
Abstract
Background:
The use of allografts for anterior cruciate ligament (ACL) reconstruction in young athletes is controversial. No long-term results have been published comparing tibialis posterior allografts to hamstring autografts.
Purpose:
To evaluate the long-term results of primary ACL reconstruction using either an allograft or autograft.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
From June 2002 to August 2003, patients with a symptomatic ACL-deficient knee were randomized to receive either a hamstring autograft or tibialis posterior allograft. All allografts were from a single tissue bank, aseptically processed, and fresh-frozen without terminal irradiation. Graft fixation was identical in all knees. All patients followed the same postoperative rehabilitation protocol, which was blinded to the therapists. Preoperative and postoperative assessments were performed via examination and/or telephone and Internet-based questionnaire to ascertain the functional and subjective status using established knee metrics. The primary outcome measures were graft integrity, subjective knee stability, and functional status.
Results:
There were 99 patients (100 knees); 86 were men, and 95% were active-duty military. Both groups were similar in demographics and preoperative activity level. The mean and median ages of both groups were identical at 29 and 26 years, respectively. Concomitant meniscal and chondral pathologic abnormalities, microfracture, and meniscal repair performed at the time of reconstruction were similar in both groups. At a minimum of 10 years (range, 120-132 months) from surgery, 96 patients (97 knees) were contacted (2 patients were deceased, and 1 was unable to be located). There were 4 (8.3%) autograft and 13 (26.5%) allograft failures that required revision reconstruction. In the remaining patients whose graft was intact, there was no difference in the mean Single Assessment Numeric Evaluation, Tegner, or International Knee Documentation Committee scores.
Conclusion:
At a minimum of 10 years after ACL reconstruction in a young athletic population, over 80% of all grafts were intact and had maintained stability. However, those patients who had an allograft failed at a rate over 3 times higher than those with an autograft.
An anterior cruciate ligament (ACL) tear is a common injury with an increased incidence in a young, active population and an estimated incidence of 250,000 tears annually,9,41,58 with over 200,000 ACL reconstruction procedures performed per year in the United States.6,7,22 Nonoperative treatment is an option; however, ACL-deficient knees have been linked to an increased development of chondral and meniscal pathologic abnormalities.17,49,63,64 The typical treatment for an ACL rupture in an active patient is surgical reconstruction. ACL reconstruction has been shown to be economically advantageous as well as to increase quality of life when compared with rehabilitation and nonoperative management. 44
Reconstruction can be performed with either autogenous or allogenic tissue.1,11,34,50,51,55,65 Traditionally, the use of a patellar tendon autograft has been considered the “gold standard.”15,25,33,65 With improved techniques for femoral and tibial fixation, the use of soft tissue grafts has become more common for ACL surgery. Specifically, the hamstring tendon autograft has increased in popularity because of comparable clinical outcomes, decreased anterior knee pain and kneeling discomfort, lower donor site morbidity, and decreased potential injuries to the extensor mechanism.3,8,21,23,50,62
Over the past decade, allografts have been used in greater frequency for both primary and revision ACL surgery. In a recent study of over 16,000 ACL reconstructions from a community-based registry, allografts were used in 42.4% of primary and 78.8% of revision ACL reconstructions. 42 The primary advantage of allograft tissue is the lack of donor site morbidity. Additional advantages include a shorter operative time, improved cosmesis, multiple graft options and sizes, and decreased overall cost.12,16,52,57 However, the risks of allogenic tissue include potential disease transmission, delayed incorporation, and depending on the processing technique employed, decreased graft strength and stiffness.4,18,30,32,35,46,53,54
In several recent comparison studies, allografts have been shown as a viable alternative to autograft tissue.14,24,36-38,59 Myriad studies comparing various graft types with allografts have shown comparable results.2,17,20,43,51,56,57 Despite this, there has been a lack of literature comparing hamstring tendon autografts to soft tissue allografts. 19 Sun et al 59 reported on 186 patients who had undergone ACL reconstruction randomized to receive either a hamstring autograft or an allograft. They reported on subjective and objective characteristics of the 2 groups but did not specifically comment on failure rates. At over 7 years postoperatively, they found no difference in the outcomes of their patients who had received either an autograft or an allograft.
The purpose of this study was to compare the long-term clinical and subjective outcomes in patients after ACL reconstruction with either a hamstring autograft or tibialis posterior tendon allograft. The primary outcome measures were graft survivorship and subjective functional knee stability.
Methods
The original prospective, randomized study and the subsequent long-term follow-up of these patients were approved by the institutional review board and the human use committee at Tripler Army Medical Center. Investigators adhered to the policies for the protection of human participants as prescribed in 45 Code of Federal Regulations 46.
Patients 18 years of age or older with symptomatic ACL deficiency, confirmed by magnetic resonance imaging (MRI), were eligible for participation in the study. Multiligamentous injuries (concomitant grade I or II medial collateral ligament injuries were not excluded), previous knee ligament surgery (previous knee arthroscopic surgery was not excluded), and time remaining on the island of less than 6 months were exclusion criteria. Participating patients were randomized by study design using sealed envelopes to undergo ACL reconstruction with either 1 of 2 soft tissue graft types: tibialis posterior allograft (Figure 1A) or hamstring autograft (Figure 1B). The patients, once randomized, were not blinded as to their graft type. All allografts were obtained from the same American Association of Tissue Banks–certified tissue bank (Musculoskeletal Transplant Foundation). All the allografts were fresh-frozen, aseptically harvested, and not terminally irradiated. All patients underwent a preoperative clinical examination by the senior author (C.R.B.), knee radiography, and MRI to confirm ACL deficiency and to identify concomitant meniscal and/or chondral pathologic abnormalities.
