
Abstract
Background:
Tunnel widening after anterior cruciate ligament reconstruction (ACL-R) is a well-accepted and frequent phenomenon, yet little is known regarding its origin or natural history.
Purpose:
To prospectively evaluate the cross-sectional area (CSA) changes in tibial and femoral bone tunnels after ACL-R with serial MRI.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients underwent arthroscopic ACL-R with the same surgeon, surgical technique, and rehabilitation protocol. Each patient underwent preoperative dual-energy x-ray absorptiometry and clinical evaluation, as well as postoperative time zero MRI followed by subsequent MRI and clinical examination, including functional and subjective outcome tests, at 6, 12, 24, 52, and 104 weeks. Tibial and femoral tunnel CSA was measured on each MRI at tunnel aperture (ttA and ftA), midsection (ttM and ftM), and exit (ttE and ftE). Logistic regression modeling was used to examine the predictive value of demographic data and preoperative bone quality (as measured by dual-energy x-ray absorptiometry) on functional outcome scores, manual and instrumented laxity measurements, and changes in tunnel area over time.
Results:
Eighteen patients (including 12 men), mean age 35.5 ± 8.7 years, underwent ACL-R. There was significant tunnel expansion at ttA and ftA sites 6 weeks postoperatively (P = .024 and .0045, respectively). Expansion continued for 24 weeks, with progressive tunnel narrowing thereafter. Average ttA CSA was significantly larger than ftA CSA at all times. The ttM significantly expanded after 6 weeks (P = .06); continued expansion to week 12 was followed by 21 months of reduction in tunnel diameter. The ftM and both ttE and ftE sites decreased in CSA over the 2 years. Median Lysholm and International Knee Documentation Committee scores significantly improved at final follow-up (P = .0083 and <.0001, respectively), and patients returned to preoperative activity levels. Pivot shift significantly decreased (P < .0001). Younger age (<30 years), male sex, and delayed ACL-R (>1 year from time of injury) predicted increased tunnel widening and accelerated expansion in CSA (P < .005).
Conclusion:
Tunnel expansion after ACL-R occurs early and primarily at the tunnel apertures. Expansion may not affect clinical outcome. Younger age, male sex, and delay from injury to ACL-R may be potential risks for enlargement.
Keywords
Function of an anterior cruciate ligament reconstruction (ACL-R) requires secure healing of a tendon graft transplanted into bone tunnels. 35 Graft incorporation and healing is a slow and incompletely understood process. A clinical concern that has emerged is bone tunnel widening after ACL-R.9,12,25,34,38,42 The complications associated with tunnel widening include possible delayed graft incorporation and resultant knee laxity, as well as the additional cost and risk associated with staged revision surgery, if necessary.9,12,15
Despite its recognition, there is a paucity of knowledge regarding the origin and natural history of bone tunnel widening. Tunnel widening likely occurs due to a complex interplay between biologic and mechanical factors. The biologic factors involved may include synovial fluid–derived cytokines and inflammatory mediators, the patient’s bone quality, the graft choice, and cell necrosis from drilling.2,8,12,33,37,38,40 Allograft-specific factors that may contribute include the immune response to allograft and potential toxicity of chemicals used during allograft processing. The mechanical factors identified include local stress deprivation of the bone tunnels in the early postoperative period or excessive graft tunnel motion in the coronal or sagittal planes. The mechanical environment is affected by graft position, graft tension, graft fixation (eg, graft fixation at the tunnel exit vs intra-articular aperture) and aggressive rehabilitation.4,16,17,35,39
Most clinical studies have measured tunnel widening as a snapshot in time and have therefore been unable to draw conclusions about the progression of tunnel expansion or closure over time.7,19,21,24,38 Few clinical studies have examined the progression of tunnel size with cross-sectional serial imaging. 14 The primary aim of this prospective longitudinal magnetic resonance imaging (MRI) study was to examine the progression of changes in bone tunnel dimensions over the initial 2 years after ACL reconstruction at 3 distinct locations along both the femoral and tibial tunnels. In addition, we examined the associations among age, sex, graft type, duration between injury and surgery, manual laxity, clinical outcome measures, and preoperative bone mineral density (BMD) on the magnitude of tunnel expansion or closure over the 2 years. To our knowledge, this is the first study to use serial MRI, starting with an MRI immediately postoperatively.
Methods
Patients
After approval by an institutional review board, patients were prospectively enrolled into the study. Inclusion criteria were ACL deficiency and age between 18 and 55 years. Exclusion criteria were previous knee injury or surgery, current multiligament injury, systemic soft tissue/connective tissue disorder, and pregnancy. Preoperative evaluations included standard history and physical examination, regional and standard BMD measures by dual-energy x-ray absorptiometry (DEXA), and functional outcome measures. All patients signed an informed consent as part of their enrollment.
Dual-Energy X-Ray Absorptiometry
The DEXA scan included standard measures of lumbosacral and femoral neck BMD to calculate standardized T and Z scores, as well as regional BMD measurements at the femoral condyle and tibial plateau of the affected knee. Standardized T and Z scores were compared with regional measures of BMD to evaluate any local changes in BMD not present in the standard DEXA evaluation. Both standard and regional BMD measurements were correlated with tunnel cross-sectional area (CSA), objective outcomes, and clinical scores.
Surgical Procedures
After the preoperative evaluations, each patient underwent ACL-R with the same surgeon (S.A.R.) using the same surgical technique. A comprehensive diagnostic arthroscopy was performed on each patient. Meniscal and chondral injuries were addressed before ACL-R.
After care for associated injuries, the appropriate graft, either bone–patellar tendon–bone (BPTB) or hamstring autograft, was harvested in a standard fashion. The grafts were prepared and measured on a back table while the femoral and tibial tunnels were drilled to the corresponding sizes. The femoral tunnel was drilled using a transtibial technique at the time when this study was performed, with care being taken to center the tunnel in the anatomic footprint, emphasizing the isometric position of the anteromedial portion of the ACL. An “over-the-top” guide was used to allow reproducible positioning of the femoral tunnel, aiming for the 10:30-o’clock position (in a right knee) using the clock face analogy. The tibial tunnel was drilled using a tibial guide. The guide was set at 55° from the horizontal and placed at the posterior aspect of the anteromedial bundle to best re-create the native ACL footprint. The entry point for the tibial tunnel guide pin was placed at the posterior border of the anterior horn of the lateral meniscus. The graft was fixed in the femoral tunnel with a bioabsorbable interference screw (Hexalon; Inion, Inc) and then preconditioned and manually tensioned before interference screw fixation (Hexalon) on the tibial side. The bioabsorbable screws used in all patients were composed of copolymers L-lactide and D-lactide mixed with trimethylene carbonate.
