
Abstract
Background:
Shoulders with recurrent anterior instability often have combined bony defects of the humeral head and glenoid. Previous studies have looked at only isolated humeral head or glenoid defects.
Purpose/Hypothesis:
The aim of this study was to define the relationship of combined humeral head and glenoid defects on anterior shoulder instability. Combined bony defects will lead to increased instability compared with an isolated defect, and the “critical” size of humeral head and glenoid defects that need to be addressed to restore stability will be smaller when combined rather than isolated.
Study Design:
Controlled laboratory study.
Methods:
Eighteen shoulder specimens were tested at 60° of glenohumeral abduction and 80° of glenohumeral external rotation. Humeral head defect sizes included 6%, 19%, 31%, and 44% of the humeral head diameter. Glenoid defect sizes included 10%, 20%, and 30% of the glenoid width. Outcome measures included percentage of intact stability ratio (%ISR; the stability ratio for a given trial divided by the stability ratio in the intact state for that specimen) and percentage of intact translation (%IT; the distance to dislocation for a given trial divided by the distance to dislocation in the intact state for that specimen).
Results:
The decrease in %ISR reached statistical significance for humeral head defects of 44%, for glenoid defects of 30%, and for a combined 19% humeral head defect with a 20% glenoid defect (65% mean %ISR). The decrease in %IT reached statistical significance for humeral head defects ≥31%, for glenoid defects ≥20%, and for a combined 19% humeral head defect with a 10% glenoid defect (69% mean %IT).
Conclusion:
In shoulders with combined humeral head and glenoid defects, bony reconstruction may be indicated for humeral head defects as small as 19% of the humeral head diameter and glenoid defects as small as 10% to 20% of the glenoid width, especially if the glenoid defect produces a significant loss of glenoid concavity depth.
Clinical Relevance:
In shoulders with combined humeral head and glenoid defects, bony reconstruction may be indicated for defect sizes smaller than would be indicated for either defect found in isolation.
Keywords
Approximately 1.7% of the general population will experience a glenohumeral dislocation.3,7,13,16,20,29 More than 98% of all glenohumeral dislocations are anterior dislocations.5,19,23,27 Recurrent dislocation is a potential consequence of instability—a condition in which the humeral head can translate excessively on the glenoid fossa, resulting in subluxation or dislocation. It has been shown that 38% of all patients who experience a primary dislocation will suffer a recurrence. 21
Burkhart and De Beer 4 reported an overall recurrence rate of 10.8% after arthroscopic Bankart repair for traumatic anterior-inferior instability, with a 4% rate of recurrence in patients without significant bony defects and a 67% rate in patients with significant bony defects (defined as “engaging” Hill-Sachs lesions or “inverted pear” glenoid lesions). Boileau et al 2 reported a 15.3% recurrence rate after arthroscopic stabilization for recurrent anterior traumatic shoulder instability, with a strong association with a glenoid defect involving >25% of the glenoid surface (P = .01) or a large Hill-Sachs lesion (arbitrarily defined if a clinically “important” part of the humeral head surface was missing on assessment during the arthroscopic procedure; P = .05). These studies highlight the importance of recognizing “critical” humeral head and glenoid bone defects. Patients with defects above this critical size may benefit from bony procedures to restore the normal humeral head and/or glenoid anatomy, as opposed to arthroscopic Bankart repair.
Combined defects have been shown to be present in 54% of patients after traumatic anterior shoulder dislocation. 28 This suggests not only that most patients with anterior shoulder instability have a bony injury but that the majority of them have combined humeral head and glenoid defects.
In recent years, several cadaveric studies attempted to define the size of critical glenoid and humeral head defects. Itoi et al 8 showed that anteroinferior glenoid defects involving more than 25% of the glenoid width have decreased stability and range of motion. Yamamoto et al 30 performed a similar study with glenoid defects made in a more clinically accurate location and showed that the stability ratio decreased significantly with glenoid defects 6 mm or greater (20% of the glenoid length and 26% of glenoid width). Kaar et al 9 evaluated glenohumeral stability in the setting of Hill-Sachs defects and showed a decrease in stability with defects greater than 31% of the humeral head diameter. These studies provided valuable information; however, they focused on isolated glenoid or humeral head defects rather than on combined defects.
The purpose of the current study was to investigate the relationship of combined humeral head and glenoid defects of various sizes to glenohumeral stability, as well as to define the critical size of those combined defects that require bony reconstruction to restore stability. We hypothesized that combined bony defects will lead to increased instability compared with an isolated defect and that the critical size of humeral head and glenoid defects that need to be addressed to restore stability will be smaller when combined rather than isolated.
Methods
Specimen Preparation
Eighteen fresh-frozen cadaveric shoulder specimens with a mean age of 58 ± 7 years at the time of death (range, 43-69 years; 9 males and 9 females; 9 right and 9 left shoulders) were used from donors. Each specimen was visually inspected to eliminate those with physical abnormalities, glenohumeral arthritis, or prior shoulder surgery. Specimens were fresh-frozen and stored at −20°C until thawed overnight at room temperature before testing. Specimen preparation and testing methods were adapted from those used in prior cadaveric studies on shoulder instability by Itoi et al, 8 Yamamoto et al, 30 and Kaar et al. 9 The skin, subcutaneous tissue, and all soft tissues (including the labrum) were removed. The decision to remove all soft tissues and labrum was made out of concern that soft tissue integrity would degrade over the course of testing and potentially bias our results toward increased stability in trials performed first. The scapula was potted with Wood’s metal (42.5% bismuth alloy; McMaster-Carr) in an aluminum potting box with approximately 3 cm protruding. During the potting process, the scapula was aligned so that the inferior glenoid circle was parallel to the floor along both the x- and y-axes. After potting, alignment of the inferior glenoid circle was confirmed with the use of a digitizer (MicroScribe; Solution Technologies Inc). The scapula-potting box was then placed on top of a horizontal drive (Zaber Technologies Inc), and a 6 degrees of freedom load cell (Mini45; ATI Industrial Automation) was placed in between the drive and the potting box.