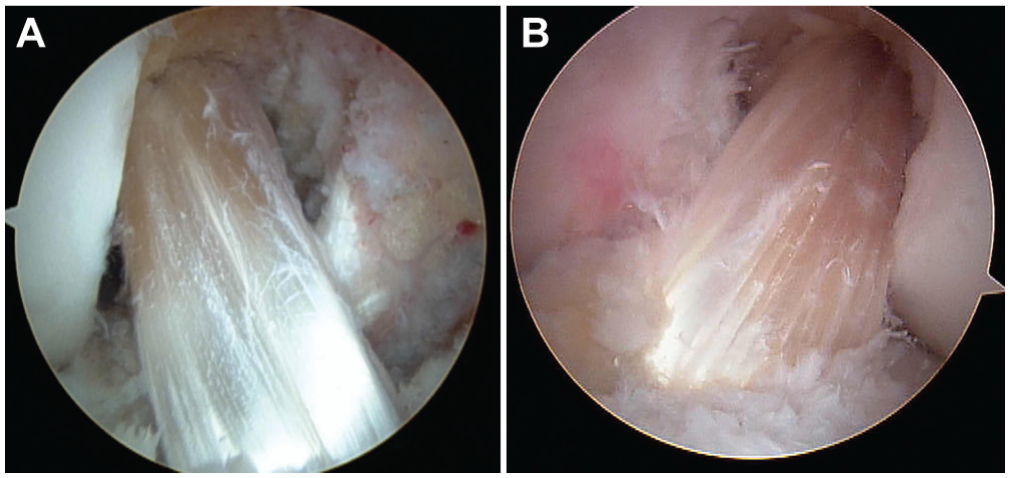
(A) Intraoperative view of anterior cruciate ligament (ACL) reconstruction with a tibialis posterior allograft. (B) Intraoperative view of ACL reconstruction with a hamstring autograft.
Operative Procedure
All patients received general endotracheal or laryngeal mask anesthesia at the discretion of the anesthesia provider. All patients were first examined under anesthesia. A standard pneumatic tourniquet was inflated after sterile preparation and draping of the lower extremity. All procedures were performed via the same technique by 1 of 2 attending surgeons (C.R.B., E.L.S.). For the autograft group, hamstring harvest was performed through a longitudinal incision over the pes anserinus. The sartorial layer was incised obliquely. Both the gracilis and semitendinosus tendons were retrieved together with a right-angle retractor and then resected from their insertion on the proximal tibia. The 2 tendons were secured together using a locking Krackow stitch of No. 5 Ethibond sutures (Ethicon Inc). After release of the fascial bands, the tendons were individually harvested with an open-ended tendon stripper (ConMed Linvatec Inc). The tendons were then scraped of remaining muscle, and the free ends were prepared with No. 5 Ethibond sutures on each end. The doubled semitendinosus and gracilis tendons were sized to determine the smallest diameter through which they would fit. The graft was then placed on 15 lb of tension using the Graftmaster board (Smith & Nephew Inc) until needed.
All of the allografts were maintained frozen in a commercially available freezer until surgery. After complete thawing in warm saline with an antibiotic, the allograft was prepared on both ends with No. 5 Ethibond sutures in a locking Krackow stitch. The size of the doubled graft was then determined and the graft placed on 15 lb of tension using the Graftmaster board until needed. The smallest diameter that allowed the graft to pass was determined with the graft sizing block (Arthrex Inc). Diagnostic arthroscopic surgery was performed through standard portals. An irrigation pump (Stryker Endoscopy) and a superomedial outflow portal were routinely used. Thorough diagnostic arthroscopic surgery included an assessment of meniscal and chondral surfaces. Meniscal repair, when indicated, was performed via an inside-out technique using No. 0 permanent sutures (Ethibond). For a small longitudinal tear that did not displace into the joint, an all-inside repair technique was employed (BioHornet; ConMed Linvatec Inc). For smaller irreparable tears, meniscal debridement was performed. Chondral surfaces were assessed and graded according to the modified Outerbridge classification. 13 Full-thickness, contained lesions were treated with subchondral microfracture after preparation of the lesion with a standard technique. 45
A 5.5-mm shaver (Tomcat; Stryker Endoscopy) was used both to remove the residual ACL stump and to perform minimal notchplasty. Enough bone was removed to adequately visualize the “over-the-top” position on the posteromedial aspect of the lateral wall of the intercondylar notch. A tibial ACL guide was then introduced into the knee, and a pin was placed in the posterior aspect of the ACL tibial footprint. An oblique tibial tunnel as described by Howell 26 allowed appropriate positioning of the femoral tunnel at the 10- or 2-o’clock position for the right and left knees, respectively. The graft was secured first in the femur with a metal cross-pin (Transfix; Arthrex Inc) (Figure 2). The knee was cycled, while tension was maintained on the graft distally for a minimum of 10 cycles. With the knee at 30° of flexion, tibial fixation consisted of a bioabsorbable interference screw (Bioscrew; Arthrex Inc) of the same diameter as the tibial tunnel. The graft or remaining sutures were secured by a bicortical 6.5-mm screw and spiked washer inserted in the proximal tibia just distal to the opening of the tibial tunnel. The tourniquet was released after tibial graft fixation, and intraoperative radiographs were obtained to assess the tunnel and hardware position. If necessary, the cross-pin was advanced further into the distal femur. Hemostasis was confirmed and standard closure completed. Care was taken to ensure that incisions were similar in appearance, irrespective of the graft type utilized.
