
Abstract
Background:
Chronic lateral epicondylitis (LE) induces cell apoptosis and autophagy, which lead to the reduction of tendon-derived cells in the torn tendon. Our previous study has shown that ultrasound-guided autologous tenocyte injection (ATI) to the torn tendon in patients with chronic resistant LE significantly improves pain, function, and structural repair at 1 year. This report is the continued assessment of the clinical outcomes of these patients at mean 4.5-year follow-up.
Hypothesis:
Improvements in LE clinical function and structural repair after ATI will be maintained at mean 4.5-year follow-up.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients with severe refractory LE underwent clinical evaluation and MRI before intervention. A patellar tendon needle biopsy was performed under local anesthetic, and tendon cells were expanded by in vitro culture. Autologous tenocytes were injected into the central tendinopathy identified at the common extensor tendon origin under ultrasound guidance on a single occasion. Patients underwent serial clinical evaluations for up to 5 years after ATI, including the visual analog scale (VAS) for pain, Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH), Upper Extremity Functional Scale (UEFS), and grip strength. Post-ATI MRI scanning was performed at 1 year and final follow-up.
Results:
A total of 16 patients (9 male, 7 female), aged between 37 and 63 years, were included in the study. The mean duration of symptoms before study recruitment was 29.24 months (range, 6-240 months). One patient elected to proceed to surgery 3 months after ATI due to reinjury at work, and 1 patient died of prostate cancer with metastases during the follow-up period. The mean final follow-up time for the remaining 15 patients was 4.51 years (range, 3.08-5.17 years). No complications were observed at the patellar tendon biopsy site for any patient. No adverse events, infection, or excessive fibroblastic reactions were observed in any patient at the injection site. Clinical evaluation revealed significant (P < .001) improvement in mean VAS pain score from 5.73 at initial assessment to 1.21 (78% improvement) at final follow-up. Mean QuickDASH, UEFS, and grip strength scores also significantly (P < .001) improved from initial assessment to final follow-up (from 45.88 to 6.61 [84%], from 31.73 to 9.20 [64%], and from 19.85 to 46.60 [208%], respectively). There was no difference in mean QuickDASH and UEFS scores at 1 year and final follow-up (P > .05); however, grip strength continued to improve (P < .001). A validated MRI scoring system indicated that the mean grade of tendinopathy at the common extensor origin improved significantly (P < .001) from initial assessment (4.31) to 1 year (2.88) and was maintained (P > .05) at final follow-up (2.87). At final follow-up, 93% of patients were either highly satisfied or satisfied with their ATI treatment.
Conclusion:
ATI significantly improved clinical function and MRI tendinopathy scores for up to 5 years in patients with chronic resistant LE who had previously undergone unsuccessful nonsurgical treatment. This study provides evidence for the midterm durability of ATI for treatment of LE tendinopathy.
Lateral epicondylitis (LE) is a common musculoskeletal complaint with a population prevalence of 1% to 3%. 3 Generally, LE is a self-limiting and mild condition, but it may cause persistent symptoms in some patients. 21 Severe and chronic cases are a common cause of occupational and sporting disability and frequently impair activities of daily living.28,29 The cost of LE by loss of productivity and inefficient health care utilization under current treatment models is high.24,37 Finding more effective evidence-based treatment options for LE is crucial to optimizing benefits for both patients and the health system.
Historically, nonsurgical management of LE has included rest, nonsteroidal anti-inflammatory drugs (NSAIDs), counterforce bracing, eccentric strengthening and other rehabilitation exercises, and corticosteroid or plasma-rich protein injections. Initial nonsurgical treatments result in favorable outcomes in approximately 80% of patients at 6 months and 90% of patients at 1 year, with only a small number of patients needing to consider surgery.6,7,32,43,46 To further improve the outcomes of nonsurgical strategies and reduce the need for surgery, the development of alternative nonsurgical treatment options for patients with chronic resistant LE tendinopathy is needed.
Lateral epicondylitis is characterized by increased numbers of fibroblasts, vascular hyperplasia, and disorganized collagen in the early phase. 1 With continued reinjury and microrupture, the accumulated pathological changes in the extensor carpi radialis brevis tendon can result in healing failure and tendon tear. Histological examination of these advanced cases has revealed an increase of extracellular matrix and collagen bundle breakdown and the induction of tenocyte apoptosis and autophagy, which lead to the reduction of functional tendon-derived cells in the central tear site.32,51 Hence, we propose that the injection of functional tenocytes into the torn tendon may replenish the functional tendon-derived cell population and thereby assist repair of the damaged tendon.
This enhanced understanding of the pathogenesis of tendinopathy has led us to the development of the novel treatment of autologous tenocyte injection (ATI). Subsequently, we have evidenced the safety and improved tendon repair biology (histology and biomechanics) by ATI in a number of tendinopathy animal models.9,10 Clinically, we have previously reported no biopsy or injection site complications and have found improved clinical function and tendon structure at 1 year in patients with chronic resistant LE tendinopathy treated by ATI. 50 Herein we present the mean 4.5-year clinical function and structure outcomes for these patients.
