
Abstract
Background:
A common treatment for posterior meniscal root tears is transtibial pull-out repair, which has been biomechanically reported to restore tibiofemoral contact mechanics to those of the intact knee. Biomechanical data suggest that there is significant displacement of the repaired meniscal root with cyclic loading, which may be responsible for the poor healing and meniscal extrusion demonstrated in some clinical studies.
Hypothesis/Purpose:
The purpose of this study was to quantify the time-zero displacement of the posterior meniscal root in response to cyclic loading after transtibial pull-out repair and to quantify the individual contributions to displacement of the following: (1) suture elongation, (2) button-bone interface, and (3) meniscus-suture interface. The meniscus-suture interface was hypothesized to result in significantly more displacement than the button-bone interface or suture elongation.
Study Design:
Descriptive laboratory study.
Methods:
Transtibial pull-out repair of the posterior medial meniscal root was performed in 6 porcine knees, and cyclic displacement was measured using a loading protocol representative of postoperative rehabilitation. Displacement from (1) suture elongation, (2) the button-bone interface, and (3) the meniscus-suture interface was determined by cyclically loading 6 specimens for each construct using the same loading protocol to determine the contribution of each component to the overall displacement of the repair construct.
Results:
After 1000 cycles, the repair construct displaced by a mean of 3.28 mm (95% CI, 2.07-4.49). The meniscus-suture component (mean, 2.52 mm; 95% CI, 2.21-2.83) displaced significantly more than the button-bone component (mean, 0.90 mm; 95% CI, 0.64-1.15; P = .006) and suture elongation component (mean, 0.71 mm; 95% CI, 0.36-1.06; P = .006) after 1000 cycles. Displacement of the button-bone and suture elongation components was not significantly different after 1000 cycles (P = .720).
Conclusion:
There was substantial displacement of the posterior medial meniscal root repaired with the transtibial pull-out technique under a cyclic loading protocol simulating postoperative rehabilitation. The meniscus-suture interface contributed to significantly more displacement than the button-bone interface and suture elongation in the transtibial pull-out repair construct.
Clinical Relevance:
The results provide a framework for optimizing the transtibial pull-out repair technique. Future studies should focus on improving suture fixation strength within the meniscus-suture interface.
Meniscal root tears have been reported to result in increased tibiofemoral contact pressures and meniscal extrusion under loads representative of normal gait.1,8,12,14,16,20 Posterior root tears of the medial meniscus may pose particularly adverse outcomes for patients,1,8,14,16 with 1 study reporting that posterior medial meniscal root tears are not significantly different than total medial meniscectomies in terms of peak tibiofemoral contact pressures. 1
One common technique for the treatment of posterior meniscal root tears is transtibial pull-out repair, which secures the meniscal root to its footprint on the tibia using sutures that are passed through a transtibial tunnel and secured over the anteromedial tibial cortex (Figure 1).1,2,7,10,12,13,16,20,21 In brief, the sutures are passed through the meniscal root tissue, brought through a tibial tunnel entering the joint at the anatomic attachment of the root, 9 and tied over a titanium button on the anterior tibia.2,7,16 Biomechanical studies on the posterior medial meniscal root have reported that the transtibial pull-out repair technique can restore tibiofemoral contact areas and pressures to those of the intact knee at time zero in vitro.1,7,16
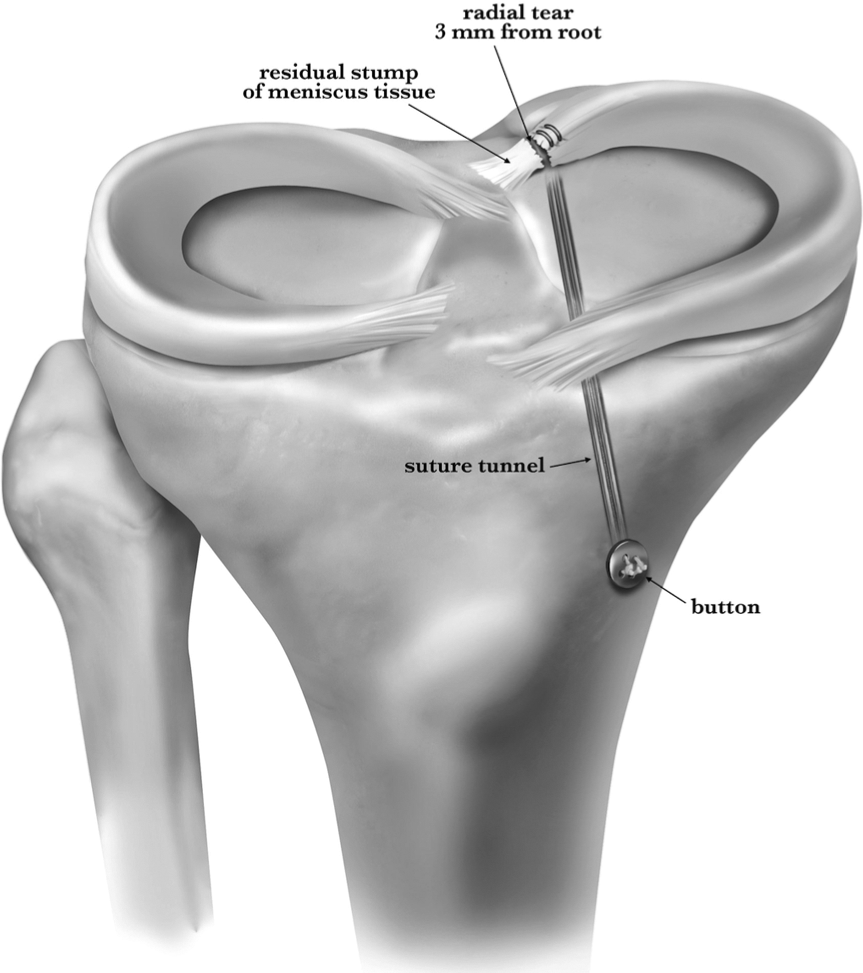
Transtibial pull-out repair for a complete radial root tear 3 mm from the bony attachment of the posterior medial meniscal root. (Reprinted with permission from Padalecki JR, Jansson KS, Smith SD, et al. Biomechanical consequences of a complete radial tear adjacent to the medial meniscus posterior root attachment site: in-situ pullout repair restores derangement of joint mechanics. Am J Sports Med. 2014;42(3):699-707.)