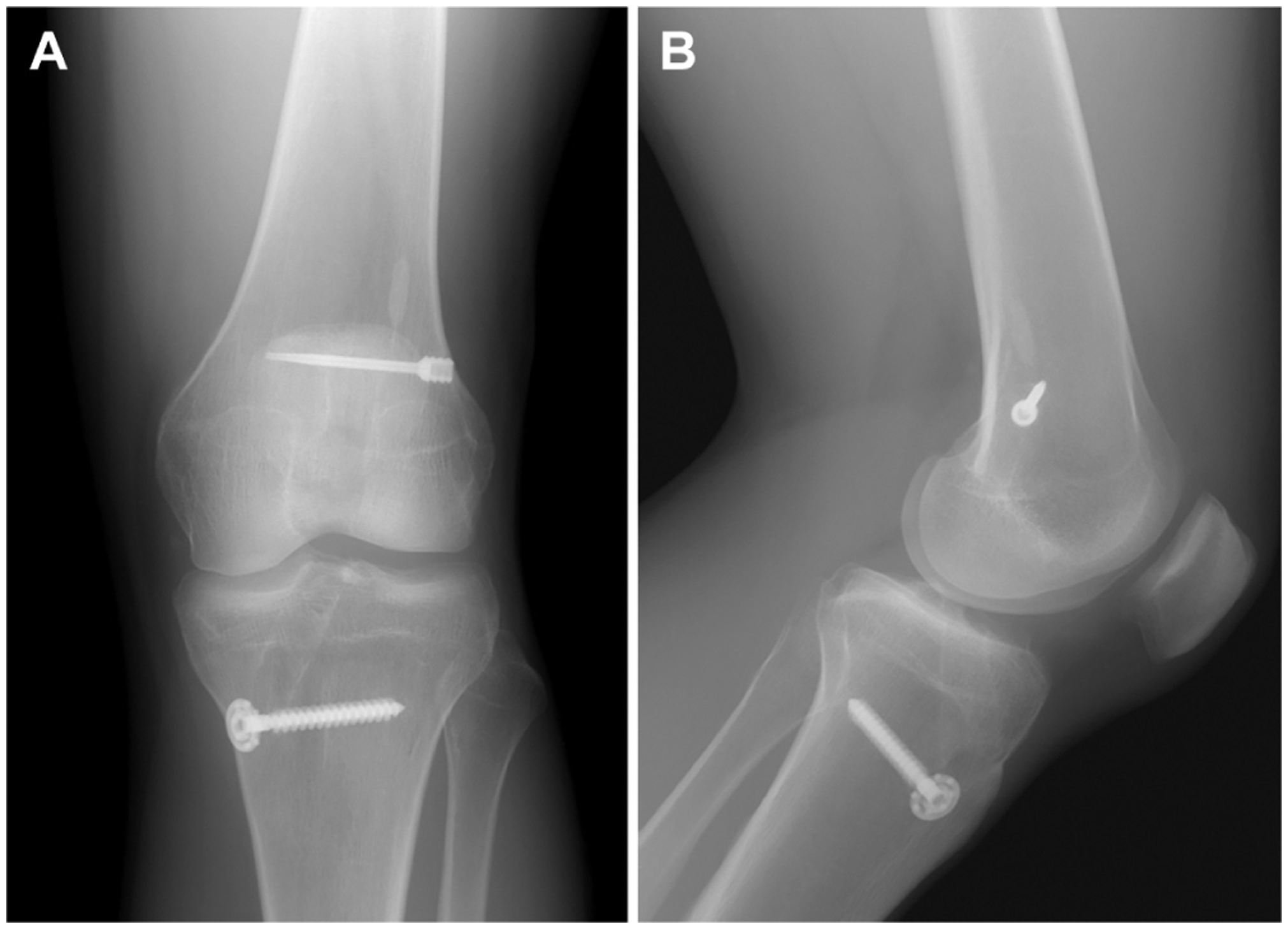
Postoperative (A) anteroposterior and (B) lateral radiographs of the femoral cross-pin (Transfix; Arthrex Inc) used in all knees.
Rehabilitation
Patients were all admitted overnight and discharged after physical therapy consultation on the following day. Patients used cryotherapy continuously for the first week (Cryocuff; AirCast/DJO Global). Emphasis was placed on maintaining knee extension and regaining quadriceps control. A drop-lock brace (DJO Global) locked in full extension was used for the first 4 weeks and then discontinued thereafter. Postoperatively, all patients followed a standardized rehabilitation protocol supervised by a military physical therapist, who was blinded as to the specific graft type employed. Of note, both techniques utilized the same incision; therefore, there was no obvious outward indication of the graft type used. Full weightbearing was allowed immediately, except in cases where meniscal repair or microfracture was performed. Weightbearing was fully restricted for 6 weeks after microfracture and for 4 weeks after meniscal repair. Full active motion was encouraged in all cases, except when meniscal repair was performed. In these patients, knee flexion was restricted to 90° for the first 4 weeks and then unrestricted thereafter.
Patient Evaluations
Study patients completed all preoperative evaluations in the visit immediately preceding surgery. They were then seen at 3, 14, and 30 days postoperatively and then monthly until released to full unrestricted activity. At their latest follow-up, patients were either examined or, for the vast majority who had left the island, contacted by telephone and via Internet survey to assess their functional status and to collect subjective outcome measures. Subjective outcome measures included the Single Assessment Numeric Evaluation (SANE) score, 66 indicating overall subjective function, the Tegner activity scale score, and the International Knee Documentation Committee (IKDC) subjective knee form score. The IKDC is an 18-question patient-rated instrument that evaluates symptoms, function, and sports activity. The total score ranges from 0 to 100, with a higher score representing a superior outcome. 28 It has been shown to be reliable and responsive for ACL injuries.27,29 The Tegner activity scale score ranges from 0 to 10, with 10 being a professional athlete and 0 being disability due to the knee. 60 Patients were also queried at their latest follow-up regarding subjective knee stability, any subsequent revision surgery, current military status, contralateral knee function, and present activity level.
Statistical Analysis
All statistical analyses and tests were conducted using SPSS version 17 or higher (PASW Statistics; SPSS Inc) and verified with SAS (SAS Institute Inc) when appropriate. All analyses were conducted by a biostatistician with a doctorate degree. Significant differences between levels of return to duty involving continuous variables were evaluated with 1-way analyses of variance followed by Tukey post hoc multiple comparison procedures (verified by Newman-Keuls) to isolate where significant differences lay. Significant differences involving categorical/nominal variables were evaluated with the χ2 test. Thresholds for statistical significance were set at P < .05.
