
Abstract
Background:
Multiligament knee injuries (MLKIs) can also involve the medial patellofemoral ligament (MPFL), but there is a paucity of information regarding prevalence and relevance of MPFL involvement in this setting.
Purpose:
(1) To identify the prevalence of MPFL injury in MLKIs, (2) to determine whether an MPFL tear results in symptomatic patellar instability, and (3) to report clinical and functional outcomes of patients with and without MPFL tears after MLKI surgical reconstruction.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The records of all patients who underwent surgical reconstruction of MLKI (defined as a grade 3 injury of ≥2 ligaments) at a single institution from 2007 to 2010 were reviewed. Age, sex, knee dislocation classification (according to Schenck), and MRI findings were documented. All preoperative MRI scans were reviewed by an experienced musculoskeletal radiologist to determine the presence or absence of MPFL involvement. If an MPFL tear was present, its anatomic location and severity as well as the presence of patellar or lateral femoral condyle bone bruises were documented. Inclusion criteria included (1) MLKI treated at a single institution, (2) presence of MPFL tear on preoperative MRI, and (3) minimum 2-year clinical follow-up. Patellar instability symptoms were assessed with the Kujala Knee Questionnaire. Functional outcomes were measured using the International Knee Documentation Committee (IKDC) score. IKDC scores were compared between patients who sustained MLKIs with and without MPFL tears. There were 21 patients in each group.
Results:
Over the 4-year study period, 30 of 51 patients (59%) treated surgically for a MLKI had MRI evidence of an MPFL tear. Nine were lost to follow-up, leaving 21 patients for review. There were 13 complete (62%), 5 high-grade partial (24%), and 3 partial (14%) MPFL tears. Sixteen of 21 tears (76%) occurred at the proximal third, with the remainder exhibiting diffuse signal abnormality consistent with tearing throughout the length of the MPFL. The superficial medial collateral ligament was involved in all patients. In no case was the MPFL repaired or reconstructed. At mean follow-up of 3.6 years (range, 2.0-5.7 years), only 1 of 21 patients (5%) complained of patellofemoral instability symptoms whereas 20 of 21 patients (95%) did not experience patellar subluxation or dislocation. No significant difference was found when IKDC scores were compared between patients with and without an MPFL tear (mean ± SD, 65.5 ± 22.9 vs 79.4 ± 16.1; P = .07).
Conclusion:
MPFL tears occur frequently in patients with MLKI but rarely cause instability. In the majority of cases, MPFL tears do not need to be addressed at the time of surgery.
Keywords
Multiligament knee injuries (MLKIs) refer to trauma involving at least 2 of the 4 major ligament structures of the knee. 4 Classification schemes for the knee with multiple ligament injuries can help to direct management, predict the risk of associated injuries, and determine prognosis. Schenck and colleagues 27 described a useful anatomic classification for MLKIs, with patterns of injury based on involvement of the cruciate and collateral ligaments. In addition, studies on outcome for MLKIs following nonoperative and operative treatment are common.4,12,14,19,20,25,29 However, to our knowledge, no information exists on the often-injured medial patellofemoral ligament (MPFL) in the setting of MLKI. Therefore, optimal treatment strategies remain undefined, and there is a paucity of data in the literature to assist in guiding management.
There is a great deal of controversy in the literature regarding operative versus nonoperative treatment of the MPFL after a first-time patellar dislocation.1,5-7,17,21,23,24,26,28 It is tempting to extrapolate some of these data to the setting of MLKI. However, surgical treatment of a torn MPFL at the time of MLKI reconstruction may not be necessary and could increase the risk of complications, such as stiffness. The purpose of this study was to (1) identify the prevalence of MPFL injuries in the surgically reconstructed multiligament injured knee, (2) determine whether untreated MPFL tears lead to symptomatic instability, and (3) assess whether patients with untreated MPFL tears have inferior clinical and functional outcomes compared with patients without MPFL tears in the setting of MLKI reconstruction.
Methods
After approval was granted by our institutional review board, the records of all patients 18 years and older who had undergone reconstruction after a MLKI (defined as a grade 3 injury to ≥2 ligaments) between January 2007 and December 2010 were retrospectively reviewed. Age, sex, knee dislocation classification (Schenck et al 27 ), and magnetic resonance imaging (MRI) findings were documented. Any patients who had undergone a previous surgery to treat MLKI before presentation at our institution were excluded from the study. Each MRI was performed by use of a high-field-strength 3-T magnet (3T Signa HDX 16.0; GE Healthcare) using a dedicated 8-channel transmit-receive, phased-array knee coil. The standard knee MRI protocol included sagittal proton-density-weighted images (3 mm; repetition time [TR]/echo time [TE], 2200/18 ms); sagittal, coronal, and axial fat-suppressed, intermediate-weighted sequences (3 mm; TR/TE, 4000-6000/45 ms); and coronal T1-weighted images (3 mm; TR/TE, 700-900 ms/minimum).
