
Abstract
Background:
For athletes affected by shoulder problems, the most important expectation is to resume sporting activities. The ability to return to sport is related to several parameters, including the type and level of sport played. By focusing on these parameters, the Degree of Shoulder Involvement in Sports (DOSIS) scale allows for a better assessment of the involvement of the shoulder in sports.
Purpose:
To design the DOSIS scale and test its psychometric features.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The DOSIS scale was developed as a patient self-administered scale by the Sport Committee of SIGASCOT (Società Italiana del Ginocchio Artroscopia Sport Cartilagine Tecnologie Ortopediche) to score sports activity based on 3 parameters: (1) type of sport, (2) frequency with which the sport is played, and (3) level at which the sport is played. In a subsequent phase, the psychometric features of the DOSIS scale were measured in a cohort of 85 patients who were affected by recurrent anterior shoulder instability and who underwent an open Bristow-Latarjet procedure or an arthroscopic Bankart repair. The content validity, criterion validity, construct validity, responsiveness, and test-retest reliability were measured and compared with the psychometric features of the Tegner activity scale.
Results:
Neither the DOSIS nor the Tegner activity scale showed floor or ceiling effects, but the DOSIS scale had a different distribution of scores, with a tendency toward a higher percentage of patients with high scores. The test-retest reliability analysis of the DOSIS scale revealed excellent intraobserver reliability (intraclass correlation coefficient = 0.96). Regarding the construct validity, 3 of the 4 hypotheses that we tested were significant. The DOSIS scale showed good criterion validity when compared with the Tegner activity scale (ρ = 0.3, P = .003), and the effect size between the preoperative and postoperative DOSIS scale was 1.1.
Conclusion:
The DOSIS scale showed acceptable psychometric features and seems to be a valid instrument for shoulder assessment in athletes.
The correct assessment of outcomes is mandatory after shoulder surgery. Although a large number of valid tools are available to measure outcomes in the general population, these tools can be less than ideal for the assessment of athletes. 26
Athletes cannot be judged exclusively according to the criteria used for nonathletes. For athletes, the main reason for treatment is usually return to sport, while other parameters such as ability to perform activities of daily life are generally less affected by shoulder problems.25,28 Warth et al, 29 in a study of patients treated by an arthroscopic shoulder procedure, found that the patients’ most important expectation was to continue participation in sporting activities and that resuming their sport was more important to patients than stopping the shoulder from dislocating.
Considering this priority, it is clear that in the assessment of athletes, a scale that measures ability to return to sport is preferred to scales that assess activities of daily living. Several scores and scales have been proposed recently to measure the ability to return to sport.5,7,8 However, these tools have some limitations, one of the main limitations being that they assess the return to sport without considering the type and level of sport being played. These 2 variables are extremely important and are potentially a source of significant bias. For example, it is reasonable to state that the ability to resume a sport after a specific surgery for shoulder instability is different between amateur runners and professional swimmers.
Several methods have been used to control for this confounding factor. One of the most useful is to focus the analysis of outcomes only on specific sports such as rugby 23 or soccer. 12 Unfortunately, this method can be used only by a few high-volume centers that can study sufficient numbers of athletes devoted to the same sport practiced at the same level. Another more common method, generally used when the study population is not homogeneous, is to report the details of the type and sport practiced by a single patient so that the reader can use that information to compare different studies. In this more common scenario, a scale to rank the type and level of sport in homogeneous subgroups with similar involvement of the shoulder could be of great utility.
The Tegner activity scale9,27 is one of the most commonly used scales designed specifically for this purpose. This scale ranks sports activities into subgroups that entail similar involvement of a knee affected by an anterior cruciate ligament lesion. Despite being designed for the knee, the Tegner activity scale has been used for the shoulder.1,24 However, its use for the shoulder raises some obvious concerns. Since the original scale is weighted for the knee, it means, for example, that soccer is scored higher than swimming.
The aim of this study was to design and test a modified Tegner activity scale weighted for the shoulder, called the Degree of Shoulder Involvement in Sport (DOSIS) scale. We hypothesized that the DOSIS scale would have good psychometric features and would provide a more appropriate evaluation of the shoulder compared with the original Tegner activity scale.
Methods
This study includes human subjects. However, in light of the Italian law, no institutional review board approval was mandatory for this study. The study has been performed in accordance with the ethical standards in the 1964 Declaration of Helsinki and has been carried out in accordance with relevant regulations of the Italian National Healthcare System.
Design of the DOSIS Scale
The DOSIS scale was developed by the Sport Committee of SIGASCOT (Società Italiana del Ginocchio Artroscopia Sport Cartilagine Tecnologie Ortopediche) as a patient self-administered scale used to score a sport activity based on 3 parameters: (1) the type of sport classified (no or minimal demand, moderate demand, high demand), (2) the frequency at which the sport was played (occasionally, at least twice a week), and (3) the level at which the sport was played (recreational, low level of competition, high level of competition) (Figures 1 and 2). According to these parameters, the DOSIS scale was calculated by the researchers using an allocation table (see Appendix 1, available online at http://ajsm.sagepub.com/supplemental).