Power analysis was conducted using NCSS-PASS version 1.0 (NCSS LLC). We assumed equal variances between the 2 groups, with both SDs equal to 10. We selected an α error of .05 with a 2-tailed possibility of directional difference and a difference between means of 5 points on the 100-point Lysholm score. With 50 patients in each group, the power achieved was 70%, but at a difference in means of 6 points, the power was 85%. If the data turned out to be nonnormally distributed, a nonparametric Mann-Whitney test was used and with the same assumptions. The respective powers are estimated at 68.8% and 83.6%.
Results
From June 2002 to August 2003, a total of 99 consecutive patients (100 knees) with an ACL tear and symptomatic knee instability were enrolled in the study (Figure 3). The mean and median ages of the patients at the time of surgery were 29 and 26 years in both groups, respectively; 95% of the patients were on active military duty at the time of surgery. There were 86 male and 13 female patients, with 7 female patients in the autograft group and 6 in the allograft group. One hundred knees were randomized via sealed envelopes; 50 knees underwent ACL reconstruction using a 4-stranded hamstring autograft, and 50 underwent reconstruction with a tibialis posterior tendon allograft. One patient with bilateral ACL tears was randomized to each group and underwent bilateral, simultaneous ACL reconstructions using an autograft on one side and an allograft on the other. Patient demographics, mechanisms of injury, and operative findings are displayed in Table 1. There were meniscal pathologic abnormalities in 35 (72.9%) and 33 (67.3%) patients of the autograft and allograft groups, respectively. Chondral pathologic abnormalities were found in 22 (45.8%) patients of the autograft group and 17 (34.7%) patients of the allograft group. There were no significant differences between the groups with the exception of a mild increase in chondral pathologic abnormalities of the lateral femoral condyle in the allograft group. The tourniquet time accurately reflected the operative time and excluded the variable time required for intraoperative radiographs and wound closure. The mean tourniquet times for the autograft and allograft groups were similar at 71 and 65 minutes, respectively.
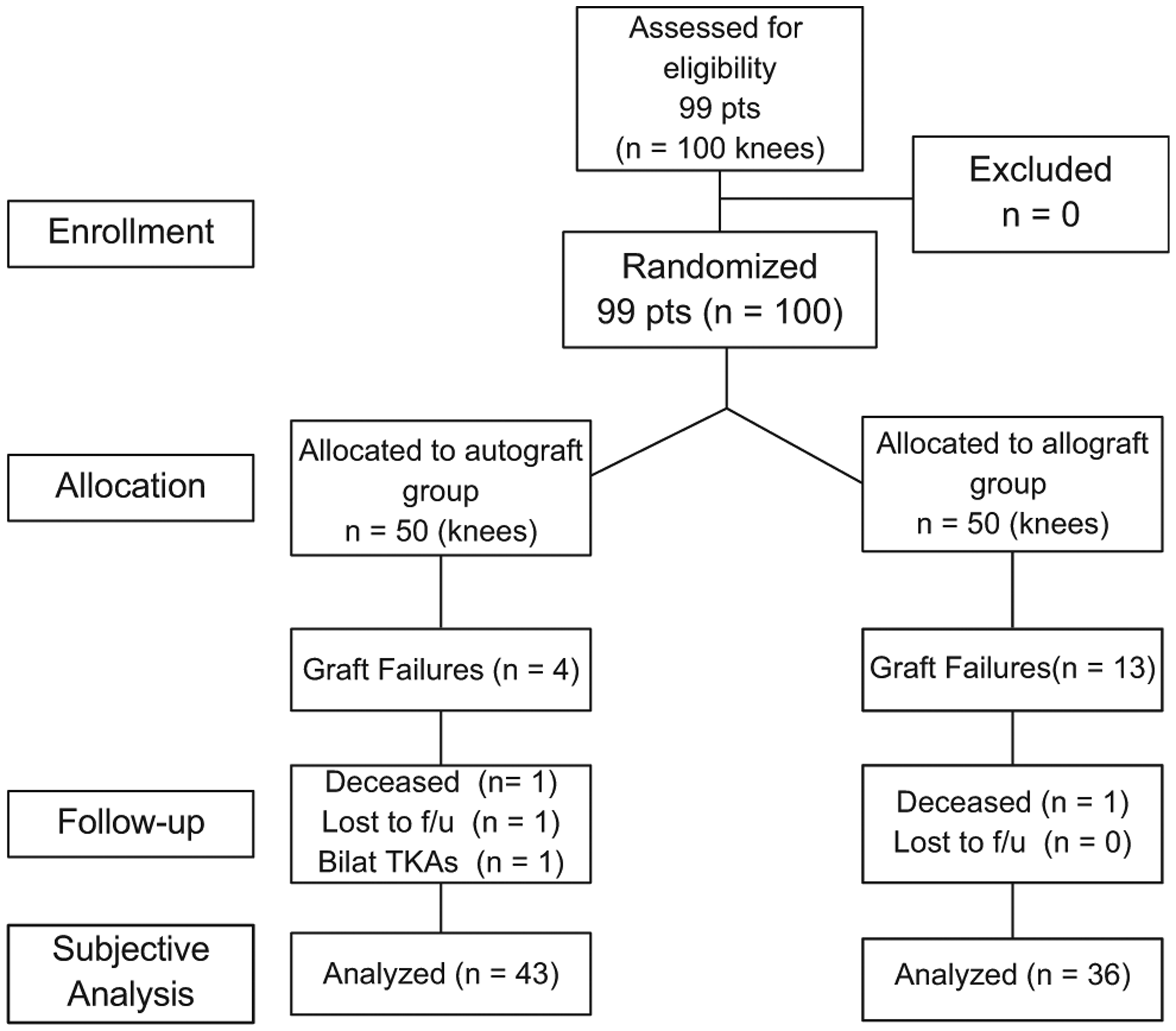
CONSORT (Consolidated Standards of Reporting Trials) flow diagram.