All preoperative MRI scans were reviewed by a fellowship-trained musculoskeletal radiologist with 15 years of experience, who had been blinded to the history of each patient, to determine the presence or absence of an MPFL tear. The severity of the MPFL tear was classified as full thickness, high-grade partial, or partial thickness based on the shape and signal abnormality seen on the axial fat-suppressed, intermediate-weighted sequences. A full-thickness tear was defined as complete morphologic fiber discontinuity with fluid signal intensity within the area of tearing (Figure 1). A high-grade partial tear was defined as marked ligamentous tissue thickening and/or disorganization and laxity with intermediate to high signal abnormality. A partial-thickness tear was defined as mild soft tissue thickening and/or disorganization with low to intermediate signal abnormality. The anatomic location of the MPFL tear was defined as proximal third (from the femoral attachment), middle third (midsubstance segment), or distal third (patellar attachment). The typical bone bruise pattern associated with lateral patellar dislocation was defined as focal areas of high signal marrow abnormality within the patella and the anterior lateral femoral condyle. Inclusion criteria included (1) MLKI treated at our institution, (2) presence of MPFL tear on preoperative MRI, and (3) minimum 2-year clinical follow-up. Presence or absence of patella alta was assessed from the lateral radiograph using the Caton-Deschamps (C-D) ratio. 9 Trochlear dysplasia was identified on the lateral and Merchant radiographs using the classification by Dejour et al. 8 Patellar instability symptoms were assessed with a subset of the Kujala Knee Questionnaire. 18 Patients were queried by telephone about patellar dislocation, subluxation, and feelings of instability with regard to the patellofemoral joint. Possible answers include (a) none, (b) occasionally in sport activities, (c) occasionally in everyday activities, (d) at least 1 dislocation after surgery, and (e) more than 2 dislocations. Functional outcomes were graded as poor, fair, good, or excellent using the International Knee Documentation Committee (IKDC) subjective score.
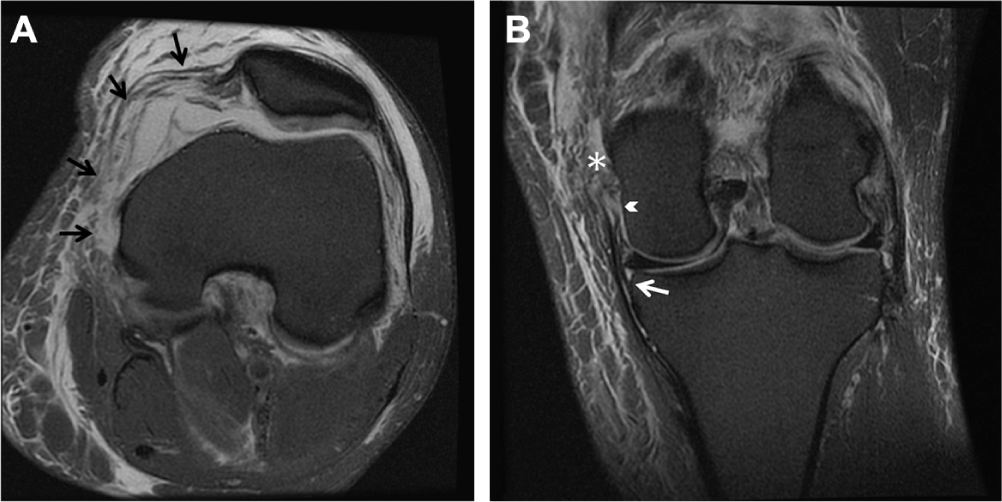
A 50-year-old male patient with multiligament knee injury. (A) Axial fat-suppressed, intermediate-weighted image demonstrates near complete disruption of the medial patellofemoral ligament (black arrows) with the exception of a few intact fibers near the patellar attachment. (B) Coronal fat-suppressed, intermediate-weighted image demonstrates complete disruption of the proximal fibers of the superficial medial collateral ligament (MCL) (asterisk) and meniscofemoral fibers of the deep MCL (arrowhead). The meniscotibial fibers of the deep MCL are intact (white arrow).