Methods
Patients
The trial initially included 16 patients (9 male, 7 female), aged between 37 and 63 years, who were diagnosed with LE that was confirmed by ultrasound and/or magnetic resonance imaging (MRI) (Table 1). Of the original cohort of 20, 2 patients withdrew after pretreatment evaluation due to unrelated medical reasons, 1 withdrew after patellar tendon biopsy due to personal circumstances, and 1 had received surgery at 3 months after ATI injection (Figure 1). All patients had partial-thickness tears (of varied severity) of the extensor carpi radialis brevis tendon as well as a >6-month history of tendinopathy symptoms and had failed nonsurgical treatment including counterforce bracing, physical therapy, and 1 or more corticosteroid injections. All patients were previously elected for surgery. The mean ± SE duration of symptoms for all 16 patients was 29.24 ± 14.26 months. Of note, after removal of a significant outlier (240 months, variable pain), the mean symptom duration was 16.06 ± 2.69 months. Exclusion criteria included a history of elbow surgery, corticosteroid injection within 3 months, an unrelated injury in the ipsilateral upper limb including nerve compression and arthritis, cervical spondylosis, mental illness, pregnancy, professional sports participation, and pursuit of compensation claims. This trial received institutional ethics approval (Sir Charles Gairdner Hospital Human Research Ethics Committee: trial no. 2007-116) and was enrolled with the Australian New Zealand Clinical Trials Registry (ACTRN12607000402448).
Participant Demographics
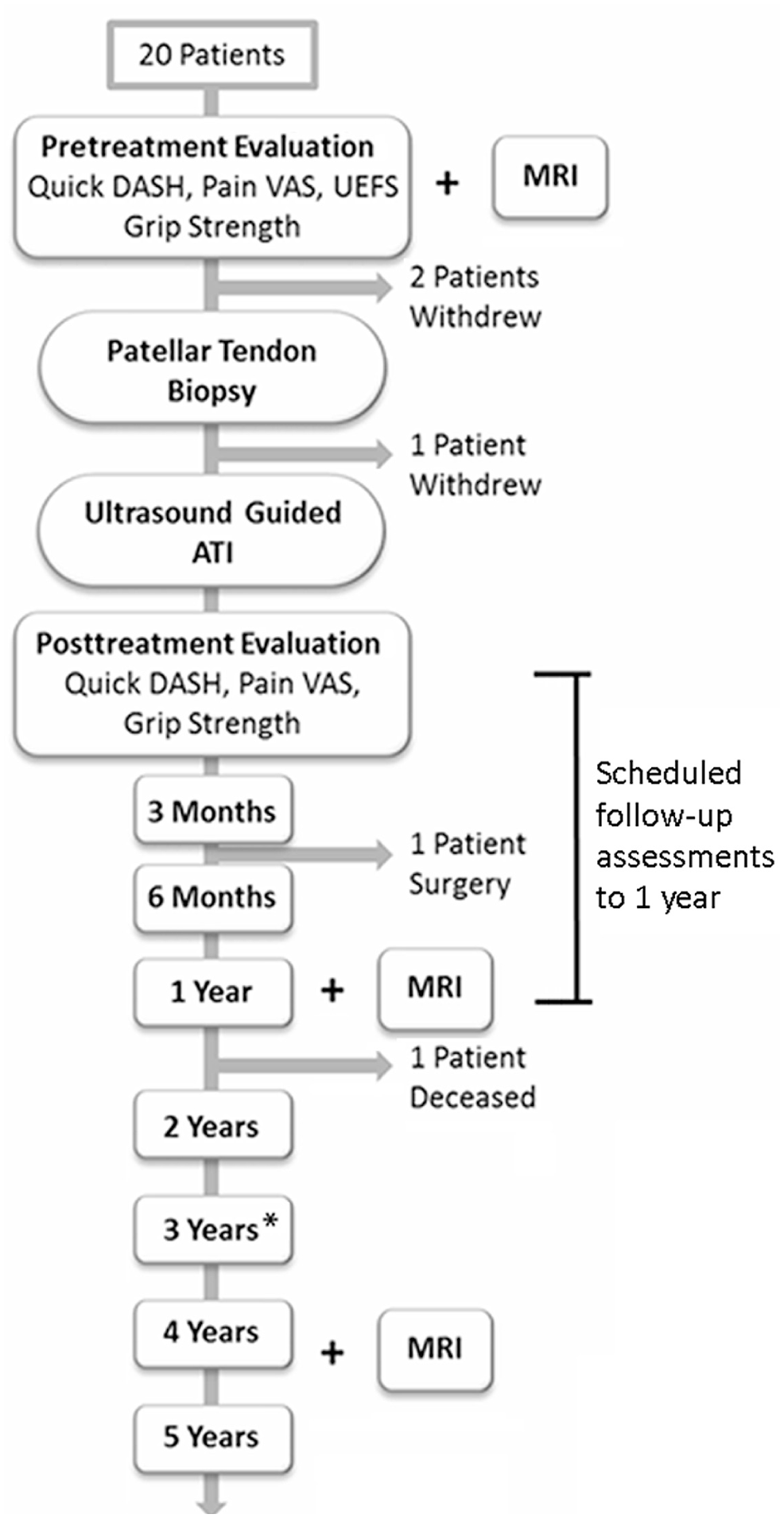
Clinical trial study design flow chart detailing long-term follow-up. The mean final follow-up time was 4.61 years (range, 4.08-5.17 years). *The final follow-up for 1 patient was conducted at 3.08 years (outlier). ATI, autologous tenocyte injection; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand; UEFS, Upper Extremity Functional Scale; VAS, visual analog scale.
Treatment
ATI is a 2-stage procedure that involves patellar tendon biopsy followed by a single injection of cultured autologous tenocytes to the site of LE tendinopathy under ultrasound guidance.
