
Abstract
Background:
Osteochondral defects (OCDs) of the talus usually affect athletic patients. The primary surgical treatment consists of arthroscopic debridement and microfracture. Various possibilities have been suggested to improve the recovery process after debridement and microfracture. A potential solution to obtain this goal is the application of pulsed electromagnetic fields (PEMFs), which stimulate the repair process of bone and cartilage.
Hypothesis:
The use of PEMFs after arthroscopic debridement and microfracture of an OCD of the talus leads to earlier resumption of sports and an increased number of patients that resume sports.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A total of 68 patients were randomized to receive either PEMFs (n = 36) or placebo (n = 32) after arthroscopic treatment of an OCD of the talus. The primary outcomes (ie, the number of patients who resumed sports and time to resumption of sports) were analyzed with Kaplan-Meier curves as well as Mann-Whitney U, chi-square, and log-rank tests. Secondary functional outcomes were assessed with questionnaires (American Orthopaedic Foot and Ankle Society ankle-hindfoot score, Foot and Ankle Outcome Score, EuroQol, and numeric rating scales for pain and satisfaction) at multiple time points up to 1-year follow-up. To assess bone repair, computed tomography scans were obtained at 2 weeks and 1 year postoperatively.
Results:
Almost all outcome measures improved significantly in both groups. The percentage of sport resumption (PEMF, 79%; placebo, 80%; P = .95) and median time to sport resumption (PEMF, 17 weeks; placebo, 16 weeks; P = .69) did not differ significantly between the treatment groups. Likewise, there were no significant between-group differences with regard to the secondary functional outcomes and the computed tomography results.
Conclusion:
PEMF does not lead to a higher percentage of patients who resume sports or to earlier resumption of sports after arthroscopic debridement and microfracture of talar OCDs. Furthermore, no differences were found in bone repair between groups.
Registration:
Netherlands Trial Register NTR1636.
Keywords
An osteochondral defect (OCD) of the talus often has a severe effect on the quality of life of young and athletic patients. 52 Currently, arthroscopic debridement and bone marrow stimulation are considered the primary treatment in osteochondral talar defects up to 1.5 cm in diameter.9,32 This treatment has an 85% overall success rate and a 76% satisfactory outcome at the long term.41,51 However, it can take up to 1 year to obtain improvement of clinical symptoms. Moreover, it is a great challenge to achieve early resumption of sports, which is the main goal of many of these young patients. Saxena and Eakin 35 reported a mean sport resumption of 15 weeks after debridement and microfracture of talar OCDs in “high-demand” athletic patients. Shortening this period would considerably improve the quality of life in these active patients. Various possibilities have been suggested to improve the recovery process after debridement and microfracture.24,29,46,50 A potential solution to obtain this goal is the application of pulsed electromagnetic fields (PEMFs). In vitro and in vivo studies have shown that PEMFs act as adenosine A2a agonists, leading to an increase of transforming growth factor β-1, thereby improving bone development, reducing cartilage damage, and increasing chondrocyte proliferation.1,7,10,30,34,49 This biophysical stimulation promotes tissue healing, suppresses inflammation, and relieves pain.8,26 Clinically, PEMF treatment improves the outcome of patients after arthroscopic treatment of chondral lesions in the ankle and knee.8,54 On the basis of these data, it can be postulated that PEMFs may act on OCDs by improving bone regeneration and suppressing inflammation evoked by surgery. To our knowledge, return to sports after OCD treatment with the use of PEMFs has not been investigated. We hypothesized that the use of PEMFs after arthroscopic debridement and microfracture of an OCD of the talus leads to earlier resumption of sports and an increased number of patients who resume sports.
Methods
A randomized, double-blind, placebo-controlled trial was conducted in 4 centers in the Netherlands and Belgium from 2009 to 2014. The trial was registered in the Netherlands Trial Register (NTR1636). Details of the study protocol were published earlier. 40 Approval was obtained from the local medical ethics committees of each participating center. Written informed consent for participation was obtained from every patient. A clinical research associate from the primary center’s Clinical Research Unit monitored the trial. Internet-based remote data capture (Oracle Clinical) was used for entering, managing, and validating data from the investigative sites.
The study included patients with a symptomatic OCD of the talus, with a diameter <15 mm (in 3 dimensions) as measured on computed tomography (CT) scans, who were scheduled for arthroscopic debridement and microfracture of the defect. Different studies have reported good clinical outcomes after arthroscopic debridement and bone marrow stimulation in osteochondral talar defects up to 1.5 cm in diameter.9,32,41,51 Furthermore, patients had to have an Ankle Activity Score (AAS) of at least 4 before symptoms. 17 Exclusion criteria were age <18 years, ankle osteoarthritis grade II or III, 45 concomitant OCD of the tibia, ankle fracture <6 months before treatment of the OCD, surgical treatment of the index ankle performed <1 year before treatment of the OCD, concomitant painful or disabling disease of the lower limb, rheumatoid arthritis, pregnancy, and implanted pacemaker.
Electromagnetic stimulation was started within 3 days after surgery with a PEMF stimulator (I-ONE; IGEAmedical), which consisted of a portable generator that was connected to a coil attached to the ankle (Figure 1). It was applied 4 hours daily for a period of 60 days.5,11 The coil of the PEMF stimulator generated a peak magnetic field intensity of 1.5 mT, supplied by an electric pulse frequency of 75 Hz.11,48 The placebo device produced a negligible peak <0.05 mT, supplied by the minimal current necessary to power the device indicators. The placebo device did not differ from the PEMF active device in shape, color, weight, and acoustic or visual signaling. Patients and investigators were blinded to the allocation of treatment. A clock inside the device recorded the hours of stimulation to monitor the patient’s compliance in both groups.