Demographic Data of Study Patients by Group a
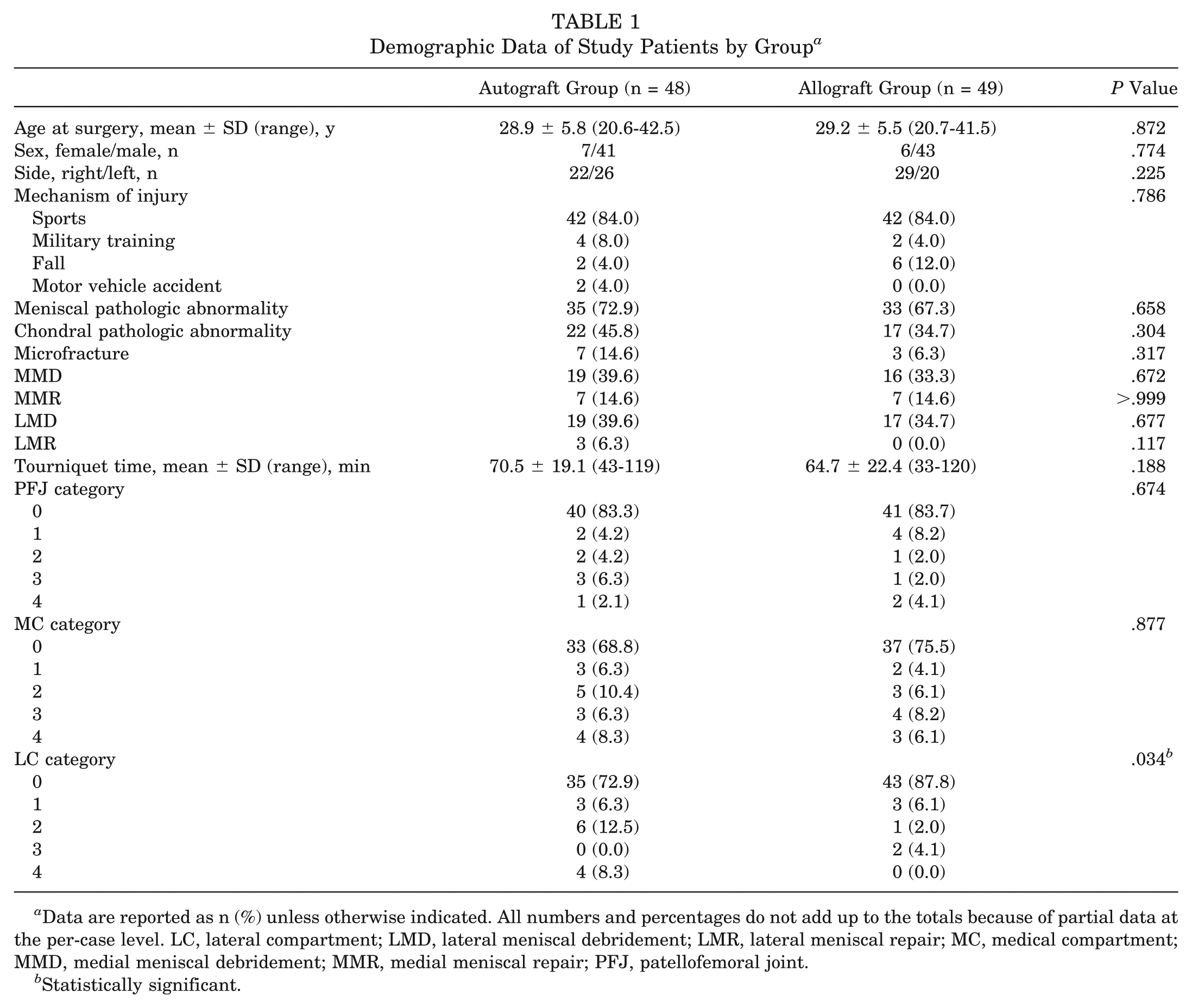
Data are reported as n (%) unless otherwise indicated. All numbers and percentages do not add up to the totals because of partial data at the per-case level. LC, lateral compartment; LMD, lateral meniscal debridement; LMR, lateral meniscal repair; MC, medical compartment; MMD, medial meniscal debridement; MMR, medial meniscal repair; PFJ, patellofemoral joint.
Statistically significant.
The patients were evaluated at their latest follow-up if still living in close proximity to the hospital. The majority of the patients had transferred duty stations and had left the island. These patients were contacted by telephone and then via an email survey. Two patients were identified to have been deceased. All but 1 of the remaining patients were located and contacted. The minimum follow-up from surgery for the remaining 96 patients was 10 years (mean, 126 months; range, 120-132 months). One patient underwent bilateral total knee arthroplasties at 8 years after his ACL reconstruction for severe degenerative arthritis. Of the remaining 95 patients (96 knees), 17 patients failed their index operation and sustained graft failure, requiring revision ACL reconstruction. Of these 17 graft failures, 13 were allografts (26.5%) and 4 (8.3%) were autografts (P = .03).
Table 2 summarizes the surgical failures and subjective outcome results of all patients. The 17 known failures, the 2 deceased patients, the patient requiring arthroplasty, and 1 patient lost to follow-up were excluded from the final subjective analysis, leaving 79 knees in 78 patients who made up the secondary study cohort. The remaining patients who had not undergone revision ACL surgery were queried as to subjective knee stability and functional status; these subjective outcome scores are summarized in Table 3. There were no statistical differences with respect to subjective outcome scores between the 2 groups.
