
Abstract
Background:
Intratendinous tears of the rotator cuff are rare, and little has been written about them.
Purpose:
To investigate the prevalence and clinical and radiological outcomes of arthroscopically confirmed intratendinous tears treated with transtendon suture bridge repair.
Study Design:
Case series; Level of evidence, 4.
Methods:
Included in the study were 33 patients (16 male, 17 female; mean age, 53.4 years) with arthroscopically confirmed intratendinous tears treated with transtendon suture bridge repair from March 2006 to July 2012. A history of trauma was found in 10 cases (30.3%). The dominant arm was involved in 26 cases (78.8%). The mean follow-up duration was 56 months. Preoperatively, a thorough physical examination was performed; at final follow-up, shoulder range of motion (ROM) in forward flexion, abduction, external rotation (ER) at the side, and internal rotation (IR) at the back was noted, and clinical outcomes (American Shoulder and Elbow Surgeons [ASES] score; University of California, Los Angeles [UCLA] score; visual analog scale [VAS] for pain; and Simple Shoulder Test [SST]) were recorded and compared with the preoperative data. Postoperative magnetic resonance imaging (MRI) was performed at 6 months to investigate rotator cuff healing status and repair integrity.
Results:
The prevalence of arthroscopically confirmed intratendinous tears was 4.7% among all arthroscopically treated partial-thickness rotator cuff tears. Impingement signs were positive in most of the patients (positive Hawkins-Kennedy test result in 78.8%, positive Neer sign in 66.7%, and either positive Hawkins-Kennedy test result or Neer sign in 84.8%). At final follow-up, mean ASES, UCLA, VAS, and SST scores improved significantly from a preoperative mean of 51.4, 18.9, 6.0, and 5.4, respectively, to a postoperative mean of 90.6, 32.9, 1.4, and 10.8, respectively (P < .001). According to the UCLA rating scale, outcomes were excellent in 17, good in 13, and fair in 3 cases. Shoulder ROM in forward flexion, abduction, ER at the side, and IR at the back improved from a preoperative mean of 135°, 129°, 25°, and L2, respectively, to a postoperative mean of 161°, 160°, 29°, and T10, respectively (P < .001 for all except ER). As per the Sugaya classification, on postoperative MRI, type I healing status was found in 10 (30.3%), type II in 18 (54.5%), and type III in 2 (6.1%) cases. None of the patients showed any evidence of retears.
Conclusion:
Transtendon suture bridge repair yielded satisfactory clinical and radiological outcomes in patients with intratendinous rotator cuff tears.
Partial-thickness rotator cuff tears (PTRCTs) have been of increasing interest because of recent developments in diagnostic modalities and arthroscopic surgical techniques. Ellman 8 categorized these tears based on their location in articular, bursal, and intratendinous areas and classified them as grade I (<3 mm), grade II (3-6 mm), or grade III (>6 mm). 9 Approximately 5% to 10% of patients with shoulder pain have a symptomatic PTRCT. 41 In spite of various cadaveric and radiological studies, the exact incidence of PTRCTs is not known. From a cadaveric study of supraspinatus tendons in 306 shoulders, Lohr and Uhthoff 27 found a prevalence of 19% for full-thickness tears and 32% for partial-thickness tears. Several clinical studies have reported that articular-sided tears are 2 to 3 times more common than bursal-sided tears, 37 and cadaveric studies have noted that intratendinous tears are actually more common than bursal- or articular-sided tears. In a group of 249 cadaveric specimens, Yamanaka and Fukuda 49 reported a prevalence of supraspinatus partial-thickness and full-thickness tears of 13% and 7%, respectively. The prevalence of intratendinous tears was 7.2%, compared with the prevalence of bursal-sided tears of 2.4% and articular-sided tears of 3.6%. Other studies have reported the prevalence to be 7.9% to 25.6%.21,48
The diagnosis and differentiation of PTRCTs from full-thickness rotator cuff tears based on clinical examinations are often challenging and difficult tasks.3,41 The development of various magnetic resonance imaging (MRI) techniques, including sequence alteration, contrast arthrography, and differential arm positioning (abduction and external rotation [ER]), has improved the accuracy of diagnosing rotator cuff tears.23,32,45 Magnetic resonance imaging has remarkably variable sensitivity, ranging from 38% to 93%, but also has good specificity (70%-97%) when it is used to diagnose PTRCTs. 10 On MRI, the diagnosis of PTRCTs is based on the presence of increased signaling in the rotator cuff without discontinuity on T1-weighted images. This finding corresponds to increased signaling noted on T2-weighted sequences with the identification of a focal defect on either the bursal or articular surfaces or within the tendon substance.12,30,38 Ultrasonography and MRI provide almost similar accuracy rates for the diagnosis of PTRCTs. 44 The discrepancy between the prevalence of intratendinous tears found in cadaveric and clinical studies may be because intratendinous tears are more difficult to diagnose with arthroscopic surgery, MRI, or ultrasound than are bursal- or articular-sided tears. Because of this diagnostic dilemma, only a few publications can be found on intratendinous rotator cuff tears.26,46
The purpose of our study was to (1) investigate the prevalence of intratendinous rotator cuff tears in a consecutive series of patients and (2) report the clinical and radiological outcomes of intratendinous rotator cuff tears with the arthroscopic transtendon suture bridge repair technique at midterm follow-up. The hypothesis was that arthroscopic transtendon suture bridge repair of intratendinous rotator cuff tears in symptomatic patients will be helpful in relieving patients’ pain and disability.