The application of pulsed electromagnetic fields on the ankle, generated in the green coil and attached with the elastic band (I-ONE; IGEAmedical).
The participants were randomized to receive either an active or placebo device, stratified for participating center, body mass index (≤25 kg/m2 vs >25 kg/m2),4,9 and diameter of the defect (≤10 mm vs >10 mm). 52 Randomization was performed in randomly allocated blocks of 2 or 4 patients via a validated web-based computer program (ALEA; NKI-AVL). 3 Treatment allocation was managed by an independent, unblinded research assistant (I.N.S.) who was not involved in patient care or assessment. Any (serious) adverse event during the trial period was recorded and reported to the central medical ethics committee.
Operative Technique
All surgical procedures were performed with a standardized anterior ankle arthroscopy technique. 44 The OCD was identified with a probe and debrided with a curette and bonecutter shaver. All unstable bone and cartilage were removed. Any cyst underlying the defect was opened, followed by curettage. After full debridement, the subchondral bone was perforated with a microfracture awl, with intervals of approximately 3 mm. At the end of the procedure, a pressure bandage was applied.
Postoperative management consisted of a protocol-based rehabilitation program, guided by a physiotherapist. Partial (eggshell) weightbearing on crutches was allowed as tolerated and progressed to full weightbearing over a period of 6 weeks. During this 6-week period, active nonweightbearing and partial weightbearing sagittal range of motion exercises were encouraged. After this period, resumption of sports was permitted as tolerated. 46
Outcome Assessment
The primary outcome measures were the number of patients that resumed sports and the time to resumption of sports. Resumption of sports was defined as initiation of any sport with a minimum level of the presymptoms level minus 1 point on the AAS, maintained for at least 30 days. The AAS is a 10-point score based on the type and level of sport or work, with 0 points indicating the lowest activity and 10 points indicating the highest activity. 17 A diary was used to monitor resumption and maintenance of sports and activity levels.
The secondary clinical outcome measures included time to resumption of work, the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot score,21,22 Foot and Ankle Outcome Score (FAOS),33,37 EuroQol (EQ-5D),23,39 and numeric rating scales (NRSs) for pain (at rest and when running) and satisfaction. Resumption of work was defined as the ability to perform normal work activities without any deficits in work quality. 38 The AOFAS is a 100-point score, with a subjective and an objective component, which devotes 40 points to pain, 50 to function, and 10 to alignment. 22 The FAOS is a validated subjective questionnaire consisting of 5 subscales: pain, other symptoms, activities of daily living (function), sports, and quality of life.33,37 Each subscale’s highest possible score is 100. The EQ-5D is a validated and extensively used general health questionnaire to measure quality of life.13,23,39 It comprises 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Patients’ level of quality of life was assessed with the vertical visual analog scale of the EQ-5D, where the endpoints are labeled “best imaginable health state (1.00)” and “worst imaginable health state (−0.33).” The NRS is an 11-point scale, representing the spectrum of no pain (0 points) to the worst pain imaginable (10 points) and not satisfied (0 points) to maximal satisfaction (10 points). 15
Patients were evaluated at the outpatient clinic preoperatively and at 2 weeks, 2 months, and 12 months postoperatively. Additionally, they completed questionnaires containing NRSs for pain and satisfaction, EQ-5D,23,39 and resumption of sport and work at 1 month and 6 months postoperatively.
Radiology
CT scans were obtained preoperatively to measure the 3-dimensional size and to grade the defect according to the modified Berndt and Harty classification.6,36 To objectively assess bone repair, CT scans were also obtained 2 weeks postoperatively (only at the main research center) and 1 year after surgery. CT scanning has been proven to be accurate in the detection and follow-up of OCDs of the talus, regarding location and extent as well as healing of the defect.28,47,53 The level of the subchondral plates (ie, flush, depressed, or proud) was analyzed on the 1-year postoperative CT scans. The bone volume filling of the OCDs at final follow-up was analyzed in comparison with the 2-week postoperative CT scans and graded as good (67%-100%), moderate (34%-66%), or poor (0%-33%).16,25 To assess the intraobserver reliability, measurements were performed twice by a single physician with an interval of 1 week and in different order, and the assessor was blinded to both treatment allocation and clinical outcome.
Statistics
Sample size calculation was based on the combined primary endpoints. On the basis of our experience, it was expected that 50% of patients would resume and maintain sports within 1 year after the surgical intervention. 40 Offering additional PEMF treatment, we aimed to improve this outcome to 75%. Saxena and Eakin 35 reported a mean sport resumption of 15 ± 4 weeks after debridement and microfracture. A 20% reduction in time to return to sports was considered clinically relevant (ie, 3 weeks). A sample size of 30 patients in each group (60 patients in total) had an 80% power to detect a joint difference (control group proportion of 0.50 vs treatment proportion of 0.75; control group mean of 15 weeks vs treatment group mean of 12 weeks, assuming a common standard deviation of 4), based on a Fisher combination test with a 2-sided significance level of 0.05. In reported clinical trials with this device, 9% to 13% of included patients dropped out.5,54 Therefore, 34 patients were included in each treatment group (68 patients in total).
All data were analyzed according to the intention-to-treat principle. Patient baseline characteristics were summarized in terms of simple descriptive statistics. Categorical data are presented as frequencies. Continuous data are presented as means with standard deviations or as medians with interquartile ranges (IQRs), depending on their distribution. The number of patients who resumed sports were analyzed with the chi-square test. The difference in time to sport resumption was analyzed by the Mann-Whitney U test. Kaplan-Meier survival curves and the log-rank test were also used for comparing time to resumption of sports. P < .05 was considered statistically significant for the primary outcomes.