In contrast, level 3 and 4 clinical outcome studies have reported controversial results using this repair technique.10,13,15,21 At clinical follow-up of 1 to 3 years after using transtibial pull-out repair, clinical outcomes have been reported to improve significantly.10,13,15,21 However, studies have also reported less than satisfactory results with regard to meniscal extrusion10,15 and the healing of meniscal tissue on second-look arthroscopic surgery.13,21 Further, significant time-zero displacement of the transtibial pull-out repair construct of 2.2 to 3.8 mm has been observed in a porcine model after cyclic loading, representative of the loads experienced during postoperative rehabilitation.5,17,23 As shown in a porcine biomechanical model, nonanatomic placement of the meniscal root by only 3 mm significantly compromises meniscal function 22 ; therefore, displacement of the root by the levels shown in previous studies may also undermine meniscal functioning.5,17,23 To date, the reasons for this displacement have yet to be elucidated; however, there is believed to be a “bungee effect” in which suture elongation or longitudinal motion of the sutures within the transtibial tunnel results in displacement of the repaired meniscal root. 5 A better understanding of the contributions of individual components of the transtibial pull-out technique, including the “bungee effect,” to displacement of the repair construct would allow optimization of the surgical technique. Specifically, optimizing the component that induces the most displacement, via suture elongation, the button-bone interface, or the meniscus-suture interface, may enhance the biomechanical properties of the repair construct and potentially improve clinical outcomes.
Therefore, the purpose of this study was to quantify the time-zero displacement of the posterior medial meniscal root in response to cyclic loading after transtibial pull-out repair in a porcine biomechanical model and to quantify the specific contributions of the individual components of this technique including the following: (1) suture elongation (the “bungee effect”), (2) the button-bone interface on the anteromedial tibia, and (3) the meniscus-suture interface. It was hypothesized that the meniscus-suture interface would result in significantly more displacement than either suture elongation or the button-bone interface.
Materials and Methods
Specimen Preparation
Eighteen porcine knees were used in this study. These specimens were obtained from Innovative Medical Device Solutions and were within the range of 8 to 10 months of age. This porcine model was chosen because it has been used in numerous previous biomechanical testing models for meniscal repair.4-6,17,18,22,23 Knees were dissected free of all extra-articular skin, muscle, and soft tissue. The femoral attachments of the anterior and posterior cruciate ligaments, medial and fibular collateral ligaments, and posterior lateral meniscal attachments were sharply transected to expose the tibial plateau, metaphysis, and 4 cm of the proximal tibial diaphysis. The fibula was also removed from the tibia.
Repair Technique
Knees were randomly and evenly distributed between the full repair construct group, button-bone interface group, and meniscus-suture interface group, with 6 specimens per group. The first group (full repair construct) received standardized transtibial pull-out repair of the posterior medial meniscal root. The posterior medial meniscal root was sharply transected at its anatomic attachment to the tibial plateau. The tip of an anterior cruciate ligament guide (Acufex, Smith & Nephew) was placed at the anatomic attachment of the posterior root and set at a tunnel distance of 5 cm. A guide pin was drilled from the anteromedial tibia to the posterior medial meniscal root attachment. A 5-mm cannulated reamer (Arthrex Inc) was then used to ream over the guide pin. Two No. 2 nonabsorbable sutures with half-circle tapered needles (FiberWire, Arthrex Inc) were then inserted using a 2–simple suture configuration, 5 mm from the posterior root attachment of the medial meniscus. This 2–simple suture configuration was chosen because it is the preferred technique of the senior author (R.F.L.) because of its ability to be placed in the tight tibiofemoral joint and its reported capacity to resist displacement in comparison to more complex suture techniques.2,4 In addition, the specific type of No. 2 nonabsorbable suture has also been recommended for transtibial pull-out repair by a study evaluating suture types because of its low displacement and high maximum yield and stiffness compared with other suture types. 6 The 2 individual sutures, 4 limbs in total, were then shuttled through the transtibial tunnel and tied over a metal 6-hole surgical button on the anteromedial tibia by a single surgeon using a surgeon’s knot followed by 3 half-hitches on alternating posts. The sutures were cut approximately 1 cm from the knot.