Materials and Methods
Institutional review board approval was obtained before patients were enrolled in the study. From March 2006 to July 2012, a total of 2417 shoulder arthroscopic surgeries for various shoulder disorders were performed at a single institution. We recruited these participants from a patient population undergoing shoulder arthroscopic procedures at a university clinic, where approximately 400 to 500 shoulder arthroscopic procedures are performed yearly. During the study period, there were 296 cases of full-thickness rotator cuff tears and 765 cases of PTRCTs. Of these 762 cases, a total of 36 patients were found to have arthroscopically confirmed intratendinous tears. The prevalence of articular, bursal, both articular and bursal, and intratendinous PTRCTs was 321 (42%), 227 (30%), 178 (23%), and 36 (5%) cases, respectively.
Inclusion criteria were the failure of nonoperative treatment in patients with shoulder pain or discomfort for at least 6 months, preoperative MRI scans suggestive of intratendinous high signal intensity on T2-weighted images, arthroscopically confirmed intratendinous rotator cuff tears, and at least 24 months’ postoperative follow-up. A radiologist specializing in musculoskeletal disorders reported all MRI scans as showing intratendinous tears. Nonoperative treatment included activity modification, rest, local heat or cold application, nonsteroidal anti-inflammatory medications, gentle physical exercises, and administration of a subacromial corticosteroid injection (a mixture of 40 mg triamcinolone acetate and 3 mL lignocaine 2%). Exclusion criteria were PTRCTs other than intratendinous tears, any associated lesions such as a subscapularis tear, acromioclavicular arthritis, a Bankart lesion, a superior labral anterior-posterior lesion, a biceps injury (fraying or tearing), or an intratendinous tear extending into the articular or bursal layer of the rotator cuff. Despite MRI findings of an intratendinous tear, 3 cases were excluded because no arthroscopic confirmation (bubble sign and arthroscopic probing of an intratendinous rotator cuff defect) was made afterward. Of 36 arthroscopically confirmed intratendinous tears, 33 patients met the inclusion criteria. Two patients were lost to follow-up, and 1 patient had fewer than 24 months of follow-up.
Of the 33 included patients, 16 were male and 17 were female, with a mean age of 53.4 ± 9.1 years (range, 32-72 years). A history of trauma was found in 10 cases (30.3%), and a history of heavy weight lifting was found in 4 cases (12.1%). The dominant arm was involved in 26 cases (78.8%). The mean follow-up period was 56 months (range, 26-72 months). Fifteen of the patients regularly participated in a sports activity such as tennis, badminton, golf, or recreational sports at a gymnasium. We also evaluated the acromion type in these patients: type 1 was present in 8 cases, type 2 in 23 cases, and type 3 in 2 cases.
All patients underwent a thorough physical examination. Preoperatively, shoulder range of motion (ROM) in forward flexion, abduction, ER at the side, and internal rotation (IR) at the back was measured with a goniometer by the senior author (J.-H.J.). Clinical outcomes from the American Shoulder and Elbow Surgeons (ASES) score; University of California, Los Angeles (UCLA) score; visual analog scale (VAS) for pain; and Simple Shoulder Test (SST) were noted. All patients underwent a preoperative imaging assessment. Shoulder radiographs in anteroposterior, axillary, and supraspinatus outlet views were obtained in all patients. An MRI assessment was performed using a 3.0-T MRI system (Siemens Somatom Plus S scanner, Siemens Medical Systems). All MRI scans showed a definitive presence of increased signal intensity in the rotator cuff without discontinuity on T1-weighted images, with a concomitant finding of increased signaling on T2-weighted sequences, with a focal defect within the tendon substance and without any defect on the articular or bursal side of the rotator cuff. A pure intratendinous tear was confirmed in all patients with an arthroscopic examination using the “bubble sign,” 26 with concomitant abnormal changes on the bursal surface of the rotator cuff such as fraying, bulging, depression, softening, or erosion.
