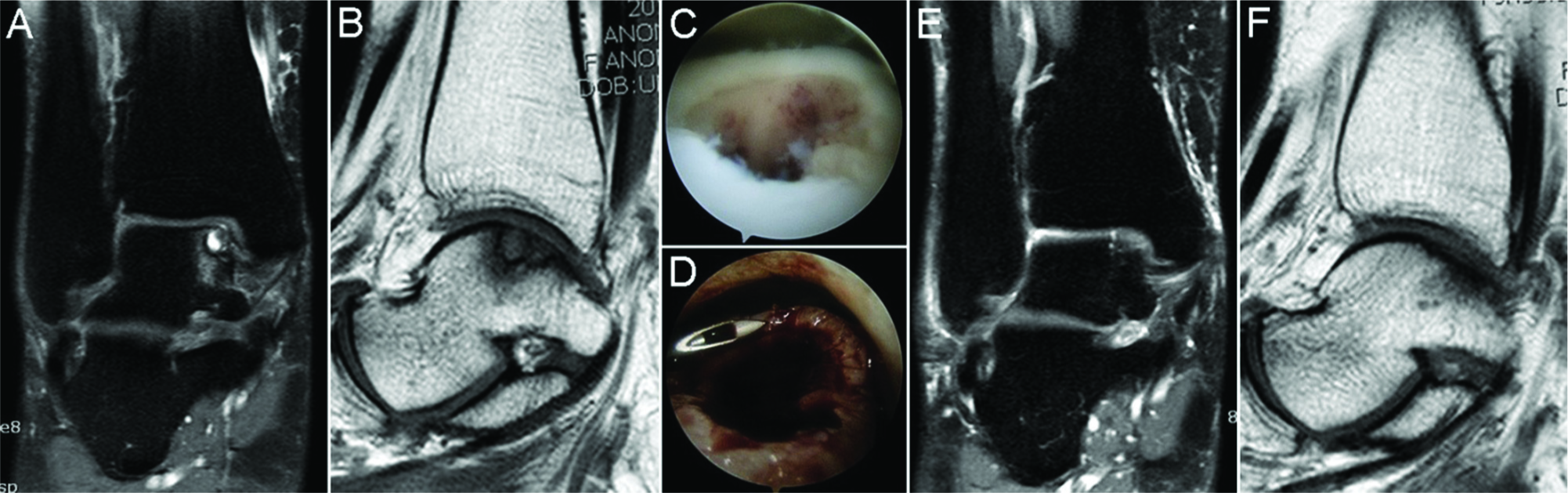
(A) Preoperative fat-saturated proton density coronal image and (B) T1-weighted sagittal image of the left ankle in a 49-year-old female patient. An osteochondral lesion of the talus with subchondral cyst and adjacent bone marrow edema was observed in the medial talar dome. (C) Arthroscopic view after microfracture with decompression of the subchondral cyst. (D) Arthroscopic view after an injection of a stromal vascular fraction containing mesenchymal stem cells. (E) Follow-up fat-saturated proton density coronal image and (F) T1-weighted sagittal image at 28 months after surgery. The subchondral cyst and adjacent bone marrow edema disappeared.
Outcome Assessment
For the clinical evaluation, the visual analog scale (VAS) for pain and American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale were utilized. The Tegner activity scale 56 was used to determine sporting and activity levels. Although the Tegner activity scale was originally utilized for the knee, it was intended for facilitating outcomes research in sports medicine.
For the evaluation of OLT variables, including the size and location of lesions and any associated lesions (eg, subchondral cyst), before surgery and for structural evaluation of repair tissue after surgery, a 1.5-T MRI scanner (Achieva 1.5T, Philips Healthcare) with a dedicated 8-element SENSE foot/ankle coil was used with the following sequences: (1) proton density (PD) spectral presaturation with inversion recovery (SPIR) coronal image (repetition time [TR]/echo time [TE], 4000/15 milliseconds): field of view (FOV), 150 × 150 mm; matrix, 308 × 249; slice thickness (SL), 3.5 mm with 0.35-mm gap; (2) PD SPIR axial image (TR/TE, 3500/15 milliseconds): FOV, 150 × 150 mm; matrix, 260 × 240; SL, 3.0 mm with 0.5-mm gap; (3) T2 SPIR sagittal image (TR/TE, 3200/70 milliseconds): FOV, 150 × 150 mm; matrix, 240 × 192; SL, 3.0 mm with 0.3-mm gap; (4) turbo spin echo T1-weighted sagittal image (TR/TE, 600/20 milliseconds): FOV, 140 × 140 mm; matrix, 240 × 240; SL, 3.0 mm with 0.3-mm gap; and (5) turbo spin echo T2-weighted axial image (TR/TE, 4700/90 milliseconds): FOV, 150 × 150 mm; matrix, 328 × 261; SL, 3.0 mm with 0.5-mm gap. To avoid potential bias, an independent observer, who was a musculoskeletal-trained radiologist not involved in the care of the patients and blinded to the intention of this study, evaluated the MRI scans retrospectively as part of this study. On preoperative MRI, the width and length of the OLT were measured on coronal, sagittal, and axial MRI scans; the largest dimension was selected. We reconfirmed the lesion size through an arthroscopic examination, and the defect size was calculated by using the ellipse formula, as described previously. 29 We compared size measurements (width, length, and size) based on MRI with those determined by arthroscopic examination, and a good correlation was found by linear regression analysis (r = 0.79, P < .001). On follow-up MRI, evaluation of repair tissue was performed using the magnetic resonance observation of cartilage repair tissue (MOCART) score, according to Marlovits et al. 39 We also investigated the presence of bone marrow edema in preoperative and follow-up MRI evaluations.
