
Abstract
Background:
Isolated infraspinatus muscle atrophy is common in overhead athletes, who place significant and repetitive stresses across their dominant shoulders. Studies on volleyball and baseball players report infraspinatus atrophy in 4% to 34% of players; however, the prevalence of infraspinatus atrophy in professional tennis players has not been reported.
Purpose:
To investigate the incidence of isolated infraspinatus atrophy in professional tennis players and to identify any correlations with other physical examination findings, ranking performance, and concurrent shoulder injuries.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 125 professional female tennis players underwent a comprehensive preparticipation physical health status examination. Two orthopaedic surgeons examined the shoulders of all players and obtained digital goniometric measurements of range of motion (ROM). Infraspinatus atrophy was defined as loss of soft tissue bulk in the infraspinatus scapula fossa (and increased prominence of dorsal scapular bony anatomy) of the dominant shoulder with clear asymmetry when compared with the contralateral side. Correlations were examined between infraspinatus atrophy and concurrent shoulder disorders, clinical examination findings, ROM, glenohumeral internal rotation deficit, singles tennis ranking, and age.
Results:
There were 65 players (52%) with evidence of infraspinatus atrophy in their dominant shoulders. No wasting was noted in the nondominant shoulder of any player. No statistically significant differences were seen in mean age, left- or right-hand dominance, height, weight, or body mass index for players with or without atrophy. Of the 77 players ranked in the top 100, 58% had clinical infraspinatus atrophy, compared with 40% of players ranked outside the top 100. No associations were found with static physical examination findings (scapular dyskinesis, ROM glenohumeral internal rotation deficit, postural abnormalities), concurrent shoulder disorders, or compromised performance when measured by singles ranking.
Conclusion:
This study reports a high level of clinical infraspinatus atrophy in the dominant shoulder of elite female tennis players. Infraspinatus atrophy was associated with a higher performance ranking, and no functional deficits or associations with concurrent shoulder disorders were found. Team physicians can be reassured that infraspinatus atrophy is a common finding in high-performing tennis players and, if asymptomatic, does not appear to significantly compromise performance.
Isolated infraspinatus muscle atrophy is common in overhead athletes, who place significant and repetitive stresses across their dominant shoulders. Studies on volleyball and baseball players report infraspinatus atrophy in 4% to 34% of players7-11,17,22,27; however, the prevalence of infraspinatus atrophy in professional tennis players has not been reported. The muscle wasting is thought to be secondary to irritation of the suprascapular nerve at the spinoglenoid notch, distal to its innervation of the supraspinatus muscle. Isolated atrophy and weakness of the infraspinatus muscle occur14,27; however, the clinical relevance is unclear, with most patients reporting no pain and apparently normal shoulder function. 7 Infraspinatus atrophy has been associated with a higher level and duration of play, leading to the term cumulative neuropraxia 7 as a suggested origin.
While suprascapular nerve compression secondary to a spinoglenoid cyst is well documented,1,26 the majority of athletes with isolated infraspinatus atrophy have no identifiable cause.13,14 Postulated mechanisms include repetitive traction over the bony wall of the spinoglenoid notch attributed to hitting movements4,9 or sport-specific biomechanical demands, 18 an ossified or bifid superior transverse scapular ligament, 14 a tight posterior glenohumeral capsule resulting in intermittent compression of the suprascapular nerve by the spinoglenoid ligament at the spinoglenoid notch, or a hypertrophied spinoglenoid (inferior transverse scapular) ligament. 24 However, the exact cause of muscle atrophy remains unclear.
While cases of isolated infraspinatus atrophy has been reported in weight lifters, tennis players, 2 and newsreel cameramen, 12 previous studies on the incidence of infraspinatus atrophy focused on baseball pitchers6,7,20 and volleyball players8,9,11,13,17,19,22,27 (Table 1). There are no studies reporting the prevalence of infraspinatus atrophy in tennis, where the dominant shoulder is placed repeatedly at similar extremes of motion to volleyball and baseball, 18 particularly during serving. The aim of this study was therefore to investigate the prevalence of isolated infraspinatus atrophy in professional tennis players and to identify any correlations with physical examination findings, ranking performance, and concurrent shoulder disorders.