Each of the 3 individual components of the transtibial pull-out repair construct was then isolated. Displacement due to elongation of the suture (suture elongation group) was measured by tying 2 No. 2 nonabsorbable sutures (FiberWire), 5.5 cm in length, to standardize the length of the sutures in the meniscal root and transtibial tunnel, over a steel rod (suture elongation group, n = 6). The sutures were then passed through a 5-mm hole in a steel plate, which was fixed to the base of the test frame, and tied over a surgical button by a single surgeon (A.J.C.) in the same manner as above. The steel plate provided a rigid simulation of the cortex.
Next, displacement due to interaction of the button and cortex of the bone on the anteromedial tibia was quantified (bone-button interface group, n = 6). In this group, the menisci were sharply dissected from their root attachment. Tunnel creation and reaming were performed following the same procedure as with the full construct group. Sutures were then looped over a metal rod and measured to be 5.5 cm in length. This required the tibial plateau to be cut approximately 2 cm from the top of the articular cartilage to allow for the sutures to pass over the steel rod. Sutures were then passed through the bone tunnel, and a surgical button was tied over the anteromedial tibia by passing the sutures through the holes in the button and tying the sutures in the same manner as above.
Lastly, displacement due to cutout of the suture through the meniscus was quantified (meniscus-suture interface group). Six knees were assigned to this group, and the menisci were sharply dissected from their tibial attachment. Just as above, two No. 2 nonabsorbable sutures were inserted into the posterior medial meniscal root, 5 mm from the root attachment. The sutures were then passed through a steel plate and tied over a surgical button to yield a total suture length of 5.5 cm, which was standardized with the full construct repair group.
Biomechanical Testing
The distal tibias of the full transtibial repair construct and button-bone interface groups were potted in polymethylmethacrylate (Fricke Dental International Inc) at a point 4 cm distal to the proximal aspect of the tibial tuberosity. 3 The tibias were rigidly secured to the base of a dynamic tensile testing machine (ElecroPuls E10000, Instron) with a custom steel fixture. The fixture allowed the position of the tibia to be adjusted such that the force vector was in line with the transtibial tunnel and perpendicular to the base. For the full repair constructs, the repaired meniscus was then marked with a surgical pen at a distance 1 cm from the sutures. Proximal to this location, metal wire was wrapped around the meniscal tissue to prevent slippage or tearing of the tissue within the clamp. 3 The meniscus was then clamped 1 cm from the sutures in the meniscus and rigidly fixed to the actuator of the tensile testing machine (Figure 2).
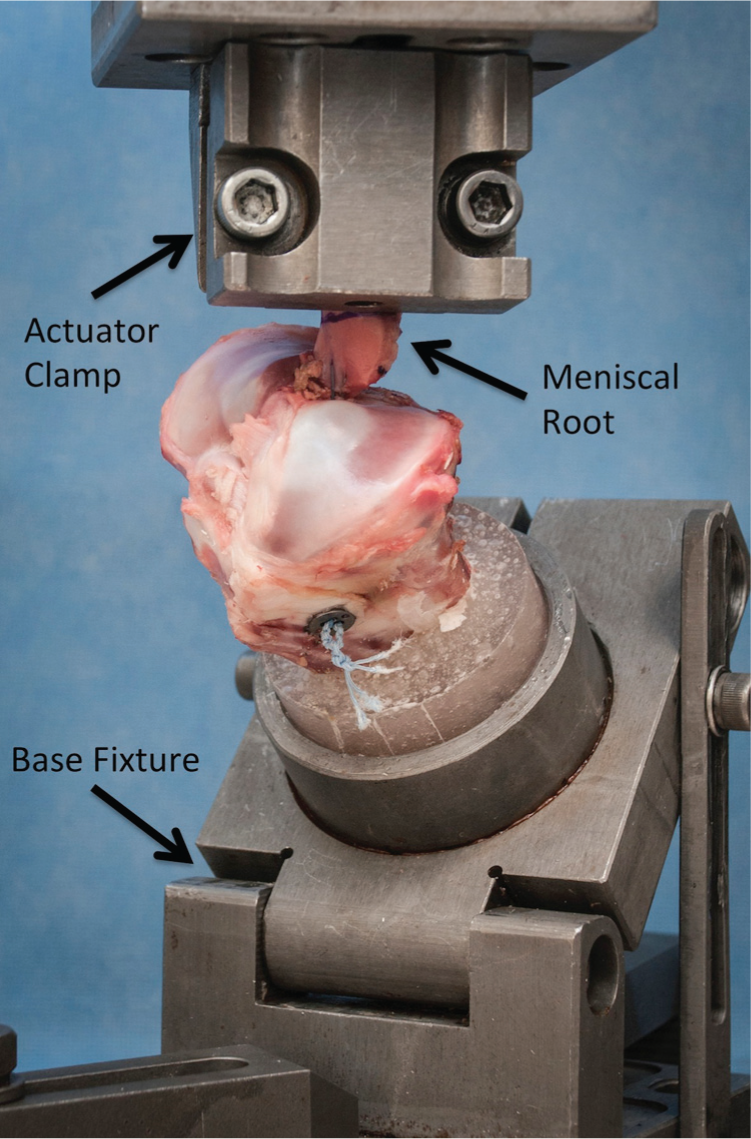
Biomechanical testing setup for the transtibial pull-out repair technique. The potted tibia was fixed in a custom fixture and secured to the base of the tensile testing machine. The repaired meniscal root was then clamped to the actuator of the tensile testing machine. The force vector was in line with the transtibial tunnel.