Rehabilitation
A standardized postoperative rehabilitation protocol was used for all patients. Protected, partial weightbearing was permitted immediately after surgery with the assistance of a brace and crutches. Early knee motion was encouraged. Patients were progressed to full weightbearing as tolerated within the first 2 postoperative weeks. The use of a brace and crutches was discontinued as quadriceps strength, coordination, and neuromuscular function improved, typically at approximately 4 weeks. When 90° of motion was achieved, cycling was permitted on a short crank ergometer. Patients were advanced to a standard ergometer once 110° of motion was present. Progression to running was based on restoration of appropriate muscle strength, endurance, balance, coordination, and proprioception, as measured by the physical therapist. Patients were generally able to meet these criteria to begin running at about 4 months, with return to sports after 6 to 8 months. The rehabilitation protocol was not altered for concomitant meniscal repair, since all tears were vertical longitudinal tears with no repairs of complex radial tears.
Tunnel Measurements
An MRI of the operative knee was conducted immediately after ACL reconstruction on postoperative day zero, as well as 6, 12, 24, 52, and 104 weeks postoperatively. All knee MRI scans were performed on the same 1.5-T magnet (General Electric Health Care) with a standardized coil (Medrad phased array) and evaluated by the same board-certified musculoskeletal radiologist (H.P.). Measurements were made with moderate echo time images (repetition time, 3500-5000 ms; echo time, 34 ms [effective]; field of view, 13 [coronal] to 16 [sagittal] cm2; matrix, 512 × 320 [coronal] to 384 [sagittal]; slice thickness, 3 [coronal] to 3.5 [sagittal] mm with no gap). Receiver bandwidth was ±31.25 kHz. Measures of tunnel CSA were calculated perpendicular to the long axis of the tunnel at 3 distinct and standardized locations along both the tibial and femoral tunnels in both the sagittal and coronal planes. The tibial and femoral tunnel aperture (ttA and ftA) measurements were calculated 0.5 cm from the joint-tunnel interface (Figure 1). The tibial and femoral tunnel midsection (ttM and ftM) measurements were calculated at the midline of the longitudinal axis of the tunnel (Figure 1). The tibial and femoral exit (ttE and ftE) measurements were calculated 0.5 cm from the termination of the tunnel (Figure 1). Cross-sectional measurements were calculated in a similar fashion to work previously published and assuming an elliptical shape of the tunnel, measured in millimeters squared (mm2).11,14,21 Tunnel expansion was defined by the change compared with measurements made on the MRI immediately postoperatively.
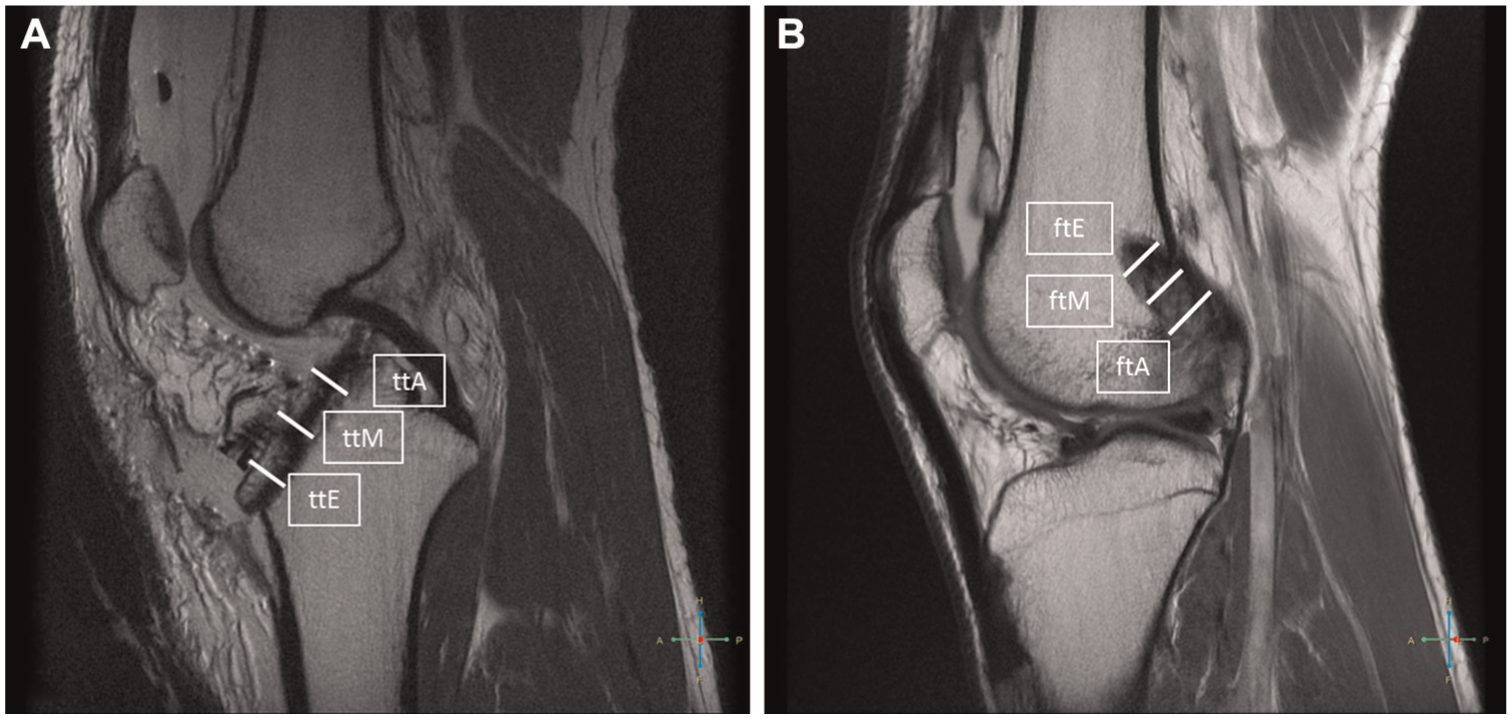
Representative sagittal magnetic resonance images of the knee demonstrating the locations of the (A) tibial and (B) femoral tunnel sites of cross-sectional area measurement. ftA, femoral tunnel aperture; ftE, femoral tunnel exit; ftM, femoral tunnel midsection; ttA, tibial tunnel aperture; ttE, tibial tunnel exit; ttM, tibial tunnel midsection.