Reported Incidence of Dominant-Shoulder Infraspinatus Atrophy in Athletes a
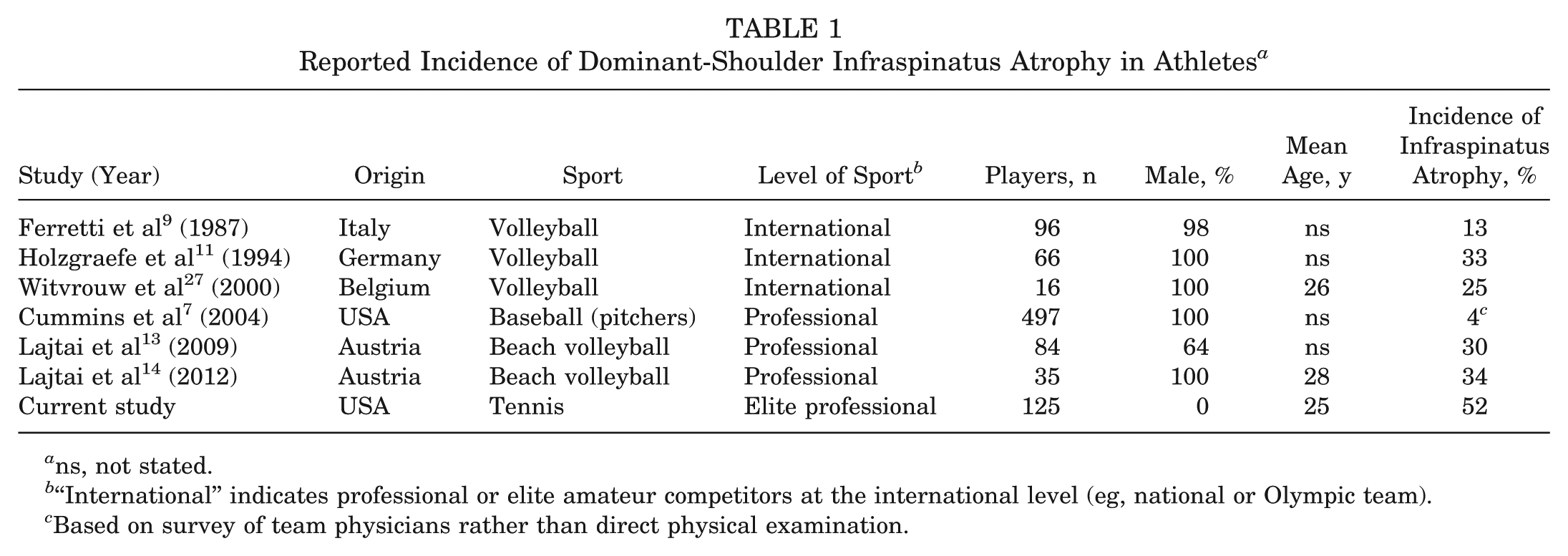
ns, not stated.
“International” indicates professional or elite amateur competitors at the international level (eg, national or Olympic team).
Based on survey of team physicians rather than direct physical examination.
Methods
A total of 125 professional female tennis players underwent a comprehensive physical health status examination in the first quarter of 2012. The study received ethical approval from a local institutional review board. Of the 125 players, 111 were ranked in the top 200 in the Women’s Tennis Association singles rankings at the time of the clinical examination. A questionnaire was administered that included a detailed medical history with type and details of any previous shoulder complaints, injuries, or surgeries. Two sports fellowship–trained orthopaedic surgeons performed a structured physical examination of the shoulders of all players. Infraspinatus atrophy was deemed to be present if there was loss of soft tissue prominence in the infraspinatus scapula fossa with increased prominence of the bony borders of the dorsal scapula of the shoulder with clear asymmetry when compared with the contralateral side when examined from the back of the athlete. Infraspinatus atrophy was considered present or absent, without quantifying the degree of atrophy. Infraspinatus atrophy was considered to be present if both surgeons reported the clinical finding.