For the suture elongation group, a steel plate was also fixed to the base of the tensile testing machine after securing the sutures to the plate with a surgical button. The sutures were looped over a 4.5-mm steel rod, which was rigidly fixed to the actuator of the test frame (Figure 3). For the button-bone interface group, the tibia was positioned in the same manner as the full repair construct. The sutures were then looped around a 4.5-mm steel rod that was rigidly attached to the actuator of the tensile testing machine, and the transtibial tunnel was aligned so that the force vector was in line with the tunnel and in line with the base (Figure 4). For the meniscus-suture interface group, the meniscus was prepared and clamped as described for the full construct group, and the steel plate was rigidly fixed to the base of the test frame after securing the sutures to the plate with a surgical button (Figure 5).
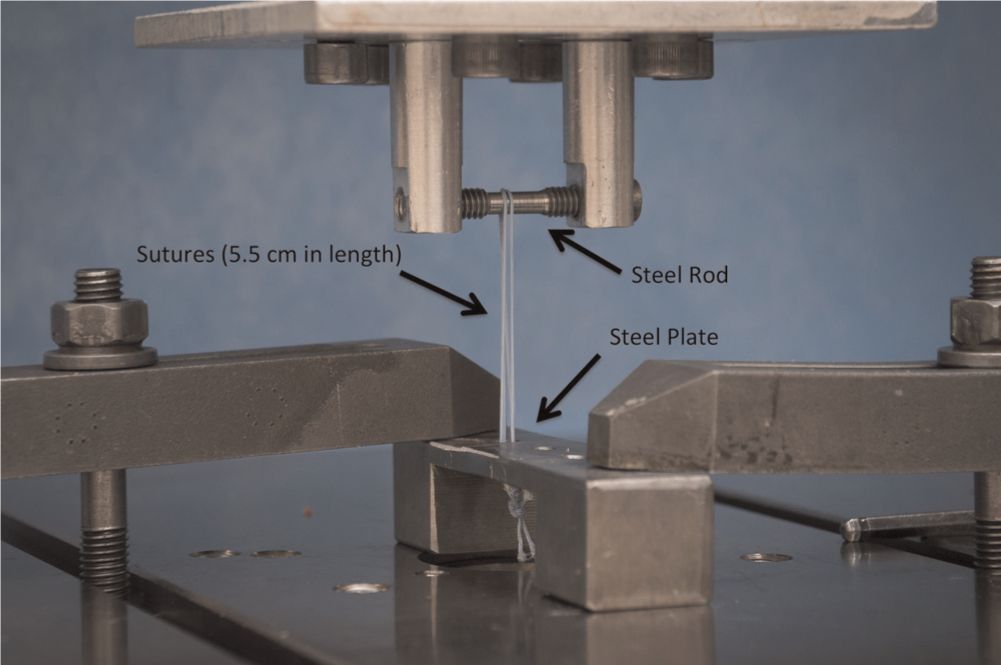
The suture elongation component was isolated by testing 2 parallel suture loops, each 5.5 cm in length. The suture length was representative of the length used in the full-repair construct. The sutures were then looped over a steel rod attached to the actuator of the tensile testing machine. The sutures were then passed through a steel plate fixed to the base of the tensile testing machine and tied over a surgical button.
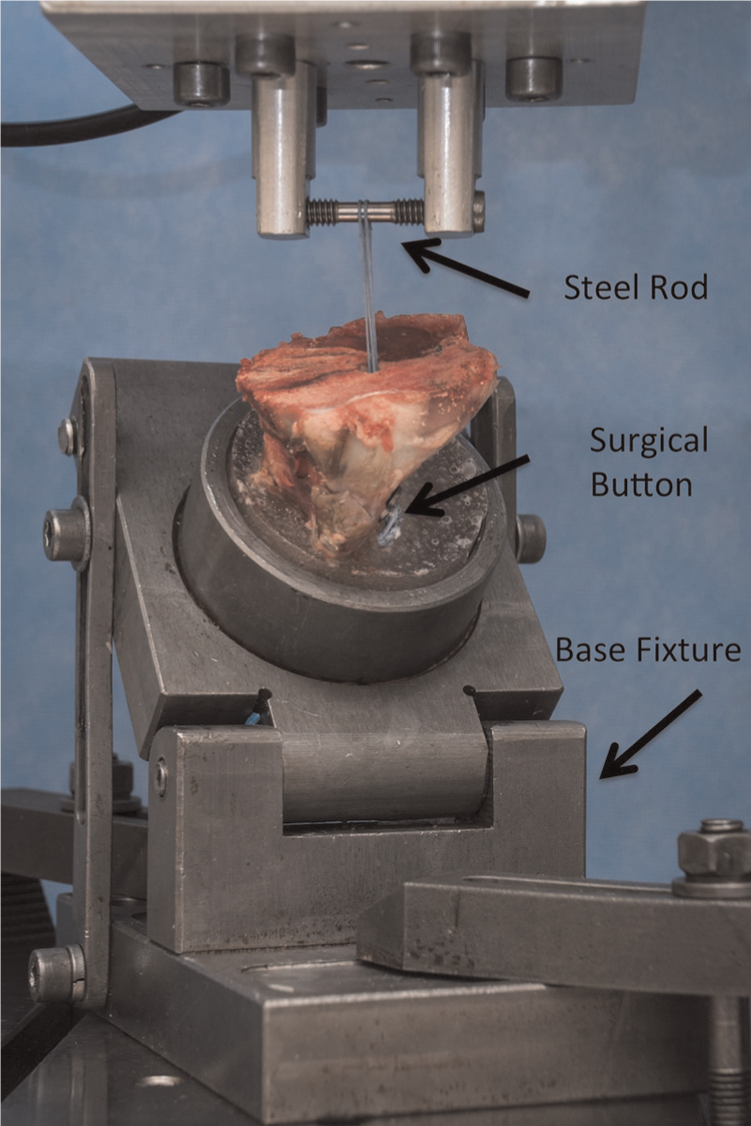
The button-bone interface was isolated by rigidly fixing the potted tibia in a custom fixture to the base of the tensile testing machine. The anterior, proximal 2 cm of the tibia was removed with a saw to allow room for the sutures to be looped over the steel rod. The sutures were placed through the transtibial tunnel, looped over a steel rod attached to the actuator of the tensile testing machine at a length of 5.5 cm, and tied over a surgical button on the anteromedial tibia.