The humerus was cut transversely approximately 15 cm from the humeral head and potted with Wood’s metal in a cylindrical aluminum tube. The potted end of the humeral shaft was mounted to a vertical jig with 3 degrees of freedom (Figure 1). This jig allowed for free movement along the medial-lateral (vertical) direction via near-frictionless bearings and allowed various combinations of external rotation and abduction angles to be applied. A laser displacement sensor (Renishaw Inc), with an accuracy of 0.4 μm, was attached to the vertical reaction frame to measure the medial-lateral displacement of the humeral head. To re-create neutral rotation of the arm, the humerus was placed in 0° of abduction and positioned with the articular surface of the humeral head centered within the glenoid fossa; the humerus was then internally rotated 20°, and this was defined as 0° of external rotation.
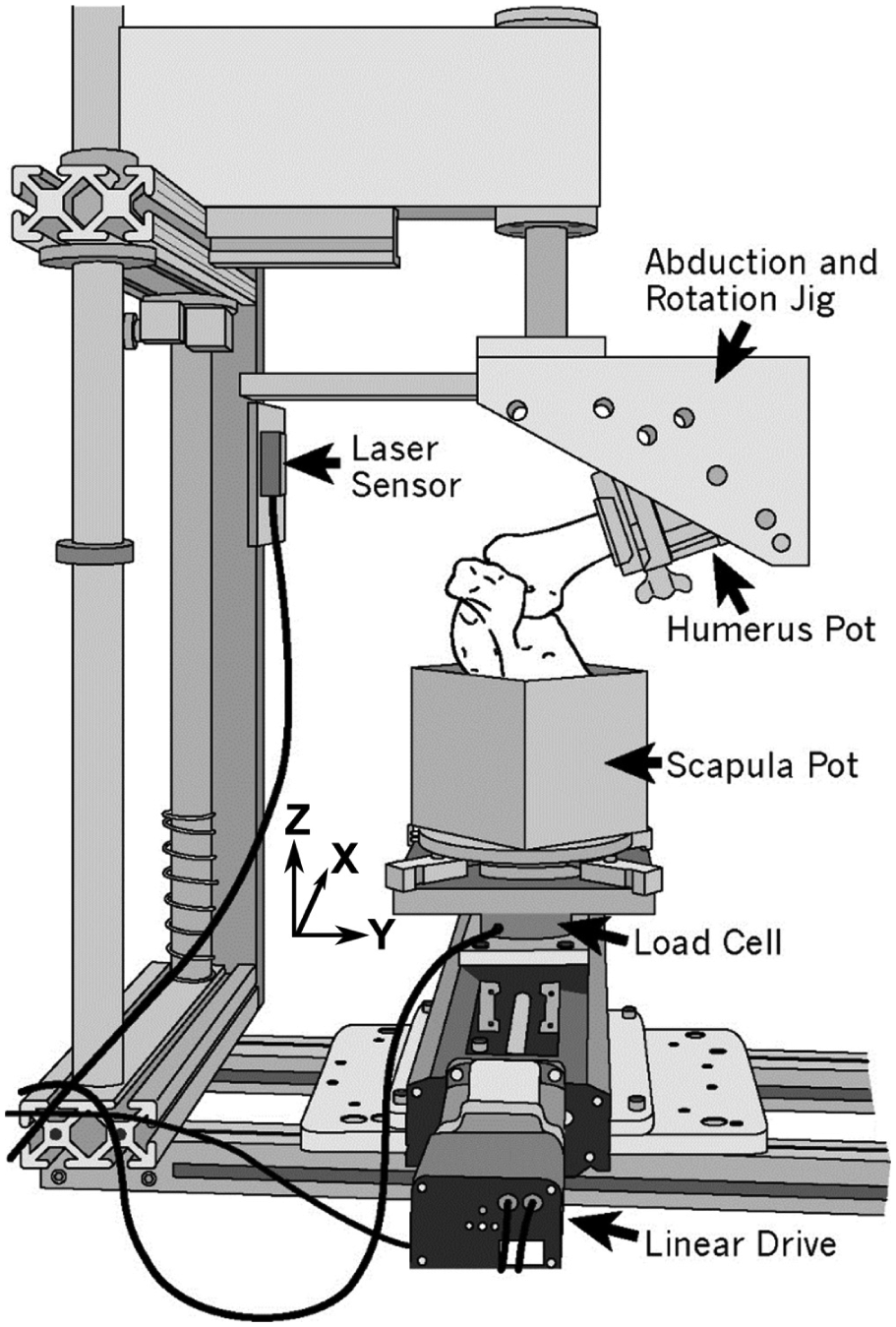
Testing apparatus.