The mean duration between the initiation of nonoperative therapy and surgery was 7.8 months (range, 6-12 months). All intratendinous tears were repaired with the arthroscopic transtendon suture bridge repair technique. Some patients showed stiffness due to shoulder pain of a long duration, and we performed intraoperative manipulation and arthroscopic capsular release. Postoperatively, shoulder radiographs in anteroposterior, axillary, and supraspinatus outlet views were obtained. Patients were followed up regularly in the outpatient clinic. At final follow-up, shoulder ROM in forward flexion, abduction, ER at the side, and IR at the back was measured with a goniometer calibrated at 1° increments by the same senior author. The clinical outcomes from the ASES, UCLA, VAS, and SST were noted. A UCLA score of 34-35 points was considered excellent, 28-33 points good, 21-27 points fair, and 0-20 points poor. All patients underwent a follow-up MRI evaluation at a postoperative 6 months to determine rotator cuff integrity and healing status of the repaired tendon. 22 We classified rotator cuff repair status as per the Sugaya classification. 42
Surgical Procedure
Under general anesthesia, the patient was placed in the lateral decubitus position with approximately 10 lb of lateral arm traction. The arthroscope was inserted into the glenohumeral joint through a standard posterior portal. An anterosuperior portal was created just above the biceps tendon for easy anchor insertion. Then, a diagnostic intra-articular examination was performed. In all cases, there was no articular-sided rotator cuff tear (Figure 1A). After that, the arthroscope was inserted into the subacromial space. Thorough bursectomy was performed to improve visualization. All cases demonstrated abnormal changes in the bursal surface of the rotator cuff such as fraying, bulging, depression, softening, or erosion but without any obvious bursal-sided rotator cuff tears. Then, we palpated this abnormal area of the rotator cuff with a hooked probe (Figure 1B). Compared with the adjacent normal and firm rotator cuff insertion site, this part of the rotator cuff appeared slack. Then, to confirm the presence of an interstitial tear, a “saline test” was performed. 26 Through the conventional lateral portal, an 18-gauge spinal needle attached to a 5-mL syringe filled with normal saline was inserted into the center of the suspected rotator cuff lesion (Figure 2A). As we injected saline into the suspected rotator cuff lesion, we noticed expansion within the rotator cuff tendon without any resistance (Figure 2B). This “saline injection and bubble sign” was a confirmatory test for palpable discontinuity in the rotator cuff tissue. This is in contrast to the adjacent normal rotator cuff tissue, where an attempt to inject saline was not possible because of significant resistance offered by the normal rotator cuff tissue. Through bursal surface erosion of the rotator cuff, we made a small hole using a hooked probe and inserted the probe into the substance of the rotator cuff (Figure 1C). In all cases, we found the probe passing easily within the rotator cuff substance, and thus, the presence of an intratendinous tear was confirmed. We confirmed the anterior and posterior extent of the tear with the probe. Before inserting the anchor, we placed No. 2 Ethibond (Ethicon) suture through the tendon to elevate the tear site for easier anchor insertion and better visualization. We inserted an 18-gauge spinal needle through the anterior and posterior tear margins, through which No. 2.0 nylon was placed and used to pass the No. 2 Ethibond suture. Again, we inserted the arthroscope into the glenohumeral joint to exclude any articular-sided tear in that area (between the anterior and posterior margins of the intratendinous tear, indicated by No. 2 Ethibond suture). After excluding the presence of an articular-sided tear, in the middle of the tear, we inserted a 4.5-mm metal anchor (Twinfix Ti suture anchor, Smith & Nephew) double loaded with No. 2 Ultrabraid (Teleflex Medical) suture into the anterosuperior portal; thus, damage to the intact articular and bursal sides of the rotator cuff could be minimized (Figure 1D). This anchor was inserted into the articular margin under the intratendinous tear and was able to damage articular cartilage a little. Yet, these threads were not located in the articular surface but at the top of the anchor, so that the intra-articular footprint of the rotator cuff was well restored. Then, all sutures from the suture anchor were retrieved through the anterior portal. As per the conventional transtendon rotator cuff repair technique, we passed all suture threads through the rotator cuff tendon and out through the skin using a suture shuttle relay (Figure 2B). Subsequently, the arthroscope was inserted into the subacromial space, and medial row repair was completed. Then, lateral row anchors were inserted (Footprint anchor, Smith & Nephew), thus sealing and compressing the intratendinous tear (Figure 1E). Standard acromioplasty was performed to complete the procedure. Finally, we confirmed the intra-articular status of the repaired tendon (Figure 1F). Also see the online Video Supplement.
