
Abstract
Background:
Recent literature has demonstrated that involvement in pivoting sports at the time of injury, increased posterior-inferior tibial slope (PITS), anterolateral capsular ligament (ALCL) disruptions, and combined lateral meniscal lesions all contribute to a higher grade of pivot shift after acute anterior cruciate ligament (ACL) injuries.
Purpose:
To identify risk factors associated with grade 3 pivot shift after acute ACL injuries.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A database of patients undergoing primary ACL reconstruction from 2009 to 2015 after acute ACL injuries was retrospectively reviewed. A total of 30 patients (30 knees) with grade 3 pivot shift were identified as the study group. Moreover, 30 patients (30 knees) with grade 1 and 30 patients (30 knees) with grade 2 pivot shift were randomly chosen as the 2 control groups. All pivot-shift tests were performed with the patients under anesthesia. Predictors of grade 3 pivot shift that were explored included patient age, sex, time from injury to surgery, pivoting sports involvement at the time of injury, lateral PITS, medial PITS, ALCL disruptions, preoperative KT-1000 arthrometer side-to-side difference, and combined lateral or medial meniscal lesions. Comparisons were performed between the study group and the 2 control groups. Univariable and multivariable logistic regressions were used to identify independent risk factors that were associated with grade 3 pivot shift.
Results:
Univariable and multivariable logistic regressions between the study group and the 2 control groups showed that pivoting sports involvement at the time of injury (odds ratio1 [OR1; grade 3 vs grade 1 pivot shift with grade 1 = reference], 11.88; 95% CI, 1.94-149.91; OR2 [grade 3 vs grade 2 pivot shift with grade 2 = reference], 3.41; 95% CI, 1.92-22.60), abnormal degree of lateral PITS (OR1, 14.41; 95% CI, 1.69-174.78; OR2, 6.41; 95% CI, 1.48-47.70), ALCL disruptions (OR1, 8.28; 95% CI, 1.71-117.14; OR2, 4.96; 95% CI, 1.07-28.75), and combined lateral meniscal lesions (OR1, 27.56; 95% CI, 5.48-240.52; OR2, 5.83; 95% CI, 1.21-38.56) were independent risk factors of grade 3 pivot shift after acute ACL injuries.
Conclusion:
For acute ACL injuries, the best set of predictors of grade 3 pivot shift were pivoting sports involvement at the time of injury, abnormal lateral PITS, ALCL disruptions, and combined lateral meniscal lesions. These results may provide additional information for counseling patients on residual laxity and risks for graft rerupture after ACL reconstruction.
The pivot-shift test is the most specific clinical assessment of pathologic knee joint rotational laxity after complete anterior cruciate ligament (ACL) injury when it is performed with the patient under anesthesia.18,36 The test evaluates the combined tibiofemoral internal rotation and anterior tibial translation that occur when the ACL is injured, and the pathologic motion elicited during the test is recorded as grade 0 (normal), grade 1 (glide), grade 2 (clunk), or grade 3 (locked subluxation) according to the International Knee Documentation Committee classification. 9 A grade 3 pivot shift has been shown to correlate with poorer clinical outcomes 34 as well as earlier progression of knee osteoarthritis. 17 Despite extensive clinical and biomechanical research involving the pivot-shift mechanism, there is still a paucity of knowledge about the risk factors responsible for a grade 3 pivot shift.
It has been shown that in the laboratory setting, isolated ACL transection almost never produces a pivot shift greater than grade 2. 22 Recent literature has demonstrated that lateral compartment translation of the knee joint correlates well with the clinical grade of pivot shift. 2 Brandon et al 3 showed that for ACL-ruptured knees, a steeper posterior-inferior tibial slope (PITS) could result in increased anterior tibial translation during the pivot-shift test, which was contributory to a higher grade of pivot shift. Moreover, an increase in the grade of pivot shift has also been noted with combined injuries to the lateral structures in the ACL-deficient knee. 34 In a cadaveric study conducted by Musahl et al, 24 a complete lateral meniscectomy in an ACL-deficient knee resulted in an additional increase of 6 mm for the lateral compartment translation during a simulated pivot-shift maneuver. The authors concluded that the lateral meniscus was an important secondary stabilizer to rotational forces when the ACL is ruptured. Monaco et al 22 further described the role of the anterolateral capsule in maintaining the tibial rotational stability. They found an increased grade of pivot shift in all cadavers after transecting the anterolateral capsular ligament (ALCL) in ACL-deficient knees, suggesting that ALCL disruptions might be a secondary factor causing an increase in the grade of pivot shift after ACL injuries.
Identifying predictors associated with grade 3 pivot shift after acute ACL injuries could help to identify those most at risk. In addition, knowledge of these predictors may provide additional information for counseling patients on risk of residual laxity and graft rerupture after ACL reconstruction, which may influence choice of surgical treatment in patients with grade 3 pivot-shift instability.23,25
The purpose of this study was to identify risk factors associated with grade 3 pivot shift after acute ACL injuries. We explored several pre- and intraoperative factors that may be associated with the grade 3 pivot shift, including patient age, sex, time from injury to surgery, pivoting sports involvement at the time of injury, lateral PITS, medial PITS, ALCL disruptions, preoperative KT-1000 arthrometer side-to-side difference, and combined lateral or medial meniscal lesions. On the basis of the results of previous studies, we hypothesized that for acute ACL injuries, ≥1 risk factors associated with grade 3 pivot shift would be identified.