The coordinate system for the present study was based on the orientation of the glenoid, as has previously shown to be effective in biomechanical testing of anterior shoulder stability by Yamamoto et al 30 (Figure 2). The y-axis was defined as parallel to the long axis of the glenoid face (the superior-inferior direction), the x-axis was perpendicular to the long axis of the glenoid face (the anterior-posterior direction), and the z-axis was orthogonal to the x- and y-axes (the medial-lateral direction). All axes passed through the center point of the glenoid clock face. The glenoid was orientated within the testing apparatus so that the x-axis of the glenoid was aligned parallel to the horizontal drive. Rotation around the x-axis of the glenoid was defined as abduction, while the rotation around the y-axis was defined as external rotation. During testing, the only movement allowed by the glenoid was along the x-axis as the horizontal drive moved the potting box.
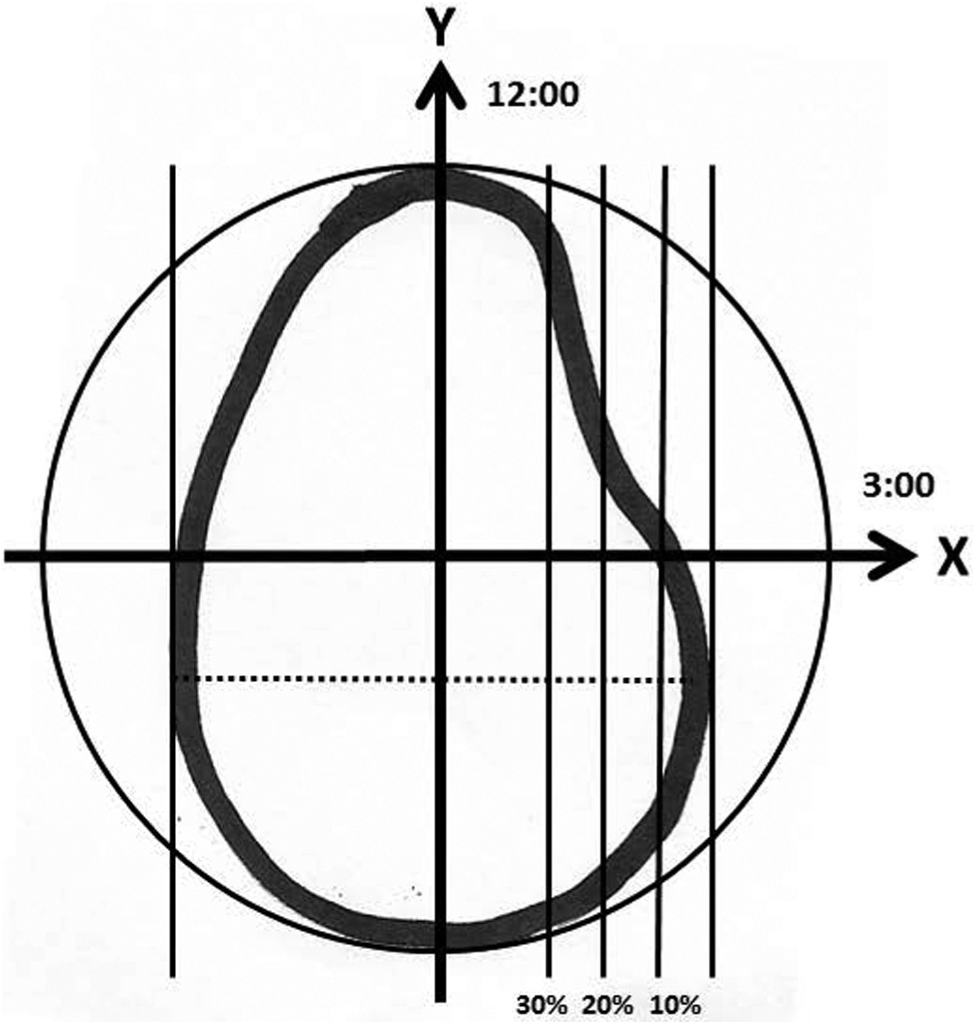
Glenoid coordinate system and location of glenoid osteotomy cuts.
To re-create the classic position of instability, testing was performed with the humerus in 60° of glenohumeral abduction and 80° of glenohumeral external rotation (equivalent to 90° of abduction and 90° of external rotation relative to the trunk).6,11 To ensure reproducibility of arm position, the testing apparatus had hash marks at each degree from −90° to 90° of rotation, and it was designed to be locked at 80° of glenohumeral abduction.
Creation of Defects
Glenoid osteotomy cuts were made in the anterior portion of the glenoid according to the methods described by Yamamoto et al. 30 A customized cutting guide was aligned parallel to the y-axis to allow for osteotomy cuts perpendicular to the x-axis. An oscillating saw was used to progressively remove 10%, 20%, and 30% of the glenoid width (Figure 2). The 0% osteotomy line was defined as a line parallel to the y-axis and tangential to the anterior rim of the glenoid (Figure 2).
Humeral head osteotomy cuts were made in the posterior superolateral portion of the humeral head according to the methods described by Kaar et al. 9 To match the location where Hill-Sachs lesions occur, defects were centered at 209° from the anterior border of the humeral head articular cartilage with the humeral head modeled as a circle viewed superiorly, as documented by Richards et al. 18 While viewing the humeral head from above, a goniometer was used to locate this point. A customized cutting guide was then centered at this point, aligned perpendicular to the articular surface and parallel to the humeral neck. The guide was placed on the humerus before each osteotomy cut. An oscillating saw was used to progressively remove 6%, 19%, 31%, and 44% (1/16, 3/16, 5/16, and 7/16) of the humeral head diameter (Figure 3).