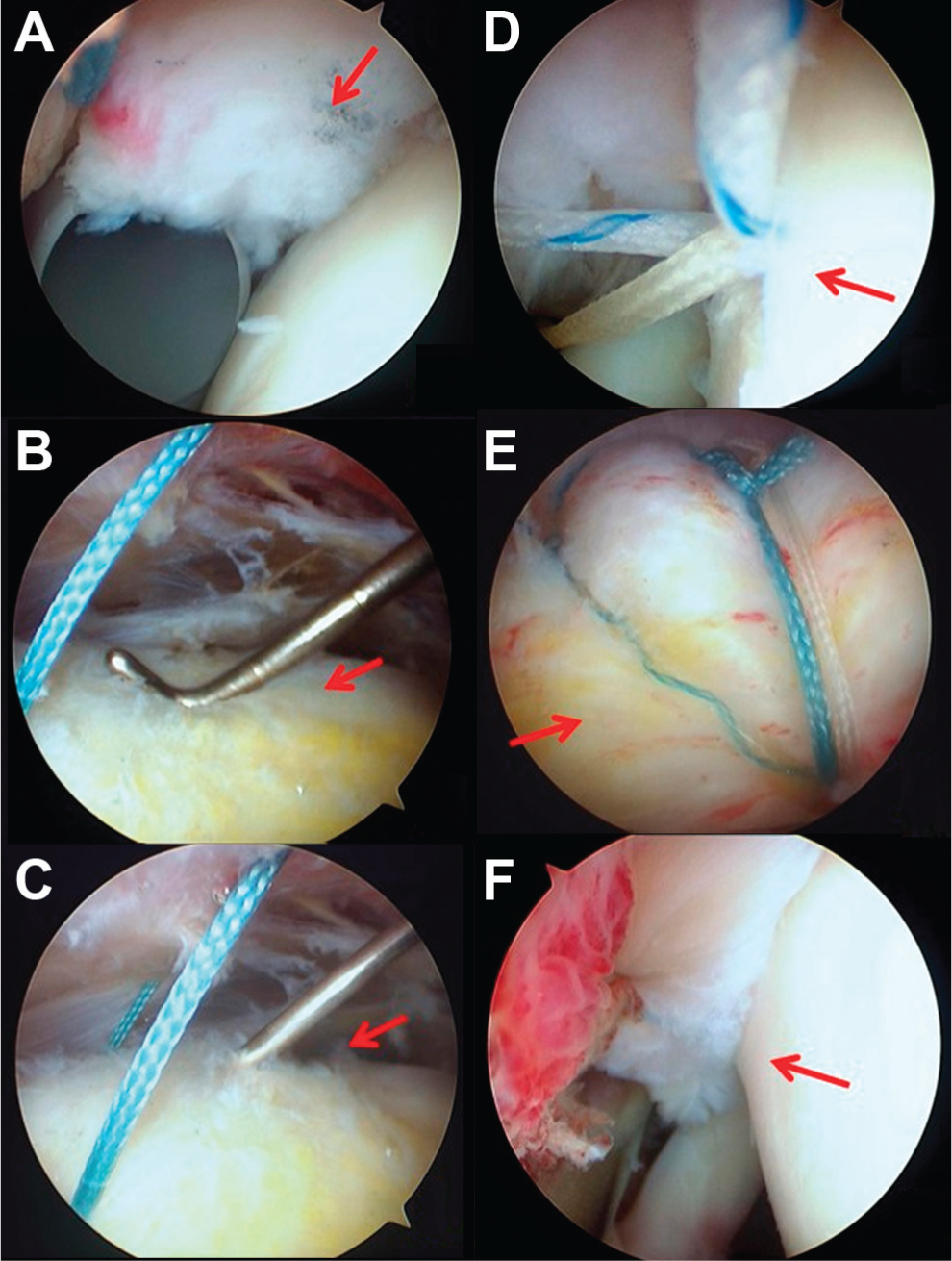
Arthroscopic findings. The arthroscope was inserted into the glenohumeral joint through the posterior portal, and the conventional anterior portal was used as working portal. (A) The arthroscopic view confirmed no articular-sided rotator cuff tear (arrow). (B) the suspected cuff lesion (arrow) of the intratendinous tear was palpated using the probe. (C) A small hole was made using a hooked probe, and the probe was inserted in the substance of the rotator cuff (arrow). (D) After inserting suture anchor in the articular margin under the intratendinous tear (arrow), all threads from the anchor were passed through the cuff and out through the skin using a suture shuttle relay. (E) In the subacromial space, lateral row anchors were inserted, thus sealing and compressing the intratendinous tear (arrow). (F) Confirmation of the intra-articular status of the repaired tendon can be seen (arrow) after completion of medial and lateral row repair.