Graft Failures and Subjective Outcome Scores of All Patients a
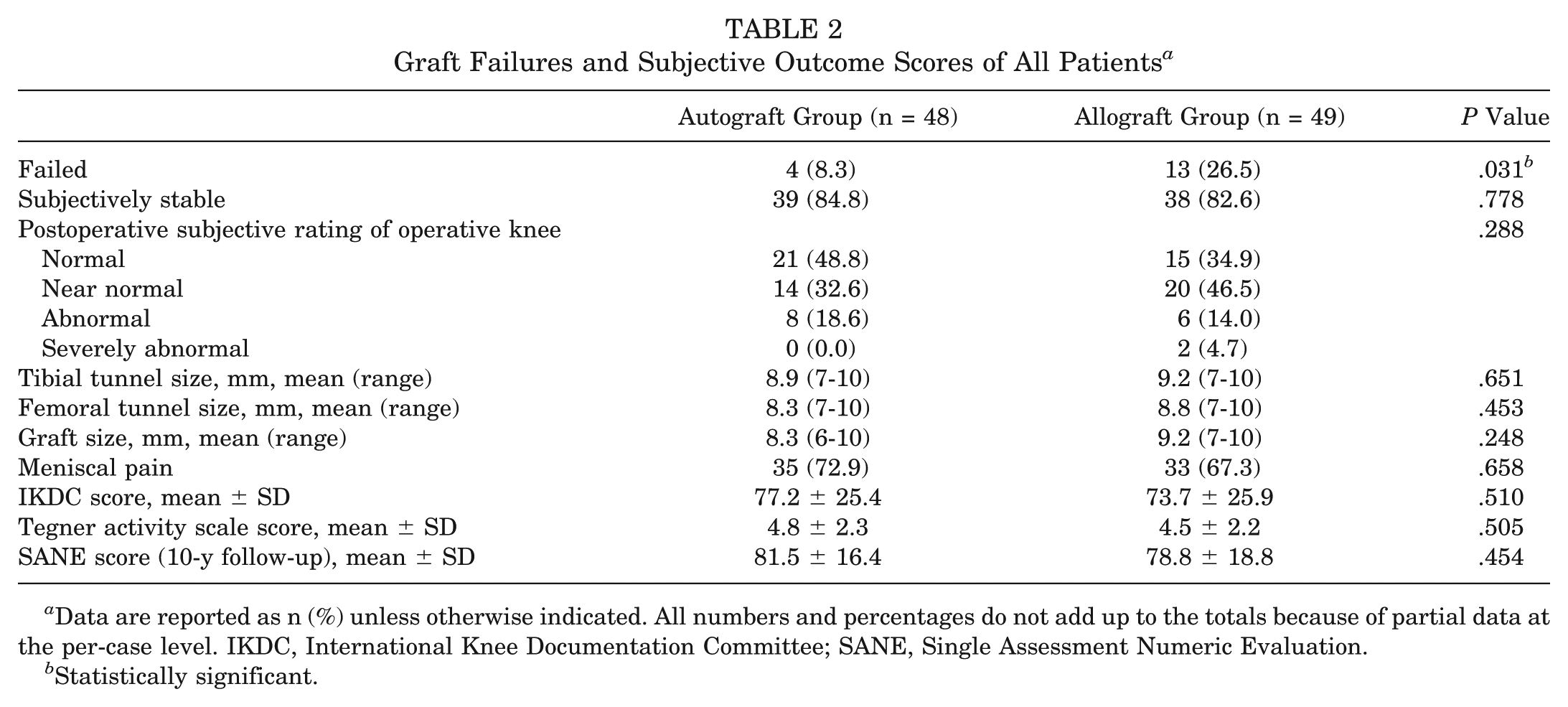
Data are reported as n (%) unless otherwise indicated. All numbers and percentages do not add up to the totals because of partial data at the per-case level. IKDC, International Knee Documentation Committee; SANE, Single Assessment Numeric Evaluation.
Statistically significant.
Outcomes of Nonfailures a
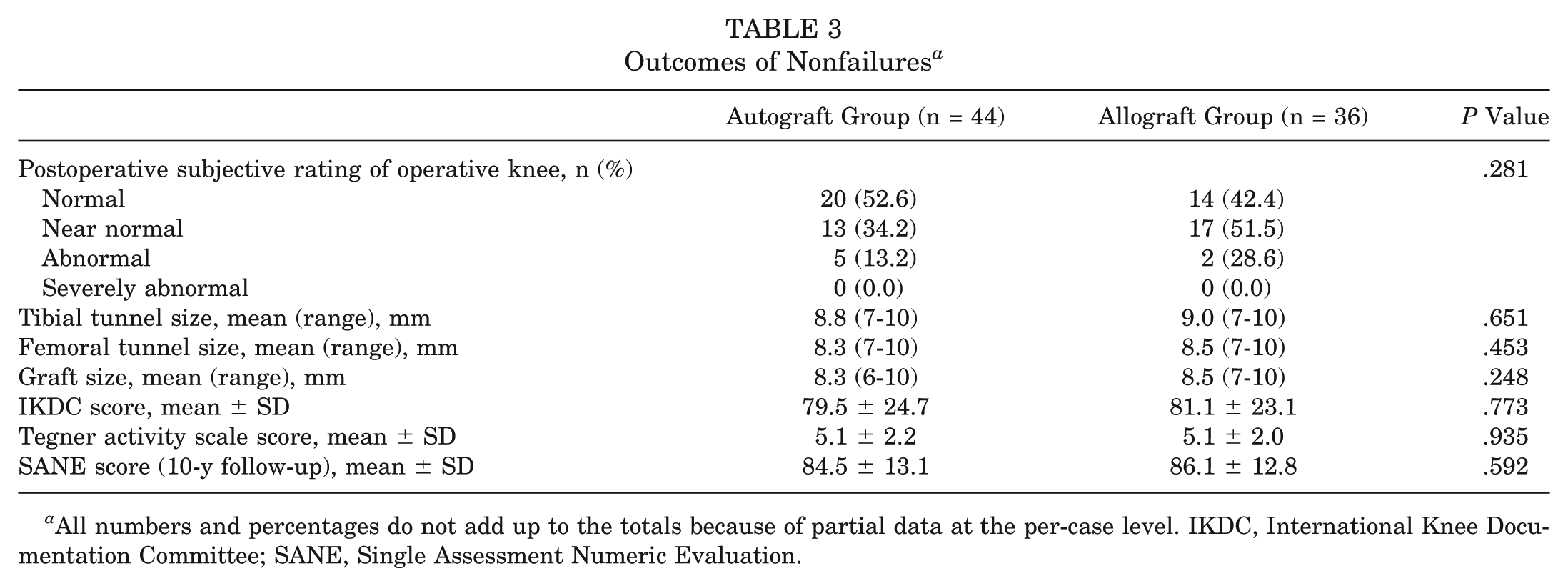
All numbers and percentages do not add up to the totals because of partial data at the per-case level. IKDC, International Knee Documentation Committee; SANE, Single Assessment Numeric Evaluation.