A goniometric assessment of range of motion (ROM) was performed, including measurements of internal and external rotation of the dominant and nondominant shoulders at the glenohumeral joint with the humerus at 90° of abduction. The ROM was measured using the Pro 3600 Digital Inclinometer (SPI-Tronic). The inclinometer allows real-time digital reading of angles in a 360° circle with respect to a horizontal or vertical reference line; accuracy, as reported by the manufacturer, is within 0.1°; and its use in ROM measurement has been reported.15,16,28 Care was taken during the examination to ensure that the athlete’s glenohumeral motion was isolated from scapulothoracic motion or spine arching, by palpably stabilizing the scapular as glenohumeral motion was assessed. Glenohumeral internal rotation deficit was calculated, with a deficit of ≥25° considered pathologic. Total rotational arc loss between the dominant and nondominant shoulders was calculated, with ≥10° of loss considered pathologic.
External rotation strength was assessed with the arm at the side and graded according to the Musculoskeletal Research Council grading scale; a score ≤4 was considered weak. Shoulders were also examined for shoulder instability (anterior apprehension tests), laxity (sulcus sign), rotator cuff lesions (Jobe empty can supraspinatus test, external rotation strength, lift-off test), subacromial impingement (Neer sign, Hawkins sign), and superior labrum anterior-posterior or biceps injuries (O’Brien test). Scapula dyskinesis was assessed using the criteria of Burkhart et al. 3
Correlations were examined between infraspinatus atrophy and previous shoulder complaints, clinical examination findings, ROM, singles tennis ranking, and age.
Statistical Analysis
Differences in ROM measurements between dominant and nondominant shoulders were assessed with paired t tests. Associations between ROM parameters and history of injury were assessed with independent sample t tests, with P < .05 considered significant. Group comparisons for categorical variables were conducted with chi-square analyses except when cell sizes were <5, in which cases the Fisher exact test was used. To examine the conditional associations of several factors with infraspinatus atrophy in a multivariate model, we followed a standard regression model building method. All variables with bivariate associations with infraspinatus atrophy with a P < .10 were entered into a logistic regression model; then, nonsignificant variables were trimmed to produce the best fit. Adjusted P values, odds ratios, and 95% CIs were produced from the model coefficients.
Results
There were 65 players (52%) with evidence of infraspinatus atrophy in their dominant shoulders (Table 2). No wasting was noted in the nondominant shoulder of any player. There was 100% agreement on identification of infraspinatus atrophy between the 2 surgeons.