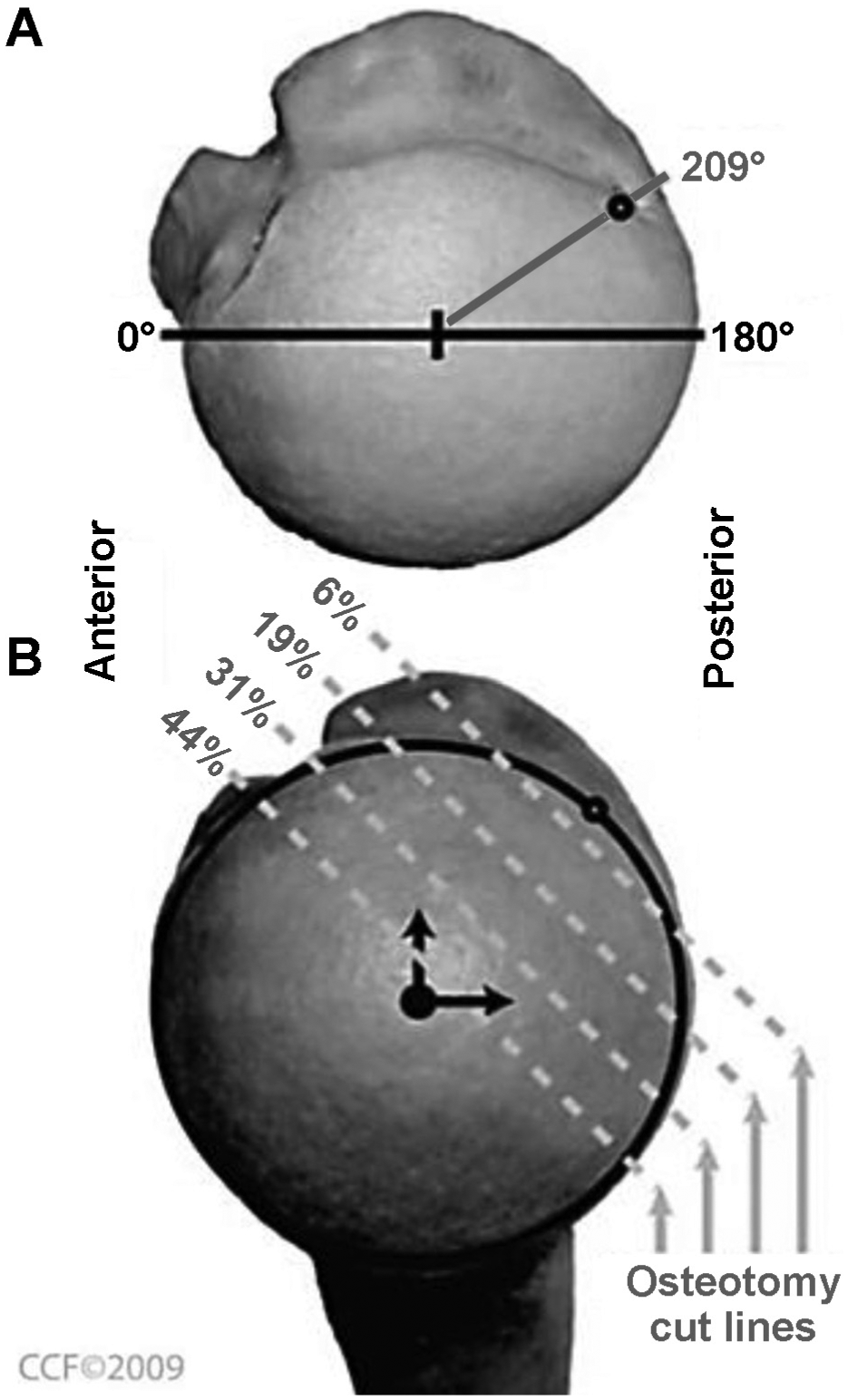
(A) Superior view of a humeral head with the point 209° from the anterior margin of the articular surface marked for the center of the osteotomy. (B) View looking directly at the articular surface demonstrating the progressive series of osteotomy cuts used to mimic Hill-Sachs defects. Osteotomy cuts were made at 6%, 19%, 31%, and 44% of the projected diameter of the humeral head. Image modified from Kaar et al 9 and reprinted with permission.
Biomechanical Testing
Biomechanical testing involved 2 factors: humeral head defect size (5 levels) and glenoid defect size (4 levels). Since it is not possible to test all defect combinations in a single specimen, the experiment was designed with 3 different pathways (3 different sequences in which humeral head and glenoid osteotomy cuts were made and tested). Pathways were designed to maximize the number of trials with intermediate-size humeral head and glenoid defect combinations (Figure 4). Each pathway began by finding a reference position for the specimen; this was followed by testing to dislocation in the intact state (no humeral head or glenoid defect), and then osteotomy cuts were made according to the assigned pathway, with testing performed after each osteotomy cut. Before testing, each cadaveric specimen was randomly assigned to 1 of the 3 pathways using block randomization to allow for 6 shoulders in each pathway.
