
Abstract
Background:
Graft extrusion after meniscus allograft transplantation (MAT) may be affected by horn fixation, which differs between medial and lateral MAT. Few studies have compared graft extrusion, especially sagittal extrusion, after medial and lateral MAT.
Hypothesis:
In patients undergoing medial and lateral MAT, graft extrusion is likely similar and not correlated with postoperative Lysholm scores.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Meniscus graft extrusion in the coronal and sagittal planes was compared in 51 knees undergoing medial MAT and 84 undergoing lateral MAT. Distances from the anterior and posterior articular cartilage margins to the anterior (anterior cartilage meniscus distance [ACMD]) and posterior (posterior cartilage meniscus distance [PCMD]) horns, respectively, were assessed on immediate postoperative magnetic resonance imaging and compared in patients undergoing medial and lateral MAT. Correlations between coronal and sagittal graft extrusion and between extrusion and the Lysholm score were compared in the 2 groups.
Results:
In the coronal plane, mean absolute (4.3 vs 2.7 mm, respectively; P < .001) and relative (39% vs 21%, respectively; P < .001) graft extrusions were significantly greater for medial than lateral MAT. In the sagittal plane, mean absolute and relative ACMD and PCMD values were significantly greater for medial than lateral MAT (P < .001 each). For both medial and lateral MAT, mean absolute and relative ACMDs were significantly larger than PCMDs (P < .001 each). Graft extrusion >3 mm in the coronal plane was significantly more frequent in the medial (78%) than in the lateral (35%) MAT group. In the sagittal plane, the frequencies of ACMDs (72% vs 39%, respectively) and PCMDs (23% vs 4%, respectively) >3 mm were also significantly greater in the medial than in the lateral MAT group. Coronal and sagittal extrusions were not correlated with postoperative Lysholm scores for both medial and lateral MAT.
Conclusion:
The amount and incidence of graft extrusion were greater after medial than lateral MAT in both the coronal and sagittal planes. In the sagittal plane, graft extrusion was greater and more frequent on the anterior than the posterior horn in both medial and lateral MAT. However, graft extrusion was not correlated with early clinical outcomes after both medial and lateral MAT.
Fresh-frozen meniscus allograft transplantation (MAT) is an effective treatment modality for subtotal or total meniscectomized knees, 10 providing short-, 16 medium-, 14 and long-term18,21 pain relief and functional improvements. A major concern regarding MAT, however, is graft extrusion, which is not infrequently found on magnetic resonance imaging (MRI) after MAT.5,12 The minimization of graft extrusion is important because extrusion due to nonanatomic positioning of the allograft can lead to biomechanical disadvantages. 24 It remains unclear, however, whether the extent of graft extrusion affects clinical outcomes.
The amount of graft extruded after MAT appears to be constant for a given allograft size. 13 Thus, if allograft sizing is accurate, graft extrusion can be minimized by precise surgical techniques. 25 These techniques usually differ for medial and lateral menisci. In general, medial MAT is performed using a bone plug method, whereas lateral MAT is performed using a bony trough (keyhole) technique. These differences in surgical techniques may lead to differences in allograft extrusion on the medial and lateral sides. To date, however, only 1 study has compared meniscus allograft extrusion after medial and lateral MAT. 9 In addition, graft extrusion has been investigated only in the coronal 4 and axial3,11 planes of MRI, not in the sagittal plane. The weightbearing function of the meniscus is based on the circumferential arrangement of collagen fibers, which should be anchored at their respective anterior and posterior horns of the meniscus. Therefore, improper osseous tunnel placement, both in the bone plug technique for medial MAT and in the keyhole technique for lateral MAT, may result in graft extrusion in the sagittal plane. 19 This study was designed to compare meniscus allograft extrusion after medial and lateral MAT, as determined by immediate postoperative MRI in both the coronal and sagittal planes. We hypothesized that graft extrusion in patients undergoing medial MAT would likely be similar to that in patients undergoing lateral MAT, as assessed on both coronal and sagittal MRI, and would not correlate with early clinical outcomes.
Materials and Methods
Study Design and Patient Inclusion
This prospective longitudinal trial included all patients who underwent isolated medial or lateral MAT without a concomitant procedure, such as ligament reconstruction, osteotomy, or a cartilage procedure, at our institution between 2009 and 2012, followed by immediate postoperative MRI. The indications for MAT included pain in 1 compartment due to the lack of a meniscus; articular chondral wear of Outerbridge grade III (focalized IV) or less, as confirmed by previous arthroscopic surgery; and neutral alignment of the lower limb, which was evaluated both clinically and using long-leg standing radiographs. The contraindications for surgery included uncorrected deformities of limb alignment involving >5° deviation toward the involved compartment, generalized osteoarthritis involving the contralateral compartment or the patellofemoral joint, or uncorrected joint instability due to a ligament tear. Of the 140 patients (140 knees, including 53 that underwent medial MAT and 87 that underwent lateral MAT) initially approached, 138 patients (138 knees) agreed to take part and were enrolled. Three patients were excluded because they did not undergo immediate postoperative MRI. Finally, data from 135 patients (135 knees, with 51 that underwent medial MAT and 84 that underwent lateral MAT) were analyzed. The preoperative demographic characteristics of the 2 groups were similar (Table 1). The study was explained to each patient, and each patient provided written informed consent. The study protocol was approved by the institutional review board of our institution.