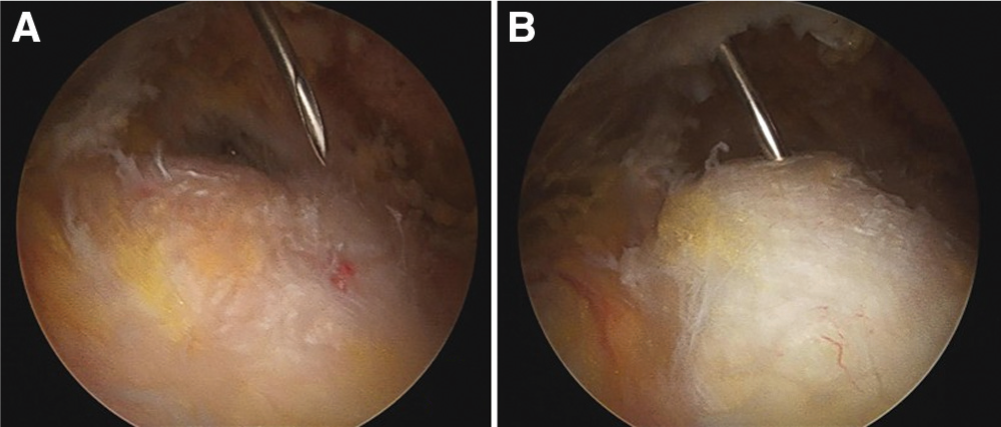
Arthroscopic findings. The “bubble sign,” which was used to diagnose the presence of an intratendinous tear. The patient is in the lateral decubitus position, and the arthroscope is in the posterior portal. (A) Through the lateral portal, an 18-gauge spinal needle is inserted, attached to a 5-mL syringe filled with normal saline. (B) The needle is inserted into the suspected lesion, and saline is injected inside the lesion. Ballooning of the rotator cuff can be seen at the tear site can be seen. Note the associated fraying in the bursal layer in this case.
Postoperatively, the patient was placed in a shoulder ultra–arm sling. From the second postoperative day, pendulum exercises were started. The sling was continued for 4 weeks, and after that, active ROM exercise was permitted, and posterior capsule stretching exercise to improve ROM was performed. At 12 weeks, strengthening exercises were initiated, with the goal of a progressive return to normal activities over the next 3 months.
Results
In our series, the prevalence of intratendinous tears was 4.7% (36/765) among arthroscopically confirmed PTRCTs. Although physical examination findings were nonspecific in the 33 cases studied, the Neer impingement sign 35 was positive in 22 (66.7%), the Hawkins-Kennedy test 19 result was positive in 26 (78.8%), the Jobe test 31 result was positive in 19 (57.6%), the O’Brien test 36 result was positive in 9 (27.3%), the Whipple test6,39 result was positive in 6 (18.2%), and the Speed test1,7 result was positive in 4 (12.1%) cases. Thus, test findings for impingement syndrome (ie, Neer sign and Hawkins-Kennedy test) were positive in most of the cases of intratendinous tears. Either the Neer sign or Hawkins-Kennedy test result was positive in 28 of 33 cases (84.8%), and both the Neer sign and Hawkins-Kennedy test result were positive in 20 of 33 cases (60.6%).
Clinical Outcomes
At final follow-up, mean ASES, UCLA, VAS, and SST scores improved significantly (P < .001 for all scores) (Table 1). According to the UCLA rating scale, the result was excellent in 17 cases, good in 13 cases, and fair in 3 cases. None of the patients showed poor results. Shoulder ROM in terms of forward flexion, abduction, ER at the side, and IR at the back also showed improvement (clinically significant for all movements, except for ER at the side [P = .28]) (Table 1). At final follow-up, most of the patients were satisfied with the treatment and showed good pain relief.
Preoperative and Postoperative Clinical Results After Treatment of Intratendinous Rotator Cuff Tears a
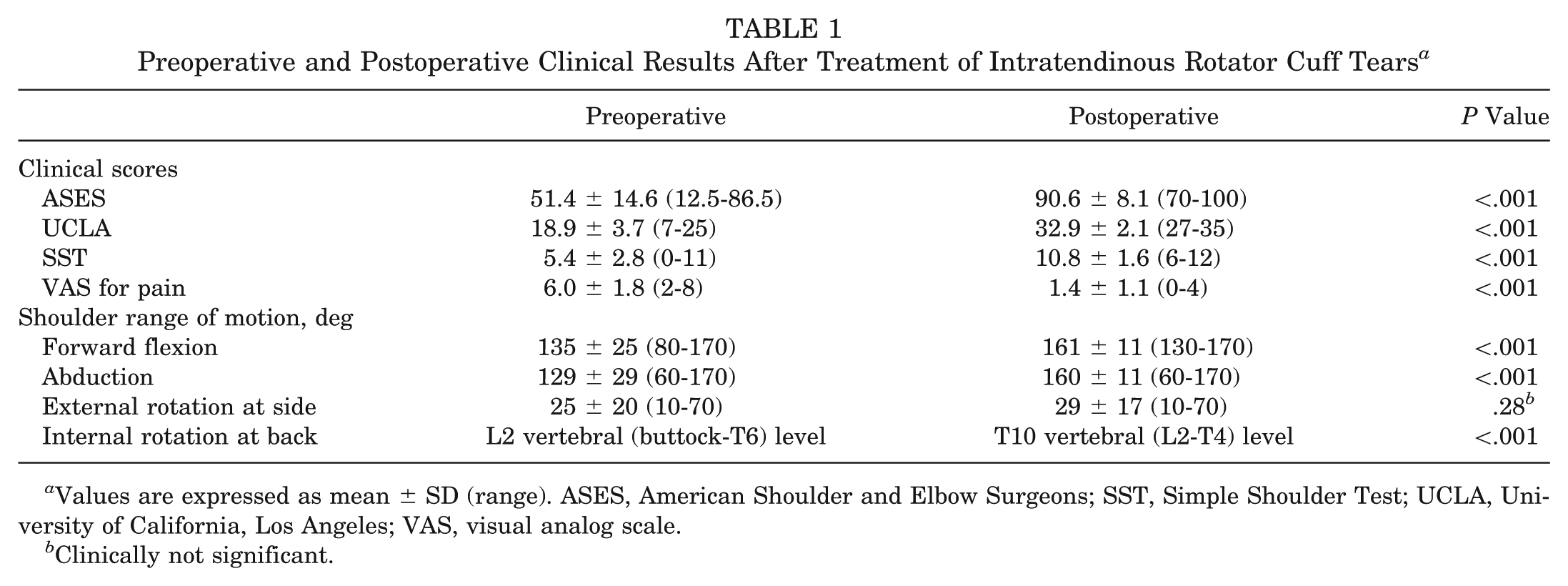
Values are expressed as mean ± SD (range). ASES, American Shoulder and Elbow Surgeons; SST, Simple Shoulder Test; UCLA, University of California, Los Angeles; VAS, visual analog scale.