Kaplan-Meier survival curves and the log-rank test were used for comparing time to resumption of work. With regard to the secondary clinical outcome scales, linear mixed models with a random intercept and—when model dimension permitted—random slope per patient were used to analyze the repeated data structure of the scales. The fixed part of the models consisted of a main linear time effect, a main group effect, and an interaction between time and group. For all outcomes, the interaction term was used to assess the difference in time trend between both groups. For NRS satisfaction, the main group effect was interpreted additionally, as this outcome was not measured preoperatively. To meet the normality assumption of the model, NRS pain at rest was analyzed on log(x + 1) scale and EQ-5D, FAOS sports, FAOS symptoms, FAOS pain, FAOS function, FAOS quality of life, and AOFAS on log(max(x) + 1 − x) scale. We also analyzed within each treatment group the scale score differences between baseline and 12-month outcome assessments using the paired t test on normal distribution and the Wilcoxon signed-rank test on skewed distribution. To correct for multiple testing, the Holm method was used for the secondary outcomes.2,20 Because 8 secondary outcome measures were involved, the adjusted significance level of the P value of the comparison with the smallest P value was set at .00625 (0.05/8), and the significance level of comparison with the largest P value was set at .05 (0.05/1). We analyzed the CT findings and number of adverse events using chi-square statistic. To assess the intraobserver reliability of the CT measurements, the intraclass correlation coefficient (ICC) was calculated; an ICC ≥0.85 indicates good reliability.12,27 All analyses were performed in SPSS (v 20.0; IBM Corp) and R (v 3.2.1; The R Foundation) and were reviewed by an independent statistician.
Results
After randomization, 36 patients were allocated to the PEMF group and 32 patients to the placebo group. As shown in Table 1, the baseline characteristics and stratification factors are well balanced. Four patients were lost to follow-up after the surgical intervention (Figure 2). The median compliance was 235 hours (IQR, 183-242) in the PEMF group and 217 hours (IQR, 187-240) in the placebo group, where the prescribed use was 240 hours.
Baseline Patient Characteristics a
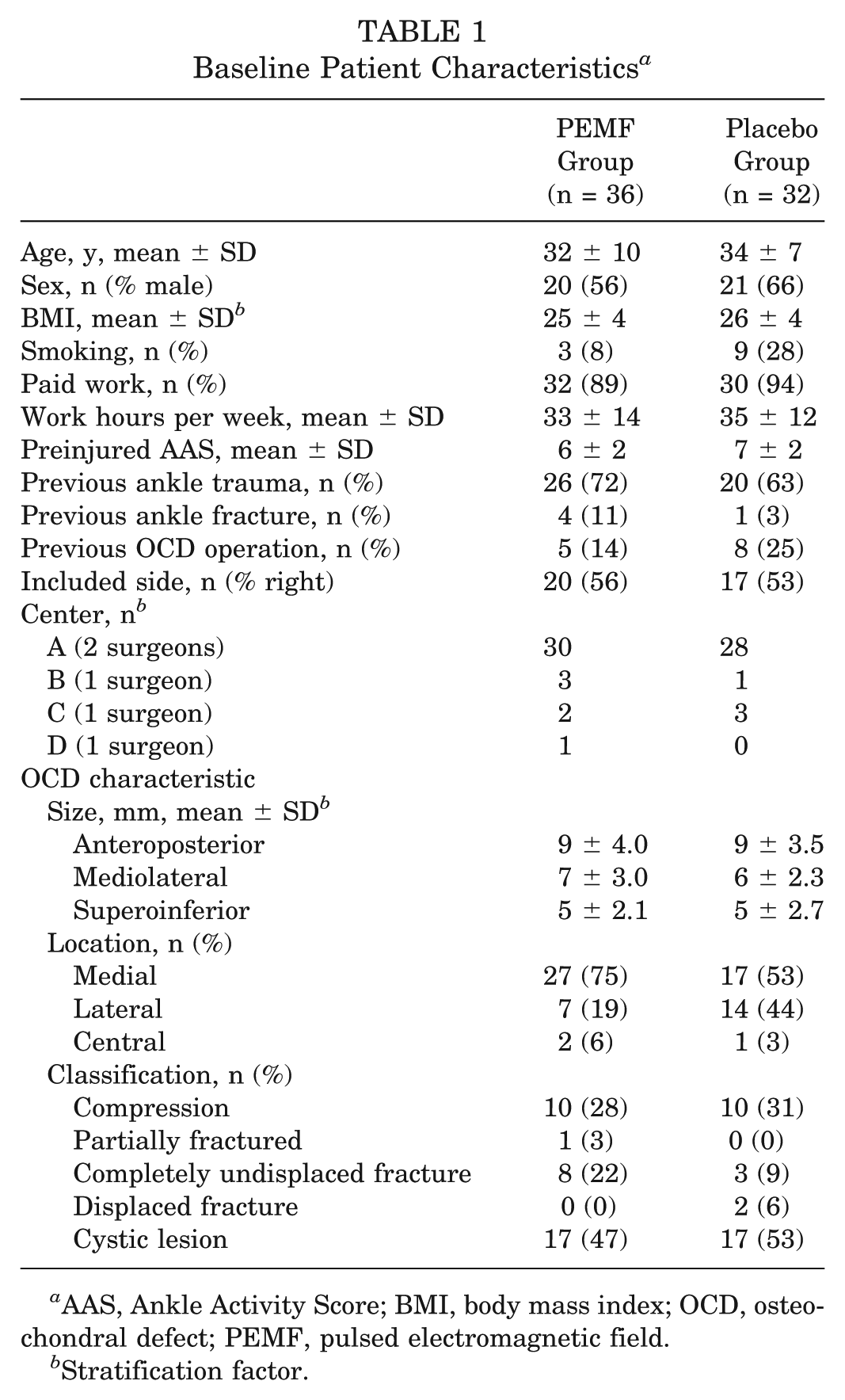
AAS, Ankle Activity Score; BMI, body mass index; OCD, osteochondral defect; PEMF, pulsed electromagnetic field.