Demographic Characteristics of Patients a
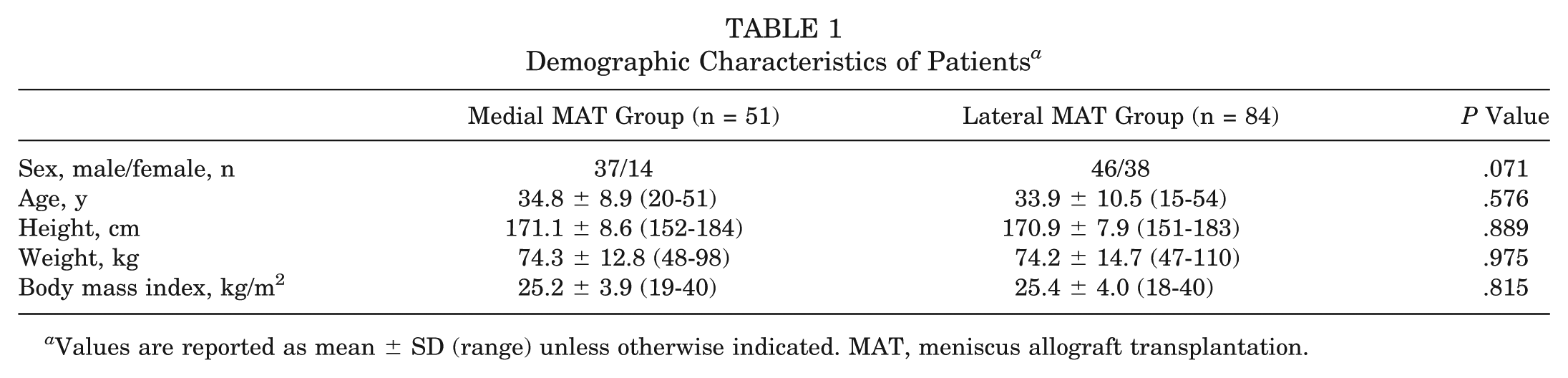
Values are reported as mean ± SD (range) unless otherwise indicated. MAT, meniscus allograft transplantation.
Allograft Sizing, Surgical Technique, Rehabilitation, and Clinical Assessment
Allografts in this study were sized based on plain radiographs taken in the anteroposterior and lateral projections because of practical limitations of MRI-based sizing methods, such as the limited ability of contralateral MRI to predict required meniscus dimensions and the inability of the tissue bank to provide transverse, cross-sectional sized-matched allografts. 26 Sizing radiographs were measured as described previously. 15 Every effort was made to obtain true anteroposterior and lateral radiographs by using a 100-mm radio-opaque rod, thus minimizing magnification and the risk of inaccurate bony landmark measurements. The desired meniscus size was communicated to the tissue bank (Korea Bone Bank), which then provided a fresh-frozen meniscus allograft that never exceeded a 10% mismatch in width or length. Graft safety was confirmed via mandatory serological screening at the tissue bank. All menisci in the medial compartment were transplanted using the modified double bone plug technique, 17 and all menisci in the lateral compartment were transplanted using the modified keyhole technique. 23 Attention was paid to re-creating the native anterior and posterior horn attachments of the meniscus using bone-to-bone healing. All implants consisted of a fresh-frozen meniscus allograft.
Host menisci were resected arthroscopically, leaving a 1- to 2-mm peripheral rim to achieve punctate bleeding. The meniscus allograft was introduced through anterior mini-arthrotomy. Two No. 2-0 nonabsorbable leading sutures, anchored at the most posterior portion of the allograft, were passed through the posteromedial or posterolateral incision by pulling on the passing wire sutures. At this point, the position and seating of the graft must be those of a normal meniscus, without graft wrinkling or flouncing. Some graft extrusion in the midbody portion could be found at this time by probing. After confirming that the graft position and seating were optimal, the 2 leading sutures were tied to each other just beneath the capsule. Using traditional inside-out meniscus repair techniques, 10 to 12 vertical No. 2-0 nonabsorbable sutures were placed at the midportion and posteromedial or posterolateral part of the meniscus allograft. The anterior part of the meniscus allograft was sutured to the anterior capsule under direct visualization.
Immediately after surgery, patients began quadriceps sets, straight-leg raises, and calf pumps. One or 2 days after surgery, the Hemovac drain (Zimmer) was removed, and continuous passive motion exercises were started during the first postoperative week. The goals for range of motion exercises were to achieve full extension equal to the contralateral side within 1 week, 90° of flexion within 4 weeks, and 120° of flexion within 6 to 8 weeks. Patients were allowed only toe-touch weightbearing during the first 2 weeks, which was increased slowly to 50% of the body weight by the fourth week and to full weightbearing by the sixth week. Rehabilitation continued for 3 months and focused on restoring full range of motion and quadriceps strength. At the last follow-up, 2 years after surgery, knee function was evaluated by assessing the Lysholm score, in which 95 to 100 indicated an excellent outcome, 84 to 94 indicated a good outcome, 65 to 83 indicated a fair outcome, and <65 indicated a poor outcome.
Coronal and Sagittal MRI Evaluations of Allograft Extrusion
Conventional MRI of the transplanted knee joint was performed on postoperative day 2 using a 3.0-T magnet (Achieva 3 T, Philips Healthcare). This early time point was selected to exclude the effects of any secondary changes in transplanted allografts caused by the remodeling process. During MRI, patients were placed in a supine position with a fully extended knee. The graft position was evaluated using sagittal and coronal proton density–weighted fast spin echo scans. Sagittal and coronal scans were acquired at slice thicknesses of 1.5 and 2.5 mm, respectively. Because maximum graft subluxation in the coronal plane usually occurs at the midbody portion, 7 consecutive coronal scans covering the entire midbody region were obtained. The subluxation distance in the coronal plane was defined as the distance between the outer edge of the articular cartilage of the tibial plateau and the outer edge of the meniscus (Figure 1A). 20 Extrusion was defined as subluxation >3 mm. Meniscus extrusion is reported as an absolute value and as a relative percentage of extrusion (RPE), defined as the width extruded divided by the entire width of the meniscus and reported as a percentage, with RPE therefore constituting a standardized measure for differently sized knees.