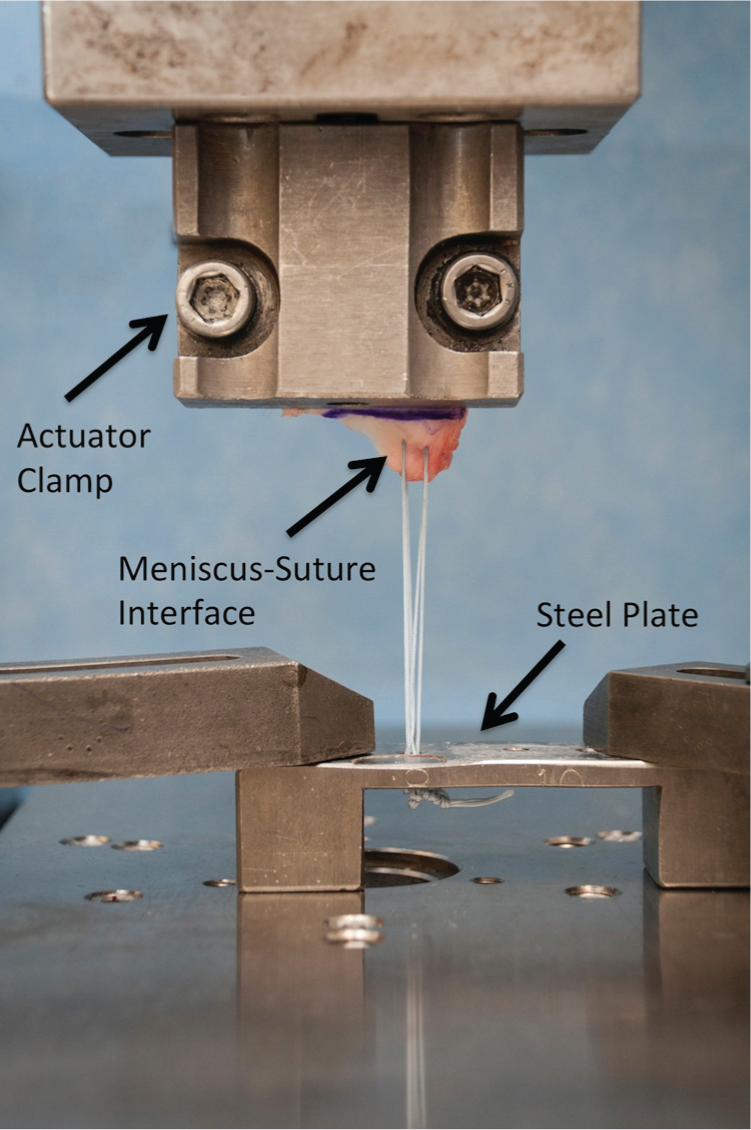
The meniscus-suture interface construct. The meniscal root was clamped to the actuator 1 cm from the entry point of the sutures in the meniscus. The sutures were then passed through a steel plate that was rigidly fixed to the base of the tensile testing machine and tied over a surgical button.
All groups were then subjected to the same cyclic tensile loading protocol. Specimens were preconditioned with 10 cycles from 1 to 10 N at 0.1 Hz to minimize any creep within the meniscal fibers. After preconditioning, the tibias were cyclically loaded for 1000 cycles from 10 to 30 N at 0.5 Hz. This protocol was chosen to approximate the tensile forces that the posterior medial meniscal root may experience under neutral rotation, knee flexion to approximately 30° to 60°, and 500 N of tibiofemoral load, which are believed to be the standard range of motion and toe-touch weightbearing protocols over the course of a typical 6-week postoperative rehabilitation regimen after meniscal root repair. 23 It should be noted that this protocol does not account for gradual healing of the meniscal root over the course of rehabilitation. Displacement was recorded at the actuator of the test frame of the tensile testing machine.
Statistical Analysis
Based on the cyclic displacement data of the first 3 specimens per group, and setting the per-comparison α level to .0167 (Bonferroni correction), sample size calculations were performed. At this midpoint, the effect size estimate for each comparison was large (in excess of 2.9). Six specimens per group was found to be sufficient to detect a conservatively reduced effect size of 2.5 among the individual components with 80% power.