Statistical Analysis
The principal dependent variables of clinical outcomes were VAS, AOFAS, and Tegner scores at final follow-up. The Wilcoxon signed-rank test was conducted to evaluate differences between preoperative and final follow-up values, while the Mann-Whitney U test was performed to compare results between groups. Either the χ2 test or Fisher exact test was used to compare categorical data. The Spearman rank-order correlation test was used to analyze correlations between the MOCART score and clinical outcomes (VAS, AOFAS, and Tegner scores) as well as between the presence of bone marrow edema and clinical outcomes at final follow-up. Associations among various factors—patient characteristics (age, sex, body mass index [BMI], duration of symptoms) and OLT variables (size and location of lesion, presence of subchondral cysts, additional lateral ligament reconstruction)—were examined independently based on the MOCART score in both groups. Median values were used as standard values for dividing patients according to age, BMI, duration of symptoms, and lesion size. Differences between individual groups were analyzed using the Mann-Whitney U test. Statistical analysis was performed using SPSS version 13.0 software (IBM Corp), with significance defined as P < .05.
Results
General Characteristics
The study population included 28 men and 21 women, with a mean age of 46.1 years (range, 21-62 years) and a mean follow-up period of 27.1 months (range, 22-41 months). The mean preoperative BMI was 27.4 kg/m2 (range, 19.6-37.3 kg/m2), and the mean duration of symptoms was 22.2 weeks (range, 16-33 weeks). There were no significant differences between groups regarding patient age, sex, BMI, duration of symptoms before surgery, follow-up period, or MRI follow-up period (Table 1).
Comparison of Baseline Demographics in Both Groups a
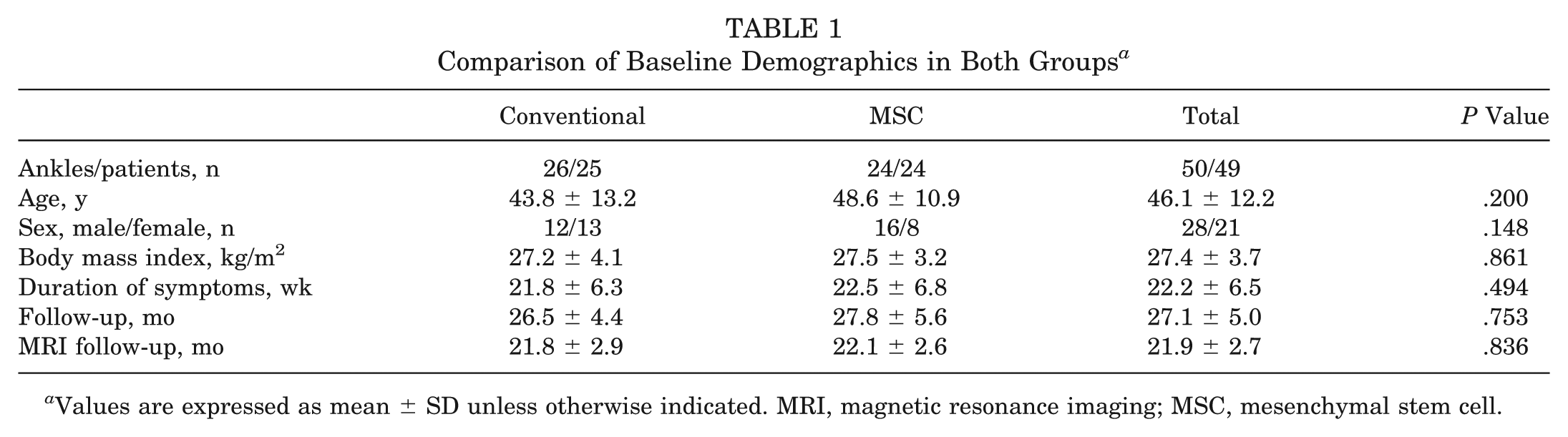
Values are expressed as mean ± SD unless otherwise indicated. MRI, magnetic resonance imaging; MSC, mesenchymal stem cell.