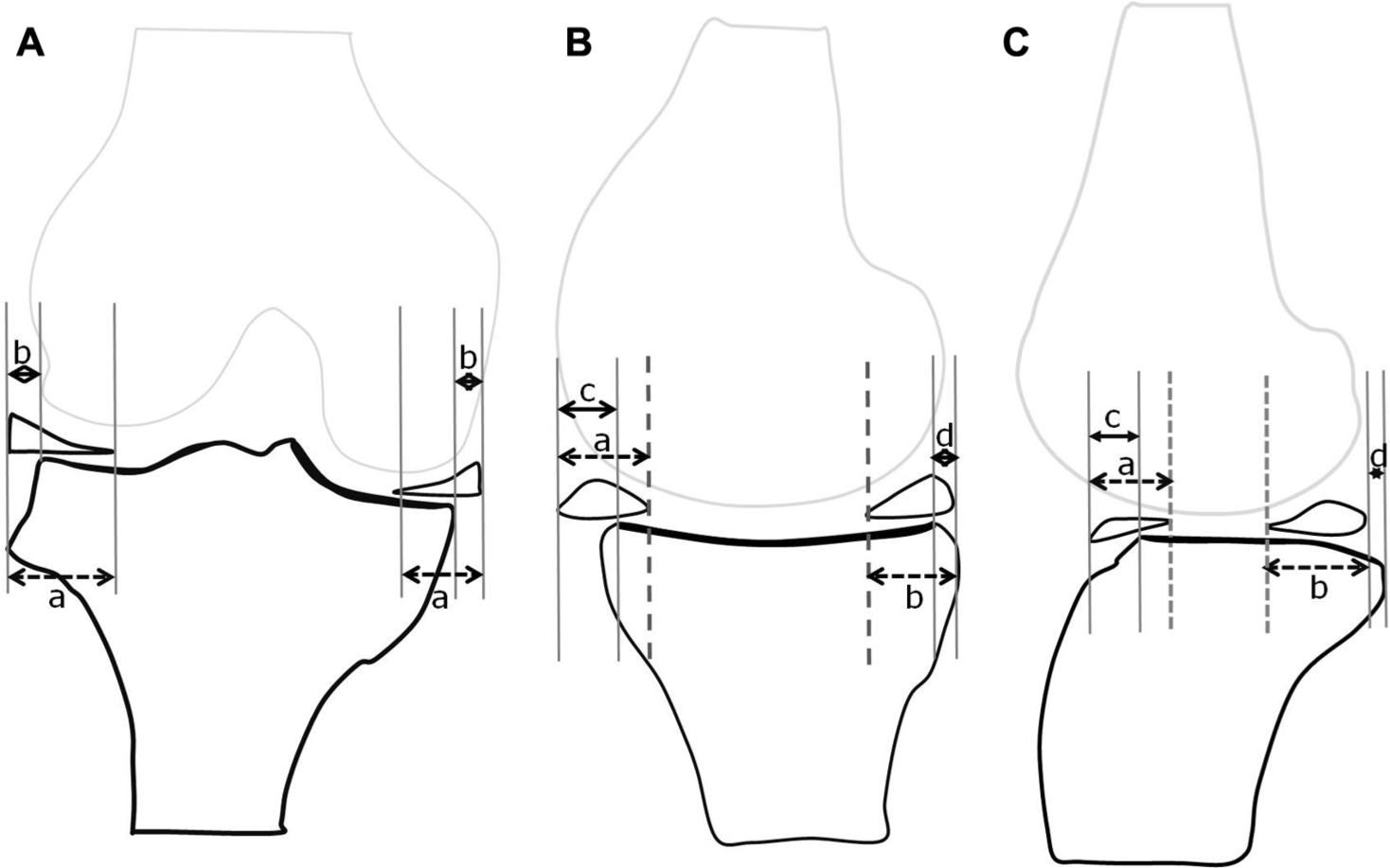
Schematic diagram for measurements of extrusion on magnetic resonance imaging. (A) In the coronal plane, absolute extrusion was measured as the distance between the outer edge of the articular cartilage of the tibial plateau and the outer edge of the transplanted meniscus allograft. The relative percentage of extrusion (RPE) was the percentage of the width of extrusion relative to the width of the entire meniscus (b/a × 100). Similarly, the extruded or intruded transplanted meniscus from the articular margin in the sagittal plane on the (B) medial and (C) lateral sides was defined as sagittal extrusion or intrusion of the anterior or posterior horn. The sagittal RPE was determined by dividing the width of extrusion by the width of the entire meniscus in the sagittal plane (c/a × 100 or d/b × 100). Extrusion was expressed as a positive value and intrusion as a negative value.
The extrusion of transplanted allografts on sagittal MRI was evaluated relative to the anterior and posterior horns. Anterior extrusion of the graft in the sagittal plane was defined as the maximum distance from the anterior articular cartilage margin to the anterior border of the anterior horn of the transplanted meniscus (anterior cartilage meniscus distance [ACMD]). Likewise, posterior extrusion of the graft in the sagittal plane was defined as the distance from the posterior articular cartilage margin to the posterior border of the posterior horn of the transplanted meniscus (posterior cartilage meniscus distance [PCMD]). Relative ACMD and PCMD were calculated as absolute extrusion divided by the width of the entire meniscus in the sagittal plane (Figure 1, B and C). Extrusion of the ACMD or PCMD outside the anterior or posterior border of the articular cartilage was expressed as positive values, whereas extrusion inside these borders was expressed as negative values.