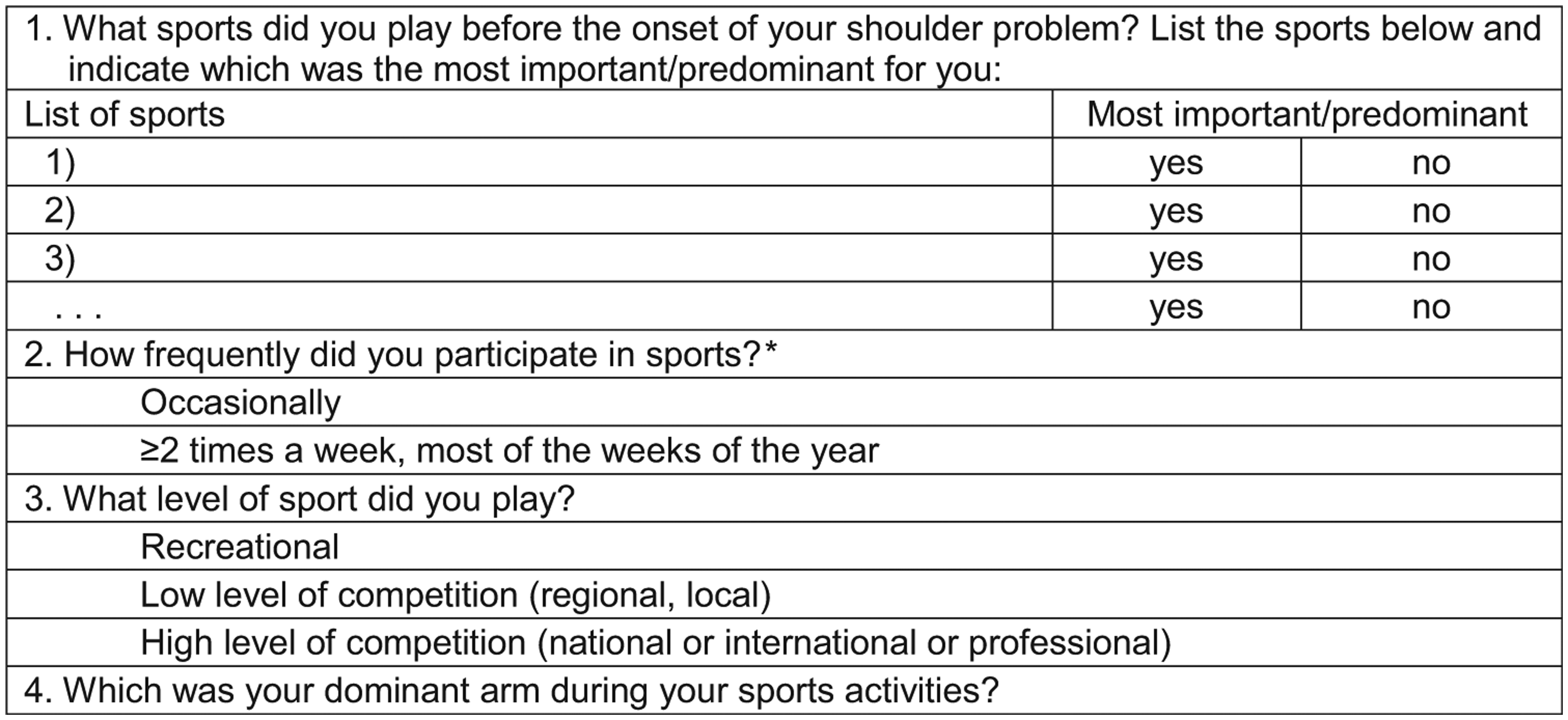
The Degree of Shoulder Involvement in Sports (DOSIS) scale. The scale can be completed either with respect to the sport performed at the time of the follow-up (postoperative DOSIS) or with respect to the sport performed during the period before the onset of the shoulder problem (baseline DOSIS; shown in this figure) or before surgery (preoperative DOSIS). The DOSIS scale was calculated for the most important or predominant sport. The information regarding dominant and nondominant arm was used to classify the sport according to Appendix 2, available online. *For seasonal sports, the frequency during the season was considered.
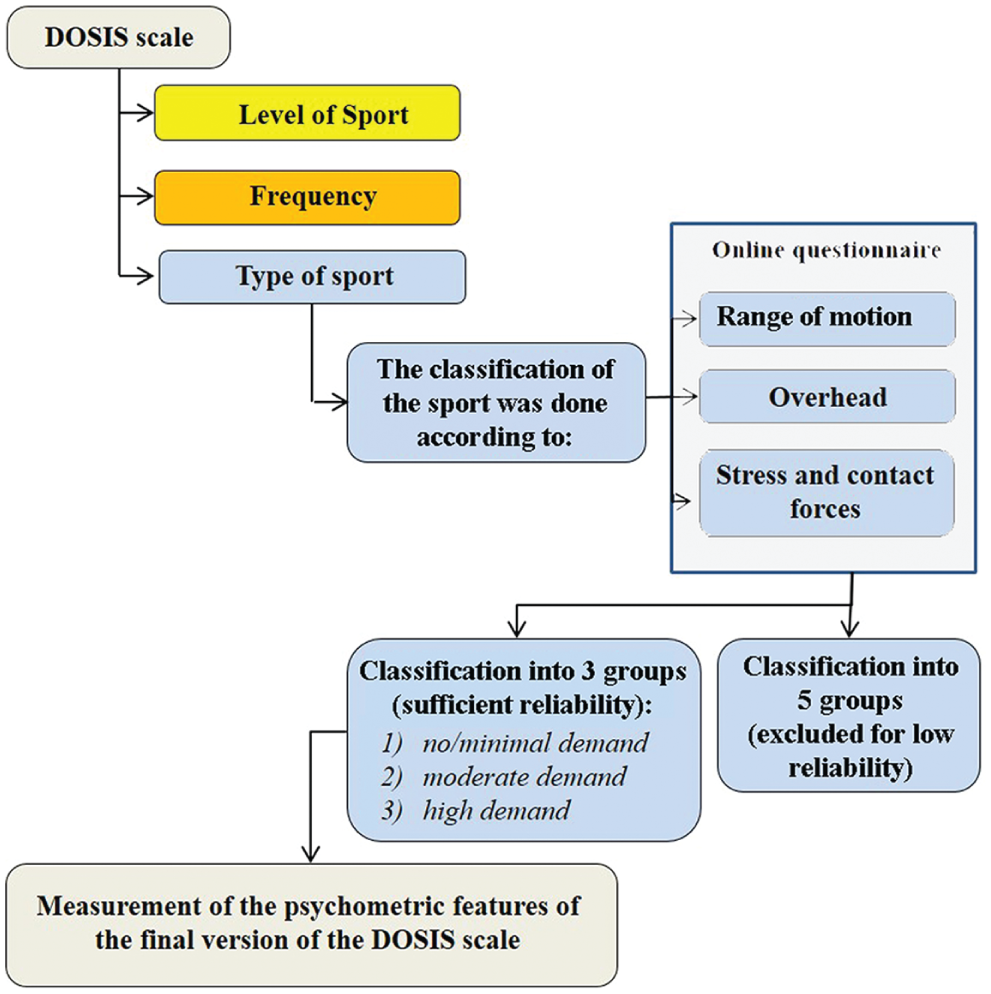
Flow chart summarizing the steps used to design the Degree of Shoulder Involvement in Sports (DOSIS) scale.