Patient Demographics a
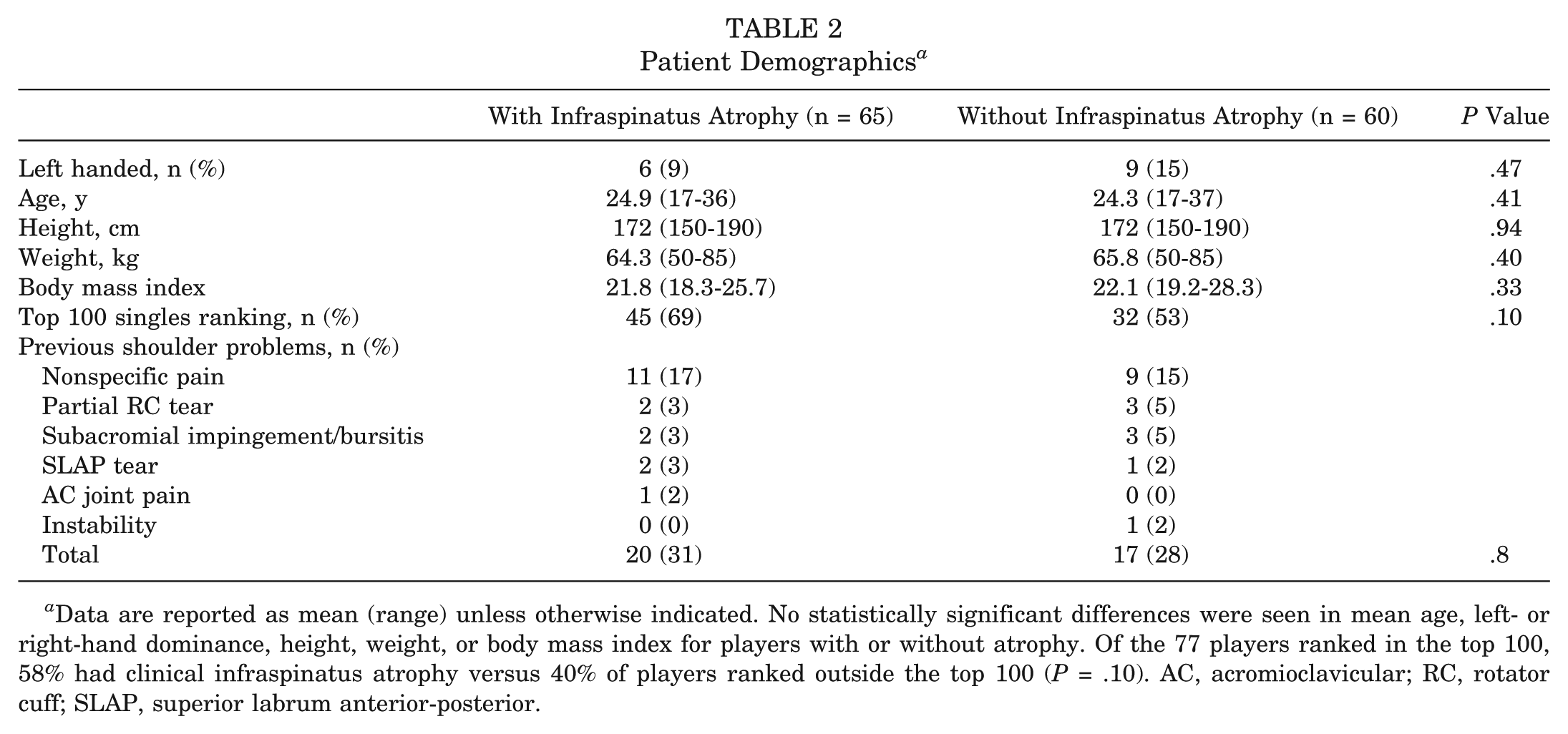
Data are reported as mean (range) unless otherwise indicated. No statistically significant differences were seen in mean age, left- or right-hand dominance, height, weight, or body mass index for players with or without atrophy. Of the 77 players ranked in the top 100, 58% had clinical infraspinatus atrophy versus 40% of players ranked outside the top 100 (P = .10). AC, acromioclavicular; RC, rotator cuff; SLAP, superior labrum anterior-posterior.
With regard to concurrent shoulder disorders, 31% of players with infraspinatus atrophy and 28% of those without atrophy reported a history of shoulder complaints (Table 2). The majority of these consisted of nonspecific shoulder pain without identifiable cause on magnetic resonance imaging. No player reported that rotational weakness of the shoulder was limiting one’s ability to play. Three players without infraspinatus atrophy had undergone previous shoulder surgery (1 arthroscopic debridement partial-thickness cuff tear, 1 arthroscopic stabilization, 1 rotator cuff repair). No player with infraspinatus atrophy had undergone previous shoulder surgery of any kind.