Methods
Patient Selection
From December 2009 to January 2015, a total of 1454 consecutive patients from a single institution (Beijing Jishuitan Hospital, Beijing, China) with clinically diagnosed ACL injury underwent ACL reconstruction. For the definition of acute ACL injury phase, the interval from injury to surgery had to be ≤3 weeks. Additionally, the contralateral knee joint had to be intact to evaluate the side-to-side difference during physical examination. Patients excluded from the study met at least 1 of the following criteria on the injured side: (1) partial ACL tear; (2) combined posterior cruciate ligament injury, posterolateral corner injury, or grade 3 medial collateral ligament injury; (3) severe intra-articular degeneration of the cartilage (Outerbridge grade 3 or 4); (4) severe malalignment of the lower extremity; (5) general joint laxity; (6) history of previous knee surgery; and (7) combined periarticular fractures. This study was approved by the ethics board at our institute and complied with the patients’ consent.
A total of 489 patients who suffered from acute ACL injury were analyzed retrospectively by a systematic review of office and operative records. We included patients according to the results of preoperative pivot-shift tests. All pivot-shift tests were performed with the patients under anesthesia by the senior surgeon, who had >20 years of orthopaedic training. Of the 489 patients, 30 were verified as having a grade 3 pivot shift. This patient group was our study group. Moreover, from the remaining 459 patients, 30 patients with grade 1 pivot shift and 30 patients with grade 2 were randomly chosen for comparison. These were our 2 control groups.
Evaluation Methods
The preoperative status—including patient demographic data, magnetic resonance imaging (MRI) scans, and physical examination with the patient under anesthesia—as well as the intraoperative findings during arthroscopic ACL reconstruction were analyzed individually and then compared between groups.
Demographic Data
Age, sex, and the time from injury to surgery were recorded. In addition, the sports activity of the patient at the time of ACL injury was categorized into pivoting and nonpivoting sports according to the classification by Hefti et al. 12 Sports with frequent pivoting (eg, soccer, basketball, handball, volleyball, alpine skiing, snowboarding, and tennis) were classified as pivoting sports. Sports with no pivoting (eg, running, walking, and weight lifting) were classified as nonpivoting sports. 11
MRI Scans
The preoperative MRI scans were reviewed by 2 radiologists with expertise in musculoskeletal imaging who were blinded to this study. The MRI scans were performed on a 1.5-T MRI unit (Sigma; GE Medical Systems) for all patients in both groups. The MRI protocols included coronal, sagittal, and axial sequences. Each sequence included the T1-weighted, T2-weighted, and fat-suppressed T2-weighted phases.