Development of the DOSIS Scale
The development of the DOSIS scale followed a stepwise method. The original idea was to rank athletes in homogeneous subgroups according to the type, frequency, and level of sport. Within the Sport Committee, substantial agreement was available for the definitions of the frequency and level parameters. However, the ranking of sports according to type of sport was more predisposed to disagreement. To reduce potential disagreement, the ranking of the sports followed a 2-step process. In the first step, a preliminary questionnaire including a list of 20 common sports and specific positions or roles (eg, goal keeper in soccer) was sent by email to 7 international experts on the shoulder and elbow (from the United States, Italy, Germany, Switzerland, Belgium, Spain, and Turkey). All of them were actively involved in research and teaching in the field of shoulder and elbow treatment and had key positions in the European Society for Surgery of the Shoulder and the Elbow and the American Shoulder and Elbow Society. This questionnaire included 3 questions for each sport that assessed 3 characteristics: (1) whether the sport requires full or almost full range of motion, (2) whether sport is an overhead sport, and (3) the amount of stress and contact forces to the upper extremity while playing that sport. The decision to send a preliminary version of the questionnaire to 7 world experts was taken to address potential clear sources of disagreement between respondents before sending a definite version to the members of SIGASCOT. An analysis of their answers revealed excellent agreement except for sports that required significantly different involvement between the dominant and the nondominant arms.
Following this observation, a definitive new questionnaire that separated the dominant and nondominant arms for some specific sports or positions/roles was created. A question was added regarding the questionnaire respondent’s degree of expertise in sport-related shoulder disorders.
This questionnaire was sent by email to the members of SIGASCOT. This society includes members with different backgrounds and with experience in sport-related trauma. Using the answers to the questionnaire, we initially classified the sports into 5 categories (no or minimal demand, low demand, moderate demand, high demand, and extremely high demand). Subsequently, to reach an interobserver reliability cutoff value of 0.7 (see below), the 5 categories were reduced to 3 categories (no or minimal demand, moderate demand, and high demand) (Table 1).
Classification of Sports According to Demand on the Upper Extremity a
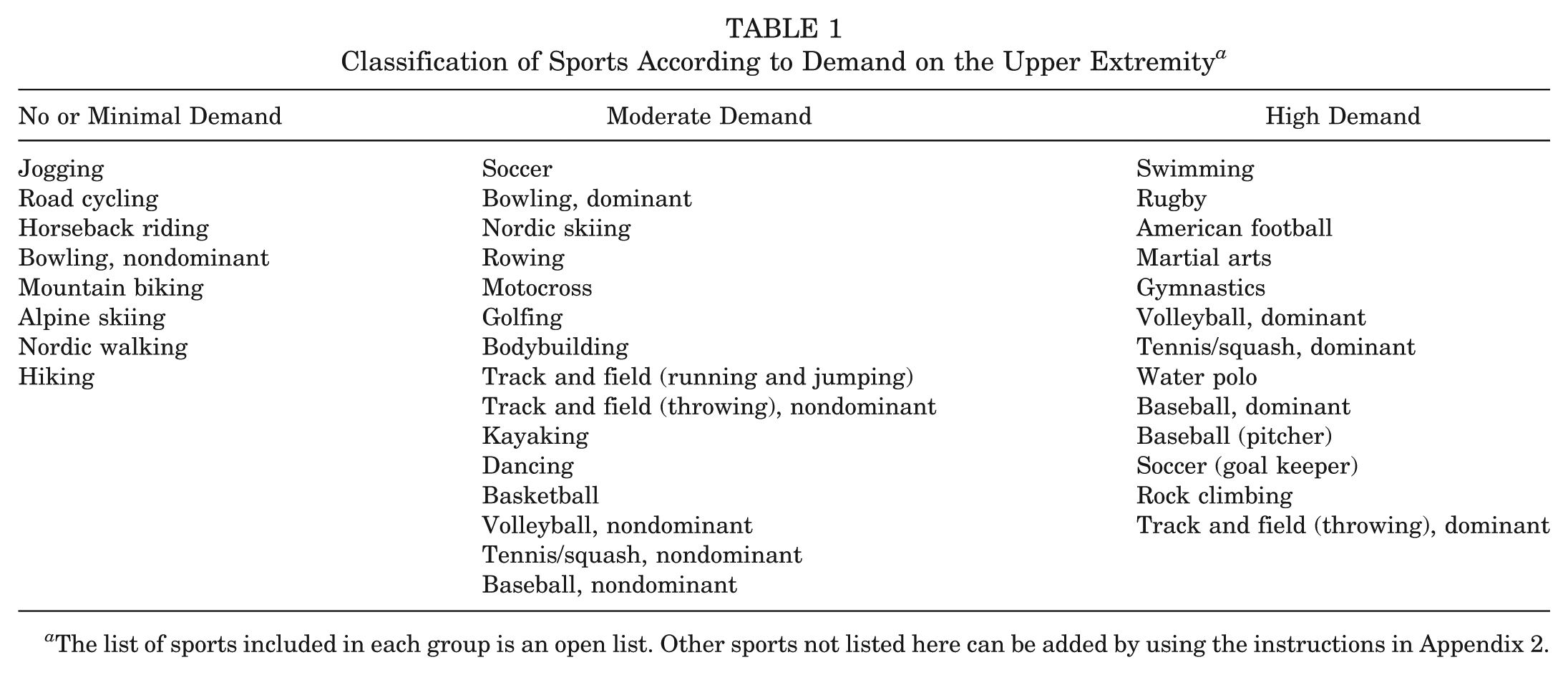
The list of sports included in each group is an open list. Other sports not listed here can be added by using the instructions in Appendix 2.