Postoperative Evaluations
Postoperative objective measures of knee stability included a Lachman test, a pivot-shift test, and an instrumented knee laxity test with the KT-1000 arthrometer (MEDmetric Corp). The operating surgeon performed all pivot-shift examinations and was blinded to the magnitude of bone tunnel change. An experienced physical therapist (J.C.), blinded to the magnitude of bone tunnel change, performed all KT-1000 arthrometer measurements, and side-to-side differences were calculated at 89 N. Functional outcome was measured using the Lysholm score, International Knee Documentation Committee (IKDC) subjective score, and Tegner activity level.
Statistical Methods
Data from tunnel measurements and postoperative evaluations were compiled in Excel (Microsoft Corp) spreadsheets and imported into SAS, version 9.3, statistical software (SAS Institute, Inc) for analysis. Frequency measures were computed for all data, and diagnostic plots were created to determine best fit. Measures of central tendency (eg, median, mean) were calculated for functional scores, and paired t tests were conducted to determine significance of change over time. Change in CSA of the tibial and femoral tunnels within patients over time was assessed using paired t tests between all time points in a chronologic stepwise fashion. Comparison of the tibial and femoral CSAs was conducted at each time point using t tests. Linear regression was then conducted using generalized estimating equations (GEEs) with an AR (1) covariance structure and controlling for repeated measurements within individuals. With use of a data-driven approach, each predictor variable was tested in a separate model controlling for time and time squared, when appropriate, as determined by significance in the model and model fit. The time-squared parameter represents acceleration of change. Additional models were created exploring predictor interactions with time and time squared. These models were created for each of the 6 outcome CSAs. Effect estimates were produced in all linear regression analyses. An alpha level of 0.05 was considered statistically significant for all tests.
Results
Eighteen patients were enrolled in the study (Table 1). Twelve patients were men, and mean age was 35.5 years (range, 19-47.9 years). The median time from injury to surgery was 50.5 days (range, 26 days–29.2 years). A BPTB autograft was used in most reconstructions, 14 of 18 (77.8%), while autograft hamstring graft was used in 3 of 18 (16.7%), and 1 patient (5.6%) received an Achilles tendon allograft. Twelve patients (66.7%) had concomitant chondral injuries: 6 lateral femoral condyle, 3 medial femoral condyle, 2 patellar, and 1 trochlear groove. Nine of the 12 were addressed with debridement and 1 underwent microfracture. Sixteen (88.8%) sustained meniscal damage: 8 medial meniscus, 7 lateral meniscus, and 1 both medial and lateral. Four meniscal tears were treated with repair, and the remainder underwent meniscectomy or debridement.
Demographic and Baseline Data for the Prospective Cohort (N = 18) Undergoing ACL-R a
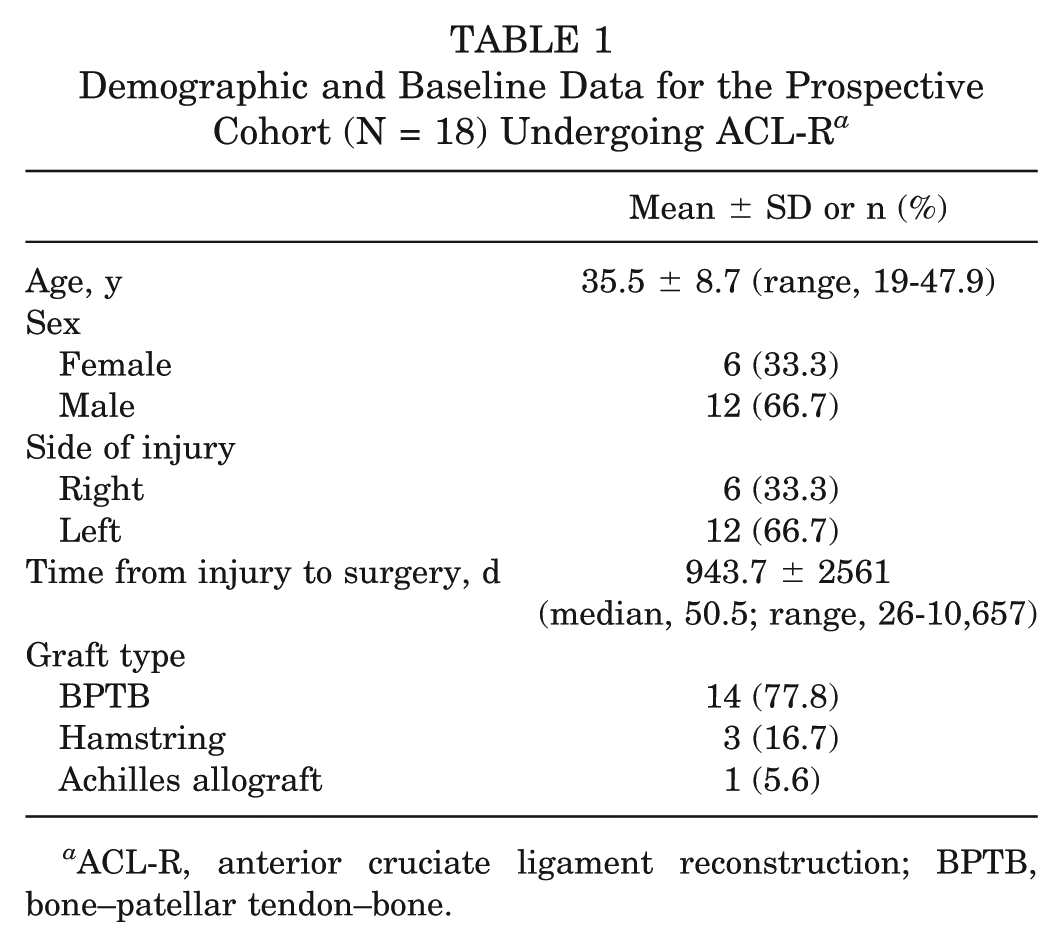
ACL-R, anterior cruciate ligament reconstruction; BPTB, bone–patellar tendon–bone.