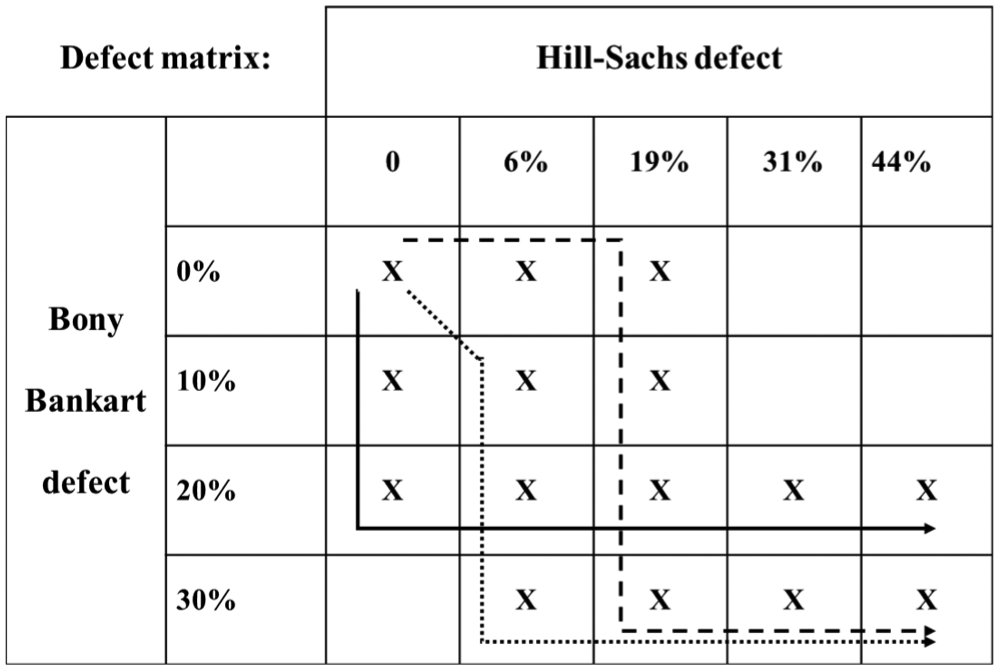
Defect creation pathways for different defect combination matrices. Pathway 1 is represented by the solid black line, pathway 2 by the hash mark line, and pathway 3 by the dotted line.
The reference position (home) was found for each shoulder by translating the humeral head 7 mm along both the x-axis (superior-inferior) and y-axis (anterior-posterior). The reference position was defined as the position where the humeral head was most medial within the glenoid. Testing was performed by placing the humeral head at the home position and then translating the glenoid posteriorly at a constant velocity of 0.5 mm/s (to minimize viscoelastic effects) 15 to cause an anterior dislocation. During testing, the glenoid was translated until the humerus reached the lateral border of the glenoid and began to visibly fall off the glenoid (typically 2-3 mm past the point of dislocation). A constant medially directed load of 50 N was applied throughout all testing to center the humeral head in the glenoid fossa and to simulate the static soft tissue load. A 50-N compressive force has been used in previous studies as a reasonable estimate of glenohumeral contact force at the time of dislocation,8,9,12,14,17,30 and it does not cause gross damage to the tissue during dislocation. 14 The real-time readings of the forces and displacements were recorded via a computer using a USB data acquisition card (National Instruments Corp) and custom-developed LabVIEW code (National Instruments Corp). All data were sampled at a frequency of 50 Hz. The specimen was sprayed with normal saline every 10 to 15 minutes to keep the tissue moist throughout testing.
Data Analysis
For each specimen, the humeral head diameter, circumference of the articular surface of the humeral head in the plane perpendicular to the osteotomy cuts, and glenoid width were measured with a ruler. Glenoid concavity depth was also recorded by measuring the maximum lateral translation of the humerus in moving from the home position to the brim of the glenoid lip just before dislocation (with a compressive 50-N load). These measurements were recorded in the intact state and after each osteotomy cut.
During each trial, translational force and distance to dislocation were recorded and then determined during postprocessing of data using Matlab (version 10.1a; MathWorks). The point of dislocation was computed as the point where horizontal reaction force in the anterior direction (x-axis) became zero. This approach was similar to that described by Walia et al. 26 Distance to dislocation was defined for each trial as the distance between the reference position (home position) and the point where dislocation occurred along the x-axis. Stability ratio for each trial was defined as peak translational force divided by the applied compressive force of 50 N. 26 Primary outcome measures included percentage of intact stability ratio (%ISR) and percentage of intact translation (%IT). The %ISR was defined as the stability ratio for a given trial divided by the stability ratio in the intact state for that specimen. The %IT was defined as the distance to dislocation for a given trial divided by the distance to dislocation in the intact state for that specimen. The %ISR and %IT were chosen as the primary outcome measures instead of stability ratio and distance to dislocation to account for potential differences in shoulder size from specimen to specimen.
A balanced repeated-measures analysis of variance (ANOVA) was used to identify the significance of each factor (humeral head defect size and glenoid defect size) on the %ISR and %IT. Two-way ANOVA was performed in the R3.1 statistical package (R Core Team, 2014; R Foundation for Statistical Computing). Tukey post hoc analyses were used to determine significance of differences between factor levels. Statistical significance was set at α = .05.
Results
Data are reported as mean ± standard deviation (range). The humeral head diameter for all specimens was 43 ± 4 mm (36-50 mm), the diameter for pathway 1 was 41 ± 3 mm (38-46 mm), the diameter for pathway 2 was 43 ± 5 mm (36-49 mm), and the diameter for pathway 3 was 44 ± 5 mm (40-50 mm).