Clinical Outcomes
Clinical outcomes and activity levels from preoperatively to final follow-up in each group are summarized in Table 2. The mean VAS score improved significantly from 7.1 ± 1.2 to 3.9 ± 0.8 in the conventional group and from 7.1 ± 0.8 to 3.2 ± 0.8 in the MSC group (P < .05 for both). There was a significant difference in the mean VAS score between groups at final follow-up (P = .003). The mean AOFAS score improved significantly from 68.5 ± 5.6 to 78.3 ± 4.9 in the conventional group and from 67.7 ± 4.7 to 83.3 ± 7.0 in the MSC group (P < .05 for both). There was a significant difference in the mean AOFAS score between groups at final follow-up (P = .009). The mean activity level according to the Tegner activity scale improved significantly from 3.4 ± 0.5 to 3.9 ± 0.7 in the MSC group (P = .005). However, in the conventional group, the mean Tegner score did not improve significantly from 3.4 ± 0.6 to 3.5 ± 0.8 (P = .564). There was a significant difference in the Tegner score between groups at final follow-up (P = .041).
Clinical Outcomes and MOCART Scores in Both Groups a
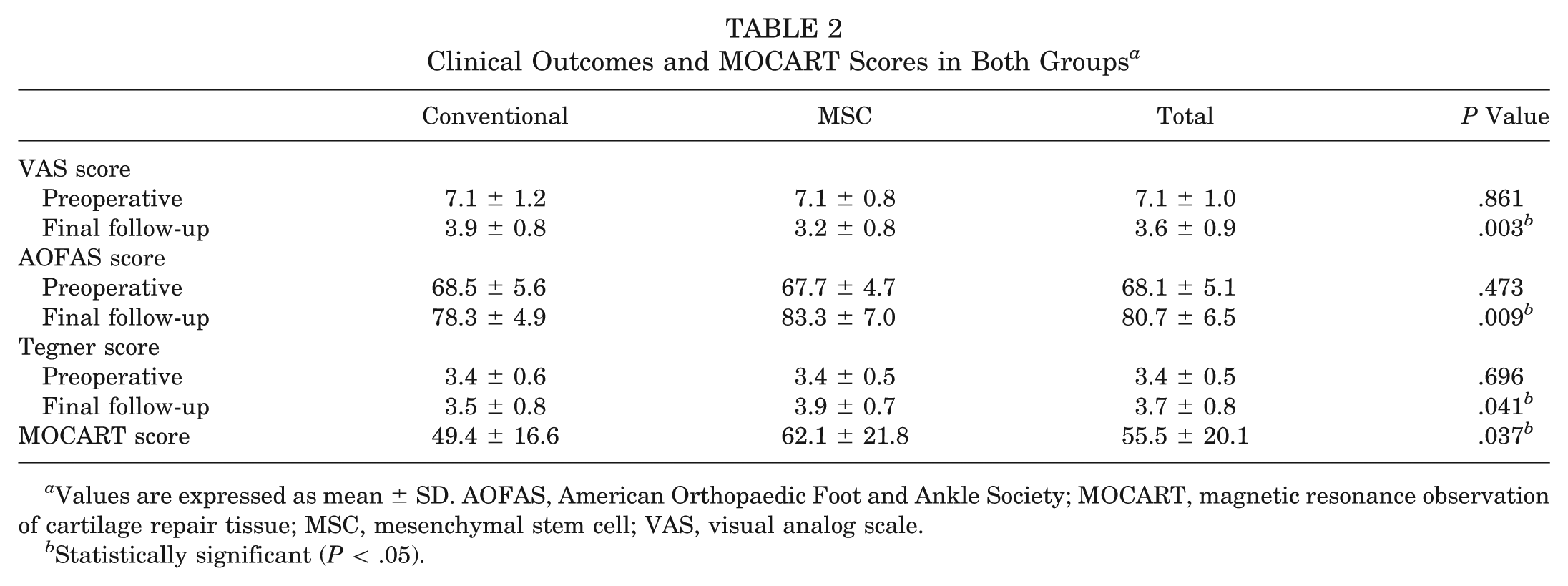
Values are expressed as mean ± SD. AOFAS, American Orthopaedic Foot and Ankle Society; MOCART, magnetic resonance observation of cartilage repair tissue; MSC, mesenchymal stem cell; VAS, visual analog scale.