The BMD results are summarized in Table 2. The mean lumbosacral T score was −0.26 ± 1.1, and the mean femoral neck T score was −0.37 ± 1.2. Six patients were considered osteopenic (preoperative T score −1.0 to −2.5), and 1 patient was osteoporotic (T score <–2.5). Local measures of BMD were conducted on the operative lower extremity femoral condyle and tibial plateau. The mean femoral condyle BMD was 0.65 ± 0.3 g/cm2, and the mean tibial plateau BMD was 0.61 ± 0.2 g/cm2. Preoperative T scores did not correlate with postoperative clinical scores or objective measures of knee laxity, nor were they predictive of rate of change or acceleration of change in tunnel CSA. Likewise, regional BMD measures at both locations (femoral condyle and tibial plateau) were not predictive of rate of change or acceleration of change in tunnel CSA, nor did regional BMD correlate with postoperative clinical scores or objective measures of knee laxity.
Preoperative Bone Mineral Density Results for the ACL-R Cohort (N = 18) a
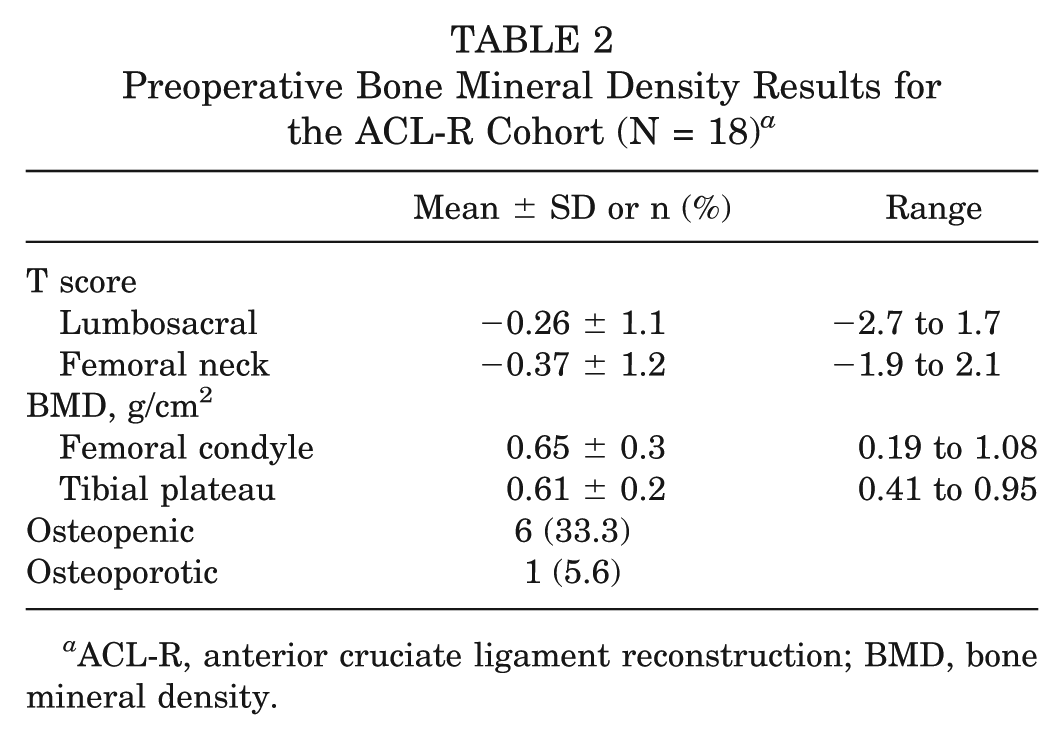
ACL-R, anterior cruciate ligament reconstruction; BMD, bone mineral density.
The clinical results from baseline (either preoperative or early postoperative) and final follow-up are presented in Table 3. There was significant improvement in the median Lysholm score (preoperative 64, final follow-up 89; P = .0083) and IKDC score (56.5 preoperatively to 91 at final follow-up; P < .0001). The activity level was returned to preoperative levels by final follow-up at 2 years as indicated by Tegner activity score (P = .19). Manual knee laxity, as measured by pivot shift, significantly decreased from the preoperative level (average grade 2) to the final follow-up (average grade 0; P < .0001) (Table 3). All patients had a positive pivot-shift examination at the preoperative visit (16/18 grade 2 and 2/18 grade 1). At final follow-up, 17 of 18 patients (94%) had a negative pivot-shift examination (grade 0), and 1 of 18 (6%) had a grade 1 positive examination. The mean side-to-side instrumented knee laxity was 0.83 mm (range, −2.5 mm to 4.0 mm) at the first calculated follow-up and 1.22 mm (range, −2.0 mm to 3.0 mm) at final follow-up. There was no significant change in the KT-1000 arthrometer side-to-side difference between 6 weeks and 2 years (P = .38) (Table 3). Seventeen of 18 patients (94%) had a side-to-side difference of <3 mm at final follow-up, and 1 patient had a 3-mm side-to-side difference at final follow-up. The patient with a 3-mm side-to-side difference also had a grade 1 pivot shift. This patient was male, had normal BMD preoperatively, and had greater than 1 year between time of injury and surgery, and reconstruction was done using autograft BPTB. His tunnel measurements were not significantly different from any other patient at any time during the study.
Summary of the Subjective and Objective Clinical Outcomes a

IKDC, International Knee Documentation Committee.
Paired t tests.
Baseline KT-1000 arthrometer measurement performed at postoperative 6- or 12-week visit.
Tibial Tunnel Area
The mean tunnel CSA, with standard deviation, at each location and at each time point is presented in Figure 2. The change in mean tunnel CSA is depicted in Figure 3. The tibial tunnel aperture site demonstrated tunnel expansion over the first 24 postoperative weeks followed by tunnel closure from 24 weeks to 2 years (Figure 2A). The early tunnel expansion was significant over the first 6 postoperative weeks, P = .024 (Figure 3A). The tibial tunnel midsection expanded over the first 12 postoperative weeks followed by tunnel closure from 3 months to 2 years (Figure 2A). In similar fashion to the tibial aperture, midsection expansion over the first 6 postoperative weeks was significant, P = .006 (Figure 3A). There was tunnel closure over the entire 2-year postoperative period at the tibial tunnel exit site (Figure 2C). The closure was significant between 12 and 24 weeks and again between 24 weeks and 1 year (P = .0073 and .036, respectively) (Figure 3A). At 2 years, the largest CSAs were present at the aperture site followed by the midsection, while the smallest CSAs were observed at the tunnel exit (Figure 2, A-C). The differences between all 3 locations were statistically significant, with the tunnel aperture greater than the midsection (P = .0085) and the tunnel exit (P < .0001). The tunnel midsection was also significantly larger than the tunnel exit (P < .0001).