The specific category into which each sport was placed was determined according to the number of points given for each of the 3 following characteristics (see Appendix 2, available online): (1) range of motion, (2) overhead motion, and (3) amount of stress and contact forces. The definite classification of a sport into a specific category (no or minimal demand, moderate demand, high demand) required a majority agreement between the respondents’ answers on the questionnaire.
For example, 100% agreement between respondents was found for baseball pitching with the dominant arm. All the respondents answered that pitching requires full range of motion, includes an overhead motion, and involves high stress or contact force on the upper extremity. Baseball was accordingly classified as a high-demand sport (Appendix 2).
Based on the classification of sports (Table 1), the frequency at which the sport was played, and the level at which the sport was played, the DOSIS scale was then calculated by use of the allocation table (Appendix 1). For the purpose of this study, the DOSIS scale was calculated only for the most important/predominant sport.
Psychometric Features of the DOSIS Scale
In a subsequent phase, the psychometric features of the DOSIS scale were measured (Figure 3). A cohort of 85 patients who were affected by recurrent anterior shoulder instability and who underwent an open Bristow-Latarjet procedure or an arthroscopic Bankart repair were included in this study. All the patients except 6 were athletes, either amateur or professional (for details, see Figure 4). All patients underwent surgery in 2 university hospitals (Mauriziano-Umberto I Hospital and Cittá della Salute e della Scienza, CTO-Maria Adelaide Hospital). The 2 hospitals are located in the same region of the country, and during the period of the study, each hospital had 1 shoulder unit staffed by 2 expert surgeons and 1 or 2 surgeons in training. Surgery was performed by surgeons not involved in the research. The information collected during the patients’ follow-up examination was used to measure the content validity, criterion validity, and construct validity. The test-retest reliability was measured in a subgroup of 41 patients. During the follow-up examination, the patients were asked to complete the DOSIS scale, Tegner activity scale, 27 Subjective Shoulder Value (SSV) measure, 16 Western Ontario Shoulder Instability Index, 21 and Oxford Shoulder Score for Instability. 13
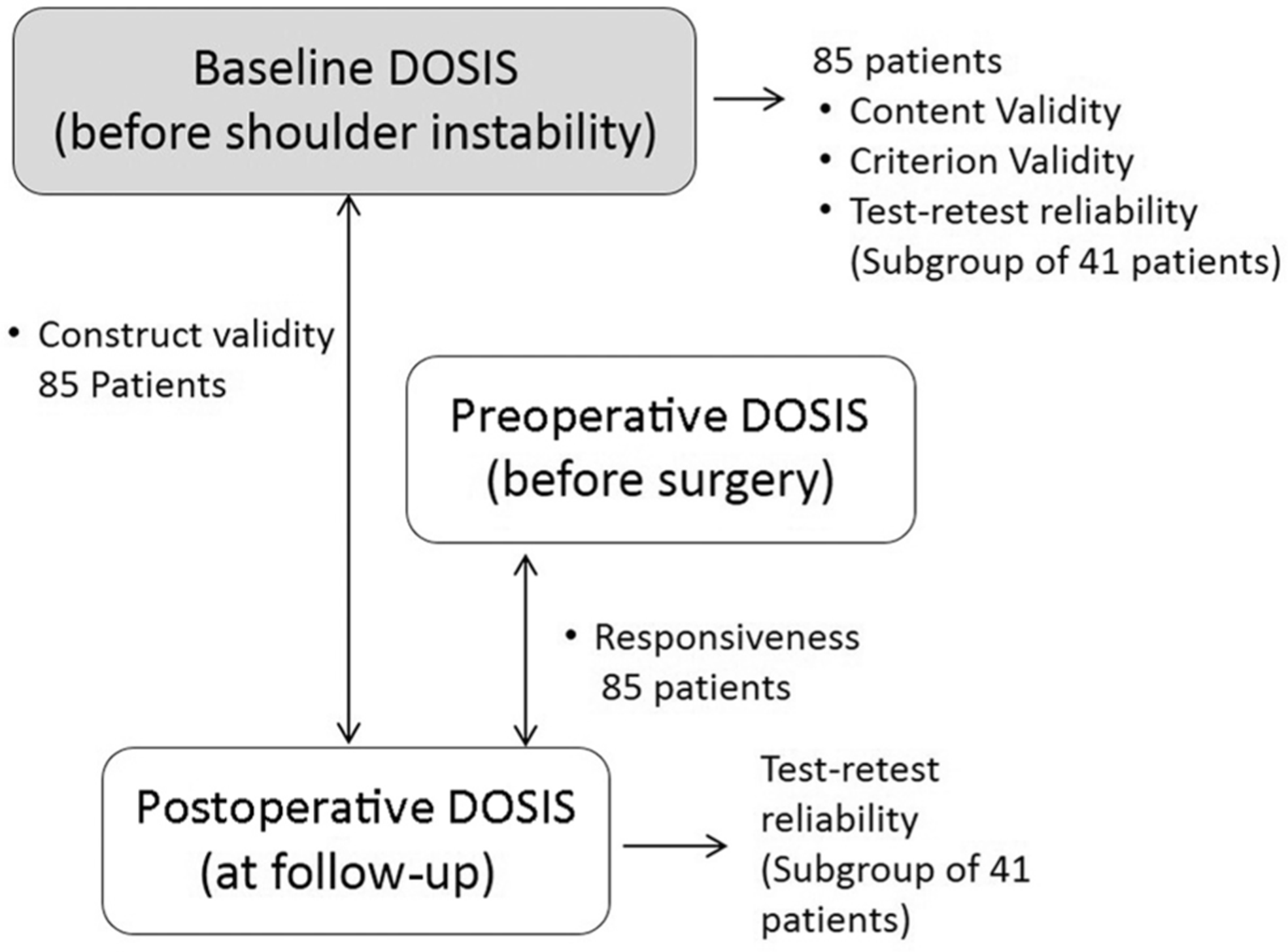
Summary of the psychometric variables measured in the study. DOSIS, Degree of Shoulder Involvement in Sports.
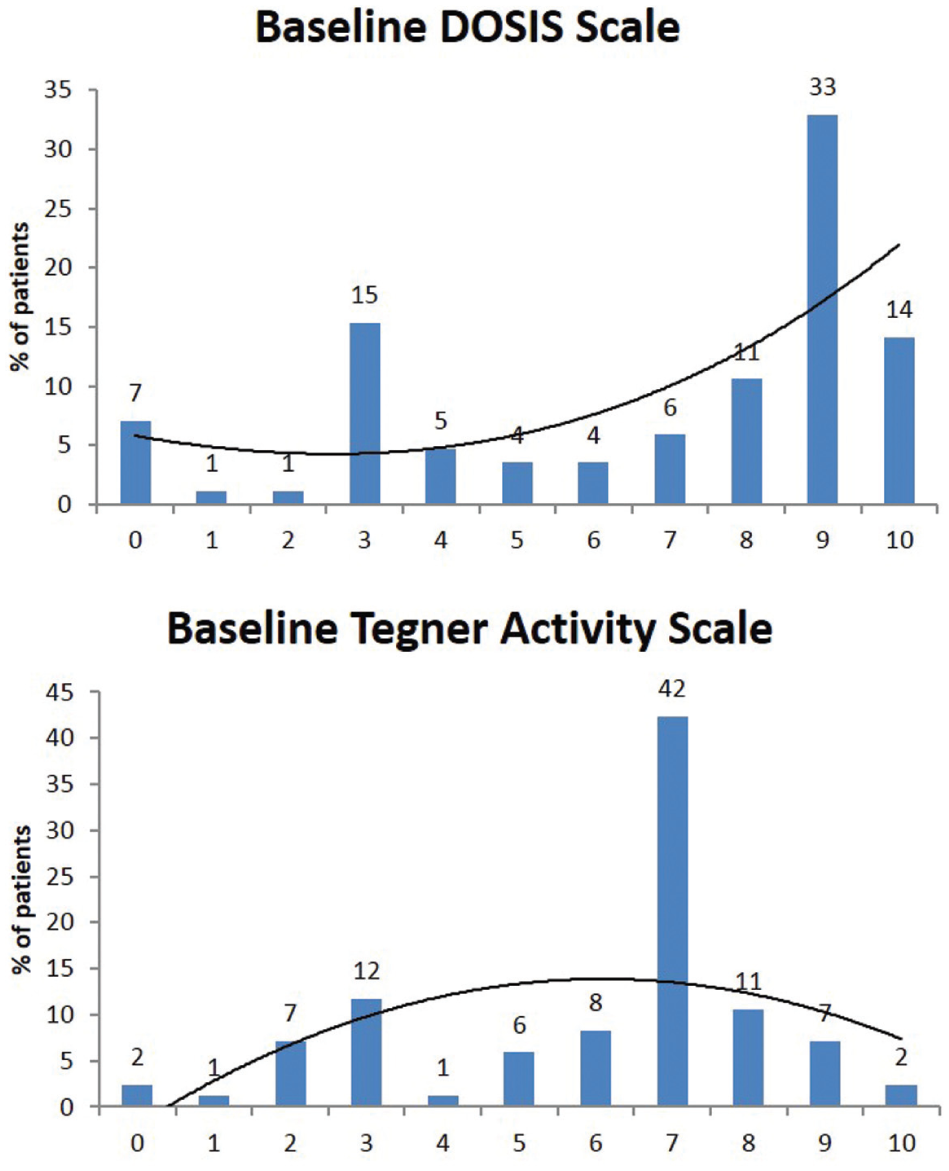
Content validity. Neither the DOSIS nor Tegner activity scales showed a floor or ceiling effect. The DOSIS scale had a different distribution of scores, with a tendency toward a higher percentage of patients with high scores. Moreover, the graph for the DOSIS scale shows that only 7% of patients (n = 6) included in the study were not athletes. DOSIS, Degree of Shoulder Involvement in Sports.