Statistically significant (P < .05).
MRI Evaluation
The MRI scans were evaluated by means of the MOCART score (see Appendix 1, available in the online version of this article at http://ajsm.sagepub.com/supplemental). The maximum score achievable in the evaluation of 9 variables is 100; individual values in both groups are shown in Appendix 1. Among the 9 variables of the MOCART scoring system, there were significant differences between groups in 2 variables (degree of defect repair and filling of the defect and subchondral bone; P = .041 and .038, respectively). At follow-up, the mean MOCART score was 49.4 ± 16.6 in the conventional group and 62.1 ± 21.8 in the MSC group. There was a significant difference in the mean MOCART score between groups (P = .037) (Table 2). Significant correlations of the MOCART score with clinical outcomes were found in both groups (Table 3). On preoperative MRI, signal intensities of bone marrow edema were observed in 13 ankles in the conventional group and 14 ankles in the MSC group. On follow-up MRI, this bone marrow edema disappeared in 4 ankles in the conventional group and 10 ankles in the MSC group (Figure 2E). In the conventional group, bone marrow edema was still observed in 9 ankles (69%) on follow-up MRI (Figure 1E). Moreover, bone marrow edema that was not present on preoperative MRI was newly observed in 4 ankles on follow-up MRI in the conventional group. There were positive correlations of clinical outcomes with the presence of bone marrow edema on follow-up MRI in both groups. However, no correlations were found between clinical outcomes and the presence of bone marrow edema on preoperative MRI in either group (Table 4).
Correlations Between MOCART Scores and Clinical Outcomes at Final Follow-up in Both Groups a
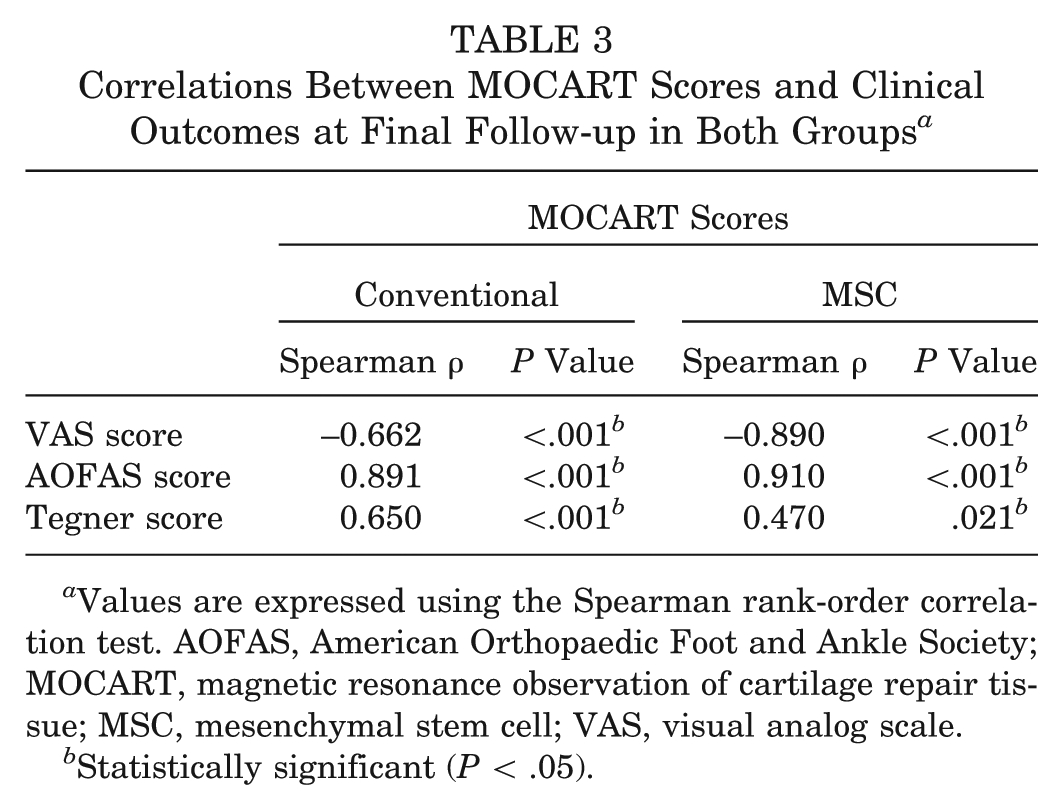
Values are expressed using the Spearman rank-order correlation test. AOFAS, American Orthopaedic Foot and Ankle Society; MOCART, magnetic resonance observation of cartilage repair tissue; MSC, mesenchymal stem cell; VAS, visual analog scale.