Scans were independently evaluated by 2 orthopaedic surgeons. Each patient was evaluated by MRI 2 days after surgery and 2 weeks later. The measurements taken by the 2 surgeons were averaged.
Statistical Analysis
The primary study endpoint was to determine whether absolute graft extrusion in the coronal plane differed in the medial and lateral MAT groups. To determine the sample size required to detect differences in absolute extrusion between these 2 groups, α was set at .05, and power was set at 0.8. The SD for absolute extrusion was 2.8 for 5 patients who underwent medial MAT and 2.3 for 5 patients who underwent lateral MAT. A sample size of 45 knees per group was required to detect between-group differences in absolute extrusion. The current study involved 51 knees that underwent medial MAT and 84 that underwent lateral MAT. Overall, the power of the present study was 0.894 for detecting a significant between-group difference in absolute extrusion.
The reliability of measurements of graft extrusion on coronal and sagittal MRI was assessed by calculating intraclass correlation coefficients (ICCs), which quantify the proportion of differences due to measurement variability. The ICC can range from 0 to 1, with >0.75 representing good agreement and <0.40 representing poor agreement. In the present study, interobserver reliability ranged from 0.745 to 0.928, and intraobserver reliability ranged from 0.758 to 0.931, indicating good reliability for measurements of graft extrusion on MRI.
The MRI measurements in the 2 groups were compared using Student t tests. The demographic characteristics and radiographic measurements of the 2 groups were compared using Student t tests or Mann-Whitney U tests for continuous variables and χ2 or Fisher exact tests for categorical variables. Correlations between the amount of graft extrusion on coronal and sagittal MRI and between extrusion and postoperative Lysholm scores were assessed using Pearson correlation analysis. All statistical analyses were performed using SPSS Statistics version 20 software (IBM Corp). A P value <.05 was considered statistically significant.
Results
Clinical Outcomes and Coronal and Sagittal Extrusion on MRI
The mean ages of the patients in the medial and lateral MAT groups were 35 years (range, 20-51 years) and 34 years (range, 15-54 years), respectively. The mean follow-up periods were 26 months (range, 24-40 months) in the medial MAT group and 25 months (range, 24-36 months) in the lateral MAT group.
Mean Lysholm scores were significantly higher 2 years after surgery than preoperatively in both the medial (91.4 vs 73.5, respectively; P < .001) and lateral (90.7 vs 71.9, respectively; P < .001) MAT groups. After 2 years, none of these patients had symptoms requiring a secondary operation. Graft extrusions on coronal MRI were significantly greater in the medial than in the lateral MAT group, measured as both mean absolute extrusion (4.3 vs 2.7 mm, respectively; P < .001) and RPE (39% vs 21%, respectively; P < .001) (Figure 2). In the sagittal plane, mean absolute and relative ACMDs and PCMDs were significantly greater in the medial than in the lateral MAT group (P < .001 each) (Table 2). In both the medial and lateral MAT groups, the mean absolute and relative ACMDs were significantly greater than the mean absolute and relative PCMDs (P < .001 each) (Figure 3). Graft extrusion >3 mm in the coronal plane was significantly more frequent in the medial (40/51, 78%) than in the lateral (29/84, 35%) MAT group. In the sagittal plane, the frequencies of ACMDs (72% vs 39%, respectively) and PCMDs (23% vs 4%, respectively) >3 mm were also significantly greater in the medial than in the lateral MAT group (Table 3).
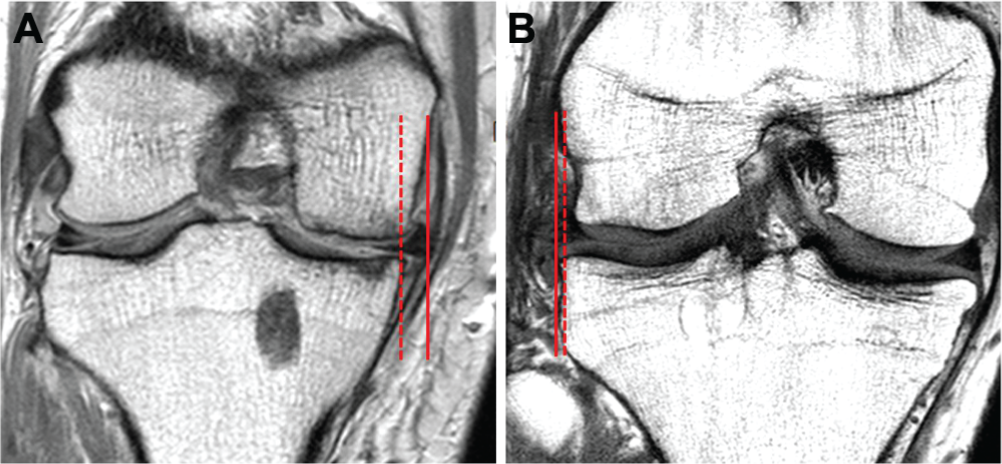
Extrusion of the transplanted meniscus on coronal magnetic resonance imaging was greater after medial (A) than lateral (B) meniscus allograft transplantation.