The data are reported as a mean (± standard deviation) for values measured on a continuous scale, including the IKDC outcome scores. The statistical analysis focused on the outcome scores of the group with an MPFL tear compared with the scores of those without a tear. A t test was used to compare the means in these 2 groups with a critical alpha value of 0.05.
Results
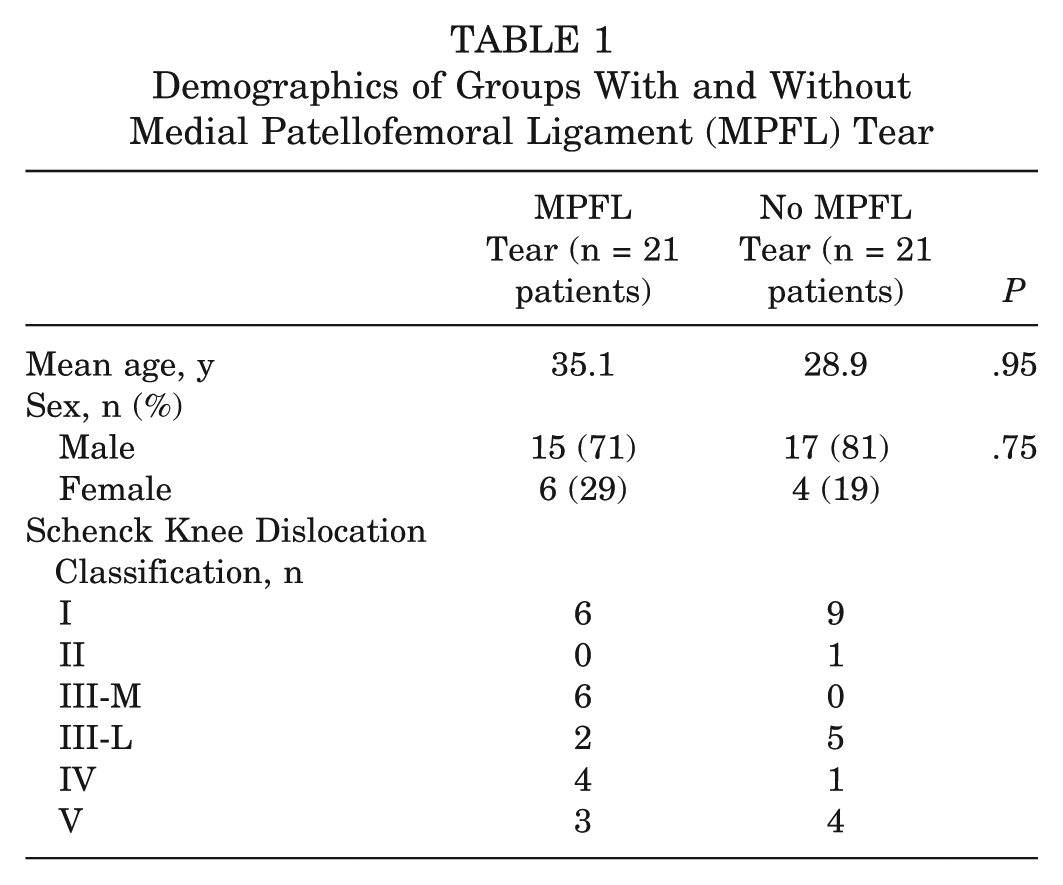
Data collection revealed 51 MLKI patients who underwent surgical reconstruction by one or both of the senior surgeons (M.J.S., B.A.L.). Thirty patients (59%) had an MPFL tear on preoperative MRI. Of these, 9 were lost to follow-up rather than not eligible for 2-year follow-up, leaving 21 patients available for inclusion in our study (30% lost to follow-up). The patients were 15 men and 6 women with a mean age of 35.1 years (range, 20-52 years). When subjects were assessed according to the Schenck Knee Dislocation (KD) Classification, there were 6 KD I injuries, 0 KD II, 6 KD III-M, 2 KD III-L, 4 KD IV, and 3 KD V. Postoperative subjective IKDC scores were obtained in patients with MPFL tear at a mean 3.2 years (range, 2.0-4.8 years) and in patients without MPFL tear at a mean 3.1 years (range, 2.0-5.0 years). The 2 groups were similar in demographics (Table 1). The group without MPFL tear had an average IKDC score of 79.4 ± 16.1, whereas the group with MPFL tear had an average score of 65.5 ± 22.9 (P = .07) (Figure 2).