Clinically not significant.
Radiological Outcomes
As per the Sugaya classification, on postoperative MRI, type I healing status was found in 10 (30.3%), type II healing status in 18 (54.5%), and type III healing status in 2 (6.1%) cases (Figure 3). None of the patients showed type IV or type V healing status or any evidence of retears.
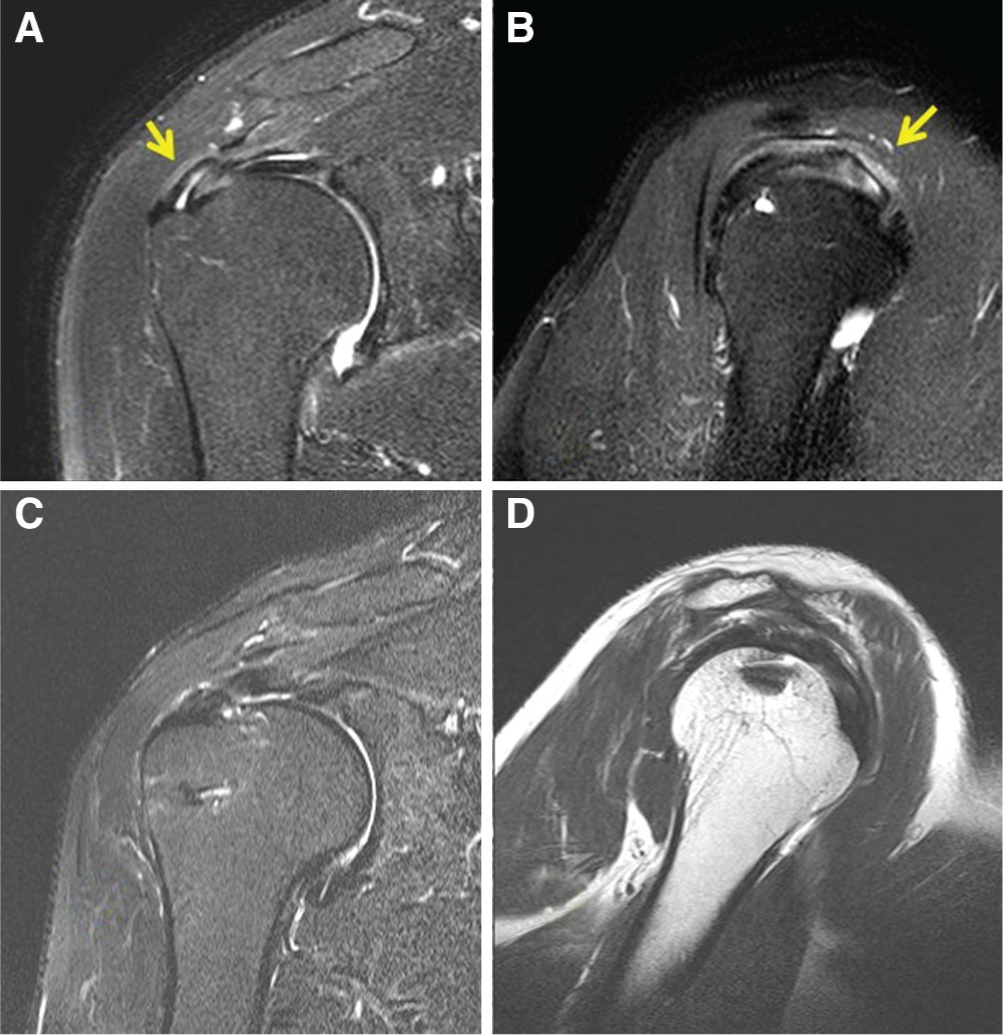
The right shoulder in a 55-year-old male patient. Preoperative magnetic resonance imaging (MRI): (A) oblique coronal T2-weighted image and (B) oblique sagittal T2-weighted image, showing the presence of an intratendinous tear (arrows). Postoperative MRI: (C) oblique coronal T2-weighted image and (D) oblique sagittal T1-weighted image, showing good repair integrity and Sugaya type II healing status.