Extrusion on Magnetic Resonance Imaging a
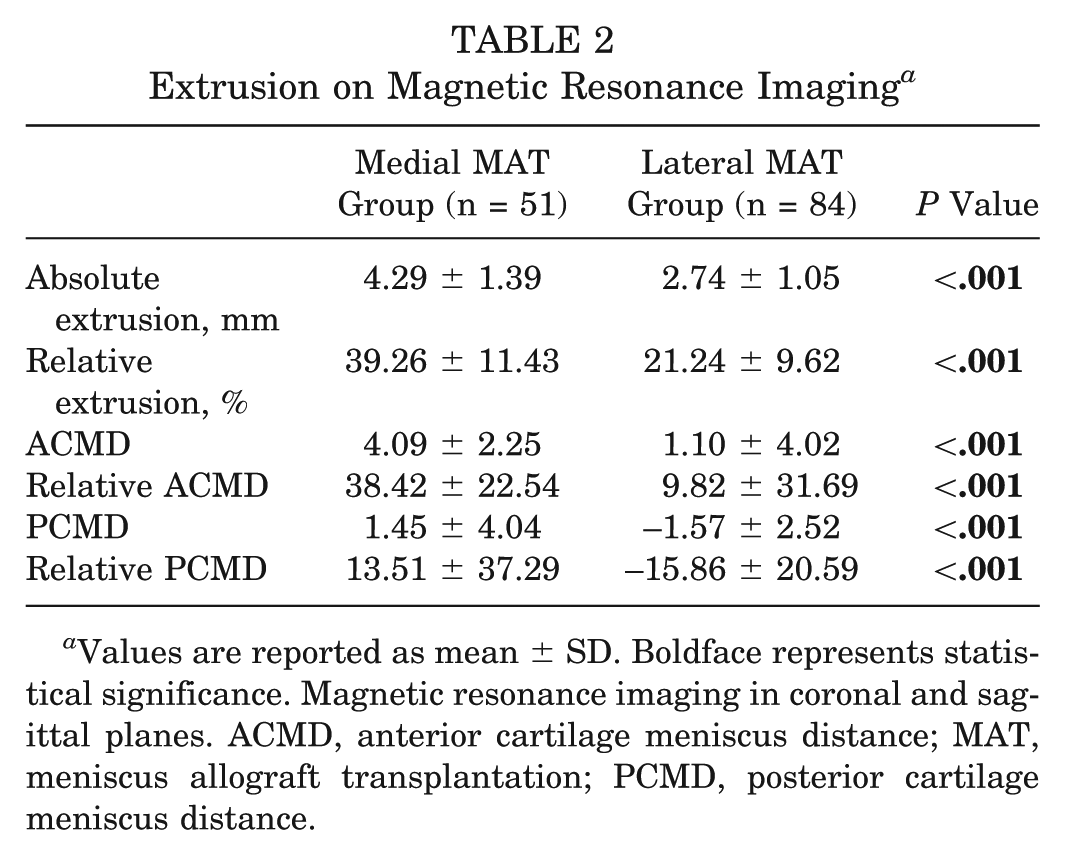
Values are reported as mean ± SD. Boldface represents statistical significance. Magnetic resonance imaging in coronal and sagittal planes. ACMD, anterior cartilage meniscus distance; MAT, meniscus allograft transplantation; PCMD, posterior cartilage meniscus distance.
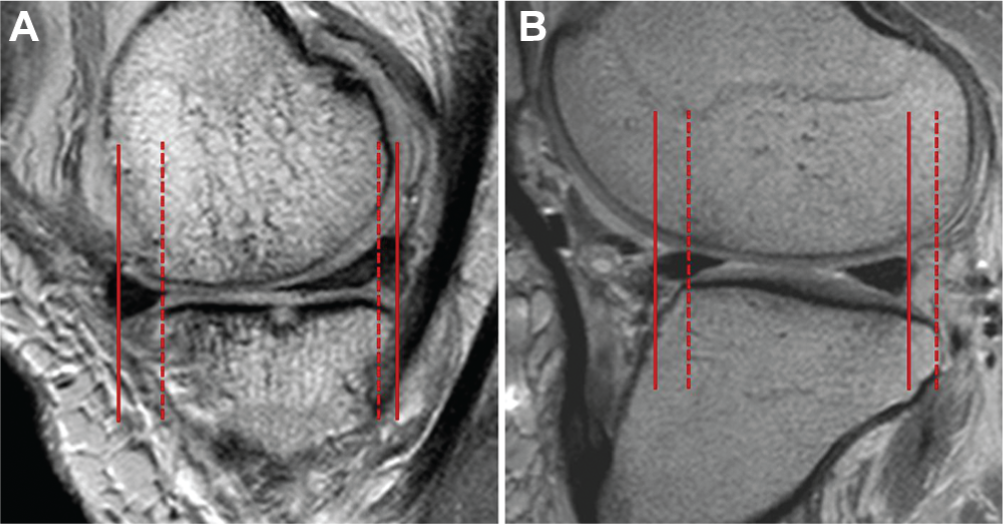
Extrusion of the transplanted meniscus on sagittal magnetic resonance imaging was greater after medial (A) than lateral (B) meniscus allograft transplantation (MAT) at both the anterior and posterior horns. Note that extrusion of the anterior horn was greater than that of the posterior horn after both medial and lateral MAT. Lateral MAT showed intrusion rather than extrusion at the posterior horn.