Measurements of the PITS with T1-weighted MRI were performed according to a 3-step method of Hudek et al 16 (Figure 1). Both the medial and lateral PITSs were measured. Since abnormal values of the PITS in ACL injuries have not yet been clearly defined, we calculated the mean and standard deviation of our 2 control groups (n = 60) and considered ≥2 standard deviations from the mean to be abnormal (≥10.6° for lateral PITS; ≥9.4° for medial PITS). 31
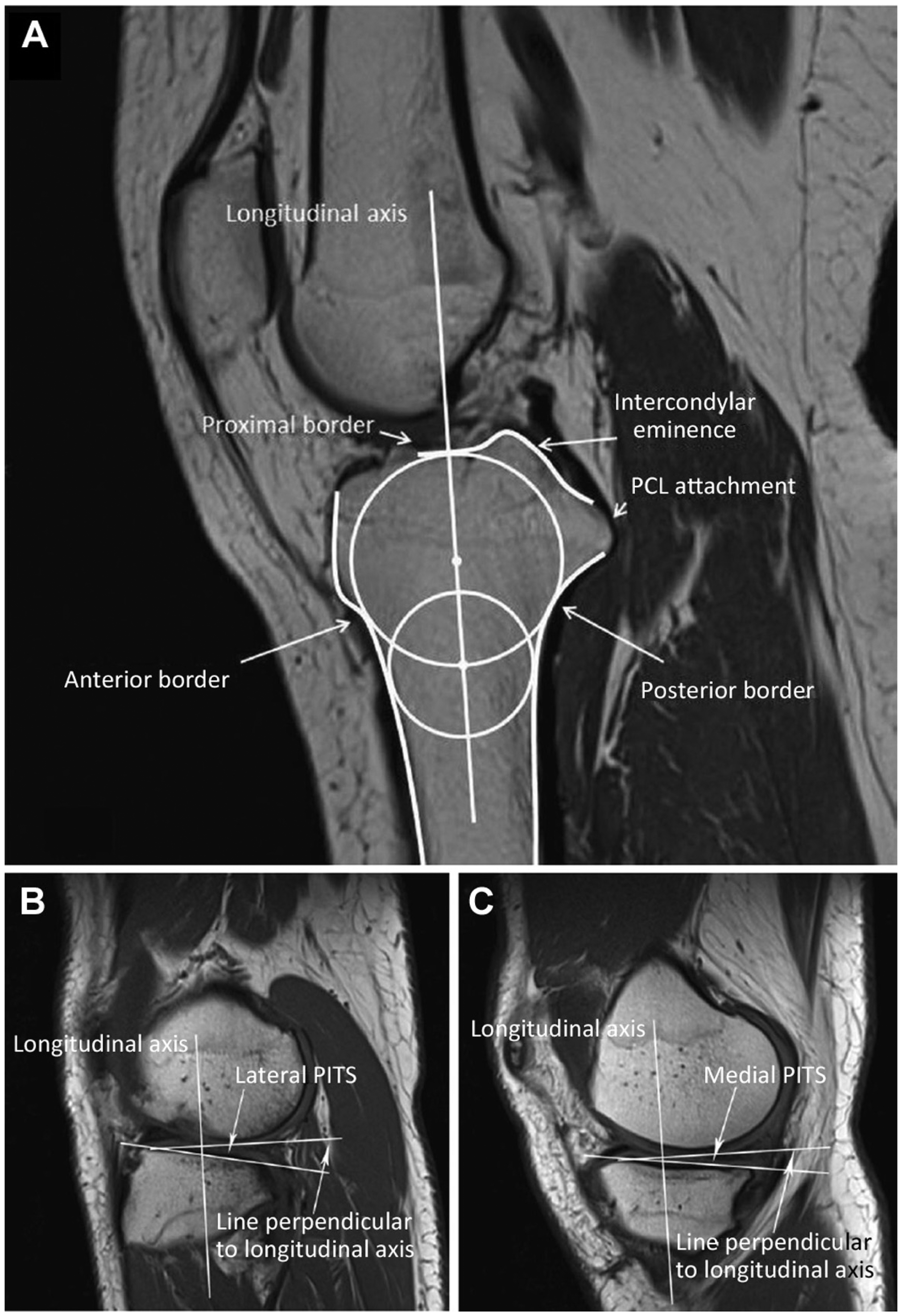
The 3-step procedure proposed by Hudek et al 16 for measuring the posterior-inferior tibial slope (PITS) by conventional magnetic resonance imaging. (A) The first step was to define the central sagittal slice, which consisted of the intercondylar eminence, the anterior and posterior tibial cortices appearing as a concave shape, and the tibial attachment of the posterior cruciate ligament (PCL). The second step was to draw a circle tangent to the proximal, anterior, and posterior tibial borders and then a second circle centered on the perimeter of the first circle. The line connecting the centers of the circles was defined as the tibial longitudinal axis. (B, C) The last step was to measure the angle between the line perpendicular to the tibial longitudinal axis and the tangent to the medial and lateral tibial plateaus. The tangent to the medial and lateral tibial plateaus was defined as the line connecting the uppermost of sites on the superoanterior and posterior cortices on the middle slice between the most mediolateral slice and the central sagittal slice. For this patient with grade 3 pivot shift, the measured lateral PITS and medial PITS were 11.5° and 9.5°, respectively.
The ALCL was examined on the T2-weighted coronal plane reconstructions according to a previously described method. 5 The ALCL was considered to be normal if low–signal intensity fibers were seen arising from the lateral epicondyle of the distal femur, running slightly oblique to the anterolateral border of the proximal tibia, and passing parallel to the medial edge of iliotibial band. The ALCL was determined to be abnormal in case of complete disruption of the ligament (all fibers discontinuous), if the contour of the ALCL was marked irregular, if intra- or periligamentous edema existed, or if a combination of these MRI features was observed (Figure 2). The 2 radiologists separately reviewed the MRI scans, and the ALCL was determined to be normal or abnormal only when both radiologists reached an agreement; otherwise, the final decision was made by the senior surgeon.
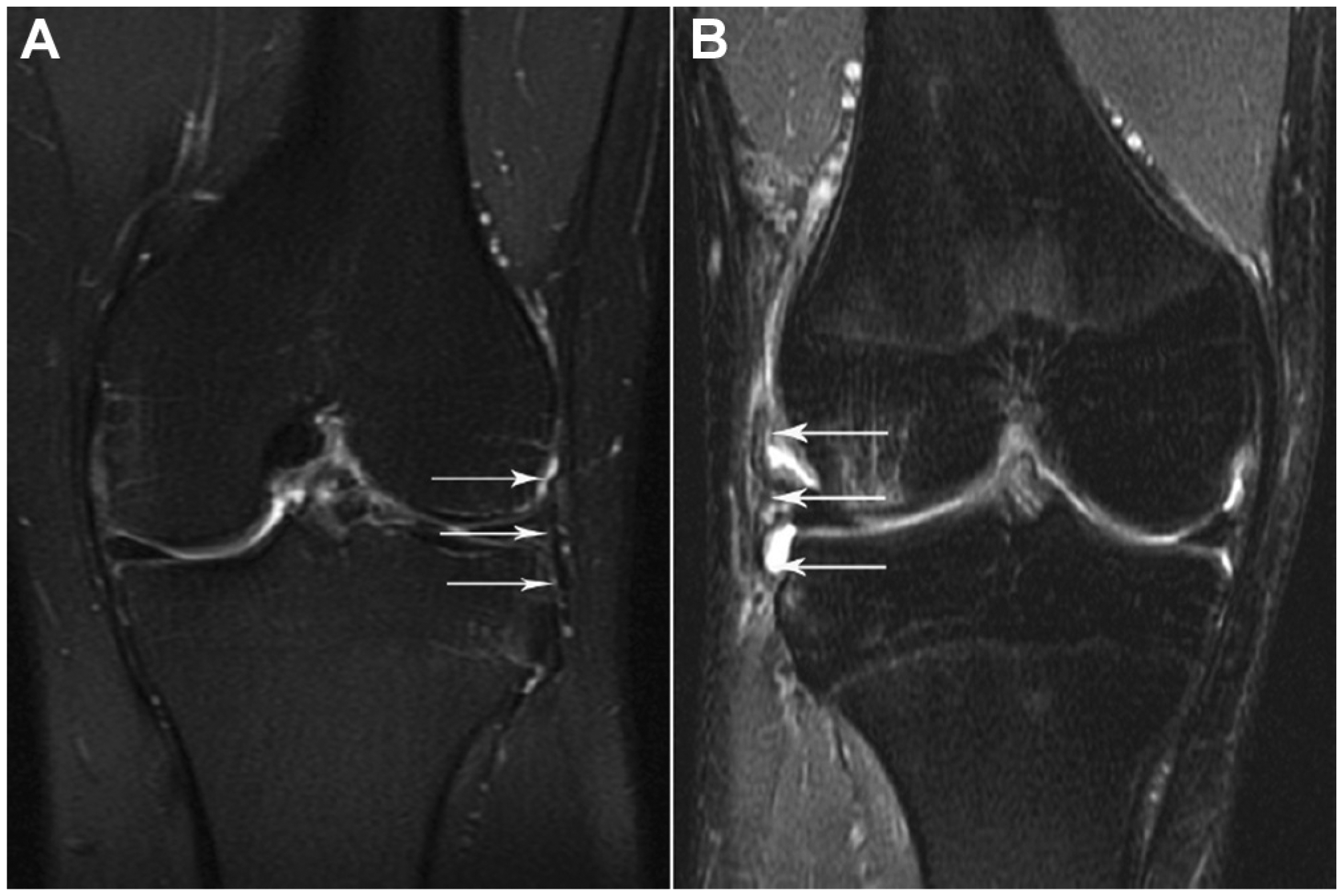
Representative magnetic resonance images of (A) normal anterolateral capsular ligament (ALCL) with low–signal intensity continuous fibers (arrows) and (B) disrupted ALCL with discontinuous fibers (arrows) and periligamentous edema seen on the T2-weighted coronal planes.