All patellar tendon needle biopsies were performed by a single surgeon (A.W.) in the same outpatient clinic under local anesthetic using a Temno Evolution biopsy needle (14 gauge × 11 cm; CareFusion Corp). The biopsy procedure obtained a 3 × 1-mm strip of tendon from the superficial surface of the patellar tendon. Tenocyte culture was performed at Orthocell Ltd under the Australian Therapeutic Goods Administration’s Code of Good Manufacturing Practice (GMP)—Human Blood and Tissues. As part of the GMP protocol, a 60-mL sample of venous blood was taken from each patient at the time of biopsy for infection and viral screening including human immunodeficiency virus, hepatitis B and C, human T-lymphotropic virus, and syphilis. Only patients testing negative for these panels were accepted for treatment.
As previously described, the characterization of tendon-derived cells was evaluated with a portion of patient cells from implantation using flow cytometry for cell surface markers (CD18, CD34, CD44, CD45, CD90, CD106, CD146, and STRO-1) and real-time polymerase chain reaction (PCR) for transcription and matrix markers (aggrecan, type I collagen, type III collagen, decorin, microfibril-associated glycoprotein 2 [MAGP2], Mohawk, scleraxis, and transforming growth factor–β [TGF-β]) to ensure the purity and potency of tendon cell phenotype. 50 In brief, the implanted tendon-derived cells are a tendon lineage–specific cell population that differs from bone marrow–derived mesenchymal stem cells and that expresses tendon matrix proteins (ie, coll-I to coll-III ratio >1.5).
Approximately 3 weeks after biopsy, up to 2 mL of autologous tenocytes (2-5 × 106 cells/mL) suspended with 10% autologous human serum was injected under ultrasound guidance by a single musculoskeletal radiologist (W.B.) into the extensor carpi radialis brevis tendinopathy site using an 18-gauge needle.
Posttreatment Rehabilitation
Patients were advised to rest for 2 days and restrict activity to light household or office duties for 4 weeks. Patients were instructed on standard forearm extensor muscle stretches that were to be performed 4 times a day. Pain medication (acetaminophen) was prescribed as required (1000 mg every 8 hours). No supervised physical therapy programs or formal strengthening exercises were prescribed. Work and sport participation restrictions were removed 4 weeks after ATI.
Clinical Assessment
Patients were assessed by a qualified exercise physiologist and the treating orthopaedic surgeon (A.W.) at the same outpatient clinic. Several clinical scores were used to evaluate patients before and after treatment at 1, 2, 3, 6, and 12 months and at final follow-up (mean, 4.5 years). These included 3 validated subjective measures: (1) the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) to assess physical function and symptoms, 5 (2) the Upper Extremity Functional Scale (UEFS) to assess the effect of upper extremity disorder on function, 39 and (3) the visual analog scale (VAS) to assess elbow pain. 40 Pain was assessed as per the American Shoulder and Elbow Surgeon Scale (ASES), which asks patients to rate their pain in the last week on a scale from 0 (no pain) to 10 (worst pain ever) for 5 scenarios: when at its worst, at rest, lifting a heavy object, when doing repeated elbow movements, and at night. The final VAS pain score was calculated as the mean response to the 5 scenarios. Grip strength was measured using the Jamar dynamometer (Sammons Preston Rolyan) on the No. 2 setting with the patient’s elbow in full extension and neutral forearm rotation as an objective measure of function. Patient satisfaction was assessed on a scale of 0 (not at all satisfied) to 10 (highly satisfied) at final follow-up.
MRI Assessment
The MRI assessment was performed by a single radiologist (W.B.) before treatment, 12 months after treatment, and at final follow-up using an Achieva 3.0-T MRI machine (Phillips Healthcare). An 8-channel coil was used with patients in the prone position and the affected arm extended in front with the forearm supinated. An experienced musculoskeletal radiologist evaluated MRI results for the extent of tendinopathy and tendon tear at the origin of the common extensor tendon. All MRI images were graded in accordance with the validated scoring system for chronic lateral epicondylitis. 49 The scoring system graded both the tear (score of 1-3) and tendinopathy (score of 1-3), giving a final combined score between 2 and 6 (see the Appendix, available online at http://ajsm.sagepub.com/supplemental). A final score of 2 indicated a tear less than 25% of the tendon thickness and complete homogeneous low-intensity or mild focal increased tendon signal on MRI; a final score of 6 indicated severe tendinopathy with a tear greater than 50% of the tendon thickness and generalized increased signal intensity on MRI.
Statistical Analysis
Primary data analysis was performed on all 16 patients, and the effect of patients lost to follow-up was assessed. All data are expressed as mean ± SE. Outliers were examined using the Grubb test. P values less than .05 were determined as significant. Reporting included percentage improvement in mean outcome data between follow-up time points. Changes in patient outcomes over time were evaluated using a multilevel, mixed-effects linear regression estimation. The fitted model used between-patient variability as a random effect. All statistical analyses were performed with Stata/IC version 13 (StataCorp LP).
Results
Participant Follow-up
Data at 3- to 5-year follow-up were available for 15 patients. The 2 patients not assessed at the final follow-up included one 44-year-old female patient who underwent surgery 3 months after ATI treatment (after reinjury to the treated tendon by a lifting incident after returning to work) and 1 patient who died after the 1-year assessment (Figure 1). The cause of death for this patient was prostate cancer with lung metastases and was considered by the medical assessment panel to be unrelated to the study treatment. Final follow-up was performed on these 15 patients at a mean 4.51 years after treatment (range, 3.08-5.17 years). One patient recruited at a later time point underwent the final follow-up 3.08 years after ATI treatment (removal of this outlier would give a mean 4.61 years of follow-up and range of 4.08-5.17 years).