Rate of Major Extrusion on Magnetic Resonance Imaging a
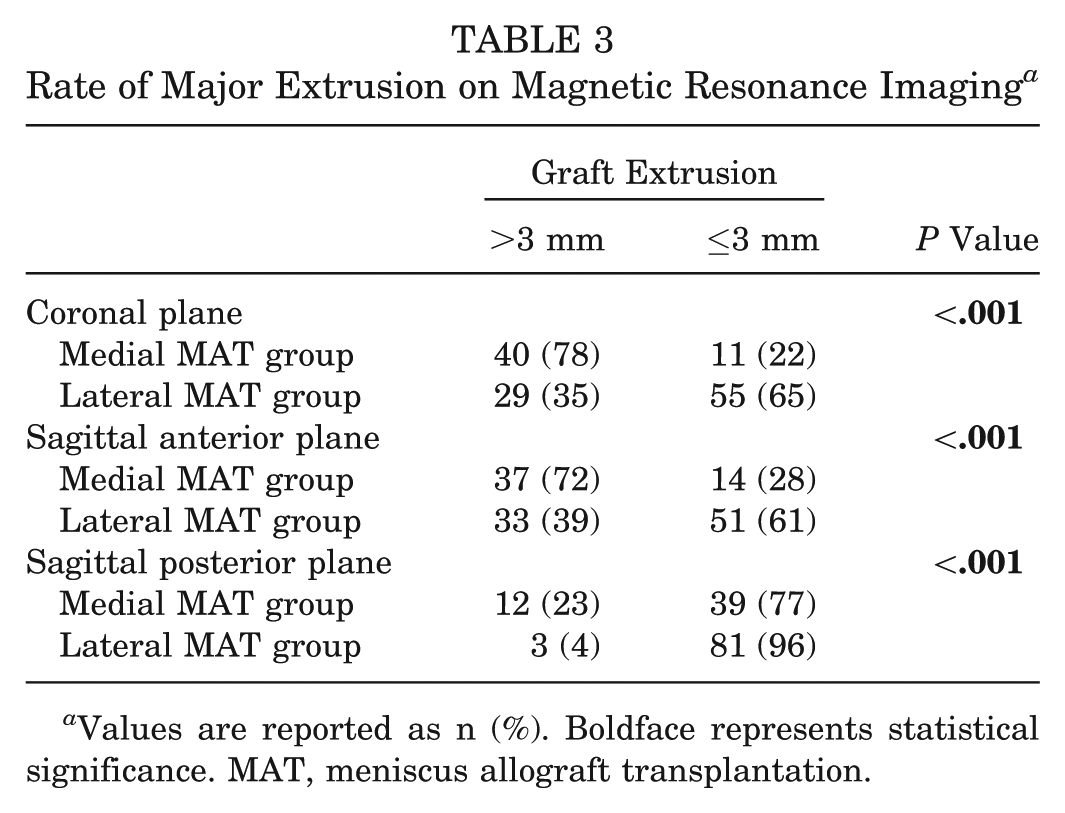
Values are reported as n (%). Boldface represents statistical significance. MAT, meniscus allograft transplantation.
Correlation Studies
In the medial MAT group, none of the parameters measured on MRI, including absolute and relative ACMDs and PCMDs, was correlated with absolute extrusion and RPE in the coronal plane. In the lateral MAT group, absolute and relative ACMDs showed positive correlations, and absolute and relative PCMDs showed negative correlations, with absolute extrusion and RPE in the coronal plane (Table 4). Assessments of clinical outcomes after surgery showed no correlations between coronal and sagittal extrusion parameters and postoperative Lysholm scores in either the medial or lateral MAT group (Table 5).
Correlations Between Absolute Extrusion and RPE on Magnetic Resonance Imaging and Clinical Outcomes a
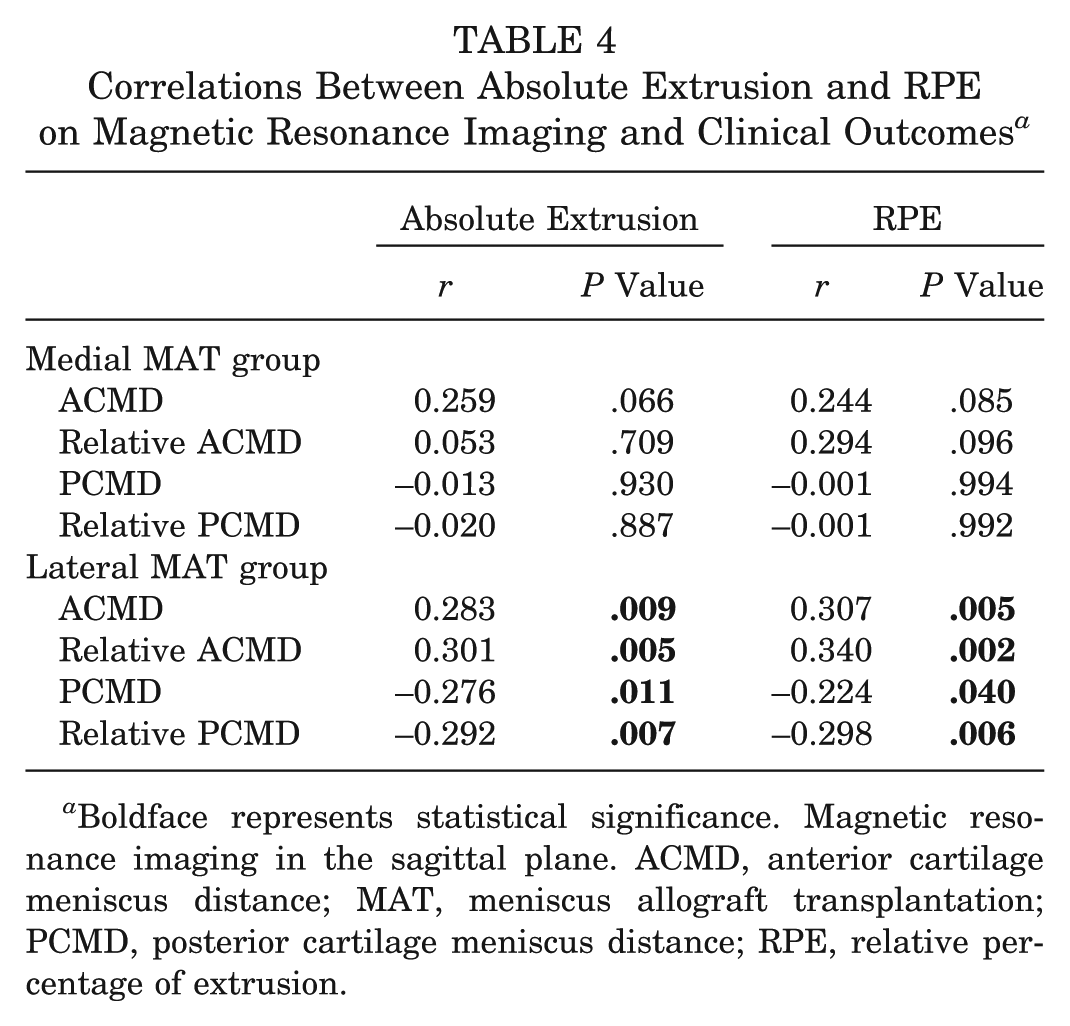
Boldface represents statistical significance. Magnetic resonance imaging in the sagittal plane. ACMD, anterior cartilage meniscus distance; MAT, meniscus allograft transplantation; PCMD, posterior cartilage meniscus distance; RPE, relative percentage of extrusion.