To determine the inter- and intraobserver reproducibility, the intraclass correlation coefficients (ICCs) were calculated by randomly selecting 20 patients (10 from the study group and 10 from the control group); ICC values >0.9 were considered excellent, and values between 0.8 and 0.9 were considered good. 13 Two radiologists who were blinded to the study separately measured the lateral and medial PITSs and defined the status of the ALCL. In addition, 1 independent observer performed all the above MRI evaluations on each of the selected patients twice, 2 weeks apart. The inter- and intraobserver ICCs were 0.91 and 0.93 for the lateral PITS measurement, 0.90 and 0.92 for the medial PITS measurement, and 0.85 and 0.88 for the definition of the ALCL status, respectively.
Physical Examination
The senior surgeon individually conducted the KT-1000 measurements for each patient and personally recorded the results. The KT-1000 measurements were also performed with the patient under anesthesia by maximal manual forces and were recorded as side-to-side differences. In this study, the KT-1000 arthrometer side-to-side difference was divided into <5 mm (normal or nearly normal) and ≥5 mm (abnormal or severely abnormal) according to International Knee Documentation Committee classification.
Intraoperative Findings
All medial and lateral meniscal lesions were systematically documented according to the representative images and videos recorded before the ACL reconstruction under arthroscopy.
Data Management and Statistical Analysis
For this study, potential risk factors for grade 3 pivot shift that were explored included patient demographic data (age, sex, time from injury to surgery, and pivoting sports involvement at the time of injury), MRI scans (lateral PITS, medial PITS, and ALCL disruptions), physical examination (preoperative KT-1000 side-to-side difference), and intraoperative findings (combined lateral or medial meniscal lesions) (Table 1). Comparisons were performed between the study group and the 2 control groups. We used the Pearson chi-square test or Fisher exact test to compare categorical variables and the Student t test to compare continuous variables. Univariable and multivariable logistic regression analyses were then performed to determine the independent risk factors that best predicted the presence of grade 3 pivot shift after acute ACL injuries. Subgroup analysis was further performed on patients with combined risk factors. If a patient had ≥2 risk factors, he or she would be defined as a high-risk individual. Inter- and intraobserver reproducibility was determined by the ICC. P < .05 was considered statistically significant. Analyses were performed with the SPSS 18.0 software package (IBM Corp).
List of Potential Variables a
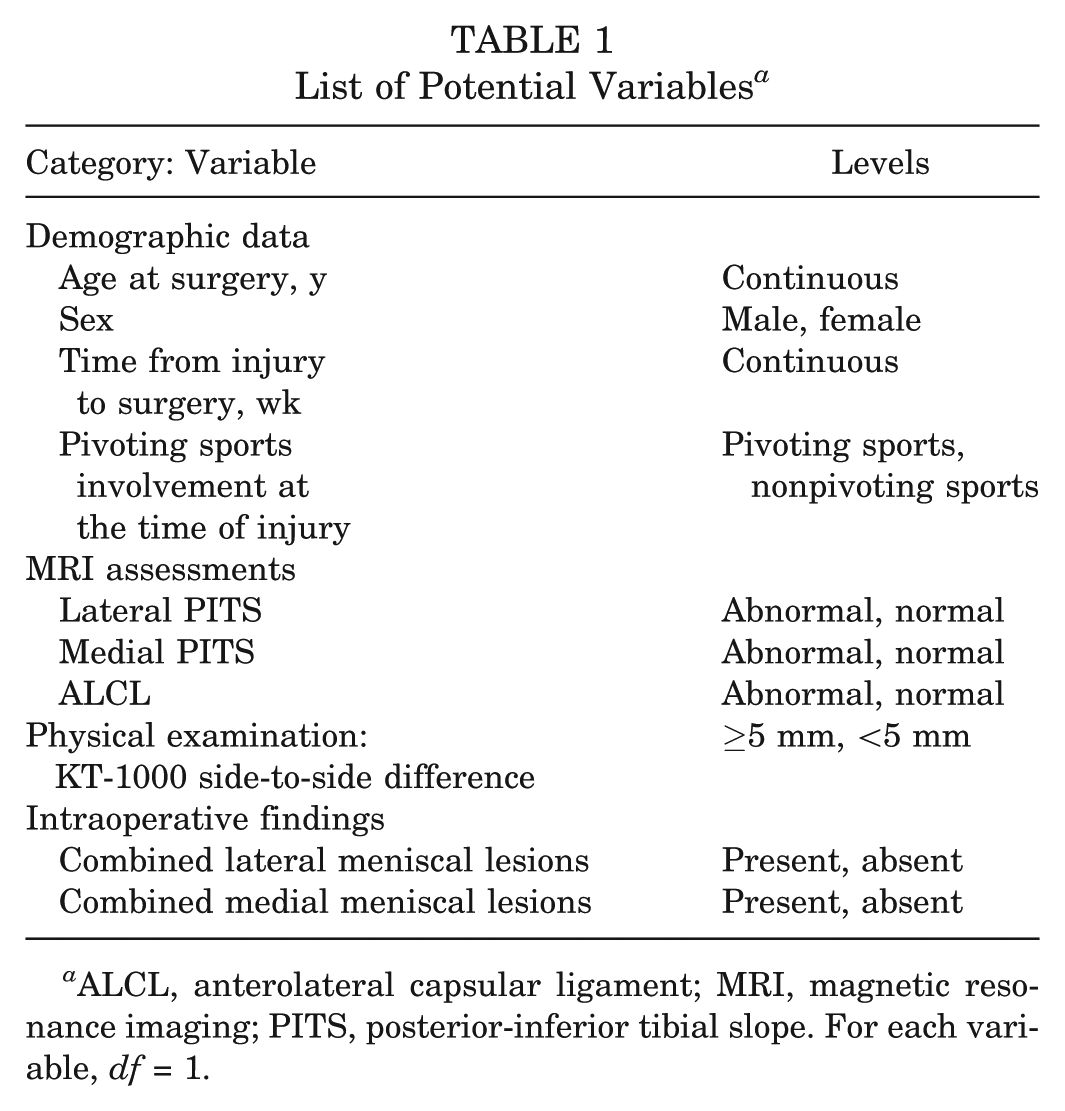
ALCL, anterolateral capsular ligament; MRI, magnetic resonance imaging; PITS, posterior-inferior tibial slope. For each variable, df = 1.