The mean circumference of the articular surface of the humeral head was 64 ± 7 mm (54-74 mm) in the intact state, 53 ± 6 mm (45-64 mm) after a 6% osteotomy cut (17% mean loss of articular circumference), 45 ± 4 mm (38-52 mm) after a 19% osteotomy cut (29% mean loss of articular circumference), 39 ± 4 mm (34-46 mm) after a 31% osteotomy cut (39% mean loss of articular circumference), and 33 ± 4 mm (29-41 mm) after a 44% osteotomy cut (47% mean loss of articular circumference).
The mean glenoid width for all specimens was 23 ± 2 mm (17.5-25.5 mm), the width for pathway 1 was 22 ± 3 mm (17.5-25.5 mm), the width for pathway 2 was 23 ± 2 mm (19-25.5 mm), and the width for pathway 3 was 23 ± 2 mm (20.5-25.5 mm).
The mean glenoid concavity depth for all specimens was 1.43 ± 0.73 mm (0.36-3.03 mm), the glenoid concavity depth for pathway 1 was 1.20 ± 0.65 mm (0.42-2.07 mm), the glenoid concavity depth for pathway 2 was 1.86 ± 0.75 mm (0.98-3.03 mm), and the glenoid concavity depth for pathway 3 was 1.24 ± 0.74 mm (0.36-2.19 mm). The differences in mean humeral head diameter, glenoid width, and glenoid concavity depth for the 3 pathways were not statistically significant.
The overall stability ratio for the intact state was 0.24 ± 0.08, for pathway 1 it was 0.22 ± 0.05, for pathway 2 it was 0.28 ± 0.09, and for pathway 3 it was 0.21 ± 0.10. To account for the difference in baseline stability ratio between pathways, analysis was performed using %ISR rather than stability ratio. There was a progressive decrease in %ISR as humeral head defect size increased and as glenoid defect size increased (Figure 5). The decrease in %ISR reached statistical significance for humeral head defects of 44%, for glenoid defects of 30%, and for the combination of a 19% humeral head defect with a 20% glenoid defect. Complete results are summarized in Table 1. The missing values in Table 1 and Figures 5 and 6 are the defect combinations not tested in this study.
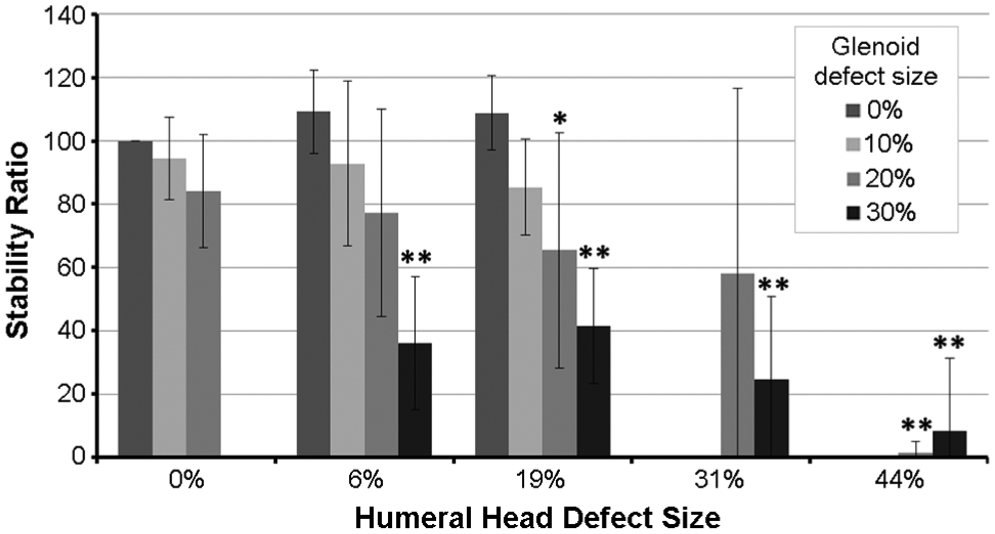
Percentage of intact stability ratio (the stability ratio for a given trial divided by the stability ratio in the intact state for that specimen). *P < .05. **P < .001.
Mean Percentage of Intact Stability Ratio and Mean Percentage of Intact Translation for All Specimens (N = 18)
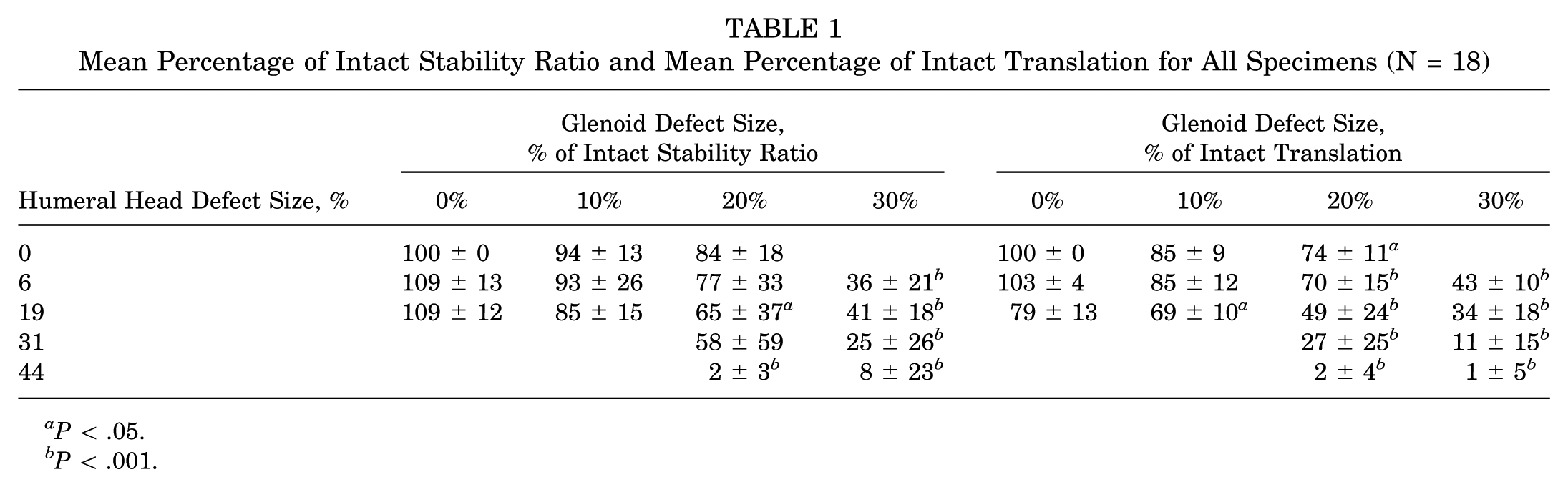
P < .05.