Complications
No complications were observed at the patellar tendon needle biopsy site for any patient. All patients demonstrated full range of movement and imperceptible scar formation. No infection, tendon rupture, hematoma, nerve injury, or ossification was observed at the elbow injection site.
Clinical Assessment
Significant improvements from baseline (preintervention) were noted to be maintained in all clinical scores for up to 5 years after treatment (all P < .001) (Table 2).
Summary of Pre- and Posttreatment Clinical Assessments a
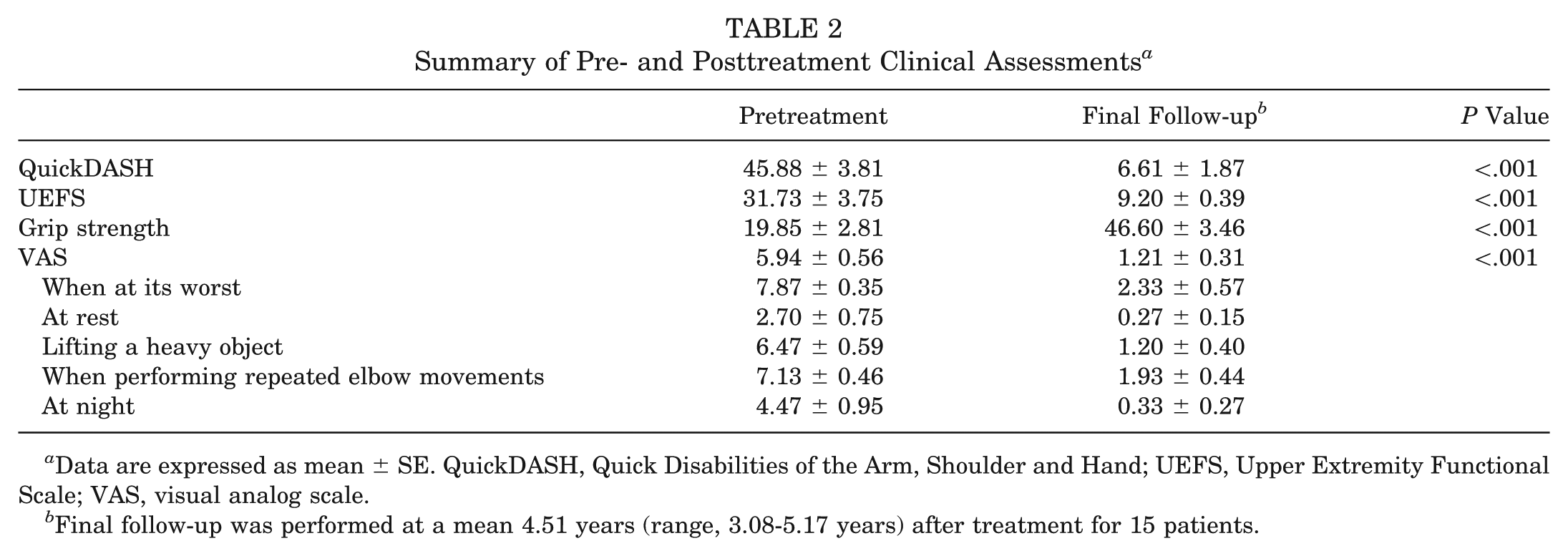
Data are expressed as mean ± SE. QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand; UEFS, Upper Extremity Functional Scale; VAS, visual analog scale.
Final follow-up was performed at a mean 4.51 years (range, 3.08-5.17 years) after treatment for 15 patients.
Before intervention, the VAS pain score (mean ± SE) was 5.94 ± 0.56. The VAS pain score improved by 86% (0.76 ± 0.14; P < .001) at the 1-year follow-up. At final assessment, the VAS pain score had improved by 78% (1.21 ± 0.31), a significant (P < .001) improvement from baseline but not significantly (P > .05) different than the 1-year results (Figure 2C).