Results
Based on the results of pivot-shift tests performed under anesthesia, there were a total of 30 patients with grade 3 pivot shift enrolled in the study group. Moreover, 30 patients with grade 1 pivot shift and 30 patients with grade 2 were included in the 2 control groups.
Table 2 shows the differences in potential predictor variables in patients with different grades of pivot shift. Pivoting sports involvement at the time of injury (P1 [grade 3 vs grade 1] < .001; P2 [grade 3 vs grade 2] = .006), abnormal degree of lateral PITS (P1 = .002; P2 = .003), ALCL disruptions (P1 < .001; P2 = .011), and combined lateral meniscal lesions (P1 < .001; P2 = .008) revealed significantly higher prevalence in the study group compared with the 2 control groups (Figure 3).
Univariable Analyses of Variables Associated With Different Grades of Pivot Shift a
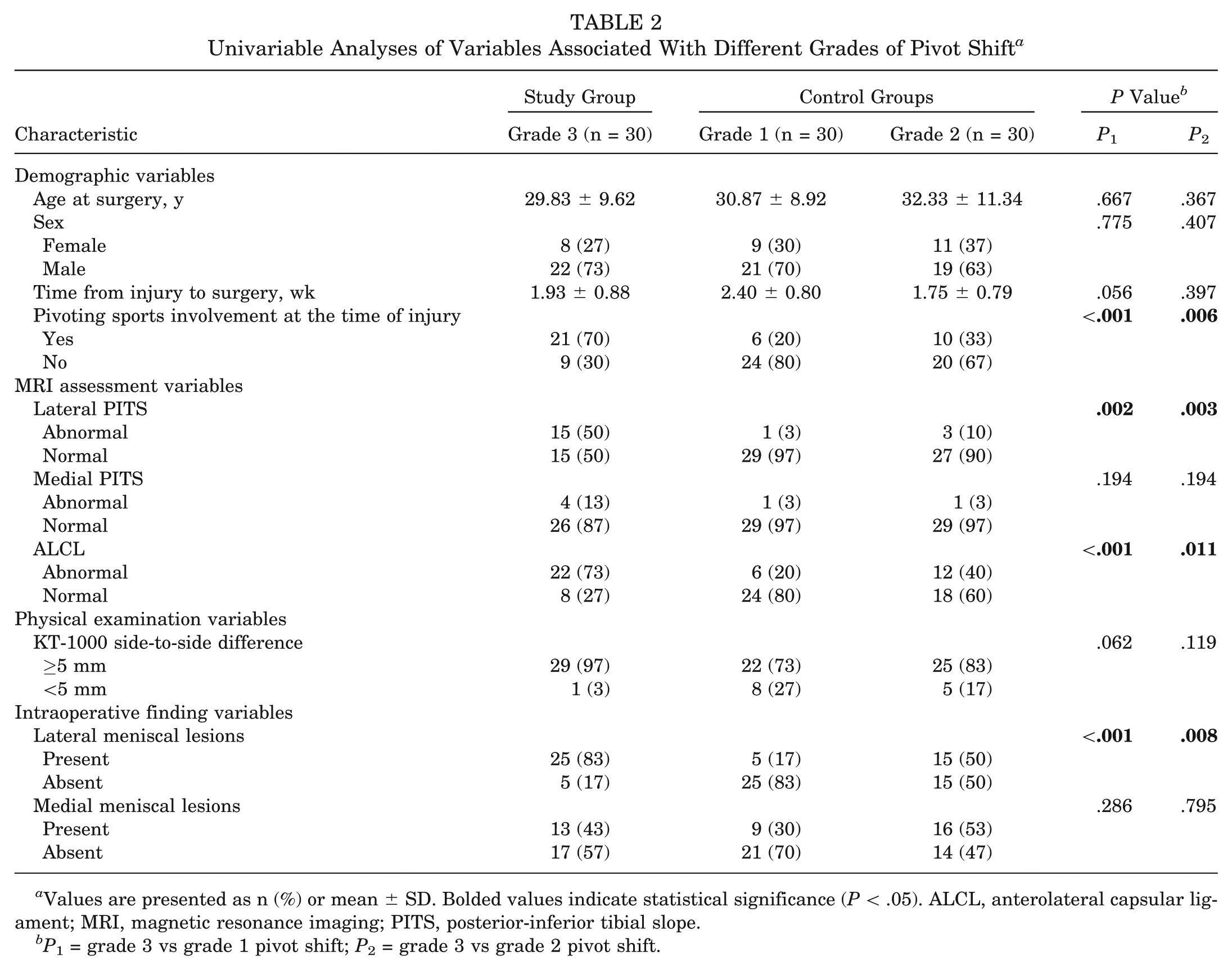
Values are presented as n (%) or mean ± SD. Bolded values indicate statistical significance (P < .05). ALCL, anterolateral capsular ligament; MRI, magnetic resonance imaging; PITS, posterior-inferior tibial slope.