Correlations Between Postoperative Lysholm Scores and Extrusion on Magnetic Resonance Imaging a
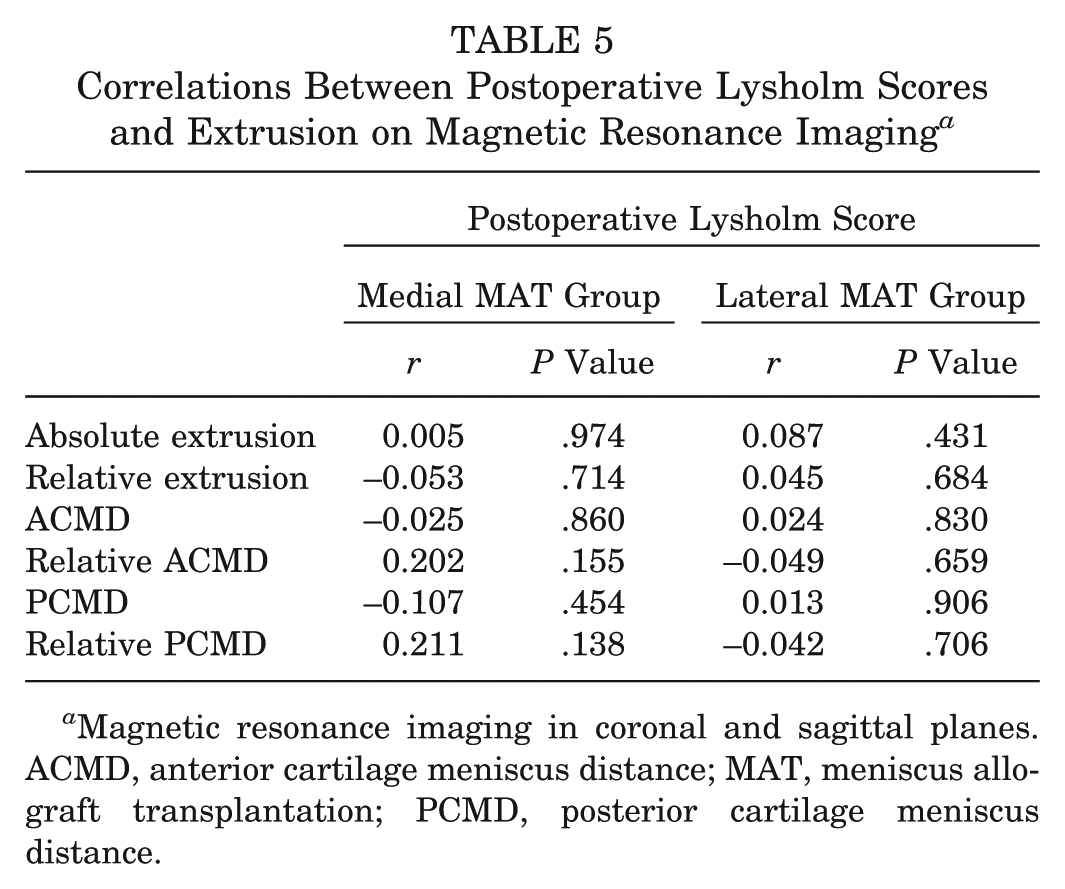
Magnetic resonance imaging in coronal and sagittal planes. ACMD, anterior cartilage meniscus distance; MAT, meniscus allograft transplantation; PCMD, posterior cartilage meniscus distance.
Discussion
The present study compared the extrusion of transplanted medial and lateral grafts, as assessed by immediate postoperative coronal and sagittal MRI. The study found that patients who underwent medial MAT had larger graft extrusion and a higher proportion of major (>3 mm) graft extrusion in both the coronal and sagittal planes than patients who underwent lateral MAT.