Statistically significant (P < .05).
Correlations Between the Presence of Bone Marrow Edema and Clinical Outcomes at Final Follow-up in Both Groups a
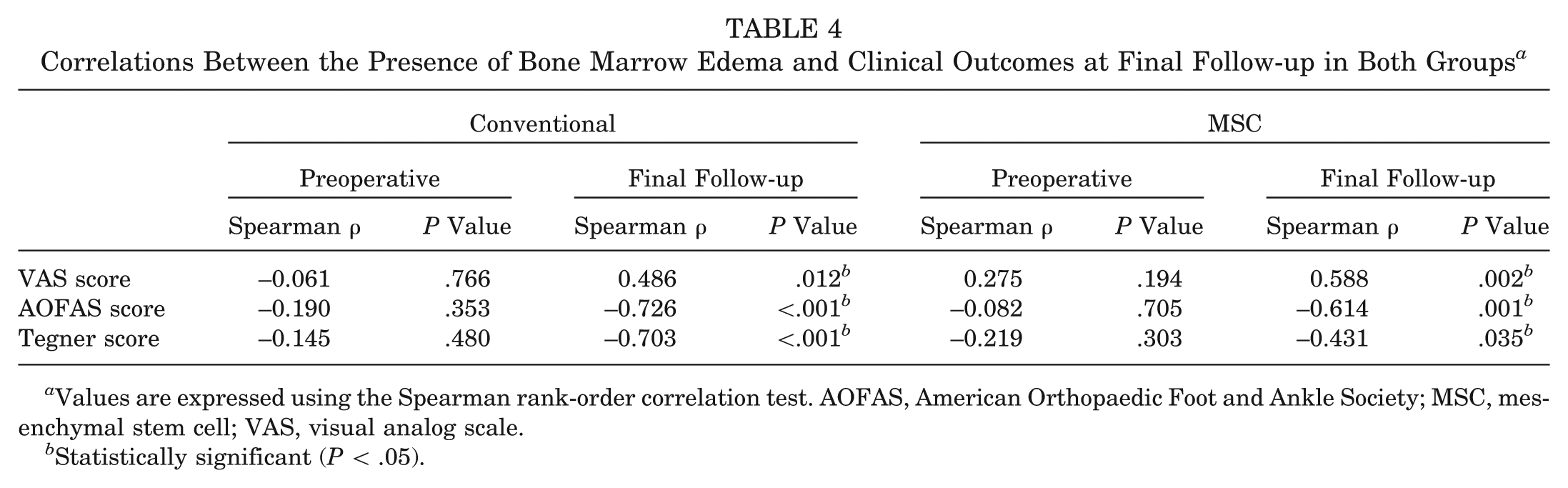
Values are expressed using the Spearman rank-order correlation test. AOFAS, American Orthopaedic Foot and Ankle Society; MSC, mesenchymal stem cell; VAS, visual analog scale.
Statistically significant (P < .05).
Associations of MOCART Score With Patient Characteristics and OLT Variables
The Mann-Whitney U test was used to assess the independent effects of patient characteristics and OLT variables in both groups (Appendix 2, available online). Median values were used to divide patients according to age (<46.1 or ≥46.1 years), BMI (<27.4 or ≥27.4 kg/m2), duration of symptoms (<22.2 or ≥22.2 weeks), and lesion size (<151.2 or ≥151.2 mm2). Statistically significant associations were found between the MOCART score and patient age, lesion size, and the presence of subchondral cysts in the conventional group. At the time of the follow-up MRI evaluation, older age (≥46.1 years), large lesion size (≥151.2 mm2), and the presence of subchondral cysts had significantly worse outcomes according to the MOCART score in the conventional group (P = .015, .004, and .013, respectively) (Appendix 2). However, these associations were not observed in the MSC group. Other prognostic factors, including sex, BMI, duration of symptoms, and additional lateral ligament reconstruction, did not seem to have a significant influence on the MOCART score in either group (P > .05).