P1 = grade 3 vs grade 1 pivot shift; P2 = grade 3 vs grade 2 pivot shift.
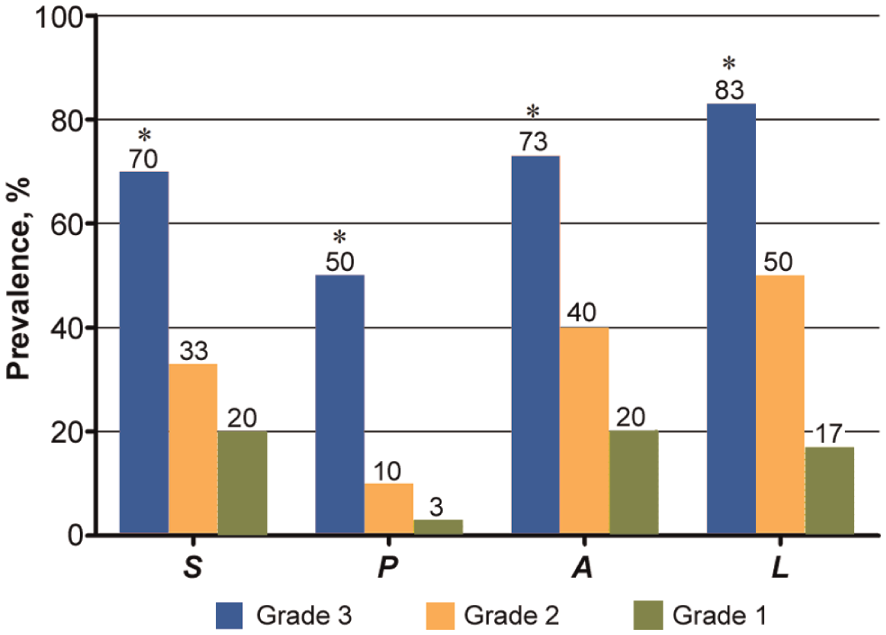
Prevalence of pivoting sports involvement at the time of injury (S), abnormal posterior-inferior tibial slope (P), anterolateral capsular ligament disruptions (A), and combined lateral meniscal lesions (L) in study group and 2 control groups. *Statistically significant difference between the study group and the 2 control groups (P1 [grade 3 vs grade 1] and P2 [grade 3 vs grade 2] < .05).
Results of the multivariable logistic regression analysis are shown in Table 3. The odds ratios (ORs) indicated that pivoting sports involvement at the time of injury (OR1 [grade 3 vs grade 1, grade 1 = reference], 11.88; 95% CI, 1.94-149.91; OR2 [grade 3 vs grade 2, grade 2 = reference], 3.41; 95% CI, 1.92-22.60), abnormal degree of lateral PITS (OR1, 14.41; 95% CI, 1.69-174.78; OR2, 6.41; 95% CI, 1.48-47.70), ALCL disruptions (OR1, 8.28; 95% CI, 1.71-117.14; OR2, 4.96, 95% CI, 1.07-28.75), and combined lateral meniscal lesions (OR1, 27.56; 95% CI, 5.48-240.52; OR2, 5.83; 95% CI, 1.21-38.56) were the independent risk factors associated with grade 3 pivot shift after acute ACL injuries.
Multivariable Logistic Regression of Potential Risk Factors for Grade 3 Pivot Shift a
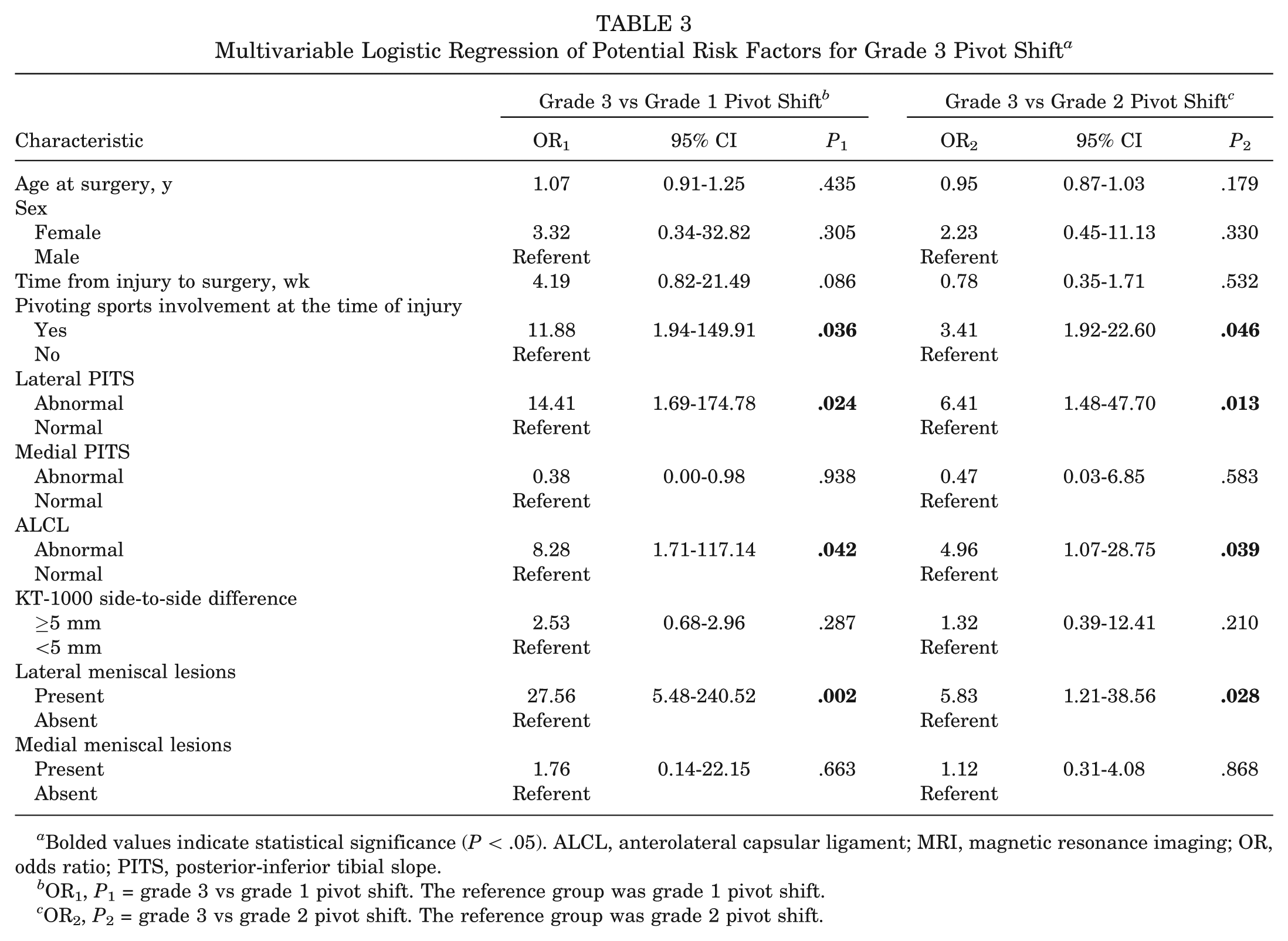
Bolded values indicate statistical significance (P < .05). ALCL, anterolateral capsular ligament; MRI, magnetic resonance imaging; OR, odds ratio; PITS, posterior-inferior tibial slope.
OR1, P1 = grade 3 vs grade 1 pivot shift. The reference group was grade 1 pivot shift.
OR2, P2 = grade 3 vs grade 2 pivot shift. The reference group was grade 2 pivot shift.