To further assess graft integrity, patients were asked specifically if their knee felt stable. Of the 78 patients (79 knees), all but 6 (4 autografts and 2 allografts) reported their knee to be stable. Table 4 summarizes the operative findings and compares those who subjectively reported their knee to be stable with those who thought their knee unstable. Although the numbers were low, there were no statistical differences in operative findings or outcome measures when comparing these 2 groups except the age of the patients and the mean SANE scores. There was a significant difference in the age of the patients at the time of surgery, with the unstable group having a mean age of 24.4 years (range, 21.5-29.1 years) compared with 30.2 years (range, 20.7-42.5 years) in the stable group (P = .01). Patients in the unstable group did have a significantly lower mean SANE score when compared with the patients who rated their knee as stable. To further assess the 6 patients who reported their knee as unstable, a repeat examination, KT-1000 arthrometer testing, and MRI were performed where feasible. Of those 6 patients, 4 were re-examined by an orthopaedic surgeon and underwent an MRI study of their operative knee. These 4 were all found to have an intact ACL graft by MRI. Two of these also underwent KT-1000 arthrometer testing and were found to have <3-mm side-to-side differences. Two remaining patients (1 autograft and 1 allograft) were unable to be assessed by physical examination or by MRI.
Comparative Stability for Nonfailures a
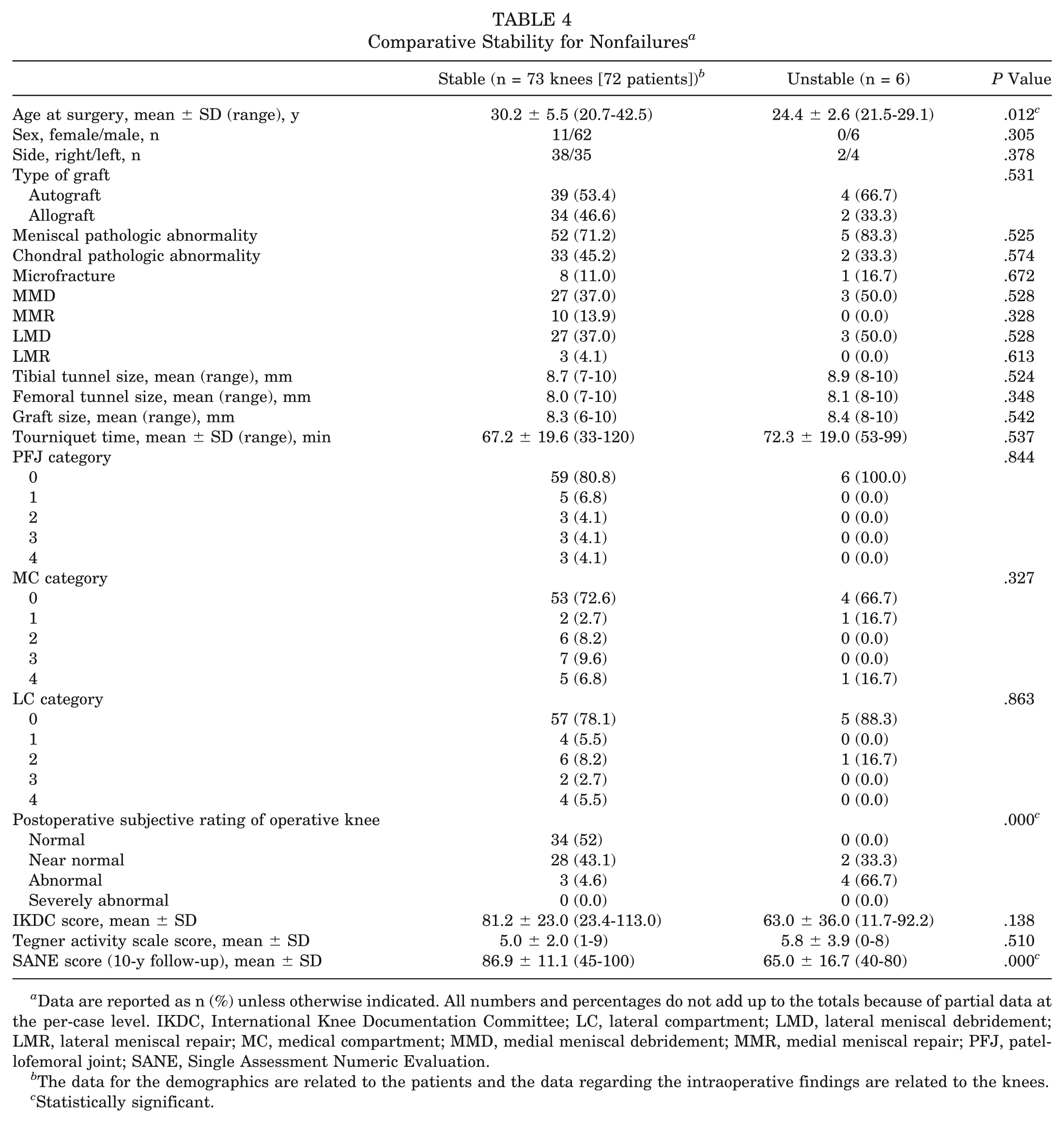
Data are reported as n (%) unless otherwise indicated. All numbers and percentages do not add up to the totals because of partial data at the per-case level. IKDC, International Knee Documentation Committee; LC, lateral compartment; LMD, lateral meniscal debridement; LMR, lateral meniscal repair; MC, medical compartment; MMD, medial meniscal debridement; MMR, medial meniscal repair; PFJ, patellofemoral joint; SANE, Single Assessment Numeric Evaluation.