Discussion
An OLT is a broad term defined as a lesion of any origin that involves the articular surface and/or subchondral region of the talus, thus affecting cartilage, bone, or both. Articular cartilage is avascular and has poor regenerative capabilities, and injuries that do not penetrate the subchondral plate have no stimulus for an inflammatory reaction and healing.16,32 Marrow stimulation for OLTs has been performed to stimulate fibrocartilage development by breaching the subchondral plate with the subsequent introduction of serum factors and development of scar tissue at the defect site. Among these marrow stimulation treatments, microfracture is known to induce perpendicularly oriented holes produced arthroscopically and a peripheral rim that potentially helps the integration of repair tissue with subchondral bone. 53 Recently, MSCs have been applied as a valuable adjunct to marrow stimulation for improved outcomes of OLT treatment. McIlwraith et al 40 reported, in their study of an MSC injection into microfractured chondral defects in equine models, that MSCs enhanced cartilage repair quality with increased aggrecan content and tissue firmness. Fortier et al 13 compared the results of cartilage repair in equine models treated with MSCs and microfracture and with microfracture alone. They also found that MSCs could result in healing of acute full-thickness cartilage defects, which is superior to that after microfracture alone. Giannini et al 17 reported that OLT treatment using MSCs in humans represents an advance in osteochondral regeneration, achieving satisfactory clinical outcomes with the formation of repair tissue and overcoming the drawbacks of previous marrow stimulation treatments. Thus, we hypothesized that an injection of MSCs might be able to contribute to the regeneration of damaged tissue in OLTs by filling the whole thickness of a defect and secreting some trophic molecules 5 ; the final result would be cartilage on the top and bone on the bottom. In our previous study, 29 we showed that the application of an SVF containing MSCs with marrow stimulation was effective, compared with marrow stimulation alone, in patients with OLTs. In the current study, we assessed the clinical outcomes of an injection of an SVF containing MSCs with marrow stimulation for OLTs and evaluated the degree of cartilage repair using MRI. To our knowledge, this is the first study to present MRI findings after an injection of an SVF containing MSCs with marrow stimulation for OLTs.
In this study, we assessed the clinical and MRI outcomes in both groups and found that all outcomes, including VAS, AOFAS, Tegner, and MOCART scores, improved significantly in the MSC group compared with the conventional group (P = .003, .009, .041, and 0.37, respectively) (Table 2). For the evaluation of the magnitudes of the differences in the outcome scores and whether these were likely to be clinically significant, we used a distribution-based method to calculate the minimal clinically importance difference (MCID). We estimated the standard error of measurement (SEM), which represents the amount of error associated with an individual patient assessment by the formula SEM = SD [(1 – R)1/2], where SD is the baseline standard deviation and R is the Cronbach α reliability coefficient in our samples. According to the distribution-based method measuring the variability of the SEM, we compared the change in clinical outcomes (VAS, AOFAS, and Tegner scores) and the MOCART score. The SEM is the variation in scores that is caused by the unreliability of the scale or measure used. Therefore, the change in score that is smaller than the SEM is likely to be the result of a measurement error rather than a true observed change. Patients achieving a difference in an outcome score of at least 1 SEM would have an MCID. 9 In this study, the SEM in differences between the groups was larger than the SEM of each group. Therefore, we considered that the differences in clinical outcomes at final follow-up and the MOCART score between the groups, although they were small differences, were truly significant differences.
In the literature, MRI has been used as an effective and objective tool to evaluate the healing of osteochondral lesions after surgical treatment because of its advantages of noninvasiveness, reproducibility, and accuracy.2,24,47 In these studies, the MOCART score, 39 which was originally developed for chondral lesions of the knee joint, was used to assess osteochondral lesions of the ankle joint. Hu et al 24 reported, in their study of 17 patients with medial OLTs treated with transplantation of an autologous osteoperiosteal cylinder graft, that the mean MOCART score was 60 ± 9.4 after surgery. Aurich et al 2 reported a mean MOCART score of 62.4 ± 15.8 after matrix-associated chondrocyte implantation in OLTs and found no relationships between the MOCART score and clinical outcomes. Although the studies mentioned above were not about marrow stimulation, a similar postoperative MOCART score was found in the MSC group in the present study. The mean MOCART score was 49.4 ± 16.6 in the conventional group and 62.1 ± 21.8 in the MSC group, which was significantly different between groups (P = .037). However, in contrast to the results of the study by Aurich et al, 2 significant correlations of the MOCART score with clinical outcomes were found in both groups (Table 3). Although the exact reason for these results cannot be explained, we consider that the MOCART scoring system is more useful for predicting clinical outcomes after marrow stimulation than those of other treatments, such as autologous chondrocyte implantation or osteochondral grafts, for OLTs. We anticipate that certain biomechanical or biochemical properties of repaired cartilage might affect the clinical outcomes after these different treatment methods for OLTs. Further studies are required to investigate the associations between the MOCART score and clinical outcomes.