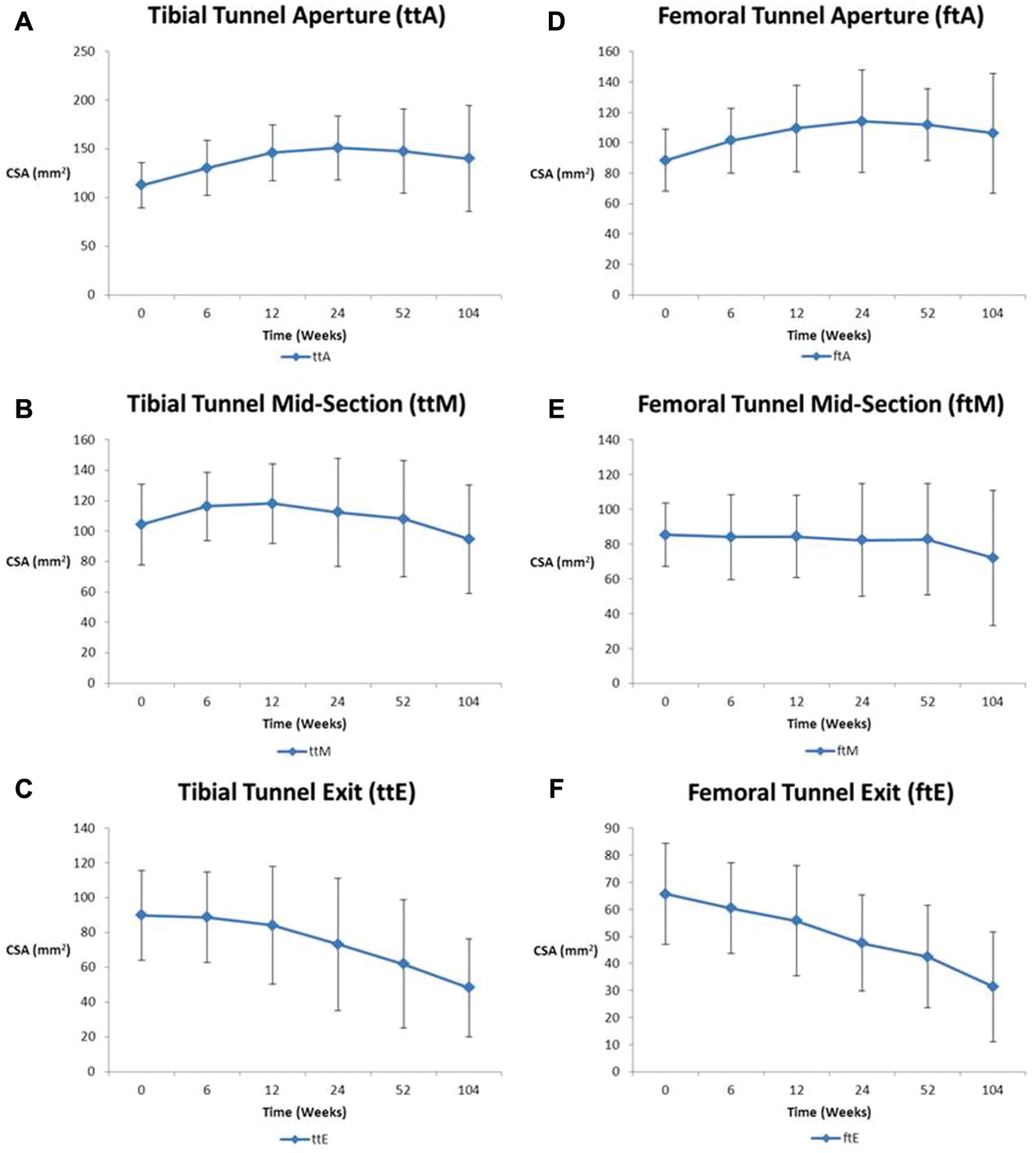
Graphic representation of the mean cross-sectional area plus or minus standard deviation at each tunnel location over the 6 time points. (A) Tibial tunnel aperture, (B) tibial tunnel midsection, (C) tibial tunnel exit, (D) femoral tunnel aperture, (E) femoral tunnel midsection, and (F) femoral tunnel exit.