Stratification factor.
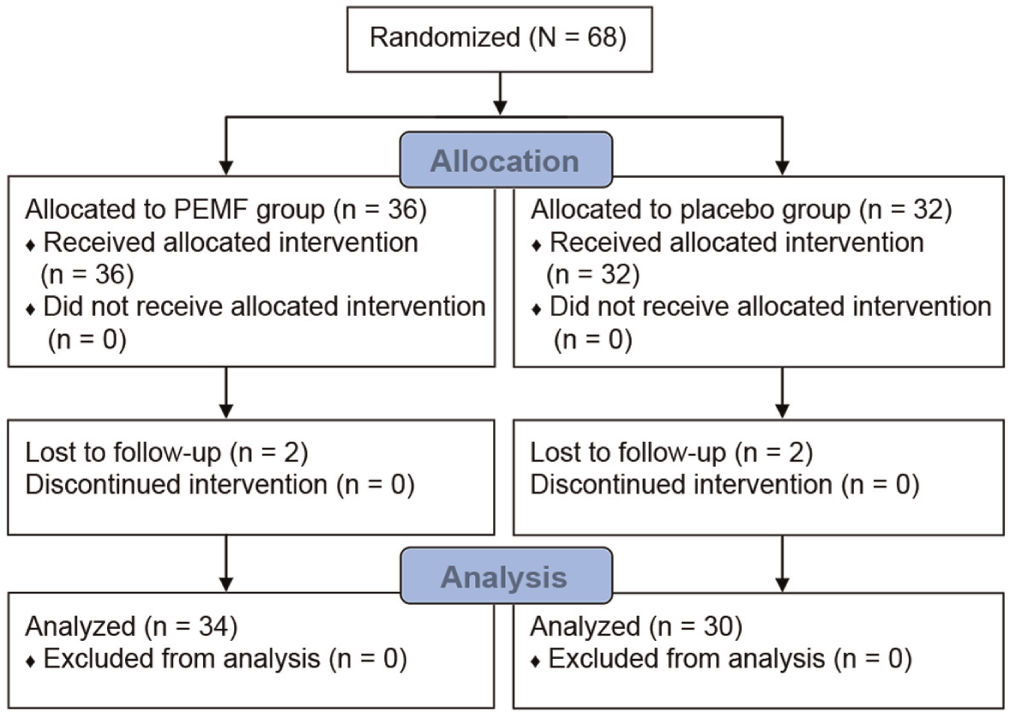
Flow diagram showing the randomization of included patients. Four patients were lost to follow-up after the surgical intervention and could not be included in the intention-to-treat analysis. PEMF, pulsed electromagnetic field.
Clinical Results
Resumption of sports was 79% in the PEMF group (27 of 34 patients) and 80% in the placebo group (24 of 30 patients) (P = .95). Of the patients who resumed sports, the median time to return was 17 weeks (IQR, 8-23) in the PEMF group and 16 weeks (IQR, 8-26) in the placebo group (P = .69) (Figure 3). An equal mean AAS of 6 ± 2 at the time of sport resumption was found in both groups. In the PEMF group, 23 of 27 patients returned to the same sport and in the placebo group, 20 of 24 patients.
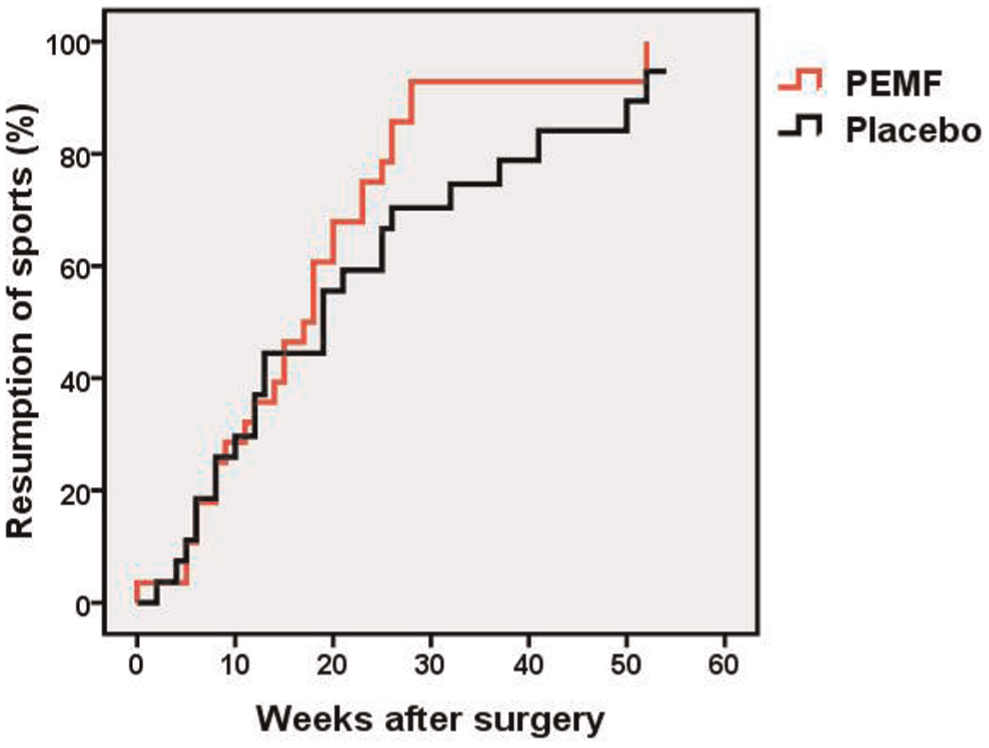
Kaplan-Meier curves of the patients who resumed sports after surgery (pulsed electromagnetic field [PEMF], n = 27; placebo, n = 24; P = .69).