In this study, we investigated individual variables of the MOCART scoring system in the conventional and MSC groups and found significant differences between groups in 2 variables (degree of defect repair and filling of the defect and subchondral bone) (Appendix 1). We consider that the injected MSCs contained in an SVF might play a role in filling the defect by repaired cartilage and the formation of subchondral bone, resulting in these significant differences between groups. In the MSC group, 10 (41.7%) of 24 ankles showed complete filling of the defect, presenting a considerably high percentage compared with 6 (23.1%) of 26 ankles in the conventional group. Marrow stimulation induces the recruitment of MSCs from bone marrow, which leads to fibrocartilage covering the lesion.21,32 Therefore, the additional application of MSCs contained in an SVF, which have chondrogenic ability, would be helpful for filling the defect with regenerated fibrocartilage. In our previous study, 29 we found that an additional injection of an SVF containing MSCs with marrow stimulation was helpful for achieving more favorable outcomes, compared with marrow stimulation alone, in older patients with OLTs. Moreover, adipose-derived MSCs have been shown to maintain their differentiation potential even in the later stages of life and may have better chondrogenic potential than bone marrow–derived MSCs. 49 In this study, adipose-derived MSCs contained in an SVF harvested from the buttock fat pad of patients were injected into the lesion. We anticipate that these characteristics of adipose-derived MSCs contained in an SVF contributed to better coverage of the defect by the regeneration of cartilage in the MSC group compared with the conventional group.
The restoration of subchondral bone in the treatment of OLTs has been emphasized for its role in the etiopathogenic processes of articular surface damage.6,41,45,46,57 Although articular cartilage and subchondral bone are different composite materials, they act together as a functional unit 46 ; thus, an injury of either type adversely affects the entire joint mechanical environment. Shirazi and Shirazi-Adl 52 reported that biomechanical perturbations caused by osteochondral alterations substantially alter the pattern and magnitude of contact pressure and cartilage strain in the joint. Moreover, inadequate subsurface support from abnormal subchondral bone might be one of the main reasons for unsuccessful cartilage repair.46,57 When subchondral bone becomes damaged because of damaged overlying cartilage, the cartilage is further injured because the underlying bone is unable to provide support. 57 In this manner, a vicious circle is started. Therefore, the restoration of subchondral bone is very important in the treatment of OLTs. Several studies have reported the effects of MSCs in the restoration of subchondral bone in articular cartilage defects.36,42,51 O’Driscoll 42 reported that when the depth of the OLT extends to subchondral bone, marrow cells are stimulated to produce new tissue in an attempt to fill the defect through marrow stimulation. Shapiro et al 51 showed that new marrow-derived cartilage undergoes endochondral ossification, forming bone on the surface of calcified cartilage cores, and in the depths of the defect, new bone forms directly from osteoblasts derived from marrow MSCs. Lin et al 36 reported, in their study using a rabbit model, that both hyaline cartilage and subchondral bone regenerated successfully after the implantation of expanded MSCs on a collagen membrane into osteochondral defects. In this study, there was a significant difference in the subchondral bone variable of the MOCART score between groups. In the MSC group, subchondral bone was intact in 21 ankles (87.5%) compared with 16 ankles (61.5%) in the conventional group. We believe that injected MSCs contained in an SVF contributed to better restoration of subchondral bone in the MSC group. Concerning these points of view, the restoration of articular cartilage and subchondral bone is important in the treatment of OLTs. Moreover, the integration between articular cartilage and subchondral bone as an osteochondral unit is also important for better outcomes of OLT treatment. Recently, tissue-engineering approaches have been addressed as potential strategies to restore the osteochondral unit using a construct of MSCs combined with a scaffold.23,55 However, clinical efficacy has yet to be established, and future studies are needed to validate the integration between osteochondral constructs. Nonetheless, we anticipate that MSCs might contribute to the restoration of both cartilage and subchondral bone by controlling the spatial distribution of the chondrogenic and osteogenic induction agents that facilitate the integration of these 2 structures. If integration is insufficient, pressure loading could not be distributed evenly on the articular surface and subsequently focused on the repaired lesion, resulting in bone marrow edema of the talus. Although there is controversy as to whether persistent bone marrow edema is a normal postoperative finding after marrow stimulation, several authors have reported that persistent edema present longer than 1 or 2 years postoperatively is pathological and may be related to poor outcomes.1,10,22 Cuttica et al 10 reported, in their study of an MRI evaluation after microfracture in OLTs, that postoperative bone marrow edema was correlated with clinical outcomes. Similar results were found in the present study. There were positive correlations of clinical outcomes with the presence of bone marrow edema on follow-up MRI in both groups. However, no correlations were found between clinical outcomes and the presence of bone marrow edema on preoperative MRI in either group (Table 4).