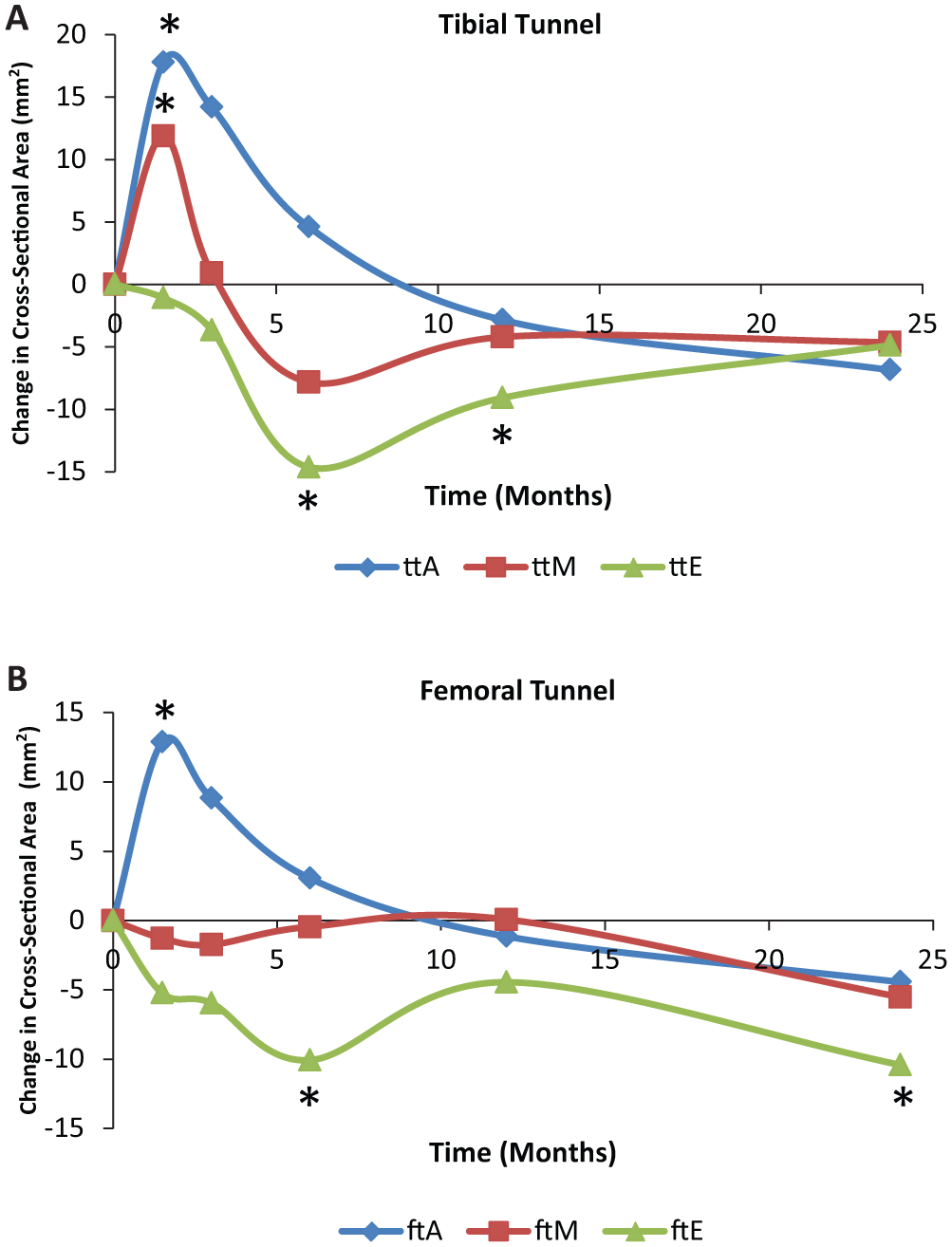
Graphic representation of the change in cross-sectional area between each postoperative time point. *Statistically significant changes. ftA, femoral tunnel aperture; ftE, femoral tunnel exit; ftM, femoral tunnel midsection; ttA, tibial tunnel aperture; ttE, tibial tunnel exit; ttM, tibial tunnel midsection.
Femoral Tunnel Area
On the femoral side, the tunnel expanded at the aperture site for 24 weeks followed by an 18-month period of progressive tunnel closure (Figure 2D). Similar to the tibial tunnel aperture, the femoral tunnel aperture expansion was significant in the early postoperative period from time zero to 6 weeks (P = .0045) (Figure 3B). Although there were no statistically significant size changes at the femoral tunnel midsection, there was a general trend toward decreasing size over time (Figures 2E and 3B). At the femoral tunnel exit site, there was closure throughout the 2-year postoperative follow-up (Figure 2F). The femoral tunnel exit site closure was significant between 12 and 24 weeks and again between 1 year and 2 years (P = .026 and .024, respectively) (Figure 3B). The mean magnitude of tunnel CSA was the largest at the tunnel aperture and the smallest at the tunnel exit (Figure 2, D-F). At 2 years, the largest CSAs were present at the aperture site followed by the midsection, while the smallest CSAs were observed at the tunnel exit (Figure 2, D-F). The differences between all 3 locations were statistically significant, with the tunnel aperture greater than the midsection (P = .0065) and the tunnel exit (P < .0001). The tunnel midsection was also significantly larger than the tunnel exit (P < .0001).
Comparison of Tibial and Femoral Tunnels
Given the significant early postoperative tunnel expansion present at the tunnel aperture sites, the tibial and femoral aperture CSA measurements were compared at each time point (Figure 4). At each time point, the mean tibial tunnel aperture CSA was significantly larger than the mean femoral tunnel aperture CSA. At time zero, the mean difference in CSA was 24.06 mm2 (P = .001). This finding was consistent with intraoperative tunnel reaming sizes, which were significantly larger on the tibial side compared with the femoral side. However, the mean difference in CSA between the 2 tunnels increased at each time point until the 24th postoperative week. The mean difference at 6 weeks was greater in magnitude than the difference at time zero. The mean difference between tibial tunnel apertures and femoral tunnel apertures was 28.98 mm2 (P = .0019) at 6 weeks, 36.48 mm2 (P = .0003) at 12 weeks, and 36.87 mm2 (P = .0006) at 24 weeks. The differences between the tibial and femoral tunnel aperture sites remained at 1 year (35.7 mm2) and 2 years (33.65 mm2). The differences in size remained statistically significant (P = .0024 and .0084 at 1 and 2 years, respectively).
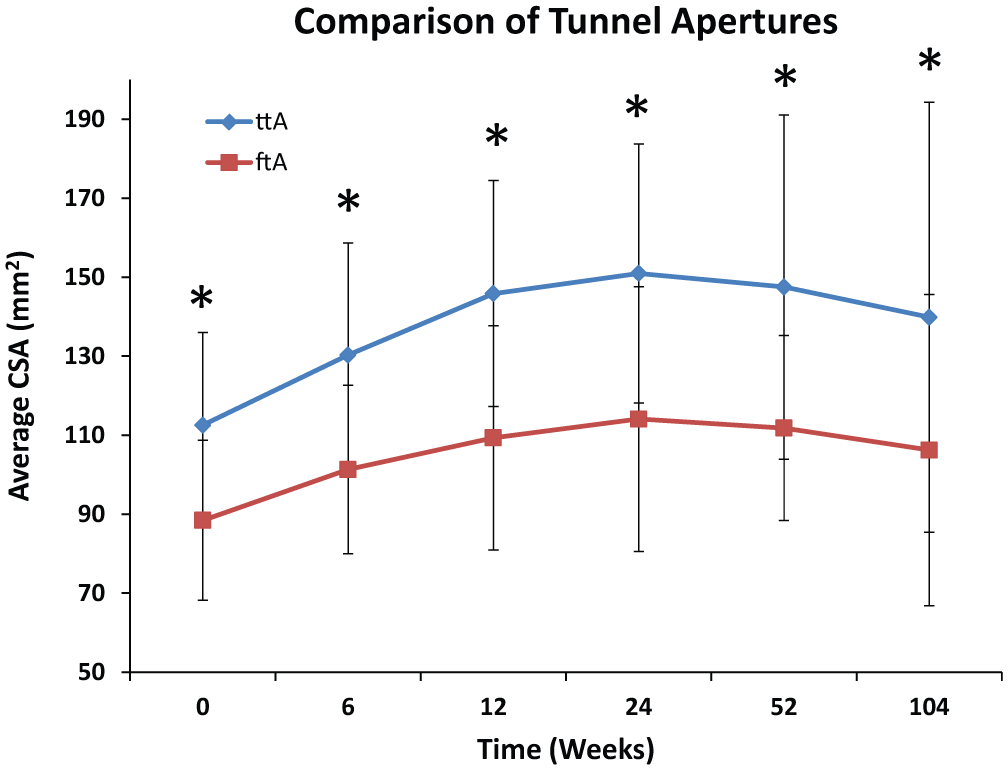
Graphic representation of the average tibial (ttA) and femoral (ftA) tunnel aperture cross-sectional area (CSA) at each postoperative time point. *Statistically significant difference in the average CSA between the tibial and femoral tunnels.