All pairwise comparisons of cyclic displacement among the 3 components were conducted using nonparametric Mann-Whitney U tests. Bonferroni corrections were applied within each cyclic loading setting (100, 500, or 1000 cycles) to account for multiple testing. The level of statistical significance was set at .05. Data are presented as means with 95% CIs. All statistical analyses were performed using SPSS Statistics (v 20, IBM Corp).
Results
Displacement after 100, 500, and 1000 cyclic loading cycles for each group is listed in Table 1. Cyclic displacement of the repair construct and individual components is reported as the mean and 95% CI. Displacement of the meniscus-suture interface group and bone-button interface group was calculated by subtracting the mean displacement of the suture elongation group.
Cyclic Displacement of Transtibial Pull-out Repair Construct and Isolated Components a
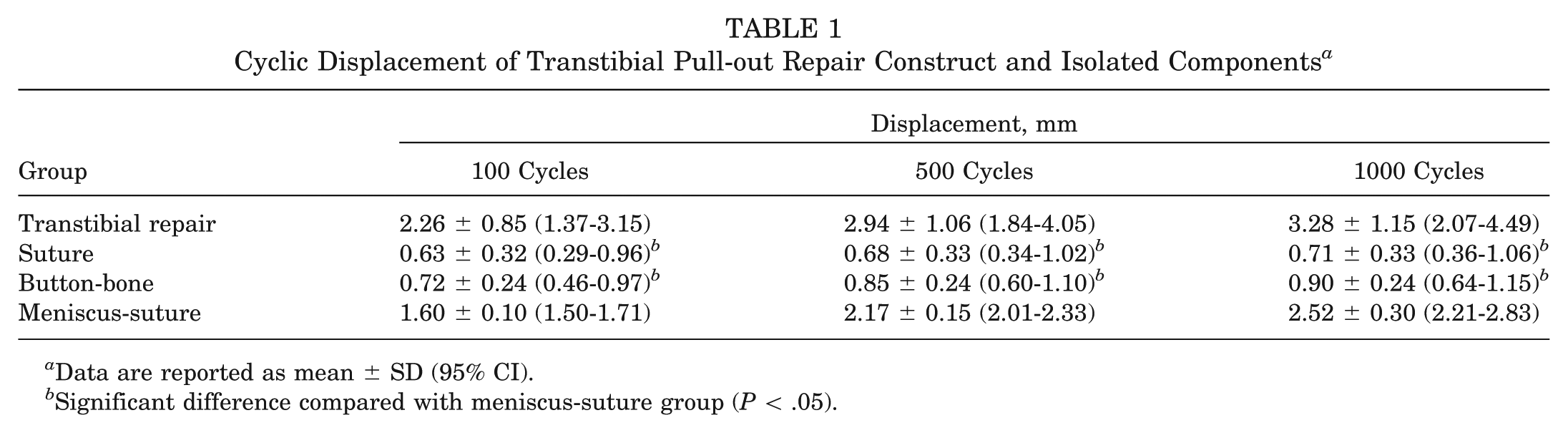
Data are reported as mean ± SD (95% CI).
Significant difference compared with meniscus-suture group (P < .05).
The entire repair construct displaced by a mean of 3.28 mm (95% CI, 2.07-4.49) after 1000 cycles. After 1000 cycles, the meniscus-suture interface component (mean, 2.52 mm; 95% CI, 2.21-2.83) displaced because of partial suture cutout of the meniscus, and it displaced significantly more than the button-bone interface component (mean, 0.90 mm; 95% CI, 0.64-1.15; P = .006) and suture elongation component (mean, 0.71 mm; 95% CI, 0.36-1.06; P = .006). After 100 and 500 cycles, the meniscus-suture interface group also significantly displaced more than the button-bone interface and suture elongation groups (P = .006 for all comparisons). Displacement due to the button-bone interface and suture elongation was not significantly different at 100, 500, or 1000 cycles (P = 1.000, .930, and .720, respectively) (Figure 6).