P < .001.
A similar pattern was seen with distance to dislocation. There was a progressive decrease in %IT as humeral head defect size increased and as glenoid defect size increased (Figure 6). The decrease in %IT reached statistical significance for humeral head defects of 31% and 44%, for glenoid defects of 20% and 30%, and for the combination of a 19% humeral head defect with a 10% glenoid defect. Complete results are summarized in Table 1.
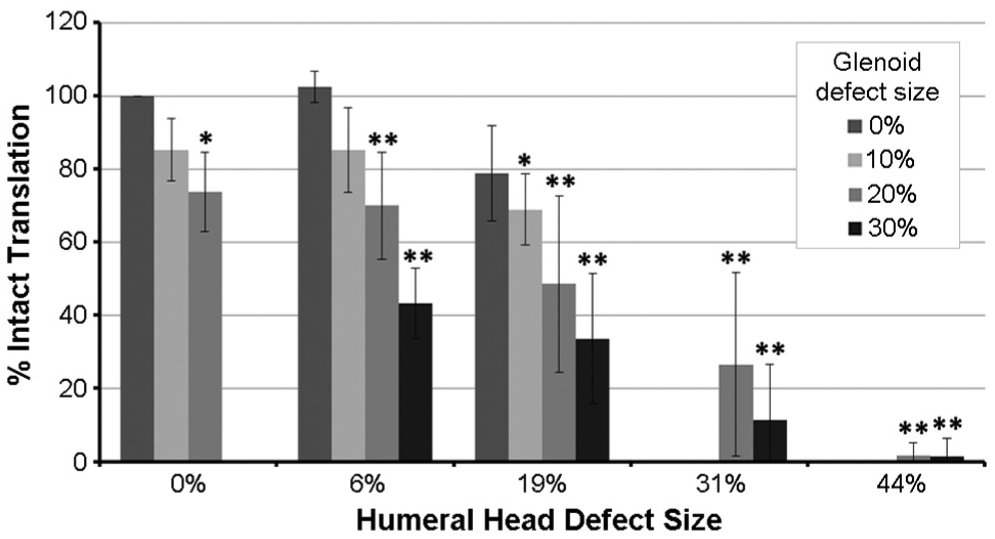
Percentage of intact translation (the distance to dislocation for a given trial divided by the distance to dislocation in the intact state for that specimen). *P < .05; **P < .001.
Discussion
The results of this study show a progressive decrease in stability as humeral head defect size increases and as glenoid defect size increases. This decrease in stability is greater for combined humeral head and glenoid defects than for respective corresponding isolated defects. Prior cadaveric studies on isolated humeral head and glenoid defects have shown a decrease in stability with humeral head defects greater than 31% of the humeral head diameter 9 and glenoid defects greater than 26% of the glenoid width. 30 Our results are consistent with these studies, showing a statistically significant decrease in stability with defects 31% to 44% of the humeral head diameter and 20% to 30% of the glenoid width. In addition, our results show a significant decrease in stability for intermediate-size humeral head and glenoid defects that occur in combination. A combined 19% humeral head defect with a 10% glenoid defect had a 15% decrease in %ISR (nearly equivalent to the 16% decrease in %ISR seen with an isolated 20% glenoid defect) and a 31% decrease in %IT (which was greater than the 26% decrease in %IT seen with an isolated 20% glenoid defect). A combined 19% humeral head defect with a 20% glenoid defect had a 35% decrease in %ISR and a 51% decrease in %IT. These results are similar to findings of a recent study that showed a decrease in stability with combined defects involving 15% of the glenoid diameter and small (0.87 cm3) or medium (1.47 cm3) humeral head defects. 1 They are also consistent with findings of a computational study that showed a magnified effect of combined defects on stability. 25
In addition to showing a loss of stability with moderate-sized defect combinations, our results show almost complete loss of stability with large defect combinations. A 44% humeral head defect with a 20% glenoid defect had a 98% decrease in %ISR and a 98% decrease in %IT, and a 44% humeral head defect with a 30% glenoid defect had a 92% decrease in %ISR and a 99% decrease in %IT. In contrast, Yamamoto et al 30 showed a decrease in stability ratio of approximately 50% with isolated defects of 26% and 35% of the glenoid width, and Kaar et al 9 showed a decrease in %IT of approximately 80% for an isolated 44% defect of the humeral head.