The data for the demographics are related to the patients and the data regarding the intraoperative findings are related to the knees.
Statistically significant.
Discussion
The foremost goal of ACL reconstructive surgery is to restore normal preinjury knee stability. The ideal graft to use to accomplish this goal is one that would have no donor site morbidity, is readily available, is strong enough to allow accelerated rehabilitation, and quickly incorporates. Unfortunately, the ideal graft does not exist. The goal of our study was to compare the long-term clinical results of 2 types of soft tissue grafts commonly utilized for ACL reconstruction in a similar group of patients. We attempted to isolate, as much as possible, the one dependent variable of the study: the graft type. The identical surgical technique, femoral and tibial fixation, and postoperative rehabilitation protocol were used in all patients. Long-term results have been reported for both hamstring and patellar tendon allografts. 40 The primary question of this study was whether soft tissue allografts perform equally to hamstring autografts.
Allografts are readily available, and their use obviates donor site morbidity; however, their use carries the risk of disease transmission. The estimated risk of HIV transmission for allograft use has been estimated at 1 in 1,600,000. 10 With careful donor screening and strict aseptic processing, as is utilized by the tissue bank from which all of our allografts were obtained (Musculoskeletal Transplant Foundation), the risk of disease transmission can be minimized. Allografts have been shown to incorporate more slowly into host tissue. 30 In a goat model, greater strength and stability of autografts have been demonstrated at 6 months in comparison with allografts. It has been noted, however, that allografts do exhibit Sharpey fibers at the graft-tunnel interface. 39 It is known that some types of sterilization can adversely affect allograft tissue.33,60 The fresh-frozen allografts in this study were neither terminally irradiated nor sterilized with ethylene oxide, both of which have been associated with decreasing allograft structural properties.
In our study, we found a greater than 3-fold increased rate of graft failure in a young, active population undergoing primary ACL reconstruction with an allograft compared with an autograft. Specifically, we found a retear rate after reconstruction with a hamstring autograft of 8.3% compared with 26.5% in those knees reconstructed with a tibialis posterior allograft. We also found that the rate of failure was independent of any concomitant meniscal or chondral pathologic abnormalities. This is contrary to the 2 other published prospective studies comparing hamstring autografts to allografts. In the study by Sun et al, 59 208 patients were randomized to receive either a hamstring autograft or fresh-frozen hamstring allograft. The mean follow-up was 7.8 years in 186 patients (91 autografts and 95 allografts). Although the authors reported that 15 knees (7 autografts and 8 allografts) had KT-2000 arthrometer laxity of >5 mm, there was no mention of overt graft failures or the need for revision in any of their patients. In addition, there was no report as to the specific type of athletic participation of their patients (ie, high school or collegiate athletes). In the study by Edgar et al, 19 104 patients were randomized to receive a hamstring autograft or hamstring allograft. However, 75% of their study patients consented to randomization, and the authors pooled both randomized and nonrandomized patients for their final assessment. In addition, the allografts used in their study were cryopreserved in the first 20 knees but then fresh-frozen in the subsequent 27 knees reportedly because of increased infection rates noted in cryopreserved allografts. Nineteen percent of their patients were lost to follow-up. Of those remaining for the final evaluation at a minimum 3-year follow-up, there was no difference reported in side-to-side laxity and Lysholm, IKDC, or Tegner activity scores. Of note, they reported 11% “borderline failures” in their allograft group based on measured laxity. Both articles came to the conclusion that an allograft is a comparable graft type in a young, active population, which is a conclusion contrary to that of our data.
Our study used a fresh-frozen tibialis posterior tendon allograft from the same tissue bank in all patients who were randomized to the allograft group. Tendon allografts have been shown to be safe for use in ACL reconstruction, with soft tissue grafts having faster incorporation than bone plug grafts.30,38,48,55 Traditionally, an allograft has the advantage of decreased donor site morbidity, improved cosmesis, ability to obtain a graft as large as necessary, and decreased stiffness in the operative knee. The primary concern with the use of allografts is disease transmission, primarily of viral pathogens. 10 Our grafts were aseptically harvested, were fresh-frozen, and did not receive terminal irradiation. This specific technique has been shown to reduce antigenicity without affecting graft strength.5,31,47 In our population of young athletes, there was uniformity of graft processing, surgical technique, graft fixation, and postoperative rehabilitation.
Our study design and operative technique ensured that the physical therapists were blinded to the graft type used. All participants followed the same rehabilitation protocol according to previously established exercise regimens. 61 The rehabilitation program was modified for any concomitant procedures, with the primary variation being nonweightbearing status after microfracture and meniscal repair. Despite this, there was an increased failure rate in the allograft group, with failure greater than 3 times higher than that seen in the autograft group.
The primary limitation of our study is the subjective assessment of graft stability. However, the functional status, activity level, and subjective rating by the patients, we believe, are more accurate determinants of graft stability and surgical success. The ability to perform clinical or radiologic examinations on a large military population at over 10 years after ACL reconstruction is not feasible. Clearly, the functional status deteriorated in most patients in our study, as would be expected in any population over the same time period. However, we believe that this deterioration is the result of chondral and meniscal injuries at the time of ACL injury. Remarkably, many of the study patients have normal function and are still participating in strenuous impact activities such as marathon running, basketball, and soccer.
Conclusion
In a young, active population, ACL reconstruction using either a hamstring autograft or tibialis posterior allograft provided stability and good to excellent subjective function in the majority (>80%) of patients past 10 years. However, the knees reconstructed with a hamstring autograft demonstrated statistically significant graft survivability when compared with the knees reconstructed with a tibialis posterior allograft. An 8.3% failure rate was demonstrated in knees after reconstruction with an autograft. In contrast, a 26.5% failure rate was found in knees reconstructed with a tibialis posterior allograft. Subjective outcomes and activity levels for those patients in whom the graft did not fail were similar.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Research and institutional support was received from Arthrex Inc and the Musculoskeletal Transplant Foundation. C.R.B. and J.M.T. are consultants for Arthrex Inc.