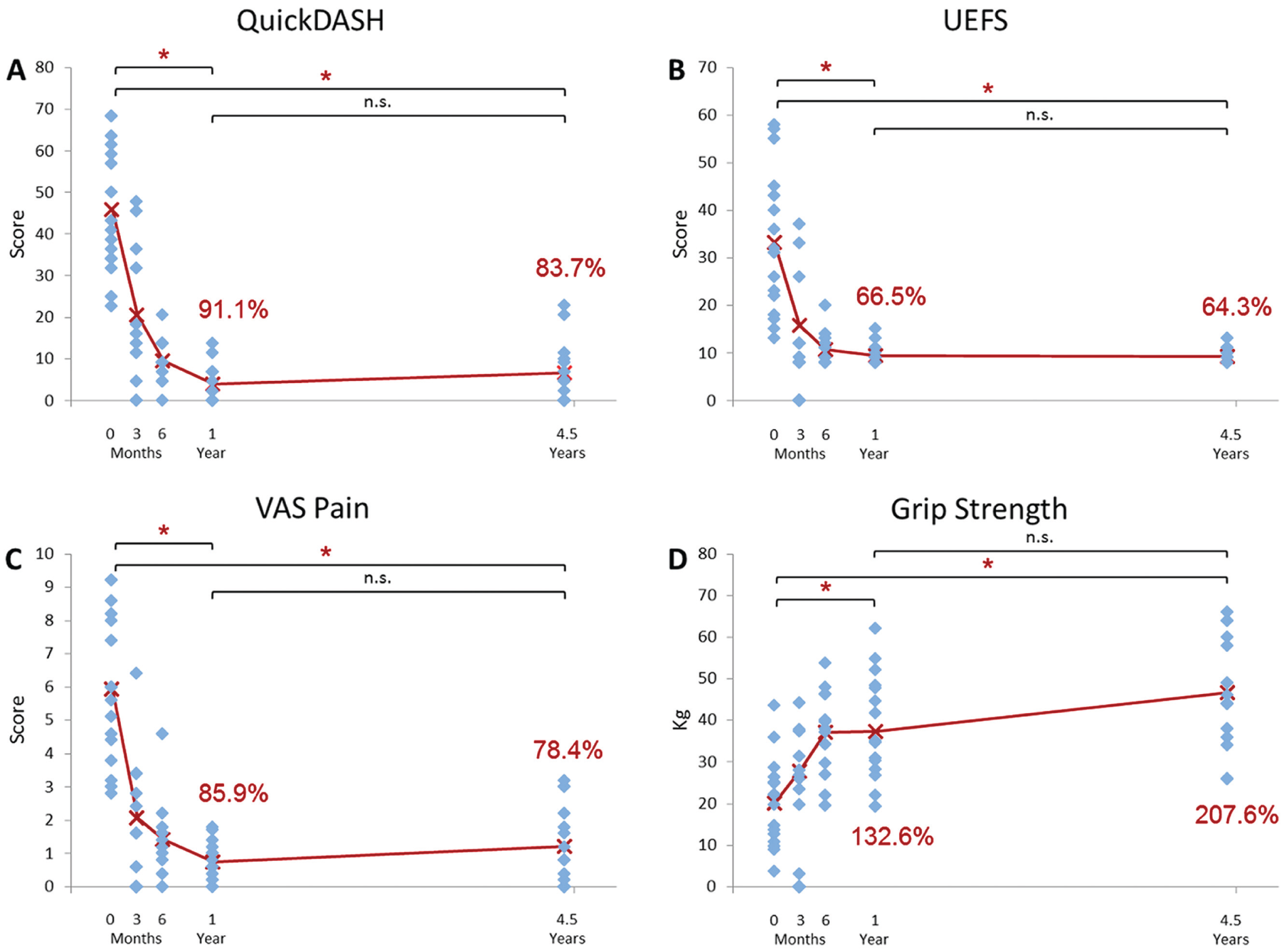
Assessment of pain and functionality at pretreatment assessment and 1-month to mean 4.5-year final assessment. Each diamond represents a patient score at the relevant time after autologous tenocyte injection. Note that some patients’ results may overlap. *Significant difference in scores compared with baseline (P < .001); n.s., not significantly different (P > .05). (A) Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) score assessing the ability to perform daily tasks showed a mean 83.7% improvement at final follow-up. (B) Upper Extremity Functional Scale (UEFS) to assess the effect of upper extremity disorder on function improved on average by 64.3%. (C) Visual analog scale (VAS) pain score improved on average by 78.4%. (D) Grip strength (kilograms) increased on average by 207.6%.
Mean QuickDASH score before intervention was 45.88 ± 3.81, improving by 91% at 1 year (mean 3.84 ± 1.05; P < .001) and 84% at final follow-up (mean 6.61 ± 1.87; P < .001) (Figure 2A). There was no statistical difference (P > .05) in QuickDASH scores between the 1-year and final follow-up. UEFS demonstrated a similar outcome, with a 66% improvement from baseline (mean, 31.73 ± 3.75) at 1 year (mean, 9.40 ± 0.52; P < .001) being maintained to a 64% improvement at final follow-up (mean 9.20 ± 0.39; P < .001 compared with baseline) and with no difference (P > .05) between 1-year and final follow-up results (Figure 2B). Grip strength scores continued to improve from baseline (19.85 ± 2.81) beyond the 1-year follow-up improvement of 132.6% (mean, 37.38 ± 3.30 kg; P < .001), with a 208% improvement at final follow-up (mean 46.60 ± 3.46 kg; P < .001) (Figure 2D).
MRI was used to evaluate the extent of tendinopathy and tear at the origin of the common extensor tendon (Figure 3). Before intervention, the mean MRI score was 4.31 ± 0.28. By 1 year the MRI score had significantly (P < .001) improved to 2.88 ± 0.18, and this was maintained for up to 5 years (mean 2.87 ± 0.19; P < .001). All but 2 patients had identical 1-year and final follow-up MRI scores. As illustrated in Figure 4, one patient demonstrated further improvement in the tendinopathy score component at a final follow-up of 4.3 years (scored 2 at 1 year and 1 at 4.3 years; total score improved from 3 to 2). The second patient progressed from a tear score of 1 to 2 due to MRI evidence of an extremely small focus of partial-thickness tearing at the deep aspect of the extensor carpi radialis brevis tendon, which was, however, less evident than at the pretreatment study. Of note, this patient has continued to play tennis.