The median time to work resumption was 6.5 weeks (IQR, 2-9) in the PEMF group and 5 weeks (IQR, 2-8) in the placebo group (P = .26). However, no statistically significant between-group differences over time were observed with regard to the AOFAS (P = .60), FAOS (P range, .03-.65), EQ-5D (P = .52), and NRS pain (rest, P = .50; running, P = .03) and satisfaction (P = .16) (Figure 4).
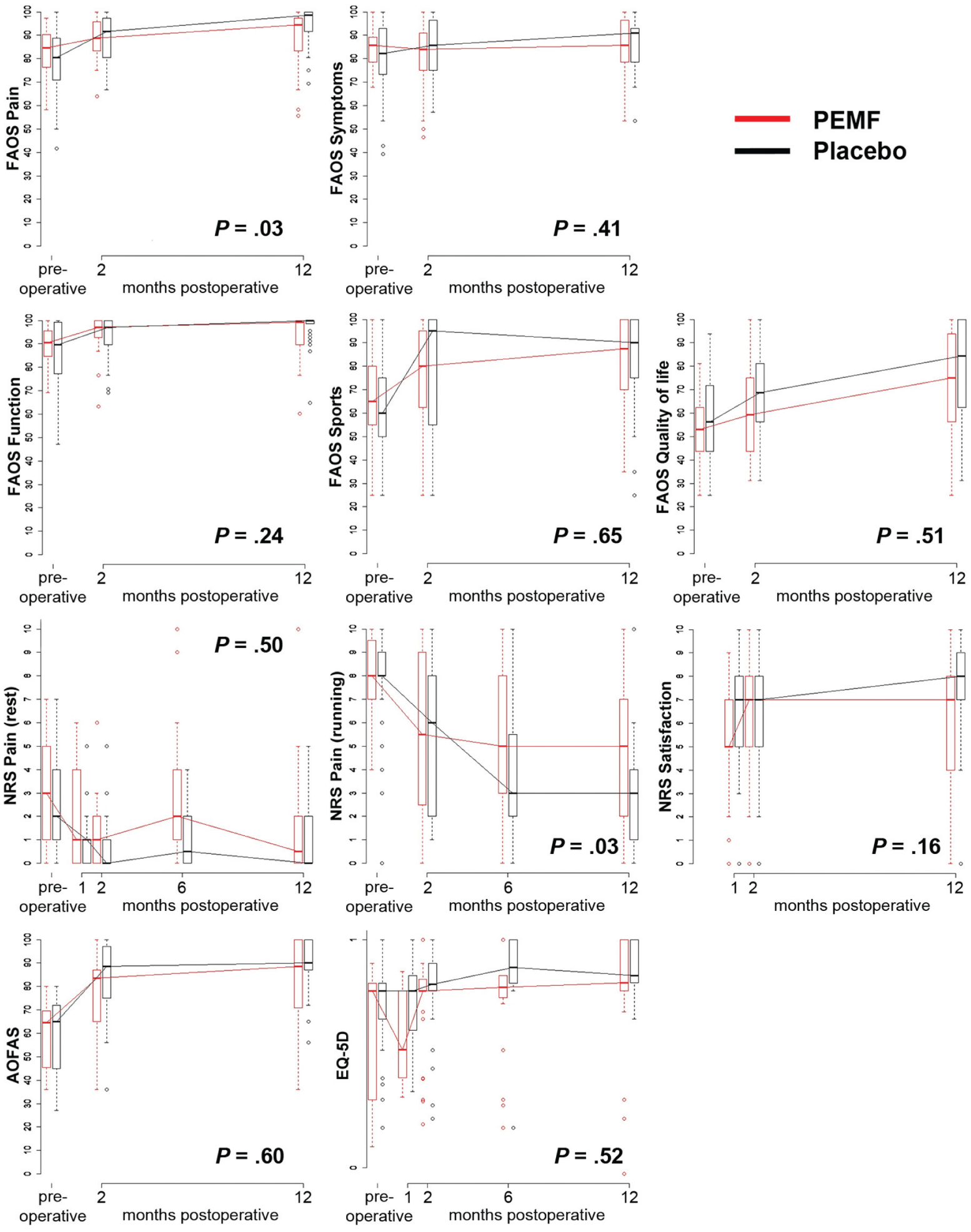
Linear mixed models showing secondary clinical outcome scores of the pulsed electromagnetic field (PEMF) and placebo groups. The boxes represent the interquartile range, and the lines denote the median. The error bars represent the minimum and maximum range. An adjusted significance level of the P value of the comparison with the smallest P value was set at .00625 (0.05/8), and the significance level of comparison with the largest P value was set at .05 (0.05/1). AOFAS, American Orthopaedic Foot and Ankle Society ankle-hindfoot score; EQ-5D, EuroQol; FAOS, Foot and Ankle Outcome Score; NRS, numeric rating scale.
As also can be observed from the graphs in Figure 4, all secondary outcome measures within both treatment groups improved from baseline to 12 months, with the exception of the FAOS symptoms subscale in the PEMF group. This time effect is illustrated in Table 2.