Postoperative Complications
None of the patients showed any evidence of wound infections or any kind of wound complications. During the follow-up period, 3 (9%) patients developed postoperative shoulder stiffness. All patients were treated nonoperatively with physical therapy and oral medication. Of these 3 patients, in 2 patients, a subacromial corticosteroid injection was given at 3 months postoperatively, and in 1 patient, it was given at 4 months postoperatively. At final follow-up, these patients showed satisfactory clinical outcomes, without any further intervention, and they regained full ROM.
Discussion
The purpose of our study was to calculate the incidence and to evaluate midterm clinical and radiological outcomes of interstitial tears treated with arthroscopic transtendon suture bridge repair. At final follow-up, all patients showed satisfactory clinical and radiological outcomes. According to the UCLA rating scale, the result was excellent in 17 cases, good in 13 cases, and fair in 3 cases.
The incidence of PTRCTs varies in the literature. Among the 3 subtypes of PTRCTs, several studies have reported that articular-sided tears are 2 to 3 times more common than bursal-sided tears.12,18 The reported incidence of intratendinous tears is 7.9%, 21 13.6%, 15 and 25.6%. 48 Among 37 throwing athletes, Nakagawa et al 33 found that of 17 anterior rotator cuff tears, 6 cases had intratendinous tears, and the authors concluded that these concealed types of tears were representative lesions among anterior rotator cuff tears in athletes. During our study period, arthroscopically confirmed intratendinous tears were found in 4.7% of cases among all arthroscopically treated PTRCTs, whereas during their study period of approximately 10 years, Uchiyama et al 46 found an incidence of 3.2% for intratendinous tears. However, their incidence was noted among cases undergoing rotator cuff surgeries and not limited to PTRCTs.
Factors causing the development of PTRCTs have been classified as intrinsic, extrinsic, or traumatic. It has been suggested that intrinsic causes including age-related metabolic and vascular changes leading to degenerative tearing along with differential shear stress within the tendon may lead to the development of intratendinous tears.2,26 Up to now, there has not been a published biomechanical study that can lead us to understand the pathogenesis of intratendinous rotator cuff tears. In a biomechanical study, Yang et al 50 reported that there is an increased risk of tear propagation in the transverse plane with the increasing depth of tears, and they suggested that their study supports the repair of grade III (>50% thickness) tears. In another biomechanical study on PTRCTs, Mazzocca et al 29 also reported that articular-sided tendon strains increase consistently across the supraspinatus tendon with greater partial-thickness tears (>50%).
Intratendinous tears may be a rare cause of persistent shoulder pain. 14 The evaluation of a patient with shoulder pain and dysfunction begins with history taking and a thorough physical examination with a complete series of plain radiographs of the shoulder. Although these are rarely helpful in making a specific diagnosis of a PTRCT, they are necessary to exclude other causes of shoulder pain and to know the acromial shape. 11 In a study by Uchiyama et al, 46 a history of trauma was documented in 16 of 19 (84.2%) patients. They believed that trauma, whether overt, obscure, or gross, is one of the important factors producing symptoms in patients with intratendinous tears. Contrary to this finding, in our study, a history of trauma was noted in only 10 cases (30.3%), and a history of heavy weight lifting was found in 4 cases (12.1%). On physical assessment, Uchiyama et al 46 found that all of their 19 patients showed positive impingement signs. Almost similar to this study, we also found that impingement signs were positive in most of our patients, although not in all (Neer impingement sign was positive in 22/33 [66.7%] cases, and Hawkins-Kennedy test result was positive in 26/33 [78.8%] cases).
Historically, arthrography and bursography have been performed to diagnose articular- or bursal-sided rotator cuff tears, respectively, and in the literature, their accuracy rate ranges from 15% to 83%.16,18 With the advent of newer MRI techniques, including sequence alteration and differential arm positioning (abduction and ER), the accuracy with which rotator cuff tears are identified has increased.23,32,45 Recently, ultrasonographic examination has improved our ability to diagnose PTRCTs, and its reported sensitivity is 94% with 93% specificity. 47 It has also been suggested that high T2 signal intensity within the tendon is the criteria for intratendinous rotator cuff tears. 13 Yet, with tendon healing, the defect is replaced by granulation or scar tissue, which might be difficult to differentiate from tendon degeneration or tendinopathy by means of MRI.4,34 It has also been suggested that if intratendinous tears are associated with a failure in continuity and thereby lengthening of the tendon, such lengthening could become a key finding on MRI for partial tears and particularly for intratendinous tears. 10 In our series, with the use of a 3.0-T MRI machine, we were able to identify the presence of intratendinous tears in all our patients, especially on T2-weighted images.