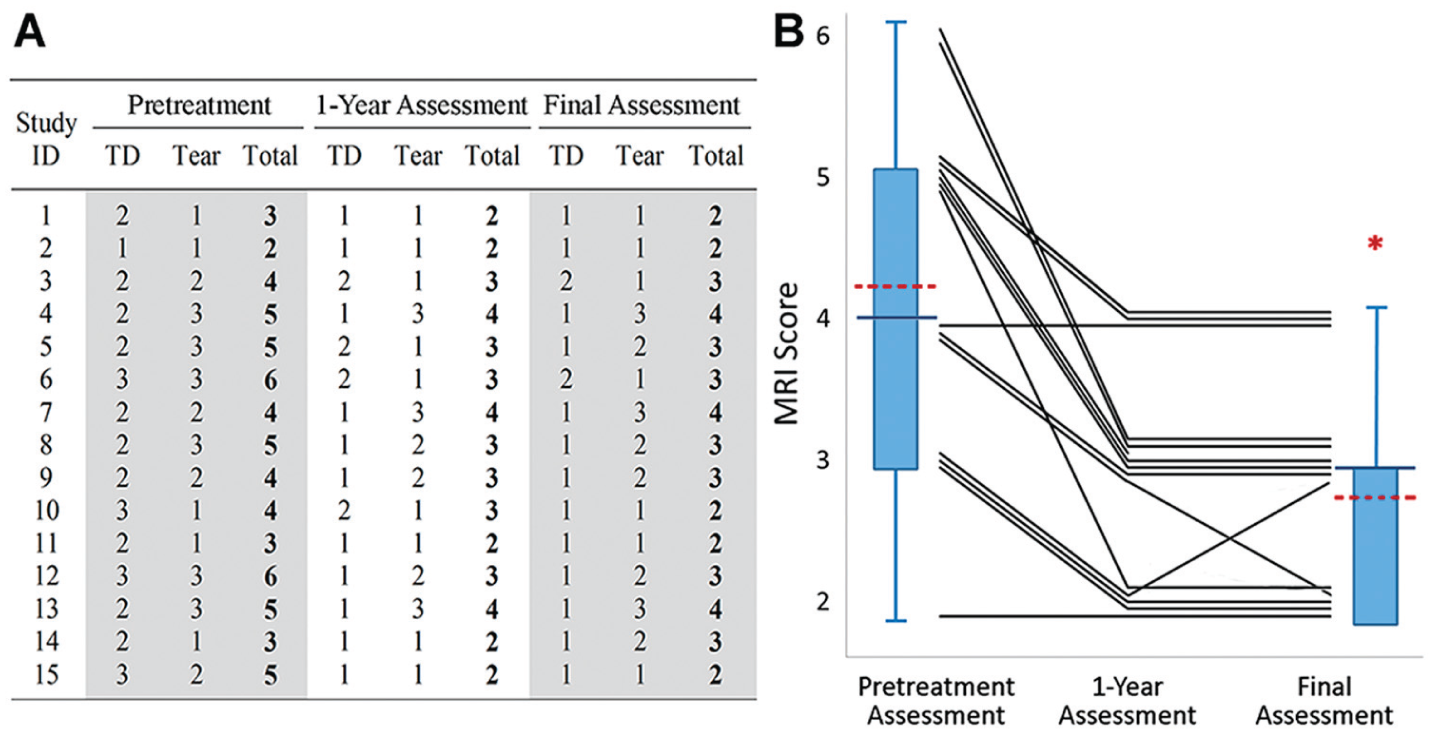
Individual magnetic resonance imaging (MRI) scores at pretreatment, 1 year, and final assessment (mean, 4.5 years). (A) Individual participant tendinopathy (TD; 1-3), tear (1-3), and total MRI scores (2-6 [best to worst]). (B) Individual total MRI scores are plotted, with box plots demonstrating the mean (dotted line), median (solid line), and interquartile range (box) of scores before and after autologous tenocyte injection. Scores were significantly (*P < .001) improved after treatment.
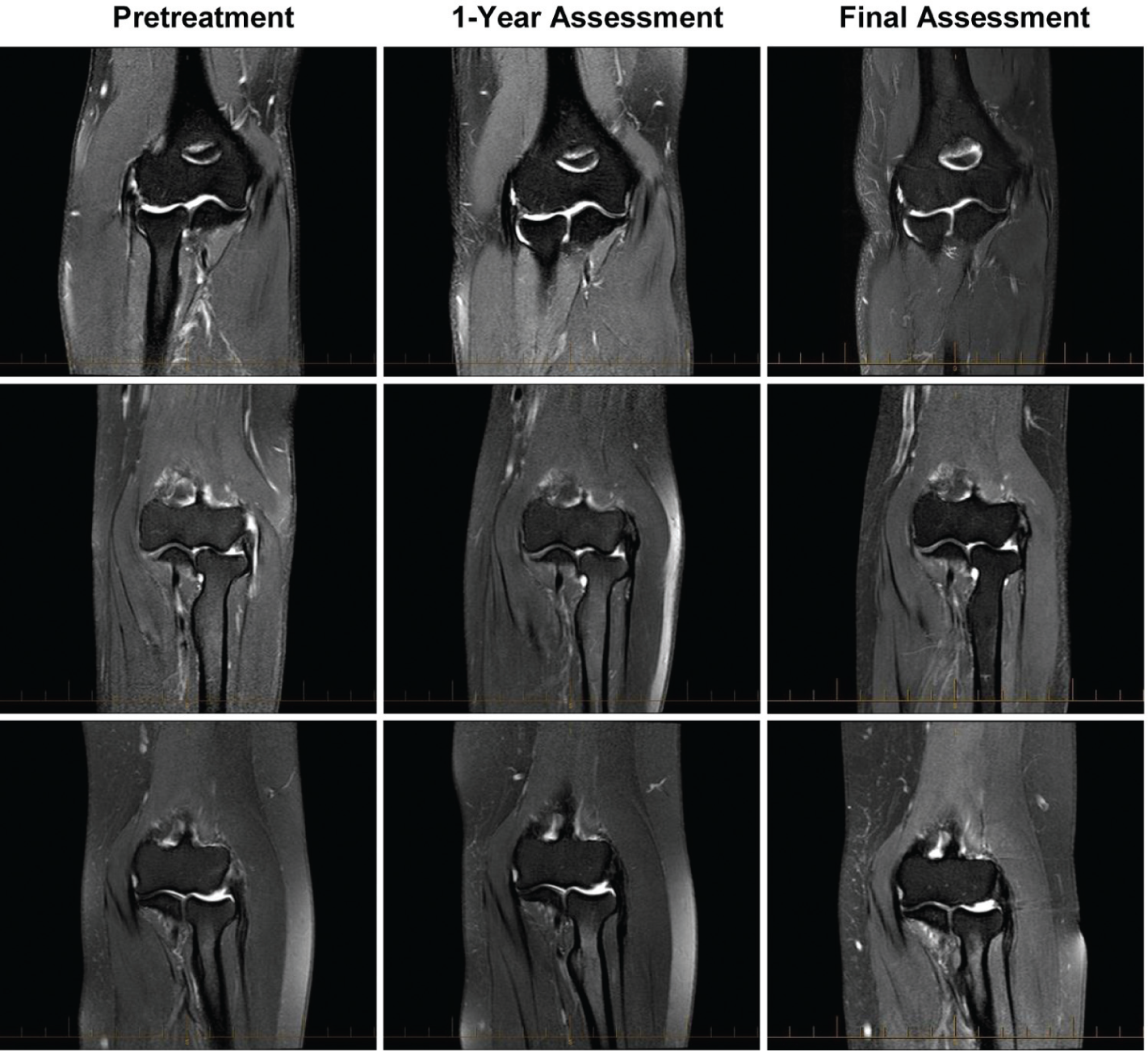
Magnetic resonance imaging (MRI) results after autologous tenocyte injection from 3 patients at pretreatment, 1 year, and final assessment. Top row: Patient 7’s score was 4 (tendinopathy [TD], 2; tear, 2) at pretreatment, 4 (TD, 1; tear, 3) at 1 year, and 4 (TD, 1; tear, 3) at long-term final assessment (4.5 years). Middle row: Patient 12’s score was 6 (TD, 3; tear, 3) at pretreatment, 3 (TD, 1; tear, 2) at 1 year, and 3 (TD, 1; tear, 2) at long-term final assessment (4.3 years). Bottom row: Patient 10’s score was 4 (TD, 3; tear, 1) at pretreatment, 3 (TD, 2; tear, 1) at 1 year, and 2 (TD, 1; tear, 1) at long-term final assessment (4.3 years). Total MRI scores ranged from 2 to 6 (best to worst).
At final follow-up, 93% (n = 14) of patients were either highly satisfied or satisfied with their ATI treatment outcome. Only 1 patient, with tear progression, was unsure of his or her satisfaction (score 5). Most patients (10/15) also reported participation in a variety of physical activities that are common aggravators of pain for LE patients, including darts, tennis, weight training, and gardening.
Discussion
Although LE tendinopathy is a self-limiting condition, surgical treatment is often the only option for chronic resistant LE tendinopathy that has failed conservative treatment. Improved understanding of the pathogenesis of LE tendinopathy has led us to the development of ATI, a novel nonsurgical approach.1,8,22,31 Our previous 1-year follow-up study of ATI showed that patients with chronic LE who have failed other nonsurgical treatment have significantly improved clinical function and structure at the origin of the common extensor tendon. The current study further confirmed that ATI improves clinical function and MRI tendinopathy scores for up to 5 years. QuickDASH, VAS pain, UEFS, and grip strength scores at final follow-up were significantly (P < .001) improved from baseline yet were similar to 1-year results (P > .05), except for grip strength, which continued to improve (208%; P < .001) at final follow-up. Overall, the outcomes of this pilot study are promising for the mid- to long-term durability of ATI.