Demographics of Groups With and Without Medial Patellofemoral Ligament (MPFL) Tear
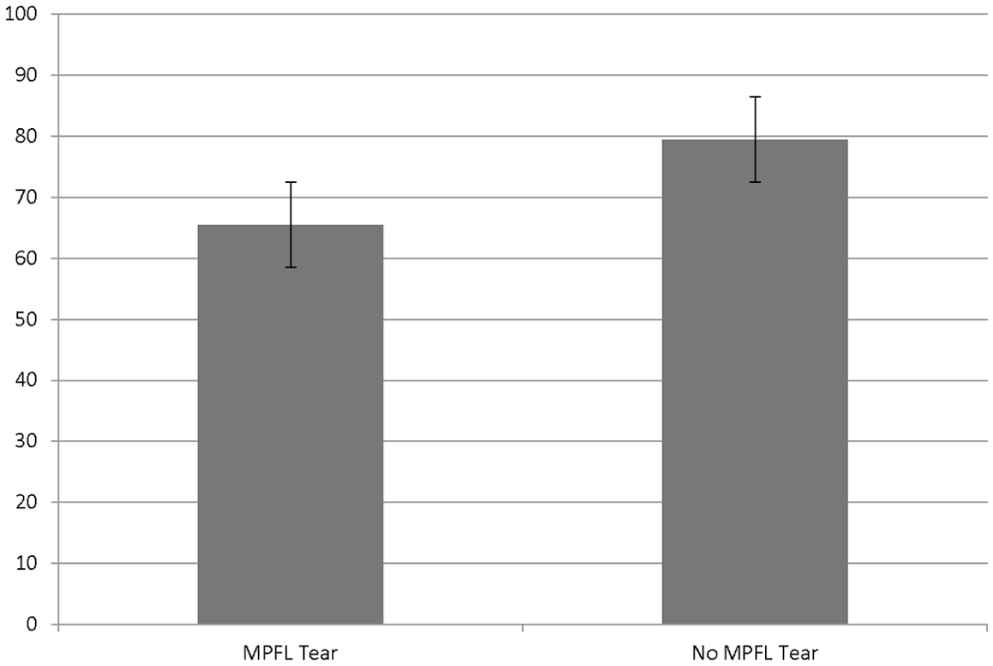
Mean International Knee Documentation Committee (IKDC) outcome scores (± SD) in patients with a medial patellofemoral ligament (MPFL) tear and those without an MPFL tear.
Of the 21 patients with an MPFL tear, the MPFL tear was classified as complete in 13 (62%), high-grade partial in 5 (24%), and partial in 3 (14%) knees. Sixteen of 21 MPFL tears (76%) occurred at the proximal third, with the remainder exhibiting diffuse signal abnormality consistent with tearing throughout the length of the MPFL. The superficial medial collateral ligament (MCL) was torn in all patients with MPFL tears. Only 1 patient in the group without MPFL tears had involvement of the superficial MCL. The patellar or lateral femoral condyle bone bruises that are typically seen on MRI after patellar dislocation were not identified in any of the patients. The mean C-D ratio was 1.0 (range, 0.6-1.3) in the MPFL group and 1.0 (range, 0.6-1.4) in the group without MPFL tear. Three patients had patella alta (C-D ratio, >1.2). Trochlear dysplasia (grade A) was present in 2 patients in both the MPFL tear group and the non-MPFL tear group. None of these patients had any patellofemoral instability symptoms. Ten patients underwent repair (n = 2) or reconstruction (n = 8) of the MCL at the time of MLKI reconstruction, including 3 KD I, 5 KD III-M, and 2 KD IV injuries. Those patients requiring MCL reconstruction were treated by use of an Achilles allograft. The allograft was secured using a 3-point fixation technique (femoral, proximal tibia, distal tibia) and posteromedial capsule imbrication. Specific repair or reconstruction of the MPFL was not performed on any of these patients. However, the MCL repair certainly could have affected the MPFL. All patients followed a standardized rehabilitation protocol as described by Fanelli et al. 10 This protocol involved a brace locked in full extension for 5 weeks and then progressive range of motion thereafter. Patients were toe-touch weightbearing for 5 to 6 weeks and then progressed to weightbearing as tolerated, with no hamstring activation for 4 to 6 months if the posterior cruciate ligament was involved.
At mean follow-up of 3.6 years (range, 2.0-5.7 years), only 1 of 21 patients (5%) complained of patellofemoral instability symptoms. This patient had a high-grade partial tear along the entire length of the MPFL in the setting of a KD III-L injury with no repair or reconstruction performed on the MCL. The patient described an occasional subluxation with everyday activities but did not experience a patellar dislocation. There were no predisposing factors, including no patella alta (C-D ratio of 0.92), trochlear dysplasia, increased femoral anteversion, genu valgum, pes planus, or secondary hyperlaxity. In this case, surgery included anterior cruciate ligament, posterior cruciate ligament, fibular collateral ligament, and posterolateral corner reconstructions. The remaining 20 of 21 (95%) patients, when contacted by telephone, denied experiencing any sensation of patellofemoral instability, patellar subluxation, or dislocation.