There was a notable difference in the mean stability ratio in the intact state between the 3 pathways. This difference was not explained by a difference in glenoid width or humeral head diameter, as the mean values for these properties were nearly identical for all pathways. There was, however, a large difference in mean glenoid concavity depth between the 3 pathways, and this appeared to correlate with the difference in mean stability ratio. This difference likely explains why our standard deviations for %ISR, which is dependent on glenoid concavity depth, were higher than were our standard deviations for %IT, which is dependent only on glenoid width. When examining the glenoid concavity depth and stability ratio in the intact state for all specimens, there appeared to be a linear relationship; moreover, linear regression provided the following formula: stability ratio = 10.7 + 8.9 × glenoid concavity depth (R2 = 0.74). This relationship is nearly identical to the relationship reported previously by Lippitt et al 14 : stability ratio = 9.7 + 10.3 × glenoid concavity depth.
Glenoid concavity depth in the intact state ranged from 0.3 to 2.5 mm. In the 6 specimens that underwent glenoid osteotomies before any humeral head osteotomy, the loss in glenoid concavity depth ranged from 3% to 42% with a 10% loss of glenoid width and from 17% to 76% with a 20% loss of glenoid width. These measurements suggest that there is significant variability in the shape and curvature of the anterior glenoid rim from shoulder to shoulder. Because of this variability, it is possible that some shoulders may become unstable with small to intermediate-sized glenoid defects if there is a significant decrease in glenoid concavity depth, while other shoulders may be stable with the same size defect if there is only a small decrease in glenoid concavity depth.
Despite a significant number of publications describing the correlation between large bone defects of the humeral head or glenoid and recurrent instability after arthroscopic shoulder stabilization, there remains a high rate of failure after this procedure. Boileau et al 2 showed a 15.3% rate of recurrence after arthroscopic stabilization for recurrent anterior traumatic shoulder instability. They showed that glenoid bone loss involving >25% of the glenoid surface and large Hill-Sachs lesions were associated with recurrent instability. However, they did not discuss how many of the shoulders with recurrent instability had combined defects or if smaller humeral head and glenoid defects— when found together—were associated with recurrence. Voos et al 24 showed an 18% rate of recurrence after arthroscopic shoulder stabilization for anterior shoulder instability despite excluding patients with bony lesions requiring fixation and having no patients with an inverted pear defect included in the study. They showed an association between Hill-Sachs lesions >250 mm3 and recurrent instability. They did not discuss how many of the shoulders with recurrent instability had combined defects or if smaller humeral head and glenoid defects—when found together—were associated with recurrence. The results of the current study could potentially help explain the high recurrence rates in these studies if the surgeons appreciated isolated large humeral head or large glenoid defects but did not appreciate intermediate-sized combined defects or shoulders with smaller glenoid defects that had a significant loss of glenoid concavity depth. Magnetic resonance imaging or computed tomography arthrogram may be a useful preoperative tool for evaluating glenoid bone loss—specifically, loss of glenoid concavity depth—as prior studies have shown that the glenoid articular surface has a significantly smaller radius of curvature than does the glenoid subchondral bone.10,22,31 In addition, humeral head defects on all of our specimens were made in the same location and orientation and thus had a similar loss of or articular surface from specimen to specimen. In the clinical setting, defects of the same size can have varying orientations and locations. Because dislocation occurs when the humeral head and glenoid defects engage, a moderate-sized humeral head defect may have a different effect on stability depending on its location and orientation.
There were several limitations to this study. Due to the number of trials performed on each specimen, there was concern that capsuloligamentous stretch, as well as the need to take down and repair the capsule for each osteotomy cut, could potentially lead to a significant decrease in soft tissue tensile strength over the course of the trials; therefore, we elected to remove all soft tissues before testing. Because of this, we cannot address to what degree the soft tissue envelope, the capsuloligamentous structures as well as rotator cuff muscles, would have provided additional static and dynamic stability. Although we would have liked to perform testing with the labrum and soft tissues intact, we thought it was more important to minimize any potential biases. Bony defects were simulated by making straight osteotomy cuts with the same orientation for all specimens. Although this allowed for easy reproducibility, it is unlikely to be representative of all humeral head and glenoid defects encountered in a clinical practice. However, we thought it was more important to ensure reproducibility and minimize potential biases than to create more clinically representative defects. There was a large, although not statistically significant, difference in baseline stability ratio and glenoid concavity depth for the 3 pathways. We controlled for this variability by using %ISR and %IT in our analysis rather than absolute stability ratio and distance to dislocation.
In summary, this study demonstrated that combined humeral head and glenoid defects produce greater instability than does either defect found alone. Bony reconstruction may be indicated for humeral head defects as small as 19% of the humeral head diameter and glenoid defects as small as 10% to 20% of the glenoid width, especially if the glenoid defect produces a significant loss of glenoid concavity depth.
Footnotes
Presented as a poster at the 41st annual meeting of the AOSSM, Orlando, Florida, July 2015.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by NFL Charities Medical Research Grant, Dissertation Research Award, from Cleveland State University and a grant from the Research Program Committee of the Cleveland Clinic. A.M. and M.H.J. have received unrestricted research grants from Arthrex, Donjoy, BREG, and Stryker. A.M. has received royalties from Zimmer and Tenet, has received nonincome support from Arthrosurface, and is a consultant for Arthrosurface and Stryker. M.H.J. is a consultant for Allergan. S.D.F. is a shareholder of Apto Orthopaedics.