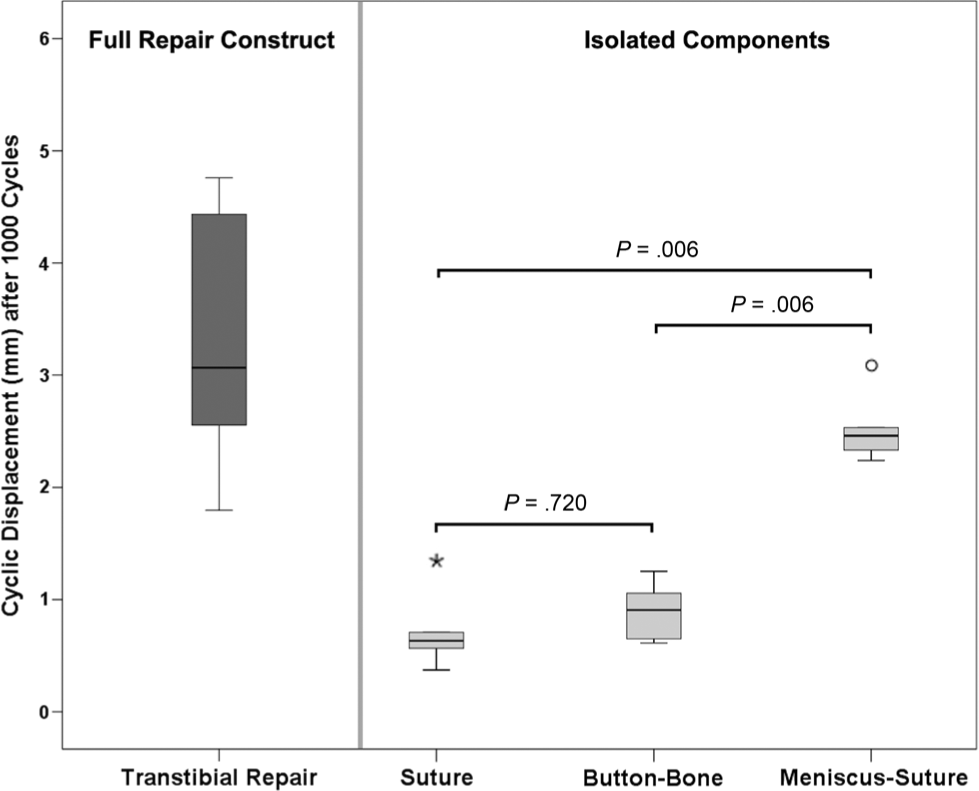
Boxplot illustrating the overall cyclic displacement of each testing group after 1000 cycles. Outliers are noted for the suture only (*) and meniscus-suture interface (°). The meniscus-suture interface contributed significantly more displacement than either suture elongation or the button-bone interface (P = .006). Suture elongation and the button-bone interface were not significantly different in terms of cyclic displacement (P = .720).
Discussion
In this study, the meniscus-suture interface group resulted in significantly more displacement than either the button-bone interface or suture elongation groups, thereby supporting our hypothesis. Furthermore, the previously theorized “bungee effect,” in which suture elongation or longitudinal motion of the sutures within the transtibial tunnel is responsible for displacement of the repair, 5 was disproven as the primary source of displacement. In addition, the full repair construct resulted in displacement that exceeded the threshold of 3 mm of displacement that has been reported to significantly alter meniscal function in a porcine model. 22 Therefore, the authors believe that there remains a significant need for optimization of the transtibial pull-out repair technique based on the isolated results of this study. We believe that the primary focus of this optimization should be aimed at reducing the amount of suture cutout at the suture-meniscus interface; however, it cannot be assumed that the same effect of displacement would be seen in vivo. Therefore, future studies should investigate this issue.
The meniscus-suture interface contributed significantly more displacement (2.52 mm) after 1000 cycles when compared with the suture elongation (0.71 mm) or button-bone interface (0.90 mm) groups. Previous studies have described suture cutout of the meniscus as the method of failure in all human and porcine specimens using the 2–simple suture technique.5,11 In addition, 1 study evaluated different meniscus-suture fixation techniques for the posterior medial meniscal root with a similar testing protocol as our meniscus-suture interface group. 4 The authors in that study reported 0.6 mm of cyclic displacement for the 2–simple suture configuration under 1000 cycles of 5 to 20 N at 0.5 Hz, 4 which is much lower than what we found in our study. The authors believe that this may indicate that when pulling directly on the meniscal tissue, as done when evaluating the meniscus-suture interface, even slightly increasing the loads on the meniscal tissue may substantially increase suture cutout. Other studies have also evaluated the displacement of 1– or 2–simple suture configurations for the posterior lateral meniscal root and reported variable results in a porcine model.6,17 However, as the posterior lateral meniscal root attaches to the femur in porcine knees, we believe that this substantial difference in anatomy, and likely the meniscal tissue, prevents any reliable comparisons between these studies and the current study because of the confounding variables that may be present.
For the full transtibial pull-out repair construct, we measured a mean of 3.28 mm of displacement after 1000 cycles of 10 to 30 N at 0.5 Hz. Two previous studies have evaluated cyclic displacement under similar loading conditions to represent the loads that may be experienced by the posterior medial meniscal root during a typical postoperative regimen.5,17,23 Feucht et al 5 reported that under a loading protocol of 1000 cycles of 5 to 20 N at 0.5 Hz, using a 2–simple suture configuration, the posterior medial meniscal root displaced 2.2 mm, approximately 1 mm less than reported in our study. Cyclic loading was applied in line with the circumferential fibers of the posterior medial meniscal root, 5 similar to our study. However, we chose a higher loading protocol than Feucht et al 5 to represent tensions that the posterior medial meniscal root may experience under neutral rotation, knee flexion from 30° to 60°, and 500 N of tibiofemoral loads, all of which we believe to be possible during a standard toe-touch weightbearing postoperative rehabilitation program after meniscal root repair. 23 We believe that our finding of increased displacement in comparison to Feucht et al 5 is consistent and intuitive, given the increased cyclic loading protocol. It should be noted that the suture anchor technique resulted in significantly lower levels of displacement than the transtibial pull-out technique in the Feucht et al 5 study (1.3 mm); however, in the opinion of the senior author (R.F.L.), it is very technically difficult to achieve anatomic placement of the medial meniscal posterior root in the small arthroscopic space without a concurrent medial collateral ligament injury. Therefore, we believe that the suture anchor repair technique is currently only indicated for a small subset of medial meniscal root tears.