The same DOSIS scale was applied at different time points. The patients were asked to answer the questionnaires retrospectively by recalling the period of time before the onset of shoulder instability (baseline DOSIS), retrospectively before surgery (preoperative DOSIS), and at follow-up examination (postoperative DOSIS) (Figure 3).
Content Validity
Content validity assesses whether the items measure what they are designed to measure and whether they measure the full range of the possible scale. The content validity of the baseline DOSIS scale was shown graphically by reporting the percentage of the patients and the scores they obtained (Figure 4).
The optimal distribution of scores was defined as having less than 30% floor and ceiling effects 20 and having a tendency to increase with an increase in the DOSIS scale. This decision was made in consideration of the hypothesis that in a population of patients affected by shoulder instability, a higher percentage of sports with a higher demand on the shoulder (such as rugby or volleyball) would be expected compared with low-demand sports (such as jogging or cycling).
Test-Retest Reliability
The test-retest reliability of a scale represents its ability to measure the same outcome over time if the conditions of the patient are unchanged.
The test-retest reliability of the DOSIS scale at the time of follow-up (postoperative DOSIS) and before the onset of shoulder instability (baseline DOSIS) was tested in the subgroup of 41 patients who underwent a Bristow-Latarjet procedure. Three weeks before the scheduled appointment, an envelope was sent to the patients containing the DOSIS scale questionnaire (Figure 1). The patients were instructed to answer the questions for the DOSIS scale within 24 hours of receiving the envelope. Two weeks before the planned visit, they were contacted again by telephone to be sure that they had received the questionnaire and had completed it. During the subsequent appointment in the outpatient clinic, the patients were then interviewed and asked to complete the DOSIS scale questionnaire again. The 3 answers to the DOSIS scale questionnaire were used to calculate intraobserver reliability. Bland and Altman analysis 6 and measurement of the intraclass correlation coefficient (ICC) were used to compare the test-retest reliability of the DOSIS scale completed at home with the scales completed in the clinic. An ICC value greater than 70% was considered acceptable. 20
Criterion Validity
Criterion validity represents the ability of a scale to agree with a gold standard that is considered the source of the true measure of the outcome. The criterion validity of the baseline DOSIS was tested by analysis of the correlation between the baseline DOSIS scale and the Tegner activity scale. Although the Tegner activity scale is weighted for the knee, it has been widely used in the literature for the shoulder and no other valid options were available.
Criterion validity was measured by use of the Spearman correlation coefficient (ρ). Correlations >0.5, 0.5-0.35, and <0.35 have been defined in the literature to be strong, moderate, and weak, respectively. 19
Construct Validity
The construct validity of the DOSIS scale was measured considering the hypothesis that a change in the DOSIS scale between the baseline and postoperative DOSIS was due to athletes’ pain and/or difficulty in playing their sport. Moreover, we tested the hypothesis that a reduction in the subjective perception of the shoulder compared with the normal shoulder (SSV) had a direct correlation with the change in the DOSIS scale.
The following 4 hypotheses were tested:
Patients with shoulder pain during sport activity at follow-up would have lower postoperative DOSIS at follow-up compared with the DOSIS before the onset of shoulder instability (baseline DOSIS).
Patients with difficulty in throwing a ball at follow-up would have a lower postoperative DOSIS compared with the baseline DOSIS.
Patients with fear of collision onto the affected shoulder would have a lower postoperative DOSIS compared with the baseline DOSIS.
Patients with lower subjective perception of the affected shoulder compared with the normal shoulder (SSV) would have a lower postoperative DOSIS compared with the baseline DOSIS.
Responsiveness
Responsiveness represents the ability of a scale to recognize differences between preoperative and postoperative status. Responsiveness to change was measured comparing pre- and postoperative DOSIS by calculating the effect size. The effect size is the difference between the postoperative mean values and the preoperative mean values divided by the preoperative standard deviation. A value higher than 0.8% was considered an acceptable value. 20
Statistical Analysis
Interobserver reliability of the classification of the sports into 3 categories and into 5 categories was assessed with the Fleiss kappa—a statistical measure for assessing the reliability of agreement between a fixed number of raters. 14 A limit of agreement of 0.7 was arbitrarily predetermined as the limit to accept the classification. This value was taken arbitrarily due to the lack of other accepted reference values. It has been noted, in fact, that guidelines are missing since the number of categories and subjects will affect the magnitude of the value. 22
If both the classifications had reached the level of 0.7 of agreement, the 5-group classification would have been used.
The DOSIS scale was considered a continuous variable. The Kolmogorov-Smirnov test for normal distribution was applied to the DOSIS scale, showing a distribution of the values significantly distant from a normal distribution (D’Agostino-Pearson test for normal distribution: reject normality, P = .0025). A nonparametric analysis of the data was therefore performed (Spearman correlation and Mann-Whitney test).
Results
A total of 125 members of SIGASCOT replied to the online questionnaire. However, 15 questionnaires were incomplete and were excluded from the analysis. The remaining 110 questionnaires were completed by SIGASCOT members, including 57 who considered themselves to be experts in shoulder disorders. The classification of the sports into 5 categories had a moderate interrater reliability among the shoulder experts (κ = 0.51) and nonexperts (κ = 0.45). The classification of the sports into 3 subgroups increased the reliability of the classification for both experts (κ = 0.71) and nonexpert raters (κ = 0.63). Therefore, the classification of the sports into 3 subgroups was adopted in the definitive version of the DOSIS scale and used for the analysis of intraobserver reliability. The DOSIS scale questionnaire was answered by 85 patients. Forty-four of 85 patients had undergone an arthroscopic Bankart repair and 41 of 85 had undergone a Bristow-Latarjet procedure. The average age at follow-up was 33 years (range, 19-63 years), 75 of the patients were male, and the average follow-up from surgery was 5.2 years (range, 2-9.8 years).