To diagnose intratendinous tears arthroscopically, the “bubble sign” was proposed by Lo et al. 26 They injected a small amount of saline (<1 mL) into the proposed lesion site and found bulging expansion of the rotator cuff. They also suggested that along with this sign, a careful preoperative MRI evaluation, thorough arthroscopic examination to rule out any combined lesions, a “sliding” sensation while probing the lesion, and subjective impression of resistance to flow during injections are necessary. We used this sign to confirm the presence of an intratendinous tear in all patients, along with the presence of abnormalities on the bursal side of the rotator cuff such as fraying, bulging, depression, softening, or erosion. The color test was also proposed by Fukuda et al 17 to accurately localize articular-sided rotator cuff tears and intratendinous extension intraoperatively. They injected indigo carmine or methylene blue dye into the shoulder joint, and the shoulder was put through ROM. Torn rotator cuff tissue was easily stained by the injected dye. They found that the test finding was positive when more than half of the tendon thickness was involved, and the accuracy of the test for the detection of articular-sided tears was 65%.
No consensus has been established regarding the modality of treatment for intratendinous tears. Partial-thickness rotator cuff tears are quite common, especially in an active, aging population. Therefore, the presence of a documented tear on MRI or ultrasound may be merely a diagnostic red herring, which may not contribute to a patient’s symptoms. 28 Thus, initial nonoperative treatment should be considered in all patients with PTRCTs. Early surgical repair can be considered for acute tears in any age group and in chronic, reparable tears in young patients (<65 years) of a substantial size (>1 cm) without significant chronic muscle changes. 43 We also tried nonoperative treatment in all our patients for at least 6 months, and after the failure of nonoperative management, we decided to perform an arthroscopic examination and repair.
Moreover, PTRCTs can be repaired after conversion to full-thickness tears. This is a relatively easy method for the repair and restoration of the tendon footprint. However, although this technique yields good clinical outcomes, the completion of partial tears removes structurally intact rotator cuff tissue, and tendon integrity is a primary concern after repair. Furthermore, complete removal of the lateral margin of the rotator cuff insertion increases the risk of nonanatomic restoration of the tendon footprint and of changing the normal biomechanics of the rotator cuff, which could reduce the potential of tendon integrity, and this may result in functional disabilities over time.
Another option of arthroscopic PTRCT repair is transtendon repair, introduced by Lehman and Perry. 24 This technique has the advantage of preserving intact rotator cuff tissue. Moreover, Lo and Burkhart 25 also described that a transtendon repair technique restores the medial footprint of the rotator cuff while preventing a length-tension mismatch that may result from removing normal rotator cuff tissue that is then advanced too far laterally. 5
We used transtendon suture bridge repair for arthroscopically confirmed intratendinous tears, and at final follow-up, the results were satisfactory. Some studies have reported that this technique is a risk factor for the development of postoperative shoulder stiffness and pain.5,20,40 Three (9%) of our patients developed stiffness, which was treated nonoperatively by physical therapy and subacromial corticosteroid injections, and these patients showed good functional recovery at final follow-up.
There are several limitations in our study. First, the retrospective nature of the study has its inherent limitations. Second, there is no control group in our study with which our surgical technique of transtendon suture bridge repair for intratendinous rotator cuff tears has been compared. Uchiyama et al 46 showed satisfactory outcomes in 18 of 19 patients with confirmed intratendinous tears treated with anterior acromioplasty and excision of the diseased tendon portion, followed by tenorrhaphy. Third, our study involved only a small number of patients as isolated intratendinous rotator cuff tears are relatively rare to find. Fourth, there is not any established method of measuring the depth of the tear for intratendinous tears. Generally, surgical treatment for PTRCTs involving >50% tendon thickness is recommended. However, we have tried at least 6 months of nonoperative treatment in all our patients, and after the failure of nonoperative treatment, we decided to perform arthroscopic repair. Lastly, we have no data on the interobserver or intraobserver reliability of detecting intratendinous tears on MRI and arthroscopic surgery because each was performed by 1 practitioner in this study.
Conclusion
Isolated intratendinous rotator cuff tears are rare, and they may be the cause of unexplained shoulder pain. In our series, the incidence of arthroscopically confirmed intratendinous tears was 4.7% among all arthroscopically treated PTRCTs. With the recent advancement of MRI, the diagnosis of intratendinous tears is not as difficult as was previously thought. Usually, physical examination shows positive impingement signs. After the failure of initial nonoperative treatment, arthroscopic transtendon suture bridge repair may yield satisfactory clinical and radiological outcomes in these patients, with significant pain relief.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.