Predictors of Tunnel Cross-Sectional Area
Using the GEEs, we accounted for all potential predictors of the CSAs of the tibial and femoral tunnels. The predictor variables assessed included age, sex, side of injury, lumbosacral T score, femoral neck T score, femoral condyle and tibial plateau BMDs, graft choice, time from injury to surgery, preoperative IKDC score, preoperative Lysholm score, preoperative Tegner activity level, preoperative pivot-shift measurement, and KT-1000 arthrometer measurement at the 6- or 12-week postoperative assessment. This modeling was conducted for the time zero CSA measurements, change in CSA over time, and acceleration in change over time; all significant associations are shown in the Appendix (available in the online version of this article at http://ajsm.sagepub.com/supplemental). The potentially pertinent predictors, those significantly associated with CSA at multiple tunnel locations, are reviewed here.
Patient age had significant associations with bone tunnel CSA, rate of tunnel area change, and acceleration in tunnel area change (Appendix). Younger age (<30 years, n = 6) consistently was associated with larger tunnel size at baseline, compared with age 30 years or older (n = 12) (effect estimates from 8.11-34.8 mm2). At the tibial tunnel aperture, younger age also predicted an increase in tunnel size over time (β = 0.088, P = .002), as well as a faster acceleration in tunnel size (β = 0.0001, P = .0007). Male sex (n = 12) was associated with larger tunnel size at the tibial tunnel aperture, with the effect estimate of 31.8 mm2 (P = .0009). Males also had significantly increased tibial and femoral tunnel aperture sizes over time, as well as significantly faster acceleration in tunnel size over time, compared with females (n = 6; ttA rate, P = .0005; ttA acceleration, P = .0012; ftA rate, P = .014; ftA acceleration, P = .015).
Time from injury to surgery was also a significant predictor of tunnel size (Appendix). A time from injury to surgery of less than 1 year (n = 14) consistently was associated with smaller tunnel CSA at all tibial and femoral tunnel locations. Furthermore, ACL-R within 1 year of injury was associated with a decreased rate of tunnel expansion over time at all tibial and femoral tunnel locations. Last, at the tibial tunnel and femoral tunnel apertures, the 2 locations at which tunnel expansion lasted for greater than 12 weeks, having ACL-R within 1 year of the time of injury predicted a slower acceleration during the periods of tunnel expansion (both P < .0001).
Graft type was generally not a significant predictor of time zero tunnel size, rate of change over time, or acceleration over time. The only significant difference was seen in the midsection of the femoral tunnel. The BPTB (n = 14) cohort had a significantly smaller tunnel size at the ftM compared with the hamstring cohort (n = 3; P = .011). The BPTB cohort also had a significantly higher rate of tunnel closure at the ftM compared with the hamstring cohort (P = .0041). Aside from the ftM, graft type was not a predictor of tunnel size, rate of change over time, or acceleration of tunnel area over time (Appendix).
Discussion
Despite its recognition, there is a paucity of knowledge regarding the origin and natural history of bone tunnel widening. Tunnel widening likely occurs due to a complex interplay of biologic and mechanical factors; however, little is known about which preoperative factors may be predictive of postoperative bone tunnel enlargement. Furthermore, studies that have examined these associations are largely limited by their experimental design, choosing to measure tunnel area at one time point and comparing this measurement to tunnel reamer size. One clinical study examined the progression of tunnel size with cross-sectional serial imaging. 14 To our knowledge, the present study is the first to use serial MRI, starting with an MRI on the day of surgery, to accurately quantify tunnel dimensions.
The primary aim of this prospective longitudinal MRI study was to examine the progression of tunnel expansion and narrowing over the initial 2 years of follow-up at 3 distinct locations along both the femoral and tibial tunnels. In addition, we examined the associations among graft choice, patient age, sex, duration between injury and surgery, manual and instrumented laxity, clinical outcome measures, and preoperative BMD on the magnitude of tunnel expansion or narrowing, as measured by cross-sectional area.
Our study shows that both tibial and femoral tunnels are dynamic, with tunnel expansion and contraction over time. At both the tibial and femoral tunnels, the aperture and midsection CSAs generally increased to the 24th postoperative week, eventually plateauing before decreasing in area from 1 year to final follow-up at 2 years. The significant tunnel expansion was present at both tunnel apertures and the tibial tunnel midsection, which is consistent with a prior serial measurement study of the timing of postoperative tunnel expansion. 14 This finding is notable since healing at the graft aperture is most important for graft function.20,35 In contrast to the tunnel apertures and midsections, the tunnel exit sites continually decreased in CSA over the study period at varying rates. We found no consistently significant associations between functional outcome scores or objective measures of knee laxity and tunnel CSA, which is generally consistent with previous studies. # However, at least 1 study has reported a positive relationship between tunnel expansion and knee laxity. 21
Graft tunnel motion has been postulated to be an etiologic factor for bone tunnel expansion. Previous studies of ACL-R fixation techniques have suggested that aperture fixation with interference screws may limit graft micromotion and tunnel expansion compared with suspensory fixation.16,17,31,35,39 It has also been postulated that the magnitude of femoral tunnel widening at the aperture is less than that at the tibial tunnel aperture due to the ability to place the femoral interference screw directly at the joint line while the tibial interference screw is often placed somewhat distal to the joint line.1,14,18,20,29 Our study has corroborated these findings. In our study, each patient had his or her graft, whether soft tissue or BPTB, fixed with interference screws in both the femoral and tibial tunnels, and we demonstrated significantly greater tunnel CSA expansion on the tibial tunnel side compared with the femoral tunnel side.