Significant differences were also identified in the prevalence of combined severe lateral meniscal lesions (complete posterior lateral root avulsions or bucket-handle tears) (Figure 4) between groups, with the study group (21 of 30, 70%) having a significantly higher prevalence than that of both control groups: grade 1 (1 of 30, 3%; P1 < .001) and grade 2 (6 of 30, 20%; P2 = .027).
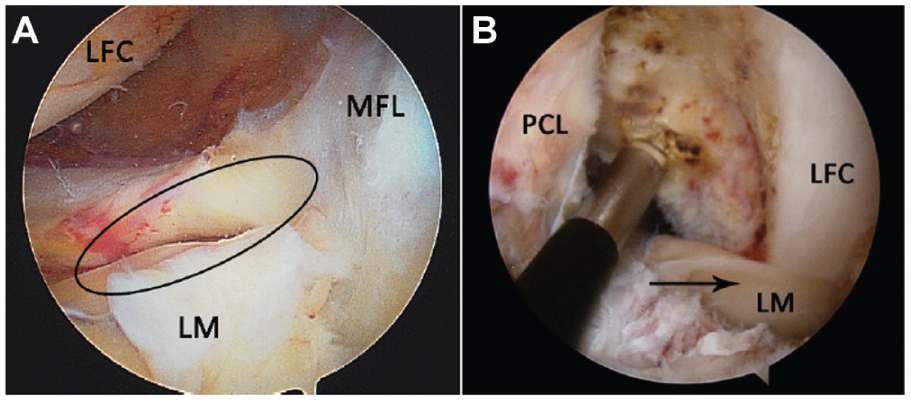
Representative arthroscopic images of the 2 combined lateral meniscal injury patterns in patients with grade 3 pivot-shift instability. (A) Complete radial tear of the posterior lateral meniscal root (ellipse) in a 29-year-old man who suffered from an anterior cruciate ligament (ACL) injury 10 days earlier while playing basketball. (B) Bucket-handle tear of the lateral meniscus in a 55-year-old man who injured his ACL while running 7 days earlier. The torn meniscal tissue was displaced into the intercondylar notch (arrow) during ACL reconstruction. LFC, lateral femoral condyle; LM, lateral meniscus; MFL, meniscofemoral ligament; PCL, posterior cruciate ligament.
Prevalence of high-risk individuals (combination of ≥2 risk factors) was 90% (27 of 30) for the study group compared with 16% (5 of 30; P1 < .001) for the grade 1 control group and 40% (12 of 30; P2 = .038) for the grade 2 control group, with results showing significant differences.
Discussion
We aimed to identify risk factors associated with grade 3 pivot shift after acute ACL injuries. Pivoting sports involvement at the time of injury, abnormal lateral PITS, ALCL disruptions, and combined lateral meniscal lesions were found to be the 4 independent risk factors that best predicted the presence of grade 3 pivot shift after acute ACL injuries.