Content Validity
Content validity is graphically reported in Figure 4. The median Tegner activity scale was 7 points, and the median baseline DOSIS scale was 8 (Mann-Whitney test, P = .007). Neither of the 2 scales showed a floor or ceiling effect; however, there was a different distribution of scores between them, with a tendency for a higher percentage of patients with high scores when the DOSIS scale was used.
Test-Retest Validity
The test-retest validity analysis was performed on the 41 patients in the Bristow-Latarjet group. In this group, the average age at follow-up was 31 years (range, 19-45 years), 36 patients were male, and the average follow-up from surgery was 5 years (range, 2-8.6 years).
Both administrations of the DOSIS scales, baseline and postoperative, had excellent intraobserver reliability. For the baseline DOSIS, the systematic error between the first and the second assessment of the DOSIS scale at follow-up was 0 points with a 95% upper limit of agreement of 0.88 points. The ICC was 0.96 (95% IC, 0.99-0.93). For the postoperative DOSIS, the systematic error between the first and the second assessment of the DOSIS scale at follow-up was 0 points with a 95% upper limit of agreement of 0.6 points. The ICC was 0.97 (95% CI, 0.99-0.95).
Construct Validity
Of the 4 hypotheses tested, 3 were significant. Patients with shoulder pain during sport activity had lower (but not statistically significant) postoperative DOSIS compared with their baseline DOSIS (ρ = 0.1, P = .7); patients with difficulty throwing a ball had lower postoperative DOSIS compared with their baseline DOSIS (ρ = 0.25, P = .04); patients with fear of collision onto the affected shoulder had lower postoperative DOSIS compared with their baseline DOSIS (ρ = 0.3, P = .01); and patients with lower subjective perception of the affected shoulder compared with the normal shoulder (SSV) had a lower postoperative DOSIS compared with their baseline DOSIS (ρ = 0.4, P = .002).
Criterion Validity and Responsiveness
The baseline DOSIS scale showed good criterion validity when compared with the Tegner activity scale (ρ = 0.3, P = .003).
Regarding responsiveness, the effect size between the preoperative and postoperative DOSIS scale was 1.1.
Discussion
The aim of this study was to design and test a scale for assessing athletes before and after shoulder surgery in a manner similar to what has been successfully done with the Tegner activity scale for the knee. The aim of this scale is to help the physician classify patients on the basis of their sport activity, according to specific involvement of the shoulder in that sport. The scale is not intended to indicate whether the patient is ready to return to sports.
Our hypotheses were that the DOSIS scale has acceptable psychometric features and that it has distinct features that are comparable with the original Tegner activity scale, providing a different distribution of scores. These hypotheses were satisfied with the exception of the validation of the pain component. A poor correlation was found between the DOSIS scale and “pain during sport activity.” The reasons for this poor correlation could be that athletes affected by shoulder instability are usually not significantly impaired by pain at follow-up and that reduction in sport performance is related to causes other than pain.11,15
The psychometric features of the DOSIS scale were comparable overall to those of the Tegner activity scale. Briggs et al 9 tested the psychometric features of the Tegner activity scale on approximately 500 patients. The investigators found an ICC of 0.82, compared with 0.97 in our study. This difference could be related to chance and might not be relevant. However, a possible explanation is that in our study, the patients did not choose the score that fit their activity status, as is normally done for the Tegner activity scale, but rather the score was assigned by the researcher using an allocation table. This different approach could have increased the reliability of our results. Another explanation could be that the DOSIS scale assessed only the realm of sports while the Tegner activity scale is designed to also score the patient’s occupational activity.
The test-retest reliability for the DOSIS before the onset of the shoulder pathologic condition (baseline DOSIS) and the DOSIS at follow-up (postoperative DOSIS) was measured in this study. This approach was taken because the DOSIS scale was designed to assess both pre- and postoperative conditions. As expected, the reliability of the DOSIS scale assessed retrospectively was lower than that of the DOSIS scale at follow-up. However, both administrations of the DOSIS scale had excellent reliability.
Regarding content validity, the DOSIS scale had a different distribution of possible scores compared with the original Tegner activity scale, although neither score had significant floor or ceiling effects. The DOSIS scale had a significantly greater median value compared with the Tegner activity scale and a tendency toward higher scores. These can be viewed as positive attributes since athletes affected by shoulder instability tend to play sports that pose a higher risk for shoulder dislocation; sports that are scored with higher points with the DOSIS scale are comparable with sports that pose major risk for knee instability.
Numerous valid scores and scales are available in the literature for assessment of the shoulder, and one could argue that a new scale is not necessary. However, regarding shoulder instability in athletes, proper outcome assessment is still controversial.
Stein et al 26 focused on shoulder sport-specific impairments after arthroscopic Bankart repair. The investigators concluded that sport-specific impairments are not detectable by established clinical score systems. Furthermore, Archetti Netto et al, 4 comparing arthroscopic and open techniques for the treatment of Bankart lesions, found no differences when using established scores for instability (Rowe and University of California, Los Angeles [UCLA] scores). Remarkably, the investigators found differences in scores when using the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire—a score not specifically designed for shoulder instability.
Grumet et al 17 performed a systematic review comparing arthroscopic stabilization for first-time surgeries versus surgeries for recurrent shoulder instability. The investigators concluded that there were no apparent differences in outcomes between first-time instability and recurrent instability. They also concluded that additional randomized controlled trials were needed to specifically compare patients’ abilities to return to preinjury activity levels.