There has been debate as to whether arthroscopic marrow stimulation is effective in older patients with OLTs. Several authors have indicated that older patients seem to do well with arthroscopic treatment of OLTs,7,12,25 while others have reported less favorable outcomes of marrow stimulation in older patients.8,18,33 In our previous study, 29 we compared the outcomes of an injection of an SVF containing MSCs with marrow stimulation with those of marrow stimulation alone for the treatment of OLTs to investigate the effects of MSCs on the outcomes of patients aged older than 50 years. In that study, significant differences were found in the clinical outcomes between groups at final follow-up. In the present study, the mean patient age was 46.1 years, and we divided the patients according to age (<46.1 or ≥46.1 years) to assess the independent effects of age on the MOCART score in both groups. When patients were aged older than 46.1 years, the MOCART score was significantly worse in the conventional group (P = .015) but not in the MSC group (P = .726) (Appendix 2). Concerning the results of a previous study 29 and the present study, we discern that an injection of an SVF containing MSCs with marrow stimulation could potentially be useful for better clinical results in older patients.
A review of the literature revealed significant correlations between defect size and clinical outcomes of arthroscopic treatment of OLTs.7,18,35 These studies have indicated less favorable outcomes of marrow stimulation for lesions larger than 150 mm2. A similar result was found in the conventional group in this study. At the time of the follow-up MRI evaluation, large-sized lesions (≥151.2 mm2) had significantly worse outcomes according to the MOCART score in the conventional group (P = .004); however, this association was not observed in the MSC group (Appendix 2). In this regard, we believe that an MSC injection with marrow stimulation also could be attempted in lesions larger than 150 mm2.
Although the definite pathogenesis of subchondral cysts is not completely understood, various treatment modalities for subchondral cysts in OLTs have been recommended. However, although noncystic OLTs can be treated effectively with marrow stimulation, the results of marrow stimulation for OLTs with subchondral cysts are controversial.20,37,43 The healing response after marrow stimulation could be poor when a subchondral cyst is present because of the nonviability of subchondral bone and paucity of stem cells. 24 Therefore, several authors have recommended osteochondral autograft transplantation in OLTs with subchondral cysts.30,31,50 In our previous study, 29 we found that the presence of subchondral cysts was a significant predictor of unsatisfactory clinical outcomes in patients treated with marrow stimulation alone, while no association was found between subchondral cysts and clinical outcomes in patients who received an injection of an SVF containing MSCs with marrow stimulation. In the current study, the presence of subchondral cysts had significantly worse outcomes according to the MOCART score in the conventional group (P = .013); this correlation was not seen in the MSC group (P = .653) (Appendix 2), however, and subchondral cysts healed completely after an injection of an SVF containing MSCs with marrow stimulation in 7 (87.5%) of 8 cases (Figure 2). Therefore, concerning the outcomes of these 2 studies, we believe that an injection of an SVF containing MSCs with marrow stimulation could be considered as a first-line treatment option for OLTs with subchondral cysts.
The present study does have some limitations. First, the number of patients was relatively small, and the follow-up period was short. However, randomized controlled clinical trials for this type of procedure are difficult to conduct. Certainly, a randomized comparison of marrow stimulation with or without an injection of an SVF containing MSCs with a larger series of cases and a longer follow-up period would increase the strength of this study for a more accurate evaluation of the effects of MSCs in OLTs. Second, we compared the clinical and MRI outcomes of the conventional and MSC groups and investigated the associations between clinical and MRI outcomes. Importantly, MRI has been shown to be suitable for cartilage imaging and especially for the evaluation of cartilage repair. However, as we know, according to the report by Roberts et al, 48 histological cartilage findings do not necessarily correlate with MRI; thus, a histological analysis or biochemical assessment of cartilage using T2 mapping is necessary to identify the effects of MSCs more precisely. Third, follow-up MRI was performed at 22 months postoperatively, and it is unknown how the repaired cartilage will behave over time; changes in influencing factors after 22 months cannot be predicted. Fourth, the number of MSCs contained in an SVF to be injected to achieve an optimal response is unknown; we plan to perform a study on this in the future. Lastly, MSCs injected into the patients in this study represented a mean of 9.1% of SVF cells; therefore, we cannot know for sure whether the positive effects observed in this study were caused by the MSCs alone.
In conclusion, this study showed that the clinical and MRI outcomes of an injection of an SVF containing MSCs with marrow stimulation were encouraging, compared with marrow stimulation alone, in patients with OLTs. Furthermore, an injection of an SVF containing MSCs with marrow stimulation influenced better outcomes than marrow stimulation alone when the patient was aged older than 46.1 years, the lesion size was larger than 151.2 mm2, or in the presence of subchondral cysts. Therefore, although this treatment is still in the early stages of application, we propose that an injection of an SVF containing MSCs with marrow stimulation should be considered as a treatment for OLTs, even if there are poor prognostic factors, including older age, large-sized lesion, or the presence of subchondral cysts.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.