Although our data suggest the importance of aperture fixation to prevent mechanically induced micromotion and subsequent bone tunnel enlargement, other important factors in addition to fixation position need to be considered. Graft tunnel motion is primarily affected by stiffness of the bone-graft-bone construct. For example, cortical-based fixation has higher stiffness compared with cancellous fixation. The overall stiffness of the bone-graft-bone construct is determined by the interaction between fixation-to-fixation distance and the stiffness of the fixation device. Thus, aperture fixation is not the only factor to consider, since the stiffness of the overall construct is determined by several factors.
There are a number of previous reports on tunnel enlargement after ACL-R.9,12,14,18,21,24,29,42 In comparison to these previous studies, a strength of our study is the experimental design. Most of these previous studies are prone to inaccurate tunnel measures for 2 methodologic reasons. The first is the use of the reamer drill size as the initial tunnel area measurement when making tunnel enlargement comparisons between final follow-up and initial tunnel area.9,21,24,29 A recent study by Kopf et al 27 demonstrated that sagittal and transverse drill angle can significantly affect tunnel aperture size for the same drill-bit diameter, thus calling into question area measurements made on reamer drill size alone. Furthermore, transtibial techniques may lead to changes in the tibial tunnel after it is drilled, due to passage of the drill through the tunnel again to drill the femoral tunnel.
The second methodologic concern is the use of a single postoperative tunnel area measurement when making statements about tunnel changes over time.12,21,24,29 We are aware of 1 previous MRI study evaluating tunnel enlargement after ACL-R; however, this study used a single follow-up assessment of tunnel dimensions and compared this measure with intraoperative reamer drill size. 24 One previous prospective, serial, cross-sectional imaging study used computed tomography to evaluate tunnel enlargement after ACL-R. 14 The authors only evaluated the tibial tunnel area over time and did not address rate of change or acceleration of change. Despite these limitations, our results are consistent with their findings of early expansion (0-6 weeks) at the tibial aperture and midsection followed by gradual tunnel narrowing.
In addition to the mechanical factors postulated as the cause of bone tunnel enlargement after ACL-R, there are likely biologic factors associated with tunnel enlargement.** Tunnel expansion is due to loss of bone, which is caused by an imbalance between osteoclastic resorption and osteoblastic formation. One of the many proposed biologic mechanisms of tunnel expansion after ACL-R is a deleterious effect on bone of intra-articular cytokine release after ACL reconstruction.9,26,36,42 It is known that inflammatory mediators such as tumor necrosis factor–α affect osteoclast activity. Using a rabbit ACL-R model, the authors found increased osteoclastic activity at sites with increased graft tunnel motion. 35 The results of our modeling of predictors associated with tunnel CSA at baseline, changes in area, and acceleration in rate of change in area may substantiate the role of inflammatory cytokines. Those patients with longer durations between time of injury and surgical reconstruction had significantly larger tunnel size at all tibial and femoral tunnel locations. Furthermore, delay to ACL-R greater than 1 year from time of injury was associated with an increased rate of tunnel expansion over time at all tibial and femoral tunnel locations. Delay to reconstruction of greater than 1 year was also significantly predictive of accelerated tunnel expansion at both the femoral and tibial tunnel apertures. This finding could be due to mechanical factors such as stress deprivation or biologic factors such as increased cytokine production. Furthermore, it is known that persistent elevations in cytokine levels occur in ACL-injured knees. 5
A biologic response to bioabsorbable screws leading to sequelae from an inflammatory response and osteolysis has been reported.10,32 However, a large body of literature has demonstrated satisfactory clinical outcomes and comparable results with poly-L-lactic acid–based screws compared with metal screws.3,13,22,28,30 In addition, the screws used in the current study have been used as the only fixation method in a previous study without screw-related adverse outcomes. 21 In the current study, none of the patients had MRI findings suggestive of a reaction to the bioabsorbable screw fixation.
The finding of an association between male sex and younger age at the time of ACL-R and postoperative tunnel widening has not yet, to our knowledge, been reported. This finding may be due to higher activity levels in younger, active patients, which has been linked to higher failure rates for ACL-R. 23 Interpretation of all of the predictive modeling should be made with caution given the small sample size in this study. These predictors and duration between injury and ACL-R should be further explored with hypothesis-driven, prospective studies with larger sample sizes.
The effect of tunnel widening on graft function and knee laxity remains unclear. Although tunnel widening was not related to knee laxity or clinical outcome scores in our study, at least 1 prior study has found a relationship. 21 Tunnel expansion can have implications for revision surgery, as a 2-stage approach may be required to first bone graft the tunnels, followed by later revision ACL reconstruction. Furthermore, tunnel expansion at time points greater than 6 months may suggest poor graft-to-bone healing, which may lead to increased laxity over time. Longer follow-up will shed light on this question.
This study is not without limitations. The first is that despite excellent patient follow-up, we had a small sample size due to the demanding study protocol with numerous MRI scans. A second limitation is related to graft selection. Despite consistent surgical technique, tunnel placement, and graft fixation, we had a heterogeneous population of graft material. Given the small sample size, it is difficult to make any meaningful conclusions about the effect of graft choice on tunnel widening in this study. Finally, this study was data driven, and directional hypotheses were not formed due to a paucity of tunnel enlargement data in the literature. Therefore, this study should be corroborated with further hypothesis-driven, directional prospective studies using larger sample sizes.
In conclusion, this serial, prospective MRI study of tunnel area change is the first such study to longitudinally examine the changes of both the tibial and femoral tunnels with baseline measurements at postoperative day zero and subsequent measurements at 6, 12, 24, 52, and 104 weeks. The results of the current study provide additional data to support the theory that limiting the distance between fixation points and limiting the distance between each individual fixation point and tunnel aperture decreases tunnel widening, as we demonstrate greater tunnel expansion at the tibial tunnel compared with the femoral tunnel. In addition, as suggested by prior studies, functional outcome scores and objective measures of knee laxity were not associated with tunnel widening. Further study is required to examine the relationship between younger age, male sex, and delay from injury to ACL-R as potential risk factors for postoperative tunnel enlargement.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.