The return to preinjury activity level is a priority for an athlete. Warth et al, 29 in a recent study of patients treated by an arthroscopic procedure, found that the most important expectation was continued participation in sporting activities. Interestingly, the patients who sought treatment for shoulder instability valued their continued participation in sports more than they valued stopping their shoulder from dislocating. This study suggests that the assessment of the rate of recurrent dislocation, although important, could be considered to be of secondary importance in athletes treated for recurrent shoulder instability.
In line with these considerations, Castagna et al 11 reported the outcomes of arthroscopic stabilization of the shoulder in adolescent athletes participating in overhead or contact sports. The investigators found a 21% rate of recurrence but found no evidence of a difference in clinical scores in the patients who had a dislocation recurrence. If return to sport is our patients’ main goal, assessment of the return to sport should be considered a primary outcome.
In a recent study using a pair-matched design, Bessière et al 5 compared 2 cohorts of patients affected by recurrent shoulder dislocation and treated with open Latarjet or arthroscopic Bankart procedures. One of the primary outcomes used for this purpose was the Subjective Shoulder Value Sport, a simple score in which the patient ranks his or her operated shoulder between 0% and 100% specifically for the practice of sport.
Another useful score designed to assess the return to sport is the SPORTS score, a patient-completed measure that evaluates (1) the ability to perform the same sport with the same level of effort and training, (2) the ability to reach the same level of performance, and (3) the ability to do these without or despite pain.7,8
These scores, although useful, cannot be used alone since they do not account for the type and level of sport played before surgery—variables that can be considered to be the missing pieces of the puzzle in outcomes measurement.
Allain et al 3 classified the type of sport according to the potential risk of injury in 4 groups, taking into account the amount of impact involved in the sport, the presence of overhead motion with hitting movements, and the presence of overhead motion and sudden stops. We included these variables in the DOSIS scale and added the range of motion required by the specific sport. Moreover, the DOSIS scale takes into account the level of sports and the frequency at which the sport is practiced. All of these variables are used to determine a final score ranging from 0 to 10 points that can be used to assess the study cohort preoperatively, to easily compare different studies, or to inform the follow-up examination.
Brophy et al 10 described an activity scale for shoulder that takes into account several features, such as carrying an object 8 lb or heavier by hand, handling objects overhead, and participating in contact and overhead sports. Similar to the DOSIS scale, the activity scale for shoulder was designed specifically to assess the level of activity. However, it does not specify particular sports. Different from this scale, the DOSIS scale considers different sport activities and the level and frequency at which the sport is or was played. We believe that these are essential features that characterize an athlete and need to be considered in a score.
We designed the DOSIS scale because of the lack of a valid tool to stratify athletes in homogeneous subgroups with similar involvement of the shoulder. The ability to compare outcomes between homogeneous groups is a key element in evidence-based medicine. The DOSIS scale was not originally conceived to be used alone to assess outcomes after shoulder surgery; rather, it assesses the level and type of sport activity performed by the athletes. For the evaluation of outcomes, other scores are more appropriate, such as the SPORTS score, 7 the Kerlan-Jobe Orthopaedic Clinic (KJOC) score, 2 and the DASH sports/performing arts module. 18 We believe that the average and range of scores on the DOSIS entail important information that complements the other available scales and scores.
Before the DOSIS scale is used in clinical practice, we must underline some limitations of this study. A limitation of this study is that although the DOSIS scale is an ordinal variable (0-10), it was analyzed as a continuous variable. This approach has been used previously by others to simplify the calculation of the psychometric features of a scale. 9
Another limitation is that the data were collected in a retrospective manner in part, since we asked patients to recall their sport activity levels (baseline and preoperative DOSIS). We chose to measure the psychometric features of the DOSIS scale retrospectively because this is the most common clinical scenario we face: When addressing an athlete’s return to sport, we must elucidate the patient’s sport activities before the onset of his or her shoulder condition.
The relevancy of this limitation was tested by comparing the test-retest reliability of the DOSIS scale measured retrospectively and the DOSIS scale measured at follow-up (postoperative DOSIS). We did not find significant differences, suggesting that the DOSIS scale is reliable even when it is measured retrospectively.
Another limitation is that the DOSIS scale has been tested in patients affected only by shoulder instability and not by other shoulder conditions. Although originally the DOSIS scale was designed to be used with degenerative disorders of the shoulder, the psychometric features measured in this study cannot be extrapolated to such a cohort of patients. We chose to begin assessment of the DOSIS scale in a population of athletes affected by shoulder instability because we thought that the need for the DOSIS scale was greater in this group of athletes. This limitation should be considered before the DOSIS scale is used for conditions other than shoulder instability.
Other limitations are that a power analysis was not performed and that for the purpose of measuring the psychometric features of the DOSIS scale, we selected to use the DOSIS scale only to describe the most important/predominant sport for each athlete. This does not preclude the possibility that for patients who practice different sports, a separate DOSIS scale can be used to define each sport.
Future prospective studies are needed to validate the DOSIS scale in larger cohorts of athletes, including analyses of different sports played by the same athlete affected by other shoulder conditions.
Conclusion
A pool of experts in sport-related injuries of the shoulder were interviewed to design the DOSIS scale. The DOSIS scale, when tested in a cohort of patients affected by shoulder instability, showed acceptable psychometric features and provided a sport-specific assessment of the shoulder compared with the original Tegner activity scale.
Footnotes
Acknowledgements
The authors thank all the members of the SIGASCOT for their answers to the questionnaire and the members of the Sport Committee of the SIGASCOT.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.