Finding alternative, effective nonsurgical treatments for chronic resistant LE tendinopathy is increasingly important. Evidence is now mounting against corticosteroid use compared with conservative regimens.13,14,42,43 Biologically, corticosteroids do not address the underlying pathobiology of tendinopathy and may result in induction of cell apoptosis and breakdown of collagen and matrix.31,34,36,41 Platelet-rich plasma (PRP) injection has also gained popularity as a treatment option, but although initial studies were encouraging, results from clinical trials are conflicting and a recent systematic review provides strong evidence against PRP for chronic LE.15-18,20,25,30,33,38,47 Interestingly, ultrasound-guided percutaneous needle electrolysis, a technique that stimulates increased native tendon cell activity and repair of the LE region, has recently reported some success in pain, DASH, satisfaction outcomes, and null recurrence at 1-year follow-up. 48 Of note, most other injection technique studies have failed to conduct more than 1 year of follow-up. A recent randomized, double-blind, controlled trial comparing injection therapies in LE found that neither glucocorticoid nor PRP was superior to saline in pain reduction. 25 In contrast to glucocorticoid, PRP, autologous blood, and other injections, which have demonstrated biological nonspecificity, the ultrasound-guided injection of autologous skin-derived tenocyte-like cells has demonstrated significant pain and function improvement in a randomized, double-blind, controlled tendinopathy trial. 11
This study suggests that specific tendon lineage cells (tenocytes or tenocyte-like) may respond better to endogenous factors and mechanical loading in vivo to enable improved tendon repair.2,23,45,52
Surgical options are generally reserved for patients with tendinopathy resistant to nonsurgical therapies. Numerous surgical variants have been described in the literature, including a number of open and arthroscopic approaches.4,12,19,26,27,35,44,48 The clinical outcomes of ATI appear comparable with various surgical interventions reported in the literature. Solheim et al 44 reported 4-year results of a 305-case series of LE with arthroscopic and open surgical treatment. The baseline assessments of these cases before surgery were very similar to our cohort, in which patients have failed nonsurgical therapies, including injection techniques. Their mean follow-up of 4 years is similar to our mean 4.5-year follow-up. While both the traditional open surgery and arthroscopic approach provided an effective treatment for the resistant LE, our mean ATI QuickDASH score of 6.6 points at final follow-up is almost identical to the surgical outcomes of Solheim et al 44 (6.2 and 6.7 for arthroscopic and open surgery, respectively).
In the current study, the mean VAS pain score in patients having ATI was 1.2 at final follow-up, which is slightly better than those reported in 33 LE cases treated by both arthroscopic and percutaneous surgeries. 35 A mean grip strength (in extension) of 46.6 kg (208% increase from baseline) at final ATI follow-up in the current study is also promising in comparison to 3 other LE studies of varied surgical approach reporting mean strengths of 28, 33, and 36 kg at 6-, 10-, and 5-year follow-up, respectively.12,26,48 We hypothesize that the continued improvement in grip strength beyond 1 year may be attributable to a progression in patient activity and associated return to full use of their elbow, which thereby facilitates improved remodeling of the tendon through biomechanical stimulation.
Although our ATI findings are superior or comparable to LE surgical outcomes in the literature, study variables (eg, previous intervention) and the lack of any randomized controlled process must be considered when comparing study outcomes. 27 However, while surgical interventions report good outcomes in most patients, success is far from universal. Clinically failed cases are still not uncommon, and complications such as infection, hematoma, and nerve injury are often observed. 27 Systemic analysis in 2007 of overall function (pain, function, and return to activity), regardless of LE surgical method, reported approximately 80% good to excellent results and 9% poor/failed results—inferior figures compared with the current study. 27 Hence, less invasive alternative treatment modalities require further exploration. While our patients were informed of surgical treatment options before they chose ATI, 1 patient had surgery after ATI due to traumatic reinjury of the treated tendon in a work accident. Although our midterm durability data for ATI indicate that ATI can reduce the rate of surgical intervention in patients with chronic resistant LE, a larger cohort study and a control group to test for both natural repair and the placebo effect are needed to validate this finding. Nevertheless, significant structural and functional improvement in this study suggests that ATI is responsible for the observed clinical outcome improvements.
Cost-effectiveness is often a decisive factor in evaluating treatment options for LE tendinopathy and their effect on clinical outcomes. Comparative cost estimates of specific treatments are complicated, as surgical costs vary widely with surgeons, hospitals, health insurance policies, and states and countries. A few published studies have discussed the cost-effectiveness of treatments for LE, although none of the studies included chronic cases or the costs of specific surgeries in their analyses.24,38,46 In evaluating the timing of treatment, it is noteworthy that nonsurgical intervention (eg, clinic visits, corticosteroid injections, braces, and occupational therapy) is recommended as first-line treatment, despite the fact that most LE cases resolve within 6 months. To this end, a recent cost-effectiveness analysis of the time to surgery in treatment of LE showed that surgical intervention after the completion of 12 months of failed nonsurgical management is not cost-effective. 37 Given the success of ATI in this study in significantly improving clinical outcomes after failed nonsurgical LE interventions, and considering that only 1 patient subsequently underwent surgery, ATI may present a more clinically useful and cost-effective alternative to current nonsurgical therapies for severe resistant LE tendinopathy. It is clear that further studies of chronic severe LE are required, which should include a controlled trial and an economic analysis component to ensure that physicians have adequate information to provide patients with a cost-effective treatment.
The main limitation of this study was the lack of control group, whereby neither alternative treatment nor placebo was part of the study design. Therefore, it is not possible to assess with certainty whether the treatment was superior to other treatments or whether a placebo effect influenced the findings (patients were not blinded to their treatment). As the outcome assessors were not blinded in the study, the possibility of bias in clinical assessments should also be noted.
In conclusion, our findings showed that ATI improves the clinical function and structure of the origin of the extensor carpi radialis brevis tendon in patients with chronic resistant LE. Although this study demonstrates the durability of ATI up to 5 years, randomized controlled trials are required to determine the relative role of ATI against natural repair, other nonsurgical therapies or surgical treatments in chronic LE tendinopathy.
Footnotes
Acknowledgements
The authors thank Dr Craig Willers for his critical suggestions on the manuscript.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work is partly supported by an Australia Research Council (ARC) linkage grant NH&MR 1049440 and ARC linkage grant LP 110100581. M.H.Z. holds stock in Orthocell Pty Ltd and received a consulting fee from Orthocell for research and development. Orthocell supplied the autologous tenocyte injections used in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.