In addition, Röpke et al 17 measured displacement of transtibial pull-out repair for the posterior medial meniscal root and reported 3.8 mm of displacement during cyclic loading. It should be noted that there are numerous methodological differences between this study and ours. First, Röpke et al 17 applied loading via the button, used a modified Kessler stitch pattern and sawbones construct, and repetitively loaded the meniscus with 100 cycles between 1 and 10 N at 1 Hz. In addition, the authors termed their recorded displacement “suture elongation” 17 ; however, in our opinion and given the results of the current study, the authors likely measured the combined displacement of both the meniscus-suture interface and suture elongation. Given the methodological differences between our study and that of Röpke et al, 17 we believe that it is difficult to realistically compare the results of cyclic displacement between these studies. In addition, it should be noted that we believe a direct measurement of suture elongation has not been previously reported in the literature; therefore, the reported 0.71 mm of suture elongation in this study may be a novel addition to the literature. Future studies should evaluate the elongation of different types of sutures.
Just as with the suture elongation group, the authors believe that displacement due to the button-bone interface has not been previously evaluated in the literature. In this study, the isolated displacement of the button-bone interface contributed 0.90 mm of displacement, which was significantly less than that of the meniscus-suture group. Previous studies using the transtibial pull-out repair technique have described using surgical buttons1,7,12,16 or screw and washers.7,10,20,21 Given the results of this study, a surgical button provides secure fixation that can theoretically be less invasive and avoid postoperative irritation compared with screw and washer fixation. Future studies should compare the biomechanical properties of the surgical button and screw and washer fixation techniques.
The results of the current study emphasize the importance of using caution during rehabilitation after meniscal root repair to minimize displacement and maximize the likelihood for anatomic healing.4,5,11 The repaired posterior medial meniscal root displaced greater than the previously reported 3-mm threshold for maintaining native meniscal function 22 under tibiofemoral loads representative of toe-touch weightbearing in the postoperative period. 23 Therefore, we believe that these results give further credence to the theory that partial toe-touch weightbearing for 6 weeks, followed by a slow progression to full weightbearing at approximately 8 weeks, is necessary to allow for adequate soft tissue healing.2,7
Lastly, the potential of the meniscus to displace significantly under low tibiofemoral loading conditions using the standard meniscus-suture fixation method of 2 simple sutures reveals further that optimization of meniscal root repair techniques is necessary. In a previous porcine study, the 2–simple suture technique was reported to result in significantly less displacement than the more complex fixation techniques of horizontal mattress and 2 modified loop stitches. 4 In addition, while not reported to be significant, the more complex modified Mason-Allen stitch was reported to result in approximately 47% more displacement than the 2–simple suture technique, although the modified Mason-Allen stitch was reported to have a higher ultimate failure strength. 4 Therefore, the 2–simple suture fixation technique may be the best current option for minimizing displacement based on the available literature, and given that 2.52 mm of displacement was reported using this technique in this study, there remains significant room for improvement. Future studies should investigate other meniscus-suture fixation methods. Theoretically, by using more sutures, 18 less abrasive sutures, varying suture techniques, and/or a greater surface area to optimize fixation, displacement due to suture-meniscus cutout may be minimized. The current study provides the framework to move forward with studies on meniscal root repair optimization.
As with any biomechanical study, there are some inherent limitations of our study. The first limitation is that because this is a time-zero study, the potential gradual healing that the meniscal root would undergo over the course of rehabilitation in vivo cannot be taken into account. Also, this study used a porcine model, which has stiffer meniscal tissue than human meniscal tissue.
19
However, the use of a young porcine model (age, 8-10 months) offered the advantage of standardized tissue and bone quality. Previous studies using human meniscal tissue reported high variability in tissue and bone quality between specimens.3,11 In addition, using a porcine model offered the ability to compare our results to the current biomechanical literature on meniscal root repair, with studies that have all used a porcine model.4-6,17,18,22,23 Although the amount of displacement in the present study may not be directly transferable to human tissue, the authors theorize that similar trends between the 3 tested components would be observed, with significantly more displacement due to the suture-meniscus interface. Therefore, because the purpose of this study was to compare how the different components contributed to displacement of the meniscal root repair construct, the high level of control and standardization of tissue and bone quality offered by the porcine model was ideal. Another limitation of this study is that the maximum number of cycles (ie, 1000) is relatively short. It is unknown if steady state is reached at 1000 cycles because we did not test beyond this number. However, we do not believe that it was necessary to test until a steady state was reached, nor would it be appropriate, because this was a time
Conclusion
Under cyclic loads similar to those experienced in postoperative rehabilitation, the transtibial pull-out repair construct of the posterior medial meniscal root resulted in more displacement (3.28 mm) than the current reported threshold for altered meniscal function (3 mm). 22 The meniscus-suture interface also contributed to significantly more displacement than the button-bone interface or suture elongation in the transtibial pull-out repair construct. Therefore, the meniscus-suture interface should be the primary target of future optimization studies aimed at eliminating the displacement of transtibial pull-out repair.
Footnotes
Acknowledgements
The authors acknowledge Barry Eckhaus for his assistance with medical photography and Grant Dornan, MSc, for his statistical expertise.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.F.L. is a consultant for Arthrex. This study was sponsored by the Steadman Philippon Research Institute.