It is believed that the risk factor analysis of grade 3 pivot shift may be suitable to focus on acute ACL-injured cases, since the chronicity of ACL deficiency can lead to increased prevalence of combined meniscal lesions. 14 Moreover, the variable degree of ALCL disruptions and edema shown on MRI are suitable to be detected in the acute setting. 5 In addition, cartilage degeneration or osteoarthritis, which are seen in chronic cases, have been reported to decrease the grade of the pivot-shift test. 34
The presence of these risk factors individually in the present study correlates with increased rotational instability in ACL-deficient knees. The prevalence of abnormal lateral PITS in our study group was significantly higher than in the 2 control groups. Similarly, Brandon et al 3 reported that for ACL injuries, patients with high-grade pivot shift had a significantly steeper mean PITS than those with low-grade pivot shift (11.1° vs 9.2°). An increased lateral PITS might lead to larger lateral tibial compartment translation in an ACL-deficient knee, which has correlated well with the clinical grade of the pivot-shift test.1,2,32
The lateral meniscus was reported to be an important secondary stabilizer to rotational loads in the ACL-deficient knee.8,10,24 In the present study, the presence of combined lateral meniscal lesions was identified as an independent risk factor. Furthermore, combined severe lateral meniscal lesions, including the complete posterior root avulsions or bucket-handle tears of the lateral meniscus, were shown to be associated with grade 3 pivot shift. Shybut et al 29 recently investigated the biomechanical role of posterior meniscal root lesions and concluded that a complete root detachment of the posterior lateral meniscus would further destabilize the ACL-deficient knee during a simulated pivot-shift maneuver. Additionally, for a bucket-handle tear of the lateral meniscus, we considered that the easily displaced torn meniscus might be stuck in the intercondylar notch during the reduction process of the lateral tibial plateau, leading to a “locked subluxation” pivot-shift mechanism.
The biomechanical role of the ALCL in restraining the internal tibial rotation during the pivot-shift maneuver has been demonstrated by several in vitro studies.4,6,7,21,22,26,27,37 Moreover, as the precise anatomy of the ALCL has recently been characterized, 7 the MRI features of ALCL have been extensively studied and identified.13,35 Claes et al 5 first performed a MRI study on 206 consecutive ACL-injured patients and reported that about 80% demonstrated ALCL abnormalities. They also pointed out that whether such a high incidence of radiologic ALCL lesions witnessed in ACL-injured subjects indeed related to pivot-shift instability still remains unknown. In the current study, the prevalence of radiologic ALCL disruptions of the patients in the study group was significantly higher than those in the 2 control groups, indicating that the additional ALCL disruption in ACL-injured subjects might lead to increased tibial rotational instability.
Although several studies evaluated for >1 risk factor and listed their individual prevalence, they did not report the presence of multiple risk factors combined in an individual with grade 3 pivot shift.3,30 In the current study, 90% (27 of 30) of the patients in the study group had ≥2 risk factors and were defined as high-risk individuals. The prevalence was significantly higher than that of both control groups: grade 1 (16%, 5 of 30) and grade 2 (40%, 12 of 30).
Knowledge of the risk factors associated with grade 3 pivot shift may provide additional information for counseling patients on residual laxity and risk for graft rerupture after ACL reconstruction. 25 An increased PITS was believed to adversely affect the postoperative stability of ACL-reconstructed knees. Webb et al 38 concluded that a PITS >12° was associated with increased odds of a further ACL injury after ACL reconstruction. Li et al 19 later claimed that a lateral PITS >3.8° would increase the risk of failure for ACL-reconstructed patients. They further reported that the OR of ACL reconstruction failure was 10.8 if the lateral PITS reached >5°. 20 Moreover, Robb et al 28 recently reported that lateral meniscal deficiency was found to be an important risk factor for residual laxity after ACL reconstruction. It seems that understanding these risk factors may influence the choice of surgical treatment in patients with grade 3 pivot-shift instability. However, future studies are still needed.
There were some limitations to this study. First, the subjective nature of the pivot-shift test should be regarded as the primary limitation. Although all the pivot-shift tests were performed with the patients under anesthesia by a single surgeon, the results might not be generalizable to the entire orthopaedic community. Second, the definition of acute ACL injury phase (<3 weeks) would have introduced some selection bias. However, the definitions of acute ACL injury phase were different among studies. Patients might sustain secondary meniscal lesions and therefore would not remember the real cause of initial ACL injuries as time passed, which would affect the accuracy of our risk factor analysis. Third, although patients in the 2 control groups were randomly chosen from the database, the study group was not, which might also have introduced some selection bias. Fourth, the decision on exploring the PITS as a potential risk factor of grade 3 pivot shift might not be optimal, as recent evidence suggested that this might not be as important as the soft tissue anatomy (meniscus slope) as we previously thought.15,33 However, measurements of the meniscus slope should be based on the integrity of the meniscus, which was unfeasible for most of the patients in our study. Finally, the method that we used to evaluate the status of ALCL on MRI might have introduced some observational bias. Although both intra- and interobserver reproducibility analyses showed good to excellent ICC values, as this is a new topic, confirmation of MRI findings was lacking. However, the method that we used was the most common one in our clinical practice, and it has also been reported as being reliable by previous studies.13,35 We therefore consider it appropriate for use in this study.
To our knowledge, this is the first study to report the prevalence of combined risk factors on high-risk individuals with grade 3 pivot shift after acute ACL injuries. We believe that the evaluation of a patient with grade 3 pivot shift should include identifying multiple risk factors predisposing to rotational instability, as 90% (27 of 30) of patients in our study group possessed ≥2 risk factors.
Conclusion
For acute ACL injuries, the best set of predictors of grade 3 pivot shift included pivoting sports involvement at the time of injury, abnormal lateral PITS, ALCL disruptions, and combined lateral meniscal lesions. These results may provide additional information for counseling patients on residual laxity and risks for graft rerupture after ACL reconstruction.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.