Clinical Outcome Measures at Baseline and at 1-Year Follow-up a
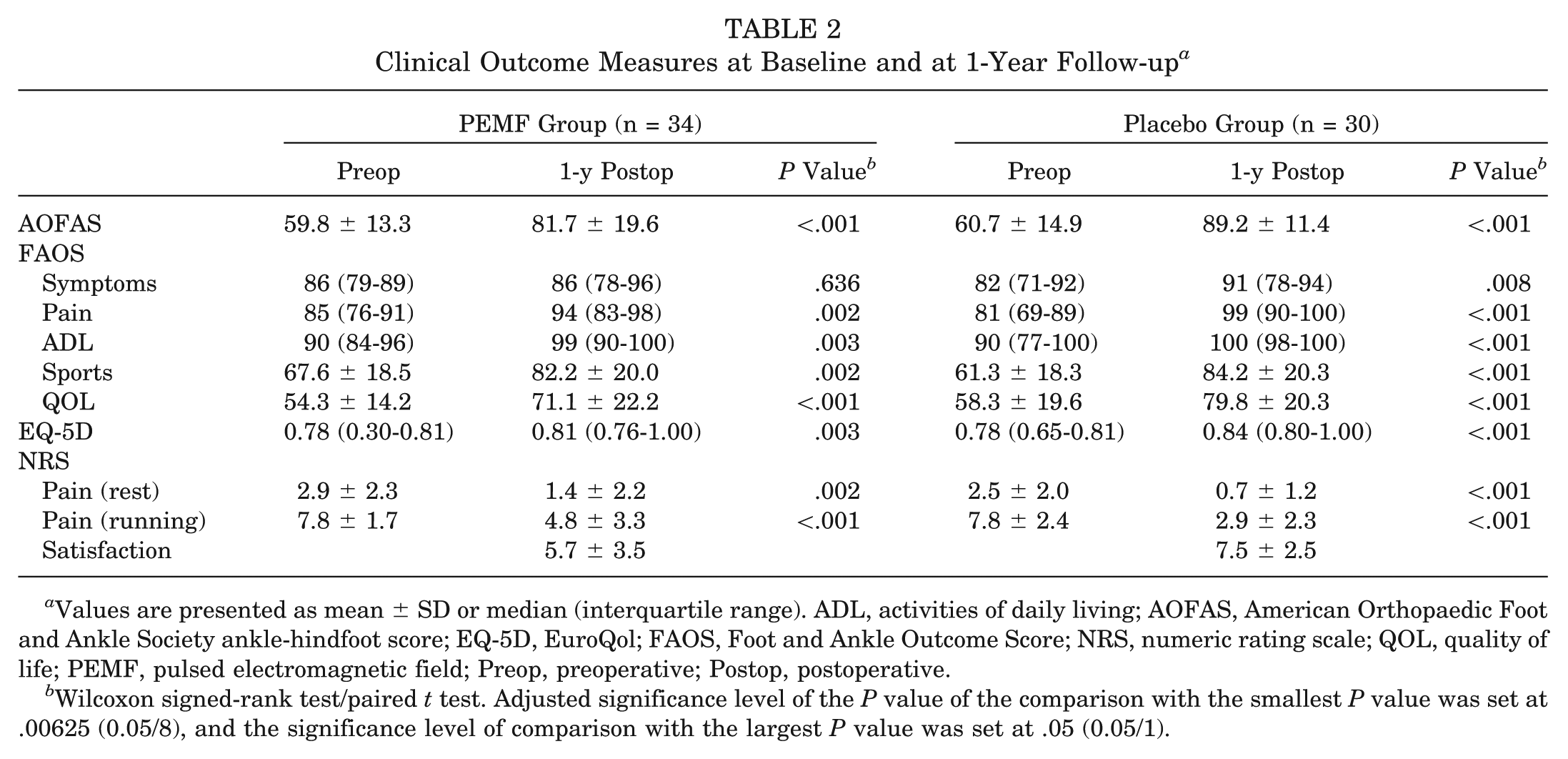
Values are presented as mean ± SD or median (interquartile range). ADL, activities of daily living; AOFAS, American Orthopaedic Foot and Ankle Society ankle-hindfoot score; EQ-5D, EuroQol; FAOS, Foot and Ankle Outcome Score; NRS, numeric rating scale; QOL, quality of life; PEMF, pulsed electromagnetic field; Preop, preoperative; Postop, postoperative.
Wilcoxon signed-rank test/paired t test. Adjusted significance level of the P value of the comparison with the smallest P value was set at .00625 (0.05/8), and the significance level of comparison with the largest P value was set at .05 (0.05/1).
Radiologic Results
In the PEMF group, 33 of 36 patients completed the preoperative and 1-year postoperative CT scans. Two patients were lost to follow-up, and 1 patient did not undergo the final CT scan because of pregnancy. In the placebo group, 29 of 32 patients completed the preoperative and 1-year postoperative CT scans. Two patients were lost to follow-up, and 1 patient underwent a HemiCAP procedure during follow-up because of persisted deep ankle pain after a new ankle distortion. 42
Intraobserver reliability of CT scan measurements was good (level of the subchondral bone plate, ICC = 0.92; bone volume filling, ICC = 0.91). No significant differences were observed between the groups (level of the subchondral bone plate, P = .24; bone volume filling, P = .33) (Table 3, Figure 5).
Computed Tomography Findings After Debridement and Microfracturing of Osteochondral Talar Defects a
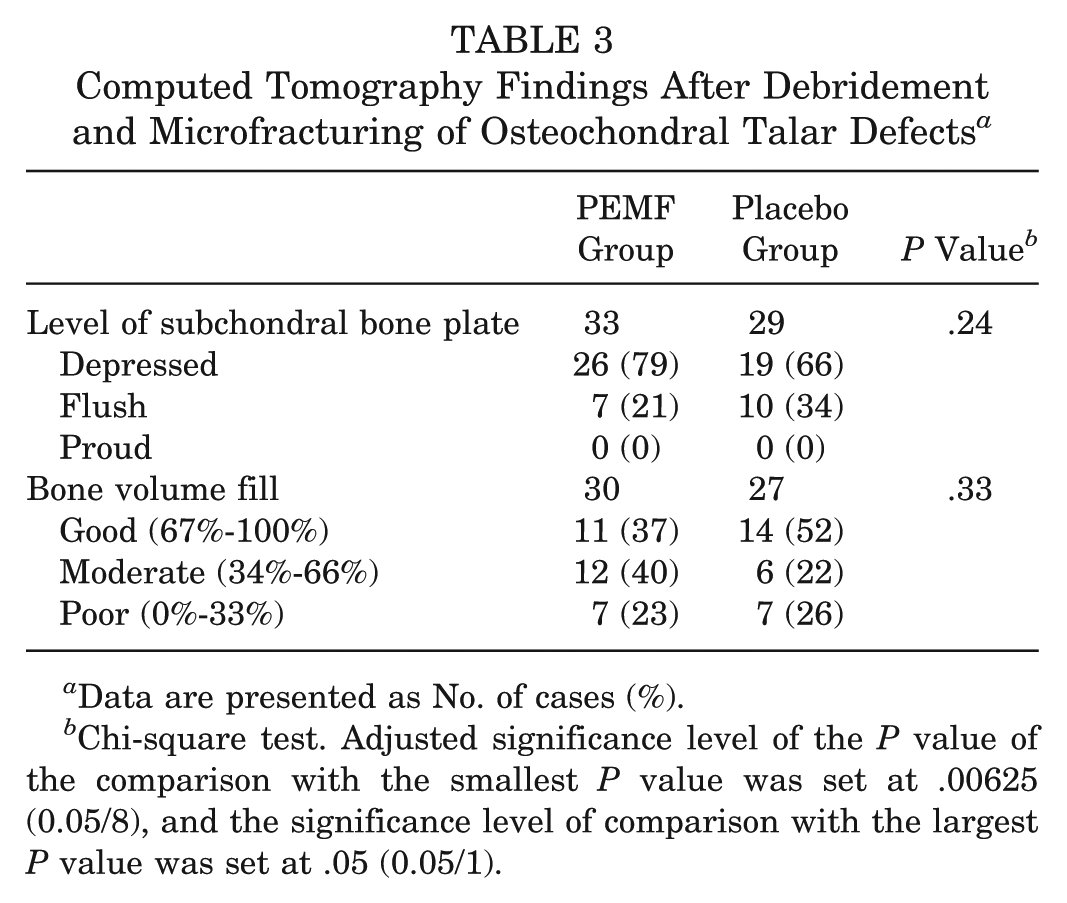
Data are presented as No. of cases (%).
Chi-square test. Adjusted significance level of the P value of the comparison with the smallest P value was set at .00625 (0.05/8), and the significance level of comparison with the largest P value was set at .05 (0.05/1).
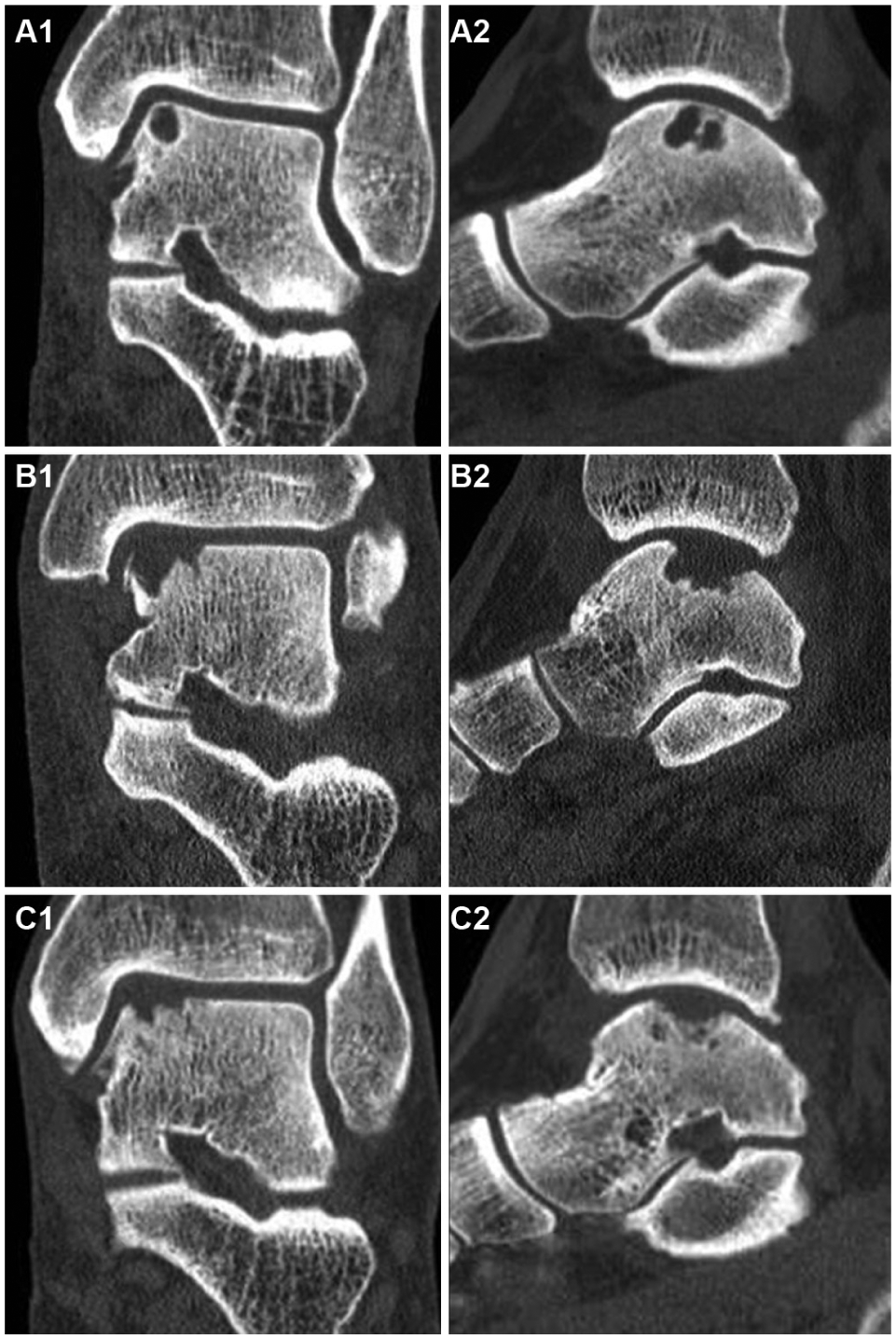
Preoperative (A1) coronal and (A2) sagittal computed tomography (CT) scans of a left ankle with a cystic osteochondral defect on the medial talar dome. Successful debridement and microfracture of the osteochondral defect are shown on the 2-week postoperative (B1) coronal and (B2) sagittal CT scans. (C1, C2) At 1-year follow-up, the subchondral bone plate is depressed; in comparison with the 2-week postoperative CT scans, a good bone volume fill (67%-100%) can be observed.
Complications
No serious adverse events occurred during the trial. Adverse events were seen in 7 patients. In the PEMF group, 2 patients reported temporary paresthesia of the dorsum of the foot, and 2 had prolonged wound leakage during the first week after surgery. In the placebo group, 1 patient reported nausea, 1 had a delayed healing of the wound, and 1 reported postoperative paresthesia of the dorsum of the foot and persistent deep ankle pain after a new distortion at 4-month follow-up. This patient was treated with a HemiCAP. 42 The number of adverse events did not differ significantly between groups (P = .81).
Discussion
This is the first double-blind, randomized, placebo-controlled trial to investigate the effect of PEMFs after debridement and microfracture of an OCD of the talus. In the present study, no differences were found in the percentage of sport resumption and time to sport resumption. Furthermore, there were no significant between-group differences with regard to the secondary functional outcomes or CT observations.
Our findings are in contrast with the scarce literature. Cadossi et al 8 found, in a randomized controlled trial, a significant AOFAS score improvement >10 points in the PEMF group after bone marrow–derived cell transplantation for OCDs of the talus at 1-year follow-up. However, the difference between the preoperative and 1-year postoperative AFOAS was 32 points in the control group and 40 points in the PEMF group. It is questionable if an 8-point difference on the AOFAS scale is clinically relevant. Furthermore, no placebo devices were used in the control group; therefore, a possible effect of the placebo intervention was not taken into account. In a randomized controlled pilot trial, Zorzi et al 54 reported a reduction in the use of nonsteroidal anti-inflammatory drugs and clinical improvement with PEMF treatment after arthroscopic chondroabrasion and/or perforation and/or radiofrequency of the knee. Although the pilot study showed a clinical improvement, a cautious interpretation is needed because of the small groups (PEMF, n = 19; placebo, n = 12) and no power analysis.
Regarding the treatment of OCDs of the talus, we consider bone regeneration more important than cartilage regeneration. Cartilage is not innervated; the patient’s pain probably arises from the bony lesion. 43 Furthermore, an advanced and irregular subchondral bone plate is associated with degradation of repaired articular surface. 31 Our study did not show any effect of PEMFs on the level of the subchondral bone plate repair. In both groups, more than two-thirds of the subchondral bone plates were depressed. This finding may explain why progression of ankle osteoarthritis is seen in 33% to 34% after arthroscopic debridement and bone marrow stimulation of an OCD of the talus at long-term follow-up.14,41 In the present study, no differences were found in the amount of bone volume filling between the PEMF and placebo groups on 2-dimensional CT analysis. Likewise, Hannemann et al 19 studied the addition of PEMFs in the nonoperative treatment of acute scaphoid fractures and concluded that PEMFs do not accelerate bone healing on CT. Furthermore, a meta-analysis of randomized controlled trials showed no differences in time to radiologic union between PEMF and placebo after surgical treatment in acute fractures. 18
Strengths of this study include the randomized, double-blind, placebo-controlled design; the high compliance in wearing the device; and the use of a broad set of validated outcome measures. Limitations include the lack of long-term follow-up and the loss to follow-up of 4 patients; however, we anticipated a follow-up loss of 8 patients in our sample size calculation. Another limitation is the 2-dimensional CT analysis of a 3-dimensional structure. Furthermore, the follow-up of the defects with CT scans may lead to higher radiation exposures, which is less accurate for cartilage evaluation in comparison with MRI; however, we were interested in the bone healing, which is better visible on CT.
In conclusion, applying PEMFs after arthroscopic debridement and microfracture of an OCD of the talus does not lead to earlier resumption of sports or to a higher percentage of patients who resume sports. Furthermore, PEMFs do not lead to functional and radiologic improvements up to 1-year follow-up.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Stryker, Waardenburg, the Netherlands, for providing financial support, and to IGEA medical, Carpi, Italy, for providing the active and placebo pulsed electromagnetic field devices.