A significantly greater percentage of players with infraspinatus atrophy had a positive Hawkins impingement sign (32% vs 12%; P = .025). No differences were seen between the 2 groups in the presence of a sulcus sign, scapular dyskinesis, anterior apprehension, or O’Brien test in the dominant shoulder (see Appendix 1, available online at http://ajsm.sagepub.com/supplemental). Seven patients with infraspinatus atrophy (11%) demonstrated external rotation weakness (Musculoskeletal Research Council grade 4) of their dominant shoulders.
The ROM parameters for the 2 groups are given in Appendix 2 (available online). Patients with infraspinatus atrophy had an average of 11° less internal rotation in abduction in their dominant arms than did patients without (P < .01). A greater number of players with infraspinatus atrophy had a glenohumeral internal rotation deficit of ≥25°, but the difference was not statistically significant (26% vs 15%; P = .12).
Discussion
Although the phenomenon of asymptomatic infraspinatus muscle atrophy is well documented in volleyball and baseball players, this is the first report documenting its prevalence in tennis players. We documented a high rate of clinical infraspinatus atrophy (52%), particularly in higher-ranked players. The rate of infraspinatus atrophy (40%) in players ranked outside the top 100 was similar to previous rates reported in high-level volleyball players (Table 1).
Reeser et al 18 compared biomechanical parameters of the shoulder during volleyball serves, tennis serves, and baseball pitches. Many similarities among the motions existed, but because of the added resistance (moment of inertia) of the tennis racquet, the tennis serve generated the slowest internal rotational velocity and the greatest proximal force at the shoulder. 18 Maximal external rotation was also greater with tennis than volleyball serving (mean, 172° vs 160°). Such biomechanical differences and the unique demands of elite tennis may explain the high rate of infraspinatus atrophy seen in this study; however, the cause of infraspinatus atrophy remains uncertain, as does the biomechanical parameters that are important in its pathogenesis.
The clinical relevance of infraspinatus atrophy is also unclear. We found no association of infraspinatus atrophy with shoulder pain or with other shoulder disorders, and no player had undergone previous shoulder surgery for any reason. Similar to previous studies,7,9,11,13,14 players with infraspinatus atrophy did not report compromised sporting performance because of external rotation weakness. Presumably, teres minor and the posterior deltoid muscle can compensate for loss of infraspinatus function; however, more subtle functional deficits may still be present. Salles et al 21 assessed proprioceptive function in 18 asymptomatic professional volleyball players with infraspinatus atrophy and found significant deficits when compared with 20 volleyball players without atrophy.
Similarly, while we found clinical weakness of external rotation in only 11% of players with infraspinatus atrophy, more subtle external rotation deficits have been associated with high-performing athletes. Cornu et al 5 assessed dynamometric properties of the infraspinatus in amateur versus professional volleyball players and found that peak external rotation torque production was significantly higher in amateur players (46.58 ± 2.62 N·m) compared with professionals (35.35 ± 1.17 N·m). No differences were seen in peak torque values for internal rotation, and the torque ratios for external/internal rotation were always significantly lower for professional versus amateur volleyball players. The authors attributed this to the greater number of practices and games for professional athletes and, therefore, repetitive at-risk shoulder motions. More intensive training regimens and further advancement in tournaments may explain our somewhat paradoxical finding of a greater rate of infraspinatus atrophy in higher-ranked players.
Weakness of external rotation in the dominant shoulder of overhead athletes appears common and may occur before clinical signs. Wang 25 found significantly reduced power of external rotation in the dominant shoulder in all 10 members of the English national volleyball when compared with the opposite side. Lajtai et al 14 divided clinical infraspinatus atrophy into “slight atrophy” (only detectable by side-to-side comparison) and “severe atrophy” (detectable already without side-to-side comparison) in 12 beach volleyball players and compared the findings to those of 23 control patients without atrophy. Control athletes without infraspinatus atrophy had significantly lower external rotation strength on dynamometry (mean, 12.9 kg in the hitting shoulder vs 14.3 kg in the contralateral shoulder; P = .006), and this was associated with normal nerve conduction velocities but reduced amplitudes. Decreased nerve conduction velocities were noted in all patients with atrophy; however, lower activation patterns on electromyographic studies were seen only in the severe atrophy group. Players with atrophy had significantly greater loss of external rotation strength than those without atrophy. This suggests graduated forms of neurapraxia exist, and mild early weakness of external rotation occurs before clinical atrophy and detectable neurophysiologic changes.