Discussion
Numerous articles in the orthopaedic literature have addressed MLKIs, but to our knowledge, this is the first to evaluate MPFL tears in the multiligament injured knee.11-16,20,22 The goals of this retrospective review were to (1) identify the prevalence of MPFL injuries in surgically reconstructed MLKIs, (2) determine whether MPFL injuries lead to recurrent instability, and (3) determine whether patients with MPFL tears have inferior clinical and functional outcomes compared with patients without MPFL tears in the setting of MLKI reconstruction. In this cohort, we report a relatively common prevalence of MPFL tear (59%), uncommon sequelae of patellofemoral instability without MPFL treatment (5%), and no significant difference in functional outcomes scores compared with matched patients without MPFL injury in the setting of surgical reconstruction for MLKI.
Limitations of this study include the retrospective review, which contains a relatively small cohort of surgically treated patients. However, MLKIs are relatively uncommon, and to our knowledge this is the largest series of clinical outcomes in patients with MPFL tears in the setting of MLKI. In addition, we did not compare this cohort with a group of patients with an MLKI and an MPFL tear who did not undergo any surgical treatment. The MRI studies were read by 1 radiologist using a classification of MPFL tears that has not yet been validated. No current, accepted classification of MPFL tears exists. However, in 2010, Balcarek et al 2 also evaluated the magnetic resonance characteristics of the MPFL after patellar dislocations. In this study, 48.6% of MPFL injuries were classified as partial tears.
In the group of patients studied here, an MPFL tear was found to occur frequently (59%) in the multiligament injured knee. Although a number of studies have reported recurrent instability or pain in over half of the patients treated without surgery after an initial patellar dislocation, the untreated MPFL tears in this MLKI cohort rarely led to recurrent instability.1,3,5-7,17,23,24,28 Nikku et al 24 reported recurrent patellar subluxation or dislocation in 30.4% of patients within the first 2 years after initial patellar dislocation.
The current study demonstrated recurrent instability in only 1 patient (5%) with MPFL tear in MLKI. None of the patients in this cohort had the typical findings associated with a first-time patellar dislocation, including bone bruises, chondral injury, or osteochondral fractures. The associated injuries to the cruciate and/or collateral ligaments may spare the articular cartilage and subchondral bone from damage. The subsequent lack of recurrent patellofemoral instability could be explained by this altered mechanism of injury, lack of predisposing factors (patella alta and trochlear dysplasia), and the robust healing response (scar formation) associated with a multiligament injury. Also, 10 patients underwent repair or reconstruction of the MCL, which could have inadvertently affected the MPFL femoral attachment. This injury pattern that involves the origin of the MCL and MPFL may be different than an isolated patellar dislocation. Interestingly, the single patient who experienced patellofemoral instability had a KD III-L injury and did not undergo repair or reconstruction of the medial-sided structures. The MRI did show some signal change of the superficial MCL, but it was functionally intact and stable on examination.
Patients with MPFL tear did not have significantly different IKDC scores than patients without MPFL tears. However, the magnitude of difference is clinically important (14 points on IKDC). This study is likely underpowered for this comparison, possibly revealing a type II error. The MPFL-injured group had a higher percentage of KD III-M and KD IV injuries than the non-MPFL-injured group. This difference could signify a higher level of knee trauma and account for the lower IKDC scores. A systematic review of the literature regarding MLKIs by Levy et al 19 demonstrated that operative treatment of MLKIs resulted in higher mean Lysholm and Tegner scores when compared with nonoperative treatment. There was also a higher percentage of excellent/good IKDC scores (58% vs 20%) in the surgically treated patients versus those treated nonoperatively at a mean follow-up of 51 months. 29 While the evidence presented in the literature suggests that operative reconstruction of MLKI leads to improved outcomes, our study demonstrates that MPFL tears need not be addressed surgically at the time of reconstruction.
In conclusion, MPFL tears occur frequently in patients with MLKI but rarely cause clinical symptoms of instability. The mechanism of an MPFL tear and the healing response in the multiligament injured knee are likely different than an isolated patellar dislocation. In the majority of cases, MPFL tears do not need to be addressed at the time of multiligament reconstruction surgery.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.