Although meniscus extrusion after MAT has been reported in previous studies, it was unclear whether the extent of extrusion was greater on the medial or lateral side. For example, a recent study comparing graft extrusion after 73 lateral MATs and 26 medial MATs found that the mean absolute extrusions were 4.7 and 2.9 mm, respectively, indicating that transplanted lateral menisci extrude to a significantly greater extent than transplanted medial menisci. 9 That study hypothesized that the greater degree of graft extrusion on the lateral side may have been caused by looser anatomic capsular restraint of the lateral than of the medial meniscus, in that the capsular attachment on the popliteal hiatus was looser for the lateral than the medial meniscus. That study, however, contained too few patients who underwent medial MAT compared with lateral MAT and did not have sufficient statistical power to detect differences in graft extrusion between the 2 groups.
Other studies have reported greater graft extrusion on the medial than on the lateral side after MAT. For example, a comparison between 11 medial MATs and 24 lateral MATs reported mean extrusions of 2.6 and 1.7 mm, respectively. 24 That study, however, included small numbers of patients in both groups and therefore lacked statistical power to detect any between-group differences in graft extrusion. In addition, the primary endpoint of that study was not a comparison of graft extrusion. A comparison of the degree of graft extrusion after MAT with conventional allograft sizing according to Pollard et al 15 and with a modified method using allografts 5% smaller found that modified allograft sizing decreased the RPE after MAT. 7 Raw data on graft extrusion showed that the mean graft extrusion was greater on the medial than the lateral side (4.2 vs 3.7 mm, respectively), regardless of the graft sizing method used, in agreement with our results showing that graft extrusion tended to be greater after medial than lateral MAT. A comparison of morphological measures in healthy adult knees found that physiological extrusion was greater for the medial than for the lateral meniscus, as were mean and maximal meniscus thicknesses. 1 These findings suggest that the greater physiological extrusion of the medial than the lateral meniscus may have resulted from a greater overstuffing effect of the former caused by the greater thickness of the medial meniscus. Likewise, the tendency of greater graft extrusion after medial than lateral MAT in our study and previous studies may be because of the greater overstuffing of the inherently thicker medial allograft into a restricted joint space.
Previous studies8,13 of graft extrusion after MAT assessed extrusion only in the coronal plane of MRI. In the current study, we first demonstrated that both the absolute amount of graft extrusion and the proportion of knees with major (>3 mm) graft extrusion were greater in the medial than in the lateral MAT group both in the coronal and sagittal planes of MRI. Views in the sagittal plane showed that the anterior horn of medial allografts extruded more anteriorly and that the posterior horn of medial allografts extruded more posteriorly than did those of lateral allografts. Furthermore, the percentage of knees showing major extrusion (>3 mm) of the anterior and posterior horns in the sagittal plane was much higher in the medial than in the lateral MAT group. The anterior horn position of medial MAT could usually be determined with the naked eye, whereas the posterior horn position was generally determined arthroscopically. In contrast, the positions of both horns during lateral MAT are determined when creating the bony trough. These separate tunnel-creating processes for anterior and posterior horn bone plugs during medial MAT may result in tunnel locations being more prone to erroneous nonanatomic positioning than observed during lateral MAT. The more complex surgical techniques required for medial than lateral MAT may result in greater extrusion during medial than lateral MAT, especially in the sagittal plane.
Interestingly, in both the medial and lateral MAT groups, the amount of extrusion and the incidence of major extrusion (>3 mm) were greater for the anterior than posterior horn. In the lateral MAT group, the posterior horn intruded more anteriorly from the posterior tibial plateau’s articular margin than did the posterior horn, as well as extruded more posteriorly, with the incidence of major extrusion of the posterior horn being only 4%. These findings suggest that the anterior horn may be more susceptible to graft extrusion than the posterior horn after both medial and lateral MAT. The anterior horn position of the bony tunnel for an anterior horn plug in medial MAT is usually determined by the naked eye. Similarly, in lateral MAT, the anterior horn location can be determined by the naked eye from the starting point of the guide wire used to ream the bony trough. Determining the anterior horn position with the naked eye may introduce errors because soft tissue such as patellar fat pads can obstruct the view of the anterior horn. This may explain, at least in part, our finding of greater graft extrusion of the anterior than the posterior horn after both medial and lateral MAT.
This study had several limitations. The sample size was relatively small, although it had acceptable statistical power for the primary endpoint (ie, difference in absolute extrusion between the medial and lateral MAT groups). Another limitation was that the accuracy of anterior and posterior horn extrusion or intrusion was lower in the sagittal than in the coronal plane, as determining the margins of the anterior and posterior horns on sagittal MRI is difficult because of a partial volume effect in which meniscus tissue may overlap with the anterior and posterior margins of the tibial plateau. 6 However, the reliabilities of parameters measured on MRI were satisfactory in our study. Although we did not observe any correlation between graft extrusion and clinical scores, the follow-up period may have been too short to show clinical outcomes of graft extrusion. Nevertheless, until graft extrusion is shown to affect long-term clinical outcomes, the best size-matched graft should be transplanted and extrusion minimized as much as possible. Overextrusion may result in mechanical malfunction and unfavorable long-term survival of the transplanted graft, as shown in previous biomechanical studies. 24 Finally, our cutoff value (>3 mm) for major sagittal extrusion at the anterior and posterior horns was to some degree arbitrary. However, we first attempted to measure sagittal extrusion, and all previous studies assessing coronal extrusion of the meniscus or transplanted meniscus allograft have used a cutoff value of 3 mm.2,7,22
Conclusion
The amount of graft extrusion and the incidence of major graft extrusion after MAT were greater on the medial than on the lateral side, as determined by MRI in both the coronal and sagittal planes. In the sagittal plane, graft extrusions were larger and more frequent for the anterior than the posterior horn for both medial and lateral MAT. However, graft extrusion did not correlate with early clinical outcomes in patients undergoing medial and lateral MAT.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study (2012-0001308) was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology. This work was also supported by Korea University grants (K1326281).