Current literature supports nonoperative treatment of players with infraspinatus atrophy but without pain or functional deficit. Ferretti et al 10 reviewed 16 players with infraspinatus atrophy treated nonoperatively at a mean 5.5 years of follow-up. While the infraspinatus atrophy remained unchanged in all 16 players, all players continued with top-level volleyball, with only 2 complaining of some limitation owing to anterior shoulder pain. Additionally, it seems that even after decompression of the nerve, atrophy of the infraspinatus is unlikely to resolve fully. 1 Ferretti et al 10 noted improvement in infraspinatus atrophy in only 1 of 3 volleyball players who underwent surgical decompression. Similarly, Sandow and Ilic 22 noted that recovery of infraspinatus bulk was incomplete in 5 players undergoing suprascapular nerve decompression at the spinoglenoid notch, although all 5 patients returned to the same or a higher level of volleyball.
Similar to previous researchers, we were unable to demonstrate any static physical examination findings (eg, scapular dyskinesis, glenohumeral internal rotation deficit, postural abnormalities) as risk factors for infraspinatus atrophy. 19 Some authors have associated increased external rotation with infraspinatus atrophy,22,27 hypothesizing that placing the abducted shoulder joint in extreme external rotation results in compression of the suprascapular nerve at the spinoglenoid notch by the spinati muscles. 22 Our data provided limited support for this hypothesis, with only 5° additional external rotation in affected versus unaffected players. Additionally, if extreme external rotation is the primary risk factor for development of infraspinatus atrophy, then other overhead athletes (particularly baseball pitchers) should exhibit infraspinatus atrophy at frequencies at least as great as those seen in volleyball athletes. Similarly, while we did find that affected players had less internal rotation than that of unaffected players (mean, 23° vs 34°; P < .001), it is unclear if this represents a risk factor for infraspinatus atrophy or occurs as a secondary result.
There are a number of limitations to our study. First, we used a clinical definition of infraspinatus atrophy, which is a subjective measure, and dynamometry was not performed. However, this is common in other studies of infraspinatus atrophy,7,9,11,13 which is, by its nature, a clinical examination finding. It also has clearly defined criteria, with the ability to compare to the contralateral side. In addition, examination of each athlete was carried out by the same 2 fellowship-trained orthopaedic surgeons, and intratester reliability in clinical examination is known to be higher than intertester reliability. 27 Additionally, the surgeons had 100% agreement on examination of infraspinatus atrophy in these athletes. Second, we did not perform advanced imaging to identify potential causes of compression; however, most players in this study with shoulder symptoms had already undergone magnetic resonance imaging scans with no compressive lesions found. In addition, previous studies have shown that in asymptomatic players with infraspinatus atrophy, magnetic resonance imaging will rarely find a cause.7,13 Third, the elite nature of the players included in this study and the unique demands placed on their shoulders mean that the results are not generalizable to tennis players at a lower level of competition. 23 Finally, the cross-sectional design of this study means that risk factors and changes of incidence of infraspinatus atrophy with time are unclear.
In conclusion, we report a high level of clinical infraspinatus atrophy in the dominant shoulder of elite female tennis players. This was associated with a higher performance ranking, and no functional deficits or associations with concurrent shoulder disorders were found. Team physicians can be reassured that infraspinatus atrophy is a common finding in high-performing tennis players and, if asymptomatic, does not appear to lead to